Rev. bras. ortop. vol.46 número6 en a03v46n6
Texto
Imagem

Documentos relacionados
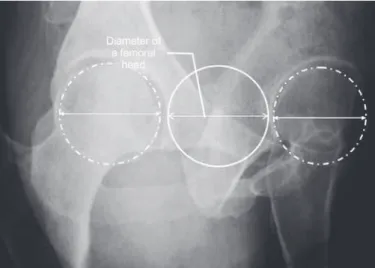
In our study, we evaluated the percentage of loss of the humeral head diameter, the depth of the HS lesion and the residual articular arc through the axial section with the largest
No statistically valid correlation was observed be- tween the subscapularis tendon lesion and its corres- ponding repair, with the occurrence of residual Popeye deformity (p =
We consider this an initial study on the adjuvant therapeutic approach using low-level laser therapy in the postoperative period of carpal tunnel syndrome. Other
WeitereBeitrage zu tramatish-mechanischen Enstenhung der “spontanen” Knorpelalblosungen (sogen. Osteochondritis dissecans). Transchondral fractures of the talus. Ferkel
The second group comprised patients treated using the posterior route associated with Smith-Petersen osteotomy, with a mean age of 27.3 years, preoperative kyphosis of 72.9°,
The results obtained in this study demonstrate that the bone marrow centrifugate was not able to induce a better quality of muscle healing, increasing the number of
Study conducted at the Knee Surgery Group of the Orthopedics and Traumatology Clinic of Hospital São Lucas da Pontifícia Universidade Católica do Rio Grande do Sul..
Miller et al (7) presented a report of fracture of the medial and lateral extremity of the clavicle with the use of a reconstruction plate and another with locking T-plate,
