Abst ract
Submitted: June 21, 2016 0RGL¿FDWLRQ6HSWHPEHU Accepted: September 22, 2016
Per iodont it is and t ype 2 diabet es
am ong w om en w it h pr evious
gest at ional diabet es: epidem iological
and im m unological aspect s in a
follow- up of t hr ee year s
Per iodont it is can cont r ibut e t o t he developm ent of insulin r esist ance. Gest at ional diabet es is a risk fact or for t ype 2 diabet es. Therefore, periodont it is, w hen associat ed w it h gest at ional diabet es, could incr ease t he r isk for t he developm ent of t ype 2 diabet es aft er pr egnancy. Obj ect ive: The aim of t his st udy was t o ver ify t he incidence on t he developm ent of t ype 2 diabet es in w om en w it h pr evious gest at ional diabet es w it h and w it hout per iodont it is aft er a t hr ee- year t im e int er val. Mat er ial and Met hods: I nit ial sam ple of t his follow- up st udy consist ed of 90 w om en diagnosed w it h gest at ional diabet es w ho under w ent per iodont al exam inat ion. Aft er t hr ee year s, 49 w om en w er e subj ect ed t o new per iodont al exam inat ion and biological, behavioral, and VRFLDOGDWDRILQWHUHVWZHUHFROOHFWHG$GGLWLRQDOO\WKHTXDQWL¿FDWLRQRIWKH C- r eact ive pr ot ein in blood sam ples was per for m ed. Fast ing glucose and glycat ed hem oglobin levels w er e r equest ed. Saliva sam ples w er e collect ed IRUTXDQWL¿FDWLRQRILQWHUOHXNLQDQGWXPRUQHFURVLVIDFWRUĮPDWUL[ m et alloprot einase 2 and 9. Result s: The incidence of t ype 2 diabet es m ellit us ZDV DQG RI SHULRGRQWLWLV ZDV 7KHUH ZDV QR VLJQL¿FDQW differ ence in t he incidence of t ype 2 diabet es m ellit us am ong w om en w it h and w it hout per iodont it is. I t was obser ved im pact of C- r eact ive pr ot ein in t he developm ent of t ype 2 diabet es m ellit us. How ever, it was not obser ved im pact of periodont it is on t he developm ent of t ype 2 diabet es m ellit us am ong w om en w it h pr evious gest at ional diabet es. Conclusions: I t was not obser ved im pact of periodont it is on t he developm ent of t ype 2 diabet es am ong w om en w it h pr evious gest at ional diabet es. The im pact of C- r eact ive pr ot ein in t he developm ent of t ype 2 diabet es m ellit us highlight s t he im por t ance of an LQÀDPPDWRU\SURFHVVLQWKHGLDEHWHVSDWKRJHQHVLV
Ke y w or ds: Gest at ional diabet es. Diabet es m ellit us. Diabet es m ellit us,
t ype 2. Per iodont it is. Pr egnant w om en. Rafael Paschoal ESTEVES LIMA1
Luis Otávio Miranda COTA1
Tarcília Aparecida SILVA1
Sheila Cavalca CORTELLI2
José Roberto CORTELLI2
Fernando Oliveira COSTA1
http://dx.doi.org/10.1590/1678-77572016-0367
1Universidade Federal de Minas Gerais, Faculdade de Odontologia, Departamento de Periodontologia
e Patologia, Belo Horizonte, MG, Brasil.
2Universidade de Taubaté, Centro de Pesquisa Periodontal, Taubaté, SP, Brasil.
I nt r oduct ion
3HULRGRQWLWLVLVDQLQIHFWLRXVLQÀDPPDWRU\FRQGLWLRQ of per iodont al t issues charact er ized by loss of t oot h
support17KHSURGXFWLRQRILQÀDPPDWRU\PHGLDWRUVLQ
t he pat hogenesis of t he disease called t he at t ent ion t o
t he sy st em ic im pact of per iodont it is and it s pot ent ial
associat ion w it h ot her condit ions13.
Diab et es m ellit u s ( DM) com p r ises a g r ou p of
disor der s charact er ized by high blood glucose levels,
an d it is con sid er ed an im p or t an t r isk f act or f or
periodont it is2$OWHUDWLRQVLQWKHLPPXQRLQÀDPPDWRU\ UHVSRQVH RI LQGLYLGXDOV ZLWK '0 FDQ LQÀXHQFH WKH prevalence, ext ension, and severit y of periodont it is. On WKHRWKHUKDQGWKHSHULRGRQWDOLQÀDPPDWRU\SURFHVV can cont ribut e t o a condit ion of insulin resist ance, wit h
im pact on t he glycem ic cont r ol and m anifest at ion of
DM. The dissem inat ion of bact er ia and t heir pr oduct s E\SHULRGRQWLWLVFDQLQGXFHDV\VWHPLFLQÀDPPDWRU\ st at e t hat can init iat e and propagat e insulin resist ance. +LJKOHYHOVRILQÀDPPDWRU\PHGLDWRUVVXFKDV t um or n ecr osis f act or alp h a ( TNF-D) , in t er leu k in 6 ( I
L-6) , and C- r eact ive pr ot ein ( CRP) , m ight cont r ibut e
t o an incr ease in insulin r esist ance2 4. Addit ionally,
p er iod on t al b act er ia can t r an slocat e t o t h e liv er,
inhibit t he insulin signaling, and r esult in decr eased
glycogen sy nt hesis17. Recent sy st em at ic r ev iew s have
dem onst rat ed t hat per iodont al t herapy can posit ively
affect t he cont r ol of DM11,22.
Gest at ional DM ( GDM) is a hy per glycem ic st at us WKDWLQLWLDWHVGXULQJJHVWDWLRQ,WSUHVHQWVVLJQL¿FDQW associat ed com p licat ion s an d h ig h m or b id it y. An
expressive risk for t he developm ent of DM t ype- 2 (
DM-2) was r epor t ed am ong w om en w it h GDM. Ther efor e,
t he diagnosis of GDM const it ut es an oppor t unit y for
ear ly int er vent ion of DM- 22.
Based on t h e possibilit y t h at per iodon t it is can
cont r ibut e t o t he developm ent of insulin r esist ance,
periodont it is, when present in wom en wit h GDM, could
also incr ease t he r isk for t he developm ent of DM- 2
aft er t he gest at ional per iod. To our k now ledge, only
one st udy evaluat ed t he im pact of per iodont it is on
t he incidence of DM- 2 am ong w om en w it h pr ev ious
GDM, point ing out t hat w om en w it h a hist or y of GDM
and periodont it is have im paired glucose m et abolism29.
Ther efor e, addit ional st udies ar e necessar y t o bet t er
addr ess t his pot ent ial associat ion.
The aim of t he present follow- up st udy was t o verify
t he incidence on t he developm ent of t y pe 2 diabet es
in w om en w it h pr ev ious gest at ional diabet es w it h and
w it hout per iodont it is aft er a t hr ee- year t im e int er val,
and t o quant ify CRP in t he blood as w ell as TNF-D,
I L- 6, int er leuk in 10 ( I L- 10) , m at r ix m et allopr ot einase
2 ( MMP- 2) , and m at r ix m et allopr ot einase 9 ( MMP- 9)
in t he saliva.
Mat er ial and m et hods
Sam pling st rat egy
The sam ple of t he pr esent follow- up st udy init ially
com prised a cohort of 90 wom en previously diagnosed
w it h GDM fr om a pr ev ious case- cont r ol st udy t hat
invest igat ed t he associat ion bet ween periodont it is and
GDM13. These w om en r eceived pr enat al car e in t he
Odet e Valadar es Mat er nit y Hospit al, in Belo Hor izont e
cit y – Brazil, fr om Febr uar y 2010 t o Novem ber 2011,
per iod w hen t hey w er e diagnosed w it h GDM.
Subsequent ly, t hese 90 w om en w er e inv it ed t o
par t icipat e in t he pr esent st udy by phone or m ail
con t act . Fr om t h is t ot al, 3 9 w om en cou ld n ot be
locat ed and t w o r efused t o par t icipat e. Ther efor e, t he ¿QDO VDPSOH FRPSULVHG ZRPHQ ZLWK D SUHYLRXV diagnosis of GDM.
The est ablished inclusion crit eria were t he presence RIQDWXUDOWHHWKDQGDEVHQFHRIFRQWUDLQGLFDWLRQV for t he periodont al exam inat ion. The exclusion crit eria
included ant ibiot ic or periodont al t herapy t hree m ont hs
p r ior t o clin ical ex am in at ion an d p osit iv e h u m an LPPXQRGH¿FLHQF\YLUXVLQIHFWLRQVHURORJ\
The pr esent st udy w as appr ov ed by t he Et hics
Resear ch Com m it t ee f r om t h e Fed er al Un iv er sit y
of Min as Ger ais ( CAAE 2 8 7 0 8 8 1 4 . 6 . 0 0 0 0 . 5 1 4 9 ) .
Part icipant s were inform ed about t he st udy and signed
an infor m ed consent for m .
Sociodem ographic charact er ist ics
Social and dem ographic dat a w er e collect ed for
each par t icipant t hr ough st r uct ur ed quest ionnair es.
We collect ed d at a r eg ar d in g ag e, m ar it al st at u s,
educat ional level, gest at ional period and delivery dat e, SDULW\VPRNLQJKDELWVDQG¿UVWGHJUHHUHODWLYHVZLWK '0 5HJDUGLQJ VPRNLQJ ZRPHQ ZHUH FODVVL¿HG DV sm oker s, for m er sm oker s, and non- sm oker s25.
Medical dat a
Weight and height of par t icipant s w er e r ecor ded
w eight , over w eight , or obese27.
Fast in g g lu cose t est an d g ly cat ed h em og lob in
levels were collect ed for each part icipant . When exam s
show ed alt er ed glycem ic levels, t hey w er e per for m ed DJDLQWRFRQ¿UPWKHGLDJQRVLVRI'09DOXHVKLJKHU t h an 1 2 5 m g/ dl for fast in g glu cose an d 6 . 4 % for
glycat ed hem oglobin w er e consider ed posit ive for t he
diagnosis of DM- 2. Pr e- diabet es was diagnosed as t he
pr esence of values higher t han 99 m g/ dl for fast ing
glucose and 5.6% for glycat ed hem oglobin, accor ding
t o t he Am erican Diabet es Associat ion2 ( 2014) . Sam ple
was divided in t wo groups according t o glycem ic levels:
a) nor m al fast ing glucose gr oup ( NFG) ; b) alt er ed
fast ing glucose gr oup ( AFG) . Subsequent ly, t hey w er e
su bdiv ided in t h r ee gr ou ps accor din g t o gly cem ic
diagnosis: nor m al, pr e- diabet es, and DM- 2.
Addit ionally, we request ed a blood t est for assessing
t he CRP levels. The CRP level less t han 5 m g/ l was
consider ed nor m al. Values gr eat er t han or equal t o 5
m g/ l w er e consider ed abnor m al20.
Per iodont al clinical exam inat ion
Par t icipant s under w ent a per iodont al ex am inat ion
dur ing gest at ion in a pr ev ious st udy13, det er m ined t o
be t he baseline ex am inat ion ( T0) , w hen param et er s
of bleeding on pr obing ( BOP) , pr obing dept h ( PD) ,
and clinical at t achm ent level ( CAL) w er e evaluat ed.
At T0, t he prevalence of periodont it is was 40% am ong
w om en w it h GDM13.
Pa r t i c i p a n t s u n d e r w e n t a n e w p e r i o d o n t a l
ex am inat ion aft er a per iod of appr ox im at ely t hr ee
year s aft er deliver y ( 34.5± 6.4 m ont hs) , det er m ined WREHWKH¿QDOH[DPLQDWLRQ73HULRGRQWDOH[DPV com pr ised cir cum fer ent ial pr obing w it h t he r ecor ding
of per iodon t al par am et er s at f ou r sit es per t oot h
( dist al, m esial, buccal, and lingual) w it h a m anual
pr obe ( UNC- 15, Hu- Fr iedy, Chicago, I L) . Per iodont al
exam inat ions w er e per for m ed by a single per iodont ist
( R.P.E.L.) , t rained and calibrat ed, r esponsible for t he
init ial exam inat ion of t he par t icipant s. I nt ra- ex am iner
agr eem ent for all clinical per iodont al param et er s of
int er est , bot h at T0 and T1, show ed kappa values
higher t han 0.90.
All collect ed dat a w er e r ecor ded and evaluat ed IRUHDFKSDUWLFLSDQWLQRUGHUWRGH¿QHVWXG\JURXSV The follow ing exclusion cr it er ia w er e also adopt ed
dur ing per iodont al ex am inat ion: t hir d m olar s, t eet h
w hose cem ent um - enam el j unct ion was im possible t o
det erm ine, t eet h wit h gingival m orphology alt erat ions,
t e e t h w i t h e x t e n si v e ca r i e s l e si o n s, t e e t h w i t h
iat r ogenic r est orat ive pr ocedur es, excessive calculus
pr esence.
7KH FULWHULD IRU SHULRGRQWLWLV GH¿QLWLRQ ZDV WKH SUHVHQFHRIWHHWKKDYLQJVLWHVZLWK3'PP DQG&$/PPDVVRFLDWHGZLWK%2315. Per iodont it is ZDVFODVVL¿HGLQUHODWLRQWRH[WHQVLRQDFFRUGLQJWR t he num ber of affect ed sit es: 30% of sit es ( localized) ,
and > 30% of sit es ( generalized) . Per iodont it is was DOVRFODVVL¿HGLQUHODWLRQWRVHYHULW\DFFRUGLQJWRWKH am ount of at t achm ent loss: 1- 2 m m ( slight form ) , 3- 4
PPPRGHUDWHIRUPDQGPPVHYHUHIRUP3.
Salivar y exam inat ion
St im ulat ed w hole saliva sam ple collect ions w er e
p er f or m ed t o q u an t i f y t h e l ev el s of I L- 6 , I L- 1 0 ,
MMP- 2, MMP- 9, and TNF-D. The collect ion of saliva
was per for m ed consider ing t he per iod of t w o hour s
aft er t he last m eal. For t he st im ulus of t he salivar y ÀRZ t he par t icipant s chew ed t he hyper boloid IRU¿YH m inut es and t he saliva pr oduced w as collect ed on
graph t ubes. The saliva sam ple was kept in a cooler
w it h ice and it was t ranspor t ed im m ediat ely t o t he
labor at or y w h er e t h e t ot al v olu m e w as r egist er ed
and cent r ifuged at 3000 r pm for 15 m inut es at 4°C.
The volum e was m easur ed w it h a m icr opipet t e. Aft er
cent rifuging, t he saliva was dilut ed in t he proport ion of
1: 1 in PBS solut ion ( 0.4 m M NaCl and 10 m M NaPO4)
cont aining pr ot ease inhibit or s ( 0.1 m M phenyl m et hyl
sulfonyl ÀXRULGH, 0.1 m M benzet honium chlor ide, 10
m M EDTA and 0.01 m g/ m L apr ot inin A) . The solut ion
was hom ogenized, dist r ibut ed in aliquot s, and fr oze
at - 8 0 °C t o per f or m t h e an aly sis by ELI SA. Th e
concent rat ions of t he cyt okines I L- 10, 2,
MMP-9, and TNF-D in t he saliva sam ples w er e det er m ined
by t he sandw ich t echnique using t he DuoSet Kit ( R&D
Syst em s, Minneapolis, MN, USA) . Det ect ion lim it s were
from 31.2 t o 1000 pg/ m L for TNF-Į, 390- 12500 pg/ m L
for MMP- 9/ TI MP2, 125- 4000 pg/ m L for MMP- 2/ TI MP2,
and 125- 2000 pg/ m L for I L- 10. The TXDQWL¿FDWLRQ of
I L- 6 was per for m ed using t he hum an I L- 6 Kit and
it s quant ikine ( R&D Syst em s, Minneapolis, MN) , w it h
det ect ion lim it s fr om 0.156 t o 10 pg/ m L. Techniques
w er e p er f or m ed accor d in g t o t h e m an u f act u r er ’s VSHFL¿FDWLRQV The concent rat ions w er e expr essed in pg/ m L. The concent rat ion of t ot al pr ot ein was used
t o cor r ect t he cy t ok ine value for each sam ple. The
St at ist ical analysis
I nit ially, a descr ipt ive analy sis of t he sam ple and
a com par ison of per iodont al st at us bet w een T0 and
T1 w er e per for m ed. For t his pur pose, t he Wilcoxon
t est w as u sed f or q u an t it at iv e v ar iab les an d t h e
McNem ar or St uar t - Max w ell ( for m or e t han t w o levels
of com par ison) w er e used for cat egor ical var iables.
For t he univar iat e analy sis, consider ing t he NFG
an d AFG gr ou ps, t h e Man n - Wh it n ey an d Kr u sk
al-Wallis t est s w er e used for quant it at ive var iables, and
t he Chi- squar ed or Fisher ex act t est es w er e used for FDWHJRULFDOYDULDEOHV6XEVHTXHQWO\WKHLQÀXHQFHRI biological, behavioral, and social variables in alt erat ions
of fast ing glucose and glycat ed hem oglobin exam s was
analy zed t hr ough a m ult inom ial logist ic r egr ession. A VLJQL¿FDQFHOHYHOLQWKHXQLYDULDWHDQDO\VLVDV w ell as t he biological plausibilit y, was adopt ed for t he
select ion of variables t o ent er t he m odels. All collect ed
dat a w er e st or ed in a dat abase ( S1 Dat aset ) , and
all analyses w er e per for m ed by m eans of st at ist ical
soft war e ( R ver sion 3.0.1, R Foundat ion for St at ist ical
Com put ing, Vienna, Aust ria) . Result s w ere considered VLJQL¿FDQWIRUDSUREDELOLW\ORZHUWKDQS
Result s
We p r esen t t h e ch ar act er ist ics of t h e sam p le
according t o biological, behavioral, and social variables
for NFG and AFG gr oups in Table 1. We obser v ed
si g n i f i can t d i f f er en ces r eg ar d i n g m ean BMI an d
glycem ic values. Sim ilar r esult s w er e obser ved in t he
analysis of t he biological, behavioral, and social dat a
according t o fast ing glucose diagnosis at T1. There was
a VLJQL¿FDQWGLIIHUHQFHEHWZHHQWKH gr oups r egar ding
m ean BMI ( p= 0. 014) . The incidence of DM- 2 w as
18.4% .
Table 2 show s WKH TXDQWL¿FDWLRQ of biochem ical
v ar iables f or NFG an d AFG gr ou ps. We descr ibed
CRP ca t eg o r i ca l l y a n d q u a n t i t a t i v el y . I m p o r t a n t
differences in t he levels of CRP were observed bet ween
t he gr oups. Appr oxim at ely 53% of t he AFG w om en
dem on st r at ed ch an ges in CRP lev els, w h ile in t h e
NFG gr oup t his per cent age w as 23.5% ( p= 0.040) .
Wh en CRP w as qu an t it at iv ely ev alu at ed, a h igh er
average was obser ved in t he AFG ( p= 0.077) . Ther e ZDV QRW DQ\ VLJQL¿FDQW GLIIHUHQFH bet w een gr oups for I L- 6, I L- 10, MMP- 2, MMP- 9, and TNF-D values.
Sim ilar r esult s w er e obser ved for t he analy sis of t he
FRQFHQWUDWLRQV RI LQÀDPPDWRU\ PHGLDWRUV in blood
and saliva accor ding t o endocr ine diagnosis. Ther e
was a differ ence bet w een t he gr oups r egar ding CRP
descr ibed cat egor ically.
We present periodont al st at us at T0 and T1 for NFG
and AFG gr oups in Table 3. At T1, t he fr equency of
per iodont it is was higher in AFG gr oup ( 46.7% ) w hen
com par ed w it h NFG gr oup ( 35. 3% ) . How ever, t his GLIIHUHQFH ZDV QRW VWDWLVWLFDOO\ VLJQL¿FDQWw her eas 38.8% of t he sam ple was diagnosed w it h periodont it is
at T1. The incidence of per iodont it is in AFG was 20% . ,W ZDV REVHUYHG D VLJQL¿FDQW GLIIHUHQFH UHJDUGLQJ t he num ber of t eet h fr om T0 t o T1 in t he sam ple.
How ever, t his differ ence was not pr esent w hen gr oups
w er e com par ed. Wom en in t he AFG gr oup pr esent ed
a higher per cent age of sit es w it h BOP and higher PD.
Fr om T0 t o T1, w om en in t he AFG gr oup pr esent ed a VLJQL¿FDQWLQFUHDVHLQWKHQXPEHURIVLWHVZLWK%23 DQG3'PPDQG&$/PP&KDUDFWHULVWLFVRIWKH sam ple concer ning per iodont al st at us at T0 and T1
ar e pr esent ed in Table 4, accor ding t o t he endocr ine
diagnosis7KHUHZDVQRVLJQL¿FDQWGLIIHUHQFHUHJDUGLQJ
t he fr equency of per iodont it is, as w ell as per iodont al
param et er s, am ong t he gr oups in bot h ex am inat ions.
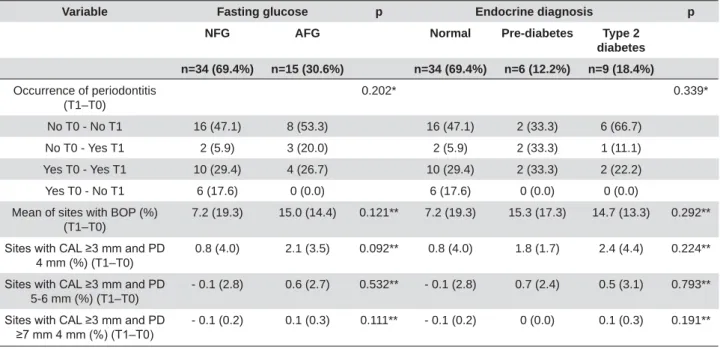
We pr esent changes in per iodont al st at us fr om T0
t o T1, for bot h AFG and NFG gr oups, and accor ding t o
t he endocr ine diagnosis, in Table 5. I n t he AFG gr oup,
t he per cent age of w om en w ho develop per iodont it is
bet w een T0 and T1 was higher. I n addit ion, w om en in
t he AFG group present ed worse periodont al param et ers
fr om T0 t o T1. The fr equency of per iodont it is at bot h
T0 and T1, or only at T1, was higher am ong w om en
diagnosed wit h pre- diabet es, alt hough not st at ist ically VLJQL¿FDQW:RPHQGLDJQRVHGZLWK'0SUHVHQWHGD higher incr ease in PD fr om T0 t o T1.
,QWKH¿QDOPXOWLYDULDWHORJLVWLFUHJUHVVLRQPRGHO RQO\ &53 UHPDLQHG DV D VLJQL¿FDQW YDULDEOH w it h g ly cem ic con t r ol ( OR 1 . 3 1 ; 9 5 % CI = 1 . 0 3 - 1 3 . 4 5 ;
p= 0.046) . Sim ilarly, t he m ult inom ial logist ic regression
m odel ( consider ing t he endocr ine diagnosis) r et ained RQO\&53DVDVLJQL¿FDQWYDULDEOHIRU'025 p= 0.022) .
We also per for m ed all analy ses using gly cat ed
h em oglobin t o est ablish t h e en docr in e diagn osis.
Sim ilar r esult s w er e obser ved using fast ing glucose
diagnosis. I t is im port ant t o highlight t hat we observed D KLJK DQG VLJQL¿FDQW DJUHHPHQW EHWZHHQ IDVWLQJ glucose and glycat ed hem oglobin exam inat ions ( kappa
Variable Glycemic control p NFG (n=34; 69.4%) AFG (n=15; 30.6%)
CRP 0.040*
Normal 26 (76.5) 7 (46.7)
Altered 8 (23.5) 8 (53.3)
CRP (mg/l) 5.4 (10.4) 7.8 (7.9) 0.077**
IL-10 (pg/mg) 24.8 (61.5) 31.2 (68.0) 0.723**
MMP-9 (pg/mg) 1356.4 (1053.1) 1136.4 (986.0) 0.641**
MMP-2 (pg/mg) 126.8 (150.7) 156.8 (163.2) 0.494**
IL-6 (pg/mg) 55.3 (93.4) 41.6 (73.3) 0.956**
TNF-D (pg/mg) 32.8 (90.1) 27.8 (58.8) 0.312**
*Chi-squared test; **Mann-Whitney test; NFG = normal fasting glucose; AFG = altered fasting glucose; CRP = c-reactive protein; IL-6 = interleukin 6; IL-10 = interleukin 10; MMP-2 = matrix metalloproteinase 2; MMP-9 = matrix metalloproteinase 9; TNF-D = tumor necrosis fator alpha
Table 2-&KDUDFWHULVWLFVRIWKHVDPSOHLQUHODWLRQWRWKHFRQFHQWUDWLRQRILQÀDPPDWRU\PHGLDWRUVLQEORRGDQGVDOLYDDFFRUGLQJWRJO\FHPLF
control
Variables Total sample (n=49) Glycemic control p NFG (n=34; 69.4%) AFG (n=15; 30.6%)
Age in years (±) 35.3 ± 5.1 34.9 ± 4.9 36.1 ± 5.4 0.317*
Marital status (%) 0.765**
with companion 41 (83.7%) 29 (85.3%) 12 (80.0%)
without companion 7 (14.3%) 4 (11.8%) 3 (20.0%)
Other 1 (2.0%) 1 (2.9%) 0 (0.0%)
Educational level (%) 0.482**
\HDUV 22 (44.9%) 14 (41.2%) 8 (53.3%)
From 9 to 12 years 25 (51.0%) 19 (55.9%) 6 (40.0%)
\HDUV 2 (4.1%) 1 (2.9%) 1 (6.7%)
Parity (±) 2.4 (1.3) 2.4 (1.1) 2.2 (1.9) 0.136*
Time since delivery in months (±)
34.5 ± 6.4 34.1 ± 6.3 35.6 ± 6.8 0.467*
Smoking habits (%)
smoker 2 (4.1%) 2 (5.9%) 0 (0.0%) 1.000**
former smoker 8 (16.3%) 6 (17.2%) 2 (13.3%) 0.702**
Diabetes (%) 4 (8.2%) 0 (0.0%) 4 (28.6%) 0.005**
Family history of diabetes (%)
29 (59.2) 18 (52.9) 11 (73.3) 0.221**
BMI (%) 0.070**
adequate 13 (26.5) 12 (35.3) 1 (6.7)
overweight 16 (32.7) 11 (32.4) 5 (33.3)
obesity 20 (40.8) 11 (32.4) 9 (60.0)
BMI (mean) 30.3 (7.5) 28.6 (6.8) 33.9 (7.7) 0.014*
Fasting glucose (mean) 103 (33.6) 87.4 (7.5) 138.7 (42.2) 0.000*
Glycated hemoglobin (mean)
5.5 (1.1) 5.0 (1.0) 6.9 (1.0) 0.000*
*Mann-Whitney test; **Chi-squared test; NFG = normal fasting glucose; AFG = altered fasting glucose
Discussion
The biological plausibilit y WKDW WKH LQÀDPPDWRU\
pr ocess induced by per iodont it is could cont r ibut e t o
insulin r esist ance, and DM- 2 developm ent can also be
applied t o GDM. The num ber of st udies t hat evaluat ed
t he r elat ionship bet w een per iodont it is and GDM is
r educed4,5,9,13,280RUHRYHU¿QGLQJVIURPWKHVHVWXGLHV
ar e cont r over sial. Som e st udies5,28 dem onst rat ed t hat
per iodont it is was m or e fr equent am ong w om en w it h
GDM com par ed w it h w om en w it hout GDM. How ever,
ot her st udies4,9,13 did not ident ify differ ences in t he
fr equency of per iodont it is am ong w om en w it h and
w it hout GDM. I m por t ant m et hodological differ ences,
su ch as sam p l e si ze an d d i ag n o st i c cr i t er i a f o r SHULRGRQWLWLV DQG *'0 GR H[LVW DQG GLI¿FXOW WKH com par isons of t he r esult s.
Findings from t he present st udy dem onst rat ed t hat
t he fr equency of per iodont it is was not higher am ong
w om en w it h pr ev ious hist or y of GDM t hat developed
Variables Total sample n=49 (%) Glycemic control p NFG n=34 (69.4%) AFG n=15 (30.6%)
Presence of periodontitis (%)
T0 20 (40.8) 16 (47.1) 4 (26.7) 0.221*
T1 19 (38.8) 12 (35.3) 7 (46.7) 0.451*
p 0.763*** 0.157*** 0.083***
Present teeth (±)
T0 27.5 (3.0) 27.3 (3.2) 27.9 (1.9) 0.635**
T1 27.1 (2.9) 26.9 (3.3) 27.7 (2.2) 0.515**
p 0.002**** 0.000**** 0.427****
Extension of periodontitis (%)
Localized T0 20 (40.8) 16 (47.1) 4 (26.7) 0.221*
Localized T1 17 (34.7) 11 (32.4) 6 (40.0) 0.741*
p 0.404*** 0.096*** 0.317***
Extension of periodontitis (%)
Generalized T0 0 (0.0) 0 (0.0) 0 (0.0)
-Generalized T1 2 (4.1) 1 (2.9) 1 (6.7) 0.489*
p 0.157*** 0.317*** 0.317***
Severity of periodontitis (%)
Moderate T0 1 (2.0) 1 (2.9) 0 (0.0) 1.000*
Moderate T1 3 (6.1) 2 (5.9) 1 (6.7) 1.000*
p 0.317*** 0.563*** 0.317***
Severity of periodontitis (%)
Advanced T0 19 (38.8) 15 (44.1) 4 (26.7) 0.341*
Advanced T1 16 (32.7) 10 (29.4) 6 (40.0) 0.515*
p 0.366*** 0.095*** 0.157***
Sites with BOP (%)
T0 22.9 (15.9) 22.6 (15.7) 23.6 (17.0) 0.905**
T1 32.5 (21.7) 29.8 (20.6) 38.5 (23.7) 0.121**
p 0.001**** 0.047**** 0.004****
6LWHVZLWK&$/PPDQG3'PP T0
T1 2.8 (3.3) 2.9 (2.8) 2.7 (4.3) 0.314**
4.0 (5.7) 3.7 (5.1) 4.8 (7.1) 0.315**
p 0.067**** 0.3757**** 0.009****
6LWHVZLWK&$/PPDQG3'PP (%)
T0 2.2 (3.3) 2.2 (3.1) 1.8 (2.5) 0.740**
T1 2.1 (5.7) 2.1 (4.2) 2.3 (3.9) 0.456**
p 0.876**** 0.868**** 0.683****
6LWHVZLWK&$/PPDQG3'PP (%)
T0 0.1 (0.4) 0.2 (0.6) 0.1 (0.4) 0.178**
T1 0.1 (0.5) 0 (0.0) 0.1 (0.3) 0.635**
p 1.000**** 0.371**** 1.000****
*Chi-squared test; **Mann-Whitney test; ***McNemar test; ****Wilcoxon test; CAL = clinical attachment level; PD = probing depth; BOP = bleeding on probing; NFG = normal fasting glucose; AFG = altered fasting glucose
DM- 2. A pr ev ious st udy29 evaluat ed t he associat ion
bet w een per iodon t it is an d t h e DM- 2 dev elopm en t
am on g w om en w it h pr ev iou s GDM. I n t h is st u dy
fr om Xiong, et al.29 ( 2013) , w om en w it h GDM and
periodont it is were only com pared wit h wom en wit hout ERWK FRQGLWLRQV DQG QR VLJQL¿FDQW GLIIHUHQFHV ZHUH found in t he m ost gly cem ic index es evaluat ed. I n
addit ion, t he st udy pr esent ed low er sam ple and shor t
follow- up per iod as w ell as it used glucose averages.
I n our under st anding, it can int er fer e w it h t he r esult s,
hinder ing t he com par ison w it h t he pr esent st udy. I n
addit ion, our r esult s did not show any im pact of t he
levels of I L- 6, I L- 10, MMP- 2, MMP- 9, and TNF-D in t he
saliva on DM- 2 or pr e- diabet es.
So m e s t u d i e s f o u n d t h a t t h e t r e a t m e n t o f
per iodont it is does not im pact t he m et abolic cont r ol of
indiv iduals w it h DM- 27,12. How ever, som e sy st em at ic
reviews and m et a- analysis11,22,24FRQ¿UPHGDEHQH¿FLDO
Variables Endocrine diagnosis p
Normal n=34 (69.4%) Pre-diabetes n=6 (12.2%)
Type 2 diabetes n=9 (18.4%)
Presence of periodontitis (%)
T0 16 (47.1) 2 (33.3) 2 (22.2) 0.451*
T1 12 (35.3) 4 (66.7) 3 (33.3) 0.316*
p 0.157*** 0.157*** 0.317***
Present teeth (±)
T0 27.3 (3.2) 28.7 (1.2) 27.4 (2.2) 0.548**
T1 26.9 (3.3) 28.3 (1.4) 27.2 (2.6) 0.626**
p 0.000**** 1.000**** 1.000****
Extension of periodontitis (%)
Localized T0 16 (47.1) 2 (33.3) 2 (22.2) 0.451**
Localized T1 11 (32.4) 4 (66.7) 2 (22.2) 0.221**
p 0.096*** 0.157*** 1.000***
Extension of periodontitis (%)
Generalized T0 0 (0.0) 0 (0.0) 0 (0.0)
Generalized T1 1 (2.9) 0 (0.0) 1 (11.1) 0.523**
p 0.317*** - 0.317***
Severity of periodontitis (%)
Moderate T0 1 (2.9) 0 (0.0) 0 (0.0) 1.000 **
Moderate T1 2 (5.9) 1 (16.7) 0 (0.0) 0.401**
p 0.563*** 0.317***
-Severity of periodontitis (%)
Advanced T0 15 (44.1) 2 (33.3) 2 (22.2) 0.547**
Advanced T1 10 (29.4) 3 (50.0) 3 (33.3) 0.647**
P 0.095*** 0.317*** 0.317***
Sites with BOP (%)
T0 22.6 (15.7) 27.6 (16.7) 20.9 (17.7) 0.646**
T1 29.8 (20.6) 42.9 (19.0) 35.6 (27.1) 0.292**
p 0.047**** 0.094**** 0.024****
6LWHVZLWK&$/PPDQG3'PP (%)
T0 2.9 (2.8) 2.6 (3.5) 2.7 (5.1) 0.590**
T1 3.7 (5.1) 4.4 (2.6) 5.1 (9.2) 0.224**
p 0.375**** 0.062**** 0.090****
6LWHVZLWK&$/PPDQG3'PP (%)
T0 2.2 (3.1) 2.5 (3.2) 1.3 (1.9) 0.776**
T1 2.1 (4.2) 3.1 (3.7) 1.8 (4.1) 0.793**
p 0.868**** 0.787**** 1.000****
6LWHVZLWK&$/PPDQG3'PP (%)
T0
T1 0.2 (0.6) 0 (0.0) 0 (0.0) 0.391**
0.1 (0.4) 0 (0.0) 0.1 (0.3) 0.191**
p 0.371**** - 1.000****
*Chi-squared test; **Kruskal-Wallis test; ***McNemar test; ****Wilcoxon test; CAL = clinical attachment level; PD = probing depth; BOP = bleeding on probing
effect of periodont al t herapy on glycem ic levels am ong
indiv iduals w it h DM- 2.
Thus, it is im port ant t o em phasize t hat t he fact t hat
t he sam ple included in our st udy pr esent s, m ost ly,
a m or e localized per iodon t it is cou ld ex plain som e
diver gences of r esult s. We can also hy pot hesize t hat
in a sam ple w it h a m or e generalized per iodont it is, FRQVHTXHQWO\ZLWKDKLJKV\VWHPLFLQÀDPPDWLRQWKH im pact on insulin r esist ance and DM- 2 developm ent
cou ld be m or e ev iden t . Alt h ou gh n ot st at ist ically VLJQL¿FDQW LQGLYLGXDOV ZLWK DOWHUHG JO\FHPLF VWDWXV pr esent ed a w or sening in per iodont al st at us bet w een
bot h exam inat ions. Findings showed an increase in t he
fr equency, ex t ension, and sever it y of per iodont it is as
w ell as in t he per cent of sit es w it h BOP, PD, and CAL.
One st udy18 evaluat ed t he effect of t oot h ext ract ion
o n g l y ce m i c co n t r o l o f i n d i v i d u a l s w i t h D M- 2 ,
dem on st r at in g t h at in div idu als u n der goin g den t al WUHDWPHQWVKRZHGDVLJQL¿FDQWUHGXFWLRQLQJO\FDWHG hem oglobin levels com par ed w it h indiv iduals w ho did
not r eceive any t r eat m ent . 7KLV¿QGLQJHPSKDVL]HV WKH SRWHQWLDO V\VWHPLF LPSDFW RI WKH LQÀDPPDWRU\ infect ious pr ocess of t he oral cav it y in t he m et abolic
cont r ol and t he developm ent of an insulin r esist ance. 6LPLODUUHVXOWVREVHUYHGIRULQÀDPPDWRU\PHGLDWRUV w er e pr ev iously descr ibed. One sy st em at ic r ev iew8
concluded t hat diabet ic and non- diabet ic indiv iduals
had sim ilar levels of I L- 6 in t he saliva, suggest ing a
lack of associat ion bet w een I L- 6 from DQLQÀDPPDWRU\
p r ocess in t h e or al cav it y an d DM- 2 . I n an ot h er
st udy, t he ex pr ession of I L- 6, I L- 10, and TNF-D in
gingival t issues was sim ilar in indiv iduals w it h and
w it hout DM- 210. Collin, et al.6 ( 2000) obser ved sim ilar
salivar y levels of MMP- 9 bet w een diabet ic and
non-diabet ic indiv iduals. Mor eov er, per iodont al t herapy
has dem onst rat ed t he abilit y t o r educe blood levels of
CRP, as w ell asLQÀDPPDWRU\ cyt okines such as I L- 6
and TNF-D23.
Fur t her m or e, w e should consider t he GLI¿FXOW\LQ
quant ify ing WKH LQÀDPPDWRU\ SURFHVV pr oduced by
per iodont it is. The DQDO\VLVRILQÀDPPDWRU\ m ediat or s
pr esent in t he saliva pr ovides a global m easur e of oral LQÀDPPDWLRQ. $OWKRXJKLQÀDPPDWRU\FHOOV pr esent in t he saliva m ainly der ive fr om t he gingival cr evicular ÀXLGcells f r om ot h er LQÀDPPDWRU\ p r ocesses of t he oral cavit y m ay be pr esent , cont r ibut ing t o t he
o v e r e st i m a t e d i n f l a m m a t i o n f r o m p e r i o d o n t i t i s.
On t he ot her hand, t he dilut ion by t he saliva m ay
under est im at e t he SHULRGRQWDOLQÀDPPDWLRQ30.
I nt er est ingly, in t he cur r ent st udy, blood levels of &53KDGVLJQL¿FDQWLPSDFWRQWKH'0GHYHORSPHQW a m o n g w o m e n w i t h a h i st o r y o f GD M. An o t h e r LQÀDPPDWRU\SURFHVV could be involved in t hese CRP levels, as w ell as ot her m ediat or s RI LQÀDPPDWLRQ,
cont r ibut ing t o t he m anifest at ion of DM- 2. This fact
m ay su ggest t h e r ole of a V\VWHPLF LQÀDPPDWRU\
pr ocess in t h e dev elopm en t of in su lin r esist an ce. 6\VWHPLF LQÀDPPDWLRQ is VLJQL¿FDQWO\ HOHYDWHG in
Variable Fasting glucose p Endocrine diagnosis p NFG AFG Normal Pre-diabetes Type 2
diabetes n=34 (69.4%) n=15 (30.6%) n=34 (69.4%) n=6 (12.2%) n=9 (18.4%)
Occurrence of periodontitis (T1–T0)
0.202* 0.339*
No T0 - No T1 16 (47.1) 8 (53.3) 16 (47.1) 2 (33.3) 6 (66.7)
No T0 - Yes T1 2 (5.9) 3 (20.0) 2 (5.9) 2 (33.3) 1 (11.1)
Yes T0 - Yes T1 10 (29.4) 4 (26.7) 10 (29.4) 2 (33.3) 2 (22.2)
Yes T0 - No T1 6 (17.6) 0 (0.0) 6 (17.6) 0 (0.0) 0 (0.0)
Mean of sites with BOP (%) (T1–T0)
7.2 (19.3) 15.0 (14.4) 0.121** 7.2 (19.3) 15.3 (17.3) 14.7 (13.3) 0.292**
6LWHVZLWK&$/PPDQG3' 4 mm (%) (T1–T0)
0.8 (4.0) 2.1 (3.5) 0.092** 0.8 (4.0) 1.8 (1.7) 2.4 (4.4) 0.224**
6LWHVZLWK&$/PPDQG3' 5-6 mm (%) (T1–T0)
- 0.1 (2.8) 0.6 (2.7) 0.532** - 0.1 (2.8) 0.7 (2.4) 0.5 (3.1) 0.793**
6LWHVZLWK&$/PPDQG3'
PPPP7±7 - 0.1 (0.2) 0.1 (0.3) 0.111** - 0.1 (0.2) 0 (0.0) 0.1 (0.3) 0.191**
*Stuart-Maxwell test; **Wilcoxon test; CAL = clinical attachment level; PD = probing depth; BOP = bleeding on probing; NFG = normal fasting glucose; AFG = altered fasting glucose
Table 5- Characteristics of the sample in relation to periodontal variables according to glycemic control and endocrine diagnosis from T0
individuals w it h DM, including high levels of CRP17,24.
A r ecen t sy st em at i c r ev i ew an d m et a- an al y si s2 6
exam ined t he associat ion EHWZHHQWKHLQÀDPPDWRU\
m ar ker s I L- 6 and CRP and t he r isk of DM- 2. Result s
show ed DVLJQL¿FDQWDVVRFLDWLRQEHWZHHQ high levels
of I L- 6 and CRP and t he r isk of DM- 2, suggest ing WKH LQÀDPPDWRU\ SURFHVV as pr edict or of t he DM- 2 developm ent26. Sim ilar ly, w om en w it h GDM pr esent ed
incr eased levels of CRP5,9. Fur t her m or e, per iodont it is
has been associat ed wit h high CRP plasm a levels14. This
fact can support t he biological plausibilit y of t he im pact
of p er iod on t al in f lam m at ion on DM- 2 . Th er ef or e,
differ ent degr ees of per iodont it is m ay have differ ent
syst em ic r eper cussions.
Th e i n ci d e n ce o f D M- 2 a m o n g w o m e n w i t h
pr ev ious GDM was 18.4% . One st udy16 show ed t hat
38.8% of w om en w it h GDM pr esent ed pr e- diabet es
and 6.6% pr esent ed DM- 2 in a per iod of 5.5 year s.
The sy st em at ic r ev iew by Kim , New t on and Knopp19
( 2002) show ed a gr eat var iat ion in t he incidence of
DM- 2 am ong w om en w it h hist or y of GDM, fr om 2.6%
t o 70% . This gr eat var iabilit y could be ex plained by
differ ences in t he follow- up per iod, in t he diagnost ic
cr it er ia for GDM, and in t he sam ple select ion.
Elev at ed BMI w as sig n if ican t ly m or e f r eq u en t
am ong w om en w it h alt er ed glycem ic levels, eit her
diagnosed w it h pr e- diabet es or DM- 2, alt hough it not UHPDLQHGVLJQL¿FDQWLQWKHPXOWLYDULDWH¿QDOPRGHO. Obesit y has been consider ed a r isk fact or for DM- 2
developm ent2. St udies invest igat ing t he associat ion
bet ween periodont it is and GDM have dem onst rat ed an
elevat ed BMI associat ed w it h GDM4,5,9,13,28. Mor eover,
obesit y has been associat ed w it h per iodont it is21.
I n t he pr esent st udy, incr eased age show ed no
im pact on t he developm ent of DM- 2 am ong w om en
w it h GDM. I ncr eased age has been consider ed a r isk
fact or for GDM13. I n addit ion, it was also dem onst rat ed
t hat t he pr evalence of DM- 2 incr eased w it h age2. The
hist or y of GDM com m on t o all indiv iduals included
in t he pr esent st udy m ay be a possible ex planat ion IRUDJHQRWVKRZLQJDVLJQL¿FDQWGLIIHUHQFHEHWZHHQ gr oups. Sam ple size could be consider ed a lim it at ion
of t he pr esent st udy t hat m ay have cont r ibut ed t o WKLV¿QGLQJ
Loss of par t icipan t s du e t o n on locat ion , n on
-answ er,or non- adher ence could also be consider ed a
lim it at ion of t he pr esent st udy. Fr om t he 90 w om en
en r olled in t h e in it ial sam p le, 4 9 com p let ed t h e
pr esent st udy. The sm aller sam ple due t o t he loss is a
lim it at ion; how ever, longit udinally, t he r esult s m ay be
an im por t ant point of init ial infor m at ion on t his issue,
and t hus dir ect ing fut ur e st udies.
The per iod of t hr ee year s follow- up aft er deliver y
for w om en w it h GDM is com pat ible accor ding t o t he
Am er ican Diab et es Associat ion2. How ev er, f u t u r e
st udies m ay include longer per iods of m onit or ing t o FKHFNWKLVSRVVLEOHLQÀXHQFH
I n t he pr esent st udy, t her e was not any im pact
of per iodon t it is on t h e DM- 2 dev elopm en t am on g
w om en w it h pr ev ious GDM. How ev er, t he num ber
of st udies on t his subj ect is r educed. I t is possible
t hat , in ot her populat ions w it h differ ent per iodont al
condit ions, per iodont it is m ay dem onst rat e im pact on
DM- 2 developm ent am ong wom en wit h previous GDM.
Ther efor e, addit ional st udies on differ ent populat ions
ar e necessar y t o bet t er under st and t he r elat ionship
bet w een t hese t w o condit ions.
The im pr ovem ent of t he k now ledge about GDM
is im por t ant , since t his condit ion can be consider ed
a unique oppor t unit y for a pr event ive int er vent ion
in r elat ion t o DM- 2, a condit ion w it h high m or bidit y
and m or t alit y. The incidence of DM- 2 am ong w om en
w it h pr ev ious GDM obser ved in t he pr esent st udy was KLJKZKDWMXVWL¿HVWKHHIIRUWVGLUHFWHGWRZDUGVWKH LGHQWL¿FDWLRQRIWKHSRWHQWLDODVVRFLDWHGULVNIDFWRUV
Conclusion
The observed im pact of CRP on DM- 2 developm ent
am ong wom en wit h a hist ory of GDM dem onst rat es t hat
dur ing t he pr enat al m onit or ing per iod, it is necessar y
t o em phasize t he m ult idisciplinar y appr oach for t he
diagnosis and t r eat m ent of V\VWHPLF LQÀDPPDWRU\
p r ocesses, m in im izin g t h e r isk f or d ev elop in g an
insulin r esist ance. UQFHUWDLQWLHVDERXWWKHLQÀXHQFH
of per iodont it is in t he developm ent of DM- 2 am ong
wom en wit h previous GDM do exist , signaling t he need
for addit ional st udies.
Refer ences
1- Albandar JM. Global r isk fact or s and r isk indicat or s for per iodont al
diseases. Per iodont ol 2000. 2002; 29: 177- 206.
$PHULFDQ 'LDEHWHV $VVRFLDWLRQ 'LDJQRVLV DQG FODVVL¿FDWLRQ RI
diabet es m ellit us. Diabet es Car e. 2014; 37: S81- 90.
$UPLWDJH*&'HYHORSPHQWRIDFODVVL¿FDWLRQV\VWHPIRUSHULRGRQWDO
diseases and condit ions. Ann Per iodont ol. 1999; 4: 1- 6.
4- Bullon P, Jaram illo R, Sant os- Gar cia R, Rios- Sant os V, Ram ir ez M,
Fer nandez- Palacin A, et al. Relat ion of per iodont it is and m et abolic
syndr om e w it h gest at ional glucose m et abolism disor der. J Per iodont ol.
5 - Ch ok w ir iy ach it A, Dasan ay ak e AP, Su w an n ar on g W, Hor m dee
D, Su m an on t a G, Pr aser t ch ar eon su k W, et al. Per iod on t it is an d
gest at ional diabet es m ellit us in non- sm ok ing fem ales. J Per iodont ol.
2013; 84: 857- 62.
6- Collin HL, Sor sa T, Meur m an JH, Nisk anen L, Salo T, Rönk ä H, et al.
Salivary m at rix m et alloprot einase ( 8) levels and gelat inase (
MMP-9) act iv it ies in pat ient s w it h t y pe 2 diabet es m ellit us. J Per iodont al
Res. 2000; 35: 259- 65.
7- Cor r ea FO, Gonçalves D, Figuer edo CM, Bast os AS, Gust afsson
A, Or r ico SR. Effect of per iodont al t r eat m ent on m et abolic cont r ol,
V\VWHPLFLQÀDPPDWLRQDQGF\WRNLQHVLQSDWLHQWVZLWKW\SHGLDEHWHV
J Clin Per iodont ol. 2010; 37: 53- 8.
8- Cost a PP, Tr ev isan GL, Macedo GO, Paliot o DB, Souza SL, Gr isi
MF, et al. Salivar y int er leuk in- 6 , m at r ix m et allopr ot einase- 8 , and
o st eo p r o t eg er i n i n p a t i en t s w i t h p er i o d o n t i t i s a n d d i a b et es. J
Per iodont ol. 2010; 81: 384- 91.
9- Dasanayake AP, Chhun N, Tanner ACR, Craig RG, Lee MJ, Moor e AF,
et al. Per iodont al pat hogens and gest at ional diabet es m ellit us. J Dent
Res. 2008; 87: 328- 33.
10- Duar t e PM, Miranda TS, Lim a JA, Dias Gonçalves TE, Sant os VR,
%DVWRV0)HWDO([SUHVVLRQRILPPXQHLQÀDPPDWRU\PDUNHUVLQVLWHV
of chr onic per iodont it is in pat ient s w it h t y pe 2 diabet es. J Per iodont ol.
2012; 83: 426- 34.
11- Engebr et son S, Kocher T. Ev idence t hat per iodont al t r eat m ent
im pr oves diabet es out com es: a sy st em at ic r ev iew and m et a- analy sis.
J Per iodont ol. 2013; 84: S53- 69.
12- Engebret son SP, Hym an LG, Michalowicz BS, Schoenfeld ER, Gelat o
MC, Hou W, et al. The effect of nonsur gical per iodont al t herapy on
hem oglobin A1C levels in per sons w it h t y pe 2 diabet es and chr onic
per iodont it is: a random ized clinical t r ial. JAMA. 2013; 310: 2523- 32.
13- Est eves Lim a RP, Miranda Cot a LO, Cost a FO. Associat ion bet w een
per iodont it is and gest at ional diabet es m ellit us: a case- cont r ol st udy. J
Per iodont ol. 2013; 84: 1257- 65.
14- Gom es- Filho I S, Fr eit as Coelho JM, Cr uz SS, Passos JS, Teixeira de
Freit as CO, Aragão Farias NS, et al. Chronic periodont it is and C- react ive
pr ot ein levels. J Per iodont ol. 2011; 82: 969- 78.
1 5 - Gom es- Filh o I S, Cr u z SS, Rezen de EJ, San t os CA, Soledade
KR, Magalhães MA, et al. Ex posur e m easur em ent in t he associat ion
bet w een per iodont al disease and pr em at ur it y / low bir t h w eight . J Clin
Per iodont ol. 2007; 34: 957- 63.
1 6 - Hu m m el S, Mu ch D, Rossbau er M, Z iegler AG, Bey er lein A.
Post par t um out com es in w om en w it h gest at ional diabet es and t heir
RIIVSULQJ32*2VWXG\GHVLJQDQG¿UVW\HDUUHVXOWV5HY'LDEHW6WXG
2013; 10: 49- 57.
17- I shikawa M, Yoshida K, Okam ura H, Ochiai K, Takam ura H, Fuj iwara
N, et al. Oral Por phyr om onas gingivalis t ranslocat es t o t he liver and
UHJXODWHVKHSDWLFJO\FRJHQV\QWKHVLVWKURXJKWKH$NW*6.ǃVLJQDOLQJ
pat hway. Biochim Biophy s Act a. 2013; 1832: 2035- 43.
18- Khader YS, Al Habashneh R, Al Malalheh M, Bat aineh A. The effect
of full- m out h t oot h ex t ract ion on glycem ic cont r ol am ong pat ient s
w it h t y pe 2 diabet es r equir ing ex t ract ion of all r em aining t eet h: a
random ized clinical t r ial. J Per iodont ol. 2010; 45: 741- 7.
1 9 - Kim C, New t on KM, Knopp RH. Gest at ional diabet es and t he
incidence of t y pe 2 diabet es: a sy st em at ic r ev iew. Diabet es Car e.
2002; 25: 1862- 8.
20- Ndr epepa G, Braun S, Cassese S, Fusar o M, King L, Kast rat i A, et
al. C- r eact ive pr ot ein and pr ognosis in w om en and m en w it h cor onar y
ar t er y disease aft er per cut aneous cor onar y int er vent ion. Car diovasc
Revasc Med. 2013; 14: 264- 9.
21- Pat ar o AL, Cost a FO, Cor t elli SC, Cor t elli JR, Dupim Souza AC,
1RJXHLUD*XLPDUmHV$EUHX0+HWDO,QÀXHQFHRIREHVLW\DQGEDULDWULF
sur ger y on t he per iodont al condit ion. J Per iodont ol. 2012; 83: 257- 66.
2 2 - Sg olast r a F, Sev er in o M, Piet r op aoli D, Gat t o R, Mon aco A.
Effect iveness of per iodont al t r eat m ent t o im pr ove m et abolic cont r ol in
pat ient s wit h chronic periodont it is and t ype 2 diabet es: a m et a- analysis
of random ized clinical t r ials. J Per iodont ol. 2013; 84: 958- 73.
6XQ:/&KHQ//=KDQJ6=:X<05HQ<=4LQ*0,QÀDPPDWRU\
cy t ok ines, adiponect in, insulin r esist ance and m et abolic cont r ol aft er
per iodont al int er vent ion in pat ient s w it h t y pe 2 diabet es and chr onic
per iodont it is. I nt er n Med. 2011; 50: 1569- 74.
24- Teeuw WJ, Ger des VEA, Loos BG. Effect of per iodont al t r eat m ent
on glycem ic cont rol of diabet ic pat ient s: a syst em at ic review and m et
a-analy sis. Diabet es Car e. 2010; 33: 421- 7.
2 5 - Tom ar SL, Asm a S. Sm ok ing- at t r ibut able per iodont it is in t he
8QLWHG6WDWHV¿QGLQJVIURP1+$1(6,,,1DWLRQDO+HDOWKDQG1XWULWLRQ
Ex am inat ion Sur vey. J Per iodont ol. 2000; 71: 743- 51.
2 6 - Wan g X, Bao W, Liu J, Ou y an g YY, Wan g D, Ron g S, et al.
,QÀDPPDWRU\ PDUNHUV DQG ULVN RI W\SH GLDEHWHV 'LDEHWHV &DUH
2013; 36: 166- 75.
27- Wor ld Healt h Or ganizat ion - WHO. The pr oblem of over w eight
and obesit y. Obesit y : pr event ing and m anaging t he global epidem ic.
I n: ______. WHO t echnical r epor t ser ies num ber 894. Geneva: WHO;
2000. p. 5- 15.
28- Xiong X, Elk ind- Hir sch KE, Vast ar dis S, Delar osa RL, Pr idj ian G,
Buekens P. Per iodont al disease is associat ed w it h gest at ional diabet es
m ellit us: a case- cont r ol st udy. J Per iodont ol. 2009; 80: 1742- 9.
29- Xiong X, Elkind- Hirsch KE, Xie Y, Delarosa RL, Maney P, Pridj ian G, et
al. Per iodont al disease as a pot ent ial r isk fact or for t he developm ent of
diabet es in w om en w it h a pr ior hist or y of gest at ional diabet es m ellit us.
J Public Healt h Dent . 2013; 73: 41- 9.
<RRQ$-&KHQJ%3KLOLSRQH(7XUQHU5/DPVWHU,%,QÀDPPDWRU\
biom ar ker s in saliva: assessing t he st r engt h of associat ion of diabet es