1
Sc.M. in Nursing Sciences, Full t im e Professor, Universit y Aut ónom a de Cd. Juárez, Chihuahua, e- m ail: lindaguerra@hot m ail.com ; 2 PhD, Full Professor, School of Nursing, Universit y Aut ónom a de Nuevo León, Mexico, e- m ail: egallego@fe.uanl.m x; 3 PhD, Prim ary Researcher, Genet ics Division, Nort heast Cent er of Biom edical Research, Mexican Social Securit y I nst it ut e, Mexico, e- m ail: ricardocerda_m x@yahoo.com .m x
Disponible en castellano/ Disponível em língua portuguesa SciELO Brasil w w w .scielo.br/ rlae
LI FESTYLE CHANGES I N DESCENDANTS OF PARENTS W I TH DI ABETES TYPE 2
Rosalin da Gu er r a- Ju ár ez1 Est her C. Gallegos2 Ricar do M. Cer da- Flor es3
Gu er r a- Ju ár ez R, Gallegos EC, Cer da- Flor es RM. Lif est y le ch an ges in descen dan t s of par en t s w it h diabet es t y pe 2. Rev Lat ino- am Enfer m agem 2007 set em br o- out ubr o; 15( 5) : 909- 13.
This st udy aim ed t o ex plor e t he disposit ion of diabet ic par ent s’ descendent s in changing eat ing and physical act ivit y pat t erns. I t was based on t he herit abilit y concept and Prochaska’s Transt heoret ical Model. This is a d escr ip t iv e- cor r elat ion al st u d y ; p ar t icip an t s in clu d ed 3 0 p ar en t s, r an d om ly select ed , an d 6 0 ch ild r en . Result s and conclusion: 68% of t he children was classified as obese, 42% wit h insulin resist ance, and 15% wit h car bohy dr at e int oler ance. None of t he r isk fact or s w as associat ed w it h t he st ages of change. The her it abilit y fact or was 1.37% ; m ore people younger t han 40 and wom en report decreasing in t he consum pt ion of fat food (
χ
i2 = 6.04, p = .020; and 4.41, p = .040, respect ively) . These result s suggest a high influence of environm ent al fact or s on t he par t icipant s’ unhealt hy life st y les.DESCRI PTORS: healt h behav ior ; env ir onm ent ; her edit y
CAMBI O EN LOS PATRONES DE VI DA EN DESCENDI ENTES DE PROGENI TORES CON
DI ABETES MELLI TUS TI PO 2 DEL NORESTE DE MEXI CO
El obj et ivo general del est udio fue explorar la disposición al cam bio de pat rones alim ent arios y act ividad física en descendient es de pr ogenit or es con diabet es m ellit us t ipo 2 ( DMT2) , aplicando un diseño descr ipt iv o correlacional. La base t eórica la const it uyó el com ponent e genét ico heredabilidad ( h2) y el Modelo Transt eorét ico de Prochaska; part iciparon 30 progenit ores con DMT2 y 60 descendient es. Result ados y Conclusión: El 68% de los descen dien t es f u er on obesos, 6 0 % con r iesgo de en f er m edad car diov ascu lar , 4 2 % con r esist en cia a la insulina ( RI ) y 15% int oler ant es a la glucosa; ninguno de los fact or es de r iesgo se asoció con las et apas de cam bio. El com ponent e genét ico par a RI fue m ínim o ( h2 = 1.37% ) . Una m ay or pr opor ción de m enor es de 40 añ os ( p = . 0 2 0 ) y de m u j er es “ con t em plan ” dism in u ir el con su m o de gr asas ( p = . 0 4 0 ) . Est os r esu lt ados sugier en un m ay or peso de fact or es del m edio am bient e sobr e el est ilo de v ida nociv o de los par t icipant es.
DESCRI PTORES: conduct a de salud; m edio am bient e; her encia
MUDANÇA EM OS PADRÕES DE VI DA EM DESCENDENTES DE PROGENI TORES COM
DI ABETES MELLI TUS TI PO 2 DO NORDESTE DO MEXI CO
O obj et iv o ger al do est udo foi ex plor ar à disposição à m udança dos padr ões alim ent ar es e at iv idade física nos descendent es de progenit ores com diabet es m ellit us t ipo 2 ( DMT2) . Aplicou- se un desenho descrit ivo correlacionar. A base t eórica const it uiu- se pelo Com ponent e Genét ico ( h2) e o Modelo Transt eorét ico de Prochaska. Part iciparam 30 progenit ores com DMT2 e 60 descendent es. Result ados e Conclusões: O 68% dos descendent es present aram obesidade, 60% com risco de doença cardiovascular, 42% com resist ência à insulina ( RI ) e 15% int olerância à glucose; nenhum dos fat ores de risco associaram - se com as et apas de m udança. O com ponent e genét ico par a RI foi m ínim o ( h2 = 1.37% ) . Um a m aior pr opor cão dos m enor es de 40 anos (
χ
i2 = 6.04, p = .020) e das m ulheres (χ
i2 = 4.41, p= .040) cont em plam dim inuir o consum o de gorduras. Os result ados sugerem um m aior peso dos fat or es do m eio am bient e sobr e o est ilo de v ida nociv o dos par t icipant es.I NTRODUCTI ON
T
ype 2 diabet es m ellit us ( DMT2) is a com plexd i se a se . Ge n e t i c a n d e n v i r o n m e n t a l co m p o n e n t s
int eract in it s developm ent . Different aut hors indicat e
t h at t h e en v ir on m en t al com pon en t ex er t s a gr eat er
w eigh t in t h e h igh pr ev alen ce r at es of t h is disease
n o w a d a y s . Th e t w o m a i n c o m p o n e n t s o f t h e
en v ir on m en t t h at r epr esen t t h e h igh est r isk for t h e
p o p u l a t i o n ’ s h e a l t h a r e f o u l e a t i n g h a b i t s a n d
decreased physical act ivit y. These conduct s const it ut e
living habit s t hat need subst ant ial m odificat ion in people
suffering from or running t he risk of DMT2( 1).
Urban fam ilies’ food is charact erized by highly
ener get ic it em s, r ich in fat s and sugar s and poor in
f i b e r s , f r u i t a n d v e g e t a b l e s . M o r e o v e r, t h e
ch a r a ct e r i st i cs o f u r b a n l i f e p r a ct i ca l l y i m p o se a
sedent ar y lifest yle on it s inhabit ant s, avoiding w alks,
s p o r t s a n d m a k i n g l e s s e f f o r t f o r w o r k a n d
h ou sew or k( 2 ).
DMT2 is diagnosed earlier and earlier and, in
m any cases, in indiv iduals w hose close r elat iv es ar e
diabet ic( 3). Healt h sy st em offer t he m eans t o cont r ol
adult s wit h t his disease, but few effort s and resources
ar e av ailable t o at t en d t o t h eir descen dan t s, w h ich
per def in it ion ar e at r isk of dev elopin g t h is ch r on ic
d i sease.
Lit er at ur e show s t hat , in m or e t han 50% of
adult s wit h DMT2, glucose levels are m uch higher t han
r ecom m en d ed or ex p ect ed lev els. I f t h ey f ollow ed
t he prescribed t reat m ent st rict ly, including a balanced
d iet w it h con t r ol of calor ie in g est ion an d su f f icien t
p h y si ca l a ct i v i t y, a b a l a n ce co u l d b e m a i n t a i n e d
b e t w e e n ca l o r i e i n t a k e a n d co n su m p t i o n( 4 ). Th i s
in for m at ion su ggest s t h at n eit h er adu lt s w it h DMT2
n o r t h ei r f am i l i es h av e m o d i f i ed t h ei r eat i n g an d
p h y si ca l a ct i v i t y h a b i t s, w h i ch e x p l a i n s t h e b a d
m et abolic cont rol and show s, m oreover, t he high risk
t h ei r d i r ect r el at i v es ar e r u n n i n g , esp eci al l y t h ei r
d e s c e n d a n t s , o f d e v e l o p i n g D M T2 o r a n o t h e r
associat ed disease( 3 ).
Be s i d e s t h i s f a c t , t h e r e i s a n i m p o r t a n t
incr ease in t he pr evalence of obesit y and over w eight
in sam ples of adult s as well as young people and school
children, t o t he ext ent t hat t his is already considered
a public healt h pr oblem( 3- 4). Obesit y has r ev ealed t o
be one of t he m ost relevant fact ors in insulin resist ance
( I R) disor der s, w h ich pr ecede t h e clear appear an ce
of DMT2( 5 ). Ther efor e, if dir ect r elat iv es of an adult
w it h DMT2 ar e also obese or ov er w eight , t he r isk of
developing t he disease is higher( 6). On t he ot her hand,
t her e ex ist s ev idence about t he pr ev ent ion of DMT2
by incorporat ing changes in eat ing and in t he physical
act iv it y lev el( 7 ). How ev er, in div idu als at r isk sh ou ld
know t hat t hey are facing an act ual risk and be willing
t o change t he conduct s t hat favor and increm ent t he
risk of get t ing ill.
I n Me x i c o , t h e r e a r e f e w s t u d i e s a b o u t
w h et h er t h e d i r ect r el at i v es o f p eo p l e w i t h D MT2
c o n s i d e r t h e m s e l v e s a t r i s k a n d t a k e s p e c i f i c
pr ev en t ion m easu r es. I n gen er al, t h e m ost st u died
t hem es ar e t he fam ilies’ suppor t t o t he per son w it h
DMT2, wit h a view t o following t he recom m ended diet
and exercises as a part of t reat m ent( 8). However, t hey
report on a negat ive at t it ude by t he fam ily in t he sense
of solidarit y wit h adult pat ient s who suffer from DMT2
i n t h e o b s e r v a n c e o f a b a l a n c e d d i e t a n d
accom panim ent t o increase physical act ivit y. Moreover,
on ly on e st u dy w as locat ed t h at in qu ir ed abou t t h e
c h a n g e p h a s e s i n p a t i e n t s w i t h D M T2 , i n t h e
m odificat ion of fat and v eget able consum pt ion( 9).
Th is r esear ch w as b ased on t w o con cep t s.
Fir st , in h er it ab ilit y ( h2) , w h ich is t h e p r op or t ion of
v a r i a n ce i n a p h e n o t y p e t h a t ca n b e e x cl u si v e l y
at t r ibut ed t o t he effect of genes. Est im at ing h2 is an
essent ial phase befor e t r ying t o locat e t he genes as,
if t he phenot ype has no or a very low h2 ( lower t han
10% for exam ple) , t he search for genes has not been
u sed b ecau se t h e en v ir on m en t al com p on en t w ou ld
have a great er cont ribut ion. Fact ors like t he Body Mass
I ndex ( BMI ) , Waist - Hip Rat io ( WHR) , cholest er ol and
t r igly cer ides h av e been r epor t ed w it h sign if ican t h2
lev els in f ir st , secon d an d t h ir d- degr ee r elat iv es in
Mex i ca n f a m i l i es( 1 0 ). Al t h o u g h w e n e i t h e r h a d a n
a d e q u a t e sa m p l e n o r a b r o a d d e si g n o f n u cl e a r
f a m i l i es t o a ssess t h e g en et i c co m p o n en t ( w h i ch
decr eases t h e st u dy ’s st at ist ical pow er ) , it seem ed
int erest ing t o us t o assess t he h2 of insulin resist ance
( I R) am ong parent s wit h DMT2 and t heir descendant s,
in or der t o est im at e t h e en v ir on m en t al con t r ibu t ion
( 1- h2) .
We a d o p t e d Pr o ch a sk a ’s Tr a n st h e o r e t i ca l
Model, which explains t he willingness t o change( 11). This
m odel considers t hat changing behaviors is a gradual
process t hat involves five phases: a) Precont em plat ion,
in w hich indiv iduals hav e no int ent t o change in t he
near fut ure; b) Cont em plat ion, when individuals int end
t o change wit hin t he next six m ont hs; c) Preparat ion,
when individuals are ready t o change in t he near fut
ch an ges t h eir lif est y les, at least du r in g t h e last six
m ont hs; y e) Maint enance, when individuals have fait h
i n t h e c h a n g e s t h e y h a v e m a d e a n d h a v e l e s s
probabilit y of relapse t o unwant ed behavior.
Wit h a v iew t o obt aining gr eat er k now ledge
ab ou t t h e p h en om en on of w illin g n ess t o ch an g e in
adult s at r isk of dev eloping DMT2, t his st udy aim ed
t o explore t he willingness t o change healt h conduct s,
specif ically in eat in g an d ph y sical ex er cise pat t er n s
in descendant s of par ent s diagnosed w it h DMT2 and
it s associat ion w it h som e r isk fact or s.
I n v iew of t h e ab ov e, t h is st u d y ’s sp ecif ic
obj ect iv es w er e: 1 .- Calcu lat e t h e h er edit ar y - gen et ic
and environm ent al com ponent of I R in t his sam ple of
par en t s- descen dan t s. 2 .- Det er m in e t h e pr evalen ce
of I R and glucose int oler ance ( GI ) in descendant s of
DMT2 pat ient s and 3.- Associat e t he change phases in
f a t co n su m p t i o n a n d ex er ci se ( Pr eco n t em p l a t i o n ,
Cont em plat ion, Act ion and Maint enance) wit h four risk
fact ors ( BMI , WHR, I R and GI ) in descendant s of DMT2
pat ien t s.
METHODS
Th e st u d y d e si g n w a s o b se r v a t i o n a l a n d
descr ipt iv e. Th e popu lat ion of in t er est con sist ed of
subj ect s w ho had at least one parent diagnosed w it h
D M T2 , m e d i c a l l y c o n t r o l l e d t h r o u g h o u t p a t i e n t
t r eat m ent at a fir st - lev el social secur it y inst it ut ion in
t h e Met r op olit an Ar ea of Mon t er r ey ( AMM) , Nu ev o
León, Mex ico. This is t he count r y ’s second indust r ial
zon e, locat ed in t h e Nor t h east of Mex ico, w it h an
im m igrant populat ion of 80% of people from t he st at es
of Tam aulipas, Coahuila, San Luís Pot osí, Zacat ecas,
Du r an go, Veracr u z an d Ch ih u ah u a.
Th e r esear ch p r oj ect w as ap p r ov ed b y t h e
I nst it ut ional Review Board at t he School of Nursing of
t he Univ er sidad Aut ónom a de Nuev o León.
Test subj ect s ( fat her or m ot her w it h DMT2 )
w ere select ed at random : based on t he updat ed list s
of 2 2 clin ics, a p at ien t w as select ed . Th e select ed
par en t sh ou ld h av e descen dan t s of 1 0 y ear s old or
older, excluding t hose alr eady diagnosed w it h DMT2.
The sam ple size was 100 subj ect s, wit h an est im at ed
error of ± .09, 95% CI , p = 0.5 ( conservat ive focus)
for an associat ion t est . Fast ing capillary glucose levels
> 1 2 6 m gs/ dl or post - ch ar ge lev els ≥ 2 0 0 m gs/ dl
w er e d et er m i n ed as an ex cl u si o n cr i t er i o n , w h i ch
elim inat ed four subj ect s.
Me a su r e m e n t s. Tw o q u e st i o n n a i r e s w e r e
applied: a) Ex er cise- Ch an ge Ph ases Sh or t For m( 1 2 ),
which m easures t he willingness t o change in exercise
pat t er n s t h r ou gh f iv e qu est ion s abou t t h e in t en t t o
e x e r ci se , cu r r e n t o r p a st e x e r ci si n g . D i ch o t o m i c
answers ( T/ F) perm it t ed ranking t he subj ect in one of
t he five change phases according t o Prochaska and b)
Fat Consum pt ion- Change Phases Short Form , wit h four
dich ot om ic- r espon se qu est ion s, w h ich m easu r es t h e
willingness t o change t he consum pt ion of fat t y foods;
according t o t he answ ers, part icipant s w ere classified
in one of t he four change phases ( pr econt em plat ion,
cont em plat ion, act ion or m aint enance) .
Th e p a r t i ci p a n t s’ w e i g h t a n d h e i g h t w a s
regist ered in ordered t o calculat e t heir BMI , using t he
form ula: Weight / height2, in funct ion of which t hey were
classif ied as n or m al w eigh t , ov er w eigh t an d obese,
according t o crit eria by t he Official Mexican St andard
for I nt egral Managem ent of Obesit y( 13). The w aist - hip
r at io w as det er m ined and subj ect s w er e classified as
i n cr eased r i sk an d su b st an t i al l y i n cr eased r i sk o f
obesit y, accor ding t o gender.
I n t h e t e s t s u b j e c t s ’ d e s c e n d a n t s ,
n o r m o g l y c e m i a a n d g l u c o s e i n t o l e r a n c e w e r e
det erm ined, as well as an at t em pt t o diagnose DMT2
t hr ough a pr e and post - char ge glucose t est w it h 75
m gs. Th e color im et r ic r eact ion t ech n iqu e in plasm a
w as ap p l i ed , u si n g a Vi t r o s DT I I Sy st em d ev i ce.
Mor eov er, b lood in su lin w as d et er m in ed , u sin g t h e
en zy m e- im m u n oassay m et h od of m icr o- p ar t icles in
ser um w it h an I M X Sy st em dev ice. I n t he par ent s,
one single blood sam ple was t aken t o det erm ine glucose
and insulin levels. I n parent s and descendant s, I R was
calculat ed, using t he form ula HOMA I R= fast ing insulin
( U/ m l) x fast ing glucose ( m g/ dl) / 4 5 , consider ing I R
when t he coefficient was ≥ 3.5( 14).
To calculat e t he her it abilit y of I R, t he SAGE
( FCOR) package v4.6 w as used( 15). St at ist ical Package
for t he Social Sciences ( SPSS) v er sion 11 w as used
for dat a analy sis. Kolm ogor ov - Sm ir nov ’s t est show ed
t h at t h e con t in u ou s v ar iab les ad ap t ed t o a n or m al
d ist r ib u t ion . Ch i- sq u ar e st at ist ics w as u sed t o look
for associat ion s. A pr obabilit y lev el u n der 0 . 0 5 w as
con sider ed sign if ican t .
RESULTS
Th e sa m p l e co n si st e d o f 6 0 p a r t i ci p a n t s,
diagnosed with DMT2. The m ean age was 34 years (SD
= 9; 13- 63) and 58% were wom en. The m ean num ber
of years of form al education was 11.63 (SD = 3.38;
4-2 0 ) ; m ost p ar en t s ( 4 5 % ) in d icat ed t h at t h ey w er e
em ployed and 60% lived with a partner. Fifty- six percent
of this sam ple adm itted having at least one grandparent
with DMT2, 78% uncles on their father’s side and 59%
on t heir m ot her’s side. Sevent y- t wo percent m ent ioned
that they did not practice any sports.
On l y 1 5 % o f t h e 6 0 d e s c e n d a n t s
d em on st r at ed a BMI w it h in n or m al lev els( 1 3 ); w h ile
6 8 % pr esen t ed obesit y an d 1 7 % ov er w eigh t . Six t y
p e r ce n t w a s cl a ssi f i e d a s a t i n cr e a se d r i sk o f a
cer eb r o v ascu l ar ev en t ( CVE) . Based o n t h e WHR,
using t he m ost direct indicat ors of m et abolic disease,
42% of t he sam ple of descendant s w as ident ified as
h av in g I R, an d 1 5 % ob t ain ed p ost - ch ar g e g lu cose
lev els t hat r ank t hem as glucose int oler ant .
As t o t he parent s, 30 persons wit h a m edical
diagnosis of DMT2 w er e st udied; t his gr oup included
t hree couples in which bot h part ners had DMT2. Hence,
d escen d an t s w er e r ecr u it ed f r om 2 7 f am ilies. Th e
par ent s’ m ean age w as 62 y ear s (SD = 8; 47 - 80)
and w om en pr edom inat ed ( 67% ) .
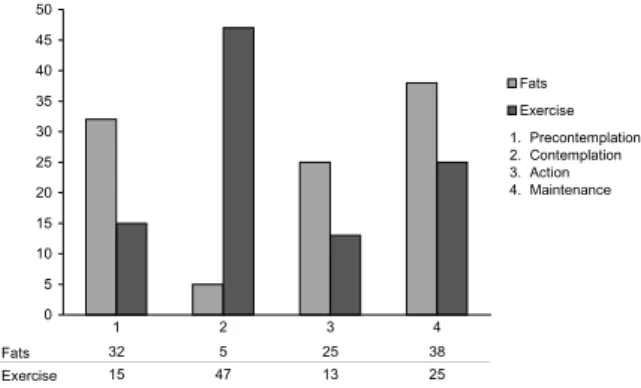
W i l l i n g n e ss t o ch a n g e i n d e sce n d a n t s o f
people w it h DMT2. Figur e 1 pr esent s t he dist r ibut ion
of par t icipant s accor ding t o t he change phase in fat
con su m p t ion an d ex er cise. Th e h ig h est p er cen t ag e
i n t e r m s o f f a t c o n s u m p t i o n i s f o u n d i n t h e
m aint enance phase, followed by t he precont em plat ion
p h a se . W h a t e x e r ci se i s co n ce r n e d , t h e h i g h e st
per cen t ages ar e f ou n d in t h e con t em plat ion ph ase,
follow ed by t he m aint enance phase.
t h e en v ir on m en t al com p on en t w as r esp on sib le f or 98. 63% . For t y - t w o per cent of t he descendant s w er e
insulin resist ant , as shown in Figure 2. Moreover, 15% pr esen t ed glu cose in t oler an ce.
0 5 10 15 20 25 30 35 40 45 50 Fats Exercise
Fats 32 5 25 38 Exercise 15 47 13 25
1 2 3 4
1. Precontemplation 2. Contemplation 3. Action 4. Maintenance
Figure 1 - Dist ribut ion of part icipant s in change phases:
consum pt ion of gat s and ex er cise
Th e g en et ic com p on en t of I R, assessed b y
calculat ing her it abilit y, cor r esponded t o 1.37% , w hile
0 10 20 30 40 50 60 70 Parents Children Resistant Non Resistant
Figur e 2 - Pr opor t ion of Resist ant and Non- Resist ant
Par en t s an d Ch ildr en
When looking for t he associat ion bet ween t he
r isk fact or s BMI , WHR, I R and GI in descendant s of p ar en t s w it h DMT2 , w it h t h e ch an g e p h ases in f at
consum pt ion and exercise, using X2 st at ist ics wit h t he
pr ev iou s dich ot om izat ion of each v ar iables in t o t h e cat egories accept able and non accept able. The result s
were not significant , as shown in Table 1.
Table 1 - Associat ion bet ween risk fact ors and change
phases in fat consum pt ion and ex er cise
s r o t c a f k s i R s e s a h p e g n a h C n o i t p m u s n o C t a
F Exercise
c
cccci2 P-Value ccccci2 P-Value
I M
B 1.43 .290 0.69 0.48 R
H
W 2.34 .174 0.01 0.56 e c n a t s i s e
R 0.40 .590 0.09 0.79 e c n a r e l o
T 0.27 .710 0.16 0.72
When associat ed w it h t he change phases in
fat con su m pt ion , gen der an d age sh ow ed st at ist ical s i g n i f i c a n c e , w h i c h i n d i c a t e s t h a t w o m e n a r e “ cont em plat ing” t he possibilit y of decr easing t heir fat
consum pt ion [
χ
i2( 1, n= 60) = 4.41, p= .04] . On t he ot herhand, descendant s y ounger t han 40 ar e av oiding fat
c o n s u m p t i o n a n d k e e p u p t h i s c o n d u c t [
χ
i2 ( 1 ,n= 60) = 6. 04, p= . 020] .
DI SCUSSI ON
An im por t ant per cent age of t he par t icipant s
con su m p t ion in t h eir f ood an d an ev en lar g er p ar t
h ad n o in t en t ( pr econ t em plat ion ) or in t en ded t o do
som et h in g ab ou t ( con t em p lat ion ) ex er cisin g in t h e
nex t six m ont hs.
A ch an ge in t h is sam ple’s diet , par t icu lar ly
i n t h e i r f a t c o n s u m p t i o n , a n d i n t h e i r p h y s i c a l
ex er cise pat t er n w ou ld be a st r at egy t h at h elps t o
delay DMT2, as som e aut hor s hav e dem onst r at ed( 7).
Balancing calor ie ingest ion and spending is t he best
com binat ion t o m anage ex cess body w eight ; in t ur n,
losing w eight is one fact or t hat can decr ease v iscer al
f a t a n d e v e n t u a l l y d e c r e a s e I R a t h e p a t i c a n d
m u s c u l a r l e v e l . H o w e v e r, a b o u t h a l f o f t h e
descendant s of par ent s w it h DMT2 w ho par t icipat ed
in t his r esear ch did not seem t o consider t his change
as n ecessar y f or t h em .
Wh en an aly zin g t h e p r esen ce of ot h er r isk
fact or s besides t he fact of being a dir ect descendant
of on e ( or bot h ) par en t ( s) w it h DMT2 , a v er y h igh
n u m ber of descen dan t s w as f ou n d w it h ov er w eigh t
and w it h a w aist circum ference of m ore t han 84 cm ,
w hich places t hem in t he cat egor y of incr eased r isk
of hav ing a CVE.
On t he ot her hand, t he lev els of I R and GI
suggest t hat descendant s are in a process of m et abolic
dy sfunct ion, w hich w ill v er y pr obably m anifest it self
as DMT2. Mor eov er, it should be appoint ed t hat ver y
few of t hese descendant s are m aking changes in t heir
fat consum pt ion and exer cise habit s, show ing a t ot al
lack of knowledge about t he high risk t hey are running
of dev eloping a disease.
The fact t hat w e did not find an associat ion
bet ween t he change phases and t he levels of indicat ors
like BMI , WHR, I R and GT indicat es descendant s’ low
w illin g n ess t o m ak e f act u al ch an g es in t h eir liv in g
pat t erns. This gives rise t o t he need t o provide m ore
i n - d e p t h i n f o r m a t i o n t o f i r st - d e g r e e r e l a t i v e s o f
pat ient s wit h DMT2. This facilit at es t he underst anding
of t he biochem ical and ant hr opom et r ic changes t hey
can obser v e in t hem selv es, w hich ar e im m inent r isk
fact or s for dev eloping t he disease.
Fi n a l l y, t h e h i g h l e v e l f o u n d f o r t h e
en v ir on m en t al com pon en t of I R ( 9 8 . 6 3 % ) in dicat es
t hat t he change in eat ing pat t erns and physical act ivit y
w er e t he m ain cont r ibut ing fact or s t o m et abolic and
ant hr opom et r ic changes in t his sam ple.
REFERENCES
1. Walt er S, Post onll C, Foreyt JP. Obesit y is an environm ent al i ssu e. At h er o escl er o si s 1 9 9 9 ; 1 4 6 ( 2 ) : 2 0 1 - 9 .
2. Fr ench SA, St or y M, Jeffer y RW. Envir onm ent al influences on eat in g an d p h y sical act iv it y. An n u al Rev Pu b lic Healt h 2 0 0 1 ; 2 2 : 3 0 9 - 3 5 .
3 . Collazo C. Diab et es t ip o 2 en n iñ os. Ob esid ad I n f an t il. Diab et es Hoy 2 0 0 4 ; 1 8 - 2 0 .
4. Gallegos EC, Bañuelos Y. Conduct as pr ot ect oras de salud e n a d u l t o s c o n d i a b e t e s m e l l i t u s t i p o I I . I n v e s t Ed u c En f er m er ía 2 0 0 4 ; 2 2 ( 2 ) : 4 0 - 9 .
5. Dushay J, Abr aham son MJ. I nsulin r esist ance and t y pe 2 d iab et es: A com p r eh en siv e r ev iew . CME/ CE [ ser ial on lin e] 2 0 0 5 ab r il [ cit ed 2 0 0 5 Ju n 6 ] ; 2 2 : [ 9 scr een s] . Av ailab le from : URL: w w w .m edscape.com .
6. Van der Sande M, Walraven G, Milligan P, Banya W, Ceesay S, Ny an O et al. Fam ily h ist or y : An op p or t u n it y f or ear ly int er vent ions and im pr oved cont r ol of hy per t ension, obesit y, a n d d i a b e t e s . B u l l W o r l d H e a l t h O r g a n i z a t i o n 2 0 0 2 ; 7 9 ( 4 ) : 3 2 1 - 8 .
7 . Diabet es Pr ev ent ion Pr ogr am Resear ch Gr oup. Achiev ing w eight and act ivit y goals am ong diabet es prevent ion program lif est y les p ar t icip an t s. Ob esit y Res 2 0 0 4 ; 1 2 ( 9 ) : 1 4 2 6 - 3 4 . 8. Rodr íguez- Mor án M, Guer r er o- Rom er o JF. I m por t ancia del apoyo fam iliar en el cont rol de la glucem ia. Salud Pública de Méx i co 1 9 9 7 ; 3 9 ( 1 ) : 4 4 - 7 .
9. Vallis M, Ruggiero L, Greene G, Jones H, Zinm an B, Rossi S et al. St ag es of ch an g e f or h ealt h y eat in g in d iab et es. Di ab et es Car e 2 0 0 3 ; 2 6 ( 5 ) : 1 4 6 8 - 7 4 .
1 0 . Ba st a r r a ch e a - Ke n t J, Ló p e z- Al v a r e n g a JC, Te j e r o E, Ar a d i l l a C, Br i t o - Z u r i t a O, Ma ch a d o - D o m i n g u e z A e t a l . Her it abilit y of Car diov ascu alr Disease ( CVD) r isk f act or s in Mex ican s. Ob esit y. I n p r ess 2 0 0 6 .
1 1 . Pr o c h a s k a JO , Re d d i n g CA , Ev e r s K E. Th e t r an st h eor et ical m odel an d st ages of ch an ge. I n : Glan z K, Rim er BK, Lew is FM, edit or es. Healt h beh av ior an d h ealt h ed u ca t i o n . Sa n Fr a n ci sco : Jo ssey - Ba ss A W i l ey I m p r i n t ; 1 9 9 7 . p . 9 9 - 1 2 0 .
1 2 . B e n i s o v i c h S V, Ro s s i JS , N o r m a n GJ, N i g g , CR. Developm ent of a m ult idim ensional m easure of exercise self-ef f icacy. Can cer Pr ev en t ion Res Cen t er 1 9 9 8 ; 1 9 ( 5 Su p p l 1 9 0 ) : 5 6 1 - 7 5 .
1 3 . Est ados Un idos Mex ican os Secr et ar ia de Salu d. Nor m a Of icial Mex ican a p ar a el Man ej o I n t eg r al d e la Ob esid ad . ( N O M - 1 7 4 - S S A 1 - 1 9 9 8 ) . [ s e r i a l o n l i n e ] 2 0 0 4 m a r z o . D i s p o n i b l e e n : U RL: h t t p : / / w w w . d i a b e t e s v i d a . c o m . m x / d iab et esv id a/ NOM. h t . m od if icación .
14. Bonora E, Targher G, Alberiche M, Bonadonna R, Saggiani F, Zener e MB et al. Hom eost asis m odel assessm ent closely m ir r or s t h e glu cose clam p t ech n iqu e in t h e assessm en t of in su lin sen sit iv it y. Diab et es Car e 2 0 0 0 ; 2 3 ( 1 ) : 5 7 - 6 3 . 1 5 . SAGE. St a t i st i ca l a n a l y si s f o r g e n e t i c e p i d e m i o l o g y [ com put er program ] . Cork ( I ) : St at ist ical Solut ions Lt d.; 2004.