PRENATAL CARE: DI FFI CULTI ES EXPERI ENCED BY NURSES
1Leila Mar ia Ger om el Dot t o2 Nelly de Mendonça Moulin3 Mar li Villela Mam ede4
Dotto LMG, Moulin NM, Mam ede MV. Prenatal care: difficulties experienced by nurses. Rev Latino- am Enferm agem 2006 set em bro- out ubro; 14( 5) : 682- 8.
This st udy aim ed t o ident ify t he difficult ies nur ses ex per ience at t he st ar t of t heir pr ofessional life in prenat al care act ivit ies. Dat a w ere collect ed t hrough int erview s w it h 25 nurses w ho accom panied prenat al care in t he basic healt h net work of Rio Branco- AC, Brazil and were grouped according t o t he frequency and level of difficult y t hey m ent ioned. We obser v ed t hat nur ses did not dem onst r at e difficult ies in a ser ies of im por t ant prenat al care act ivit ies at t he st art of t heir professional life. However, t hey report ed different levels of difficult ies in ot h er act iv it ies. Fu r t h er m or e, t h e par t icipan t s poin t ed ou t difficu lt ies in act iv it ies t h at r equ ir e k n ow ledge ( k n ow in g) as w ell as abilit ies ( k n ow - h ow ) . Th is st u dy also in dicat ed f law s in u n der gr adu at e f or m at ion w it h r espect t o pr enat al car e, inv olv ing t heor et ical aspect s as w ell as ex clusiv ely pr act ical act iv it ies.
DESCRI PTORS: pr enat al car e; obst et r ical nur sing; educat ion, nur sing
ATENCI ÓN PRENATAL: DI FI CULTADES VI VENCI ADAS POR LAS ENFERMERAS
La finalidad de est e est udio fue ident ificar las dificult ades vividas por las enferm eras en el inicio de su v id a p r of esion al, en las act iv id ad es r elacion ad as con la at en ción p r en at al. Los d at os f u er on r ecop ilad os a t ravés de ent revist as con 25 enferm eras que acom pañaban el prenat al en la red básica de salud del m unicipio de Rio Br an co- AC, Br asil, y f u er on agr u pados segú n la f r ecu en cia y el gr ado de dif icu lt ad m en cion ado por ellas. Const at am os que las enfer m er as no pr esent ar on dificult ades en una ser ie de act ividades im por t ant es en la at ención prenat al, en el inicio de su vida profesional. Sin em bargo, relat aron que enfrent aron dificult ades en ot r as. Est as dificult ades se m ost r ar on com o siendo de difer ent es gr ados. Señalar on dificult ades en act ividades qu e ex igen con ocim ien t os ( saber ) , y t am bién en act iv idades qu e n ecesit an de h abilidades ( saber - h acer ) . El est udio t odavía indicó fallas en la form ación de pregrado respect o a la at ención al prenat al, t ant o para aspect os t eór icos com o par a act iv idades ex clu siv am en t e pr áct icas.
DESCRI PTORES: at ención pr enat al; enfer m er ía obst ét r ica; educación en enfer m er ía
ASSI STÊNCI A PRÉ-NATAL: DI FI CULDADES VI VENCI ADAS PELAS ENFERMEI RAS
Est e est udo t ev e com o obj et iv o ident ificar as dificuldades v iv enciadas pelas enfer m eir as, no início de sua v ida pr ofissional, nas at iv idades r elacionadas à assist ência pr é- nat al. Os dados for am colet ados por m eio de ent r evist as com 25 enfer m eir as que acom panhavam o pr é- nat al, na r ede básica de saúde do m unicípio de Rio Branco- AC, e foram agrupados conform e a freqüência e o grau de dificuldade referido por elas. Const at am os qu e as en f er m eir as n ão apr esen t ar am dif icu ldades em u m a sér ie de at iv idades im por t an t es n a assist ên cia pr é- nat al, no início do ex er cício pr ofissional. No ent ant o, r elat ar am que enfr ent ar am dificuldades em out r as. Essas dificuldades er am de difer ent es gr aus. Apont ar am dificuldades em at ividades que exigem conhecim ent os ( saber ) com o t am bém em at iv idades qu e n ecessit am de h abilidades ( saber - fazer ) . O est u do apon t ou ain da falhas na form ação da graduação com relação à at enção ao pré- nat al, t ant o para aspect os t eóricos com o para at iv idades ex clu siv am en t e pr át icas.
DESCRI TORES: cu idado pr é- n at al; en fer m agem obst ét r ica; edu cação em en fer m agem
1 Extract from the Master’s Dissertation; 2 Obstetric Nurse, Master’s Degree in Education, Faculty, Acre Federal University, e- m ail: [email protected] .br; 3 Full
Professor, Salgado de Oliveira Universit y; 4 Obstetric Nurse, Full Professor, University of São Paulo at Ribeirão Preto College of Nursing, WHO Collaborating Centre for Nursing Research Developm ent, e- m ail: m avim [email protected]
I NTRODUCTI ON
E
ffect ive prenat al care plays a fundam ent al role in the result of the delivery and birth process, as w ell as in m at er n al an d p er in at al m or b id it y an d m ortality rates. Achieving effectiveness m eans that this care should aim to identify factors exposing m aternal and fetal health to greater risk of negative results, as well as to know the right tim e to intervene, avoiding or reducing t he noxious consequences of t hese risks( 1).Hi g h - q u a l i t y p r e n a t a l ca r e i n v o l v e s perm anent technical training of health team s to solve t he m ost pr ev ailing pr oblem s, besides com m it m ent t o t h e n eeds ex per ien ced by t h e m ost v u ln er able part s of t he populat ion( 2).
Th e Wo r l d He a l t h Or g a n i za t i o n ( W HO) estim ates that t he risk of death due to pregnancy or b i r t h - r el a t ed ca u ses d u r i n g a w o m a n ’ s l i f ecy cl e am ounts to 1/ 160 pregnancies in Latin Am erica, against 1/ 2,400 in Europe and 1/ 5,600 in North Am erica(3).
I n t h e sear ch f o r saf e m o t h er h o o d , int ernat ional ent it ies have m obilized act ion st rat egies in the attem pt to achieve safer pregnancies and births for wom en and their newborns. One of these strategies is the presence of a trained professional for care delivery to all wom en during the gravid-puerperal cycle(4).
Th ese p r of ession als h av e b een ed u cat ed , trained and are proficient in the skills needed to handle norm al pregnancies, as well as t o ident ify and refer com plicat ions, and are responsible for applying t hem wit h com pet ence( 5).
Being com petent in a specific profession does n ot on ly im p ly h av in g v ast an d lar g e k n ow led g e. Professionals need t o know how t o use, int egrat e or m obilize t his knowledge when facing a real sit uat ion for act ion( 6).
Qualified professionals should be capable of covering a range of skills and knowledge, in different for m s an d con t ex t s, t o ex er cise t h eir pr ofession al act ivit y and be acknowledged as com pet ent( 7).
Com pet ence is also defined as indiv iduals’ capacit y t o m obilize all or part of t heir cognit ive and affect iv e r esou r ces t o cope w it h a set of com plex sit uat ions. This requires t he precise ident ificat ion of t hese r esour ces, of t he r elat ions t o be est ablished am ong t hem and of t he nat ure of “ knowing how t o m obilize”( 6). Ther efor e, com pet encies do not e equal
knowledge, t hey are not j ust know- how or at t it ude. I n st ead , b ein g com p et en t m ean s t h e cap acit y t o m obilize, int egrat e and orchest rat e t hese resources. Pr o f e ssi o n a l co m p e t e n ci e s a r e co n st r u ct e d
continuously and while m oving from one work situation t o anot her( 8).
According t o t he Brazilian law t hat regulat es professional nursing pract ice, nurses can accom pany low - r isk pr egn an t w om en t h r ou gh ou t t h e pr en at al period. I n m any health institutions, in the basic health net w or k and in t he Fam ily Healt h Pr ogram s, w idely spr ead acr oss t he count r y, nur ses ar e ex pect ed t o t ake charge of prenat al care.Thus, during educat ion, n u r sin g sh ou ld t r ain t h e sk ills n eed ed t o ach iev e proficiency and com pet ency in prenat al care.
Ep i d em i o l o g i cal ev i d en ce sh o w s t h at t h e higher t he num ber of professionals qualified for care to wom en during the gravid- puerperal cycle, the lower m at ernal m ort alit y levels will be( 4).
Prenatal care is the initial sign of the result of t he delivery process, which is why high- qualit y care d u r i n g p r eg n a n cy i s f u n d a m en t a l . Th i s r eq u i r es p r of essi on al s w h o ar e q u al i f i ed t o p er f or m t h ei r act ivit ies and apt t o develop essent ial com pet encies. Healt h educat ors in general and nursing educat ors in par t icular ar e const ant ly concer ned about founding professional t raining not only on skills developm ent , but also on com pet ency acquisit ion t o per for m t he standards established for professional practice. I n this sense, w e hav e been quest ioning w het her r ecent ly graduat ed nurses are apt t o fully carry out prenat al car e for low - r isk pr egnancies? Does under gr aduat e educat ion perm it skills t raining t o achieve proficiency in prenat al care?
I n view of t hese inquiries, t his st udy aim ed t o ident ify t he difficult ies nur ses ex per ience at t he start of their professional life in prenatal care activities, as well as to report the m otives these nurses indicate for t he difficult ies t hey experience.
METHODOLOGY
We car r ied ou t a descr ipt iv e st u dy w it h a quant it at ive approach in Rio Branco ( Acre) , Brazil. I n 2002, t he basic healt h net work in t his cit y consist ed of 13 Basic Healt h Unit s ( BHUs) , dist r ibut ed acr oss t he cit y’s different neighborhoods. These unit s offer a m u l t i d i sci p l i n a r y ca r e t e a m . Th e n u m b e r o f pr ofessionals v ar ies fr om unit t o unit . The net w or k also includes 23 Fam ily Healt h Unit s.
assessm en t , adequ at e diagn osis an d t r eat m en t , a lar ge m aj or it y of t hese w om en is again r efer r ed t o t he nur ses t o cont inue pr enat al car e. I n 2002, 49 nurses offered prenatal care in the city’s basic network. The study population consisted of nurses who deliv er ed pr enat al car e in public healt h ser v ices in Rio Br anco- AC in 2002. The sam ple w as r andom ly select ed and included 25 nur ses, 12 in t he Fam ily He a l t h Un i t s a n d 1 3 i n t h e Ba si c He a l t h Un i t s, corresponding to at least 50% of the study population. Data were collected by m eans of an interview scr ipt w it h open and closed quest ions. The closed questions were used to characterize the subj ects and prenat al care, as well as t o report t he act ivit ies t he nurses faced difficulties with when they started to work in prenatal care. The open questions served to describe the m otives they m entioned for these difficulties.
We constructed a list of activities and procedures accom plished during prenatal care, from the first until the last visit. For each of these, we asked the nurses to indicate the level of difficulty (Many-M, Moderate-MO or None-N) to perform this activity or procedure at the start of their professional career in prenatal care.
Th e collect ed dat a w er e an aly zed t h r ou gh frequencies and percentages. Data about the m otives for difficult ies were coded t o facilit at e analysis.
This study was guided by the ethical precepts of research, guaranteeing autonom y, doing well, doing no har m and social j ust ice. I n accor dance w it h t he Free and I nform ed Consent Term , all subj ects received t he guarant ee of anonym it y, inform at ion secrecy and use of t his inform at ion for research purposes only.
RESULTS
Char act er izing t he subj ect s
The interviewed nurses had between one and 1 9 y ear s ex p er ien ce in p r en at al car e ( m ean 6 . 4 years) . Seventeen of them ( 68% ) had worked in this area for up t o six years ( Table1) .
Table 1 - Distribution of nurses’ experience in prenatal care services. Rio Branco- AC, 2002
On t he average, nurses in t he Fam ily Healt h Units offered between 10 and 80 prenatal visits/ m onth, and were also responsible for ot her act ivit ies besides pr enat al car e. Six nur ses r epor t ed bet w een 10 and 20 visits, four between 30 and 40, and two an average of 80 per m onth.
At t h e Basic Healt h Un it s, n u r ses w or k ed alm ost ex clusiv ely in pr enat al car e. They offer ed a variable num ber of visit s, from 50 t o 250 per m ont h, accor d in g t o t h e ar ea cov er ed b y t h eir u n it . Tw o nurses inform ed 50 visit s, t hree bet ween 60 and 80, t wo 100 visit s, four 160 and t wo 250 prenat al visit s per m ont h.
Difficult ies faced by t he nurses in prenat al care
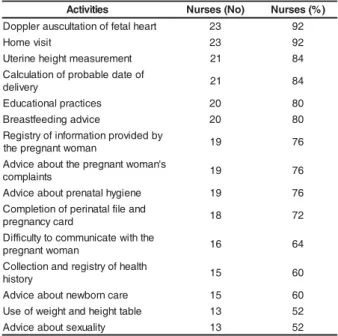
Th e com plex it y of pr en at al car e act iv it ies varies. Am ong t he list ed act ivit ies, we found t hat a lar ge m aj or it y of nur ses affir m ed no difficult ies t o perform “ Doppler auscult at ion of fet al heart ( 92% ) , hom e visits ( 92% ) , uterine height m easurem ent ( 84% ) and calculat ion of probable dat e of delivery ( 84% ) ”. Table 2 shows t he dist ribut ion of act ivit ies for which at least 50% of the nurses indicated no difficulties at t he st art of t heir professional career.
Table 3 lists activities for which at least 50% of t h e n ur ses in dicat ed m oder at e difficult ies. I t is r em ar k able t hat 72% of t he int er v iew ees r epor t ed m oderate difficulty to “ identify risk factors” at the start of t heir professional pract ice.
Table 2 - Distribution of prenatal care activities of no difficulty according to a m aj ority of nurses. Rio Branco-AC, 2002 e c n e i r e p x e e r a c l a t a n e r
P Nurses(No) Nurses(%)
s r a e y 2 o t
1 8 32
s r a e y 4 o t
3 6 24
s r a e y 6 o t
5 3 12
s r a e y 8 o t
7 3 12
s r a e y 0 1 o t
9 -
-s r a e y 0 1
> 5 20
s e i t i v i t c
A Nurses(No) Nurses(%)
t r a e h l a t e f f o n o it a tl u c s u a r e l p p o
D 23 92
t i s i v e m o
H 23 92
t n e m e r u s a e m t h g i e h e n i r e t
U 21 84
f o e t a d e l b a b o r p f o n o it a l u c l a C y r e v il e
d 21 84
s e c it c a r p l a n o it a c u d
E 20 80
e c i v d a g n i d e e f t s a e r
B 20 80
y b d e d i v o r p n o it a m r o f n i f o y r t s i g e R n a m o w t n a n g e r p e h
t 19 76
s ' n a m o w t n a n g e r p e h t t u o b a e c i v d A s t n i a l p m o
c 19 76
e n e i g y h l a t a n e r p t u o b a e c i v d
A 19 76
d n a e li f l a t a n i r e p f o n o it e l p m o C d r a c y c n a n g e r
p 18 72
e h t h t i w e t a c i n u m m o c o t y tl u c if f i D n a m o w t n a n g e r
p 16 64
h tl a e h f o y r t s i g e r d n a n o it c e ll o C y r o t s i
h 15 60
e r a c n r o b w e n t u o b a e c i v d
A 15 60
e l b a t t h g i e h d n a t h g i e w f o e s
U 13 52
y t il a u x e s t u o b a e c i v d
Table 3 - Dist r ibut ion of pr enat al car e act iv it ies of m oderat e difficult y according t o m aj orit y of nurses. Rio Br anco- AC, 2002
s e i t i v i t c
A Nurses(No) Nurses(%)
n o it a c if it n e d i r o t c a f k s i
R 18 72
c i r t e t s b o -l a c i g o l o c e n y g c if i c e p S n o it a n i m a x e l a c i s y h
p 16 64
e b i r c s e r p n a c e s r u n e h t n o it a c i d e
M 14 56
y r e v il e d r o f n o it a r a p e r p d n a e c i v d
A 14 56
n o it c e t e d r o t c a f k s i r f o e s a c n i r e f e
R 13 52
n o it a n i m a x e l a c i s y h p l a r e n e
G 12 48
Table 4 - Distribution of prenatal care activities causing m any difficult ies according t o m aj orit y of nurses. Rio Br anco- AC, 2002
s e i t i v i t c
A Nurses(Nº) Nurses(%)
y r o t a r o b a l f o t n e m s s e s s a d n a t s e u q e R s t s e
t 7 28
tl u s e r d n a n o it c e ll o c r a e m s p a P t n e m s s e s s
a 6 24
c i r t e t s b o -l a c i g o l o c e n y g c if i c e p S n o it a n i m a x e l a c i s y h
p 5 20
e b i r c s e r p n a c e s r u n e h t n o it a c i d e
M 5 20
h t i w / e t a r t r a e h l a t e f f o n o it a tl u c s u A d r a n i
P 4 16
s r e v u e n a m n o it a p l a
P 4 16
n o it a c if it n e d i r o t c a f k s i
R 3 12
n o it c e t e d r o t c a f k s i r f o e s a c n i r e f e
R 3 12
y t il a u x e s t u o b a e c i v d
A 2 8
s e c it c a r p l a n o it a c u d
E 1 4
e c i v d a g n i d e e f t s a e r
B 1 4
e l b a t t h g i e h d n a t h g i e w f o e s
U 1 4
d e d i v o r p n o it a m r o f n i f o n o it a r t s i g e R n a m o w t n a n g e r p e h t y
b 1 4
n o it a n i m a x e l a c i s y h p l a r e n e
G 1 4
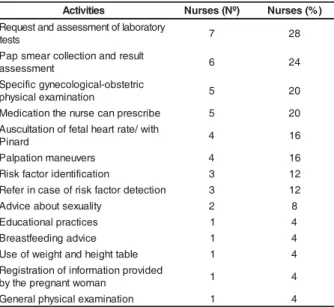
Table 4 present s all act ivit ies for which t he nurses m entioned m any difficulties at the start of their pr of ession al car eer. Th e f ollow in g deser v e special attention: “ Request and assessm ent of laboratory tests - 7 ( 28% ) , Pap sm ear collection and result assessm ent - 6 ( 24% ) , specific gy necological- obst et r ic phy sical exam ination - 5 ( 20% ) and m edication the nurse can prescribe - 5 ( 20% ) ”.
Mot ives for difficult ies faced by nurses
The coding of m ot ives for t he difficult ies t he nurses init ially experienced revealed t hat t hese were relat ed t o: flaws in undergraduat e t raining, absence o f s e r v i c e p r o t o c o l , i n e x p e r i e n c e o f r e c e n t l y g r a d u a t es a n d st u d en t ’ s l a ck o f i n t er est d u r i n g u n d e r g r a d u a t e t r a i n i n g ( Ta b l e 5 ) . “ Fl a w s i n u n d e r g r a d u a t e t r a i n i n g ” w a s m e n t i o n e d m o s t fr equent ly ( 80% ) .
Table 5 - Dist ribut ion of alleged causes of difficult ies t o per for m pr enat al car e act iv it ies. Rio Br anco- AC, 2002 s e v i t o
M Nurses(No) Nurses(%)
g n i n i a r t e t a u d a r g r e d n u n i s w a l
F 20 80
l o c o t o r p e c i v r e s f o e c n e s b
A 1 4
s e t a u d a r g y lt n e c e r f o e c n e i r e p x e n
I 4 16
g n i r u d t s e r e t n i f o k c a l s 't n e d u t S g n i n i a r t e t a u d a r g r e d n
u 2 8
The int erviewed nurses also inform ed som e strategies they used to overcom e the difficulties: 68% m ent ioned going back t o st udy, j ust ifying t hat t hey f el t t h e n eed t o st u d y an d seek t h e so l u t i o n t o pr oblem s t hey ex per ienced in t echnical book s and m an u als.
Another strategy they m entioned was to seek help fr om anot her, m or e ex per ienced pr ofessional: 4 8 % of t h e in t er v iew ed n u r ses sou g h t h elp f r om anot her nurse, while 20% consult ed t he physician.
Other nurses ( 32% ) inform ed that they ended up overcom ing t he difficult ies during daily act ivit ies.
DI SCUSSI ON
These r esult s r eaffir m t he conv ict ion t hat , alt hough com pet ency is considered a landm ark, it is n o t a f i n a l p o i n t i n p r o f e ssi o n a l d e v e l o p m e n t . According t o specialist s, it is acquired t oget her wit h pr oficiency, and t he ex per t st at us is achieved aft er m any years of experience and professional growt h( 9).
The int er v iew ed nur ses r ev ealed t heir v ast prenatal experience as a result of the num ber of visits t hey offer. This highlight s t he im por t ance of sk ills d e v e l o p m e n t t h r o u g h r e p e t i t i o n i n p r o f e ssi o n a l exercise. I n t his respect , it is not iceable t hat , while knowledge about different com pet encies is acquired during healt h professionals’ educat ion, skills relat ed t o essent ial or crit ical com pet encies for care qualit y a r e i m p r o v ed a n d a d v a n ced d u r i n g p r o f essi o n a l pract ice( 9).
I n t h e b a si c h e a l t h n e t w o r k , t h e st u d y participants are responsible for prenatal care delivery to the entire service clientele, which entails the need for high- qualit y prenat al care t raining.
nur ses offer ed less v isit s, as t hey cov er a sm aller area t han t he Basic Unit s.
I dent ify ing t he char act er ist ics desir able for high- qualit y prenat al care is one form of professional com pet ency- based assessm ent . These charact erist ics, which represent the knowledge based on professionals’ sk i l l s a n d a p t i t u d es t o so l v e p r o b l em s, a n a l y ze situations and com m unicate, allow for the recognition of com pet ence st andards for professional pract ice( 10).
A large m aj orit y of t he nurses indicat ed no difficult ies r elat ed t o “ Doppler auscult at ion of fet al heart , hom e visit s, ut erine height m easurem ent and calculat ion of pr obable dat e of deliv er y ”, r ev ealing that im portant prenatal care activities were guaranteed in their training process. Auscultation is used to verify t he fet us’ heart beat condit ions, and m easurem ent is used to identify fetal growth, allowing for the detection of deviat ions.
Au scu lt at ion an d m easu r em en t ar e sk ills ( k n o w - h o w ) t h a t r e q u i r e t r a i n i n g t o a ch i e v e pr oficiency. Sk ills ar e const r uct ed t hr ough t raining, w it h r enew ed exper iences, w hen st udent s have t he opport unit y t o exercise t hese act ivit ies( 11).
Hom e visits should be used to bring pregnant wom en who do not attend the visits back to prenatal care, as well as to com plete the educative work with t he pregnant wom an and her fam ily group( 12). These
require knowledge ( knowing) , skills ( know- how) and attitudes ( know- how- to- be) . The fact that 92% of the nurses inform ed no difficulties to perform this activity at t he st art of t heir professional career can indicat e t hey learned t his during t heir t raining.
The nurses’ report s showed no difficult ies in act iv it ies r elat ed t o dem ands for healt h adv ice and educat ion. Most of t hem inform ed t hat “ educat ional practices, advice about breastfeeding, about sexuality, ab o u t n ew b o r n car e, ad v i ce ab o u t t h e p r eg n an t w o m a n ’ s co m p l a i n t s, p r e n a t a l h y g i e n e a n d co m m u n i cat i n g w i t h t h e p r eg n an t w o m an ” w er e perform ed easily. They did not indicate any difficulties eit her in t erm s of m aking not es, such as “ regist ering of inform at ion provided by t he pregnant wom an and collect ion of healt h hist ory, com plet ing t he perinat al file and t he pregnancy card”.
These result s show t hat t he developm ent of professional skills to m ake pregnant wom en and their fam ilies take care of their own health was incorporated, during t heir undergraduat e course. This show s t hat the educational institutions attend to one of the goals o f p r en at al car e. I n t h e sam e w ay, d u r i n g t h ei r
t r a i n i n g , t h e n u r se s l e a r n e d t h e r e l e v a n ce o f regist ering all inform at ion relat ed t o t he evolut ion of pr egn an cy.
Act i v i t i e s ca u si n g m o d e r a t e d i f f i cu l t i e s included “ identifying risk factors and referring patients, general and specific gynecological- obst et ric physical ex am inat ion”.
One of t he m ain goals of prenat al care is t o id en t if y r isk f act or s t h at can im p ed e t h e n or m al ev olut ion of pr egnancy and, if necessar y, r efer t he pregnant wom an t o a m ore com plex care level, t hus guarant eeing t he early t reat m ent of t hese abnorm al co n d i t i o n s. Al t h o u g h 1 8 ( 7 2 % ) n u r ses i n d i cat ed m oder at e difficult ies t o ident ify r isk fact or s, t hese d i f f i c u l t i e s m a y e n t a i l s e r i o u s c o n s e q u e n c e s , esp ecially f or case in w h ich r ap id d iag n osis an d adequat e t r eat m ent ar e essent ial for m at er nal and fet al healt h.
Gener al and specific gynecological- obst et r ic phy sical ex am inat ions ar e per for m ed t o follow t he d e v e l o p m e n t o f p r e g n a n cy, i d e n t i f y n o r m a l m odificat ions in t he m ot her’s organism , give advice in case of com plaints and diagnose possible problem s. Pr ofessionals in pr enat al car e need t o m ast er t his knowledge ( knowing) to be able to provide safe advice and ident ify problem s.
I n case o f al t er at i o n s d u r i n g p r eg n an cy, ident ificat ion and referral are som e of t he essent ial sk ills r equir ed fr om pr enat al car e pr ofessionals, in accordance wit h t he essent ial com pet encies for basic m idw ifer y pr act ice, elabor at ed by t he I nt er nat ional Confederat ion of Midwives( 13).
The difficulties, even if m oderate, to perform physical exam s and ident ify risk fact ors reinforce t he n eed f or ed u cat ion al en t it ies t o r ev iew t each in g st rat egies for t he developm ent of essent ial m idwifery sk ills.
Mo st n u r se s a l so m e n t i o n e d m o d e r a t e d i f f i cu l t i es r el at ed t o t h e m ed i cat i o n t h ey co u l d prescribe in prenat al care. According t o t he Brazilian Federal Nursing Council ( COFEN) , nurses can prescribe drugs est ablished by t he Public Healt h Program s and b y r ou t in es ap p r ov ed in p u b lic or p r iv at e h ealt h inst it ut ions. Undergraduat e nursing course curricula should pr epar e t heir st udent s for t his r ealit y, since t his is a rout ine act ivit y nowadays( 14). On t he ot her
Fi f t y - si x p er cen t o f t h e n u r ses i n d i cat ed m oderat e difficult ies t o “ give advice and prepare for delivery”. As t he nurses did not clarify t he nat ure of d if f icu lt ies r elat ed t o ad v ice an d p r ep ar at ion f or delivery, we suggest furt her research t o ident ify t his. Pregnancy is known as a particular m om ent to dissolve m yths and erroneous views of the parturition process. Delivery is cult urally seen as a process t hat leads t o suffering and great pain.
Al t h o u g h t h e n u r se s i n d i ca t e d m a n y difficult ies t o perform a large num ber of act ivit ies at t he st art of t heir professional career, t he percent age of nurses for each ident ified act ivit y was sm all. The highest rat e was found for “ request and assessm ent of laborat ory t est s” ( 28% ) . This difficult y reflect s t he absence of care prot ocols at t he st udy inst it ut ions.
Dat a in Table 4 show t hat several act ivit ies t hat require skills ( know - how ) , such as “ Pap sm ear co l l ect i o n , g en er a l a n d sp eci f i c p h y si ca l ex a m , auscultation of fetal heart rate with Pinard and palpation m aneuvers” were associat ed wit h m any difficult ies.
Wit h r espect t o “ auscult at ion of fet al hear t rate with Pinard”, further research is needed to identify if t he problem is relat ed t o t he locat ion of t he fet al f o cu s, d u e t o d i f f i cu l t i es t o ca r r y o u t p a l p a t i o n m aneuvers and, t hus, locat e t he auscult at ion focus, or t o au scu lt at ion it self b y m ean s of t h e Pin ar d st et hoscope.
Eight y per cent of t he par t icipant s indicat ed “ f law s in u n der gr adu at e t r ain in g” as a m ot iv e f or difficult ies at t he st ar t of t heir pr ofessional car eer. The nurses inform ed t hat som e know ledge w as not d iscu ssed or r eceiv ed lit t le at t en t ion d u r in g t h eir under gr aduat e pr ogr am . They em phasized t hat t he content of the wom en’s health care nursing subj ect is very large in com parison with the available tim e. Other j ust ificat ions for t hese difficult ies included t he large n u m b er of st u d en t s f or on e sin g le su p er v isor in practice; the lack of stim uli to reflect on the knowledge p r e se n t e d i n cl a ss; a n d r e d u ce d p r a ct i ce t i m e , r esult ing in lit t le or no r epet it ion of sk ills- r equir ing act iv it ies.
These j ustifications call attention to the need t o r e v i e w t h e t e a ch i n g / l e a r n i n g p r o ce ss i n t h e d iscip lin es r esp on sib le f or p r en at al car e t r ain in g , part icularly in t erm s of offering t ools t he graduat es can use in pr ofessional act iv it ies, allow ing t hem t o con st r u ct t h e ex pect ed com pet en ce. On t h e ot h er hand, these findings showed that, at the start of their pr ofessional car eer, t he nur ses adopt ed a st at e of
con t em plat ion abou t t h eir pr of ession al pr act ice in or der t o pr epar e an d t h en act in accor dan ce w it h pr en at al car e com pet en ce st an dar ds. Th e w ay s t o overcom e their difficulties, such as returning to books, looking for t echnical m anuals and seeking help from ot h er pr of ession als r ev ealed t h e pr epar at ion t h ey su b m it t ed t h em selv es t o in or d er t o ach iev e t h e ex pect ed pr ofessional per for m ance.
When pr ofessionals m anage t o under st and t he under pinnings of cur r ent pr act ices, t his m eans t hey achieved t he prerequisit e for behavior change. Readiness for change involves a cont inuum of st eps, i n cl u d i n g p r e - co n t e m p l a t i o n , co n t e m p l a t i o n , p r e p a r a t i o n , a ct i o n a n d m a i n t e n a n ce . Th e contem plation stage is reached when the individual is ready t o change behavior( 9).
A study to assess the clinical perform ance of recent graduates indicated that their activity in clinical pract ice exceeded expect at ions, when com paring t he co m p e t e n ce l e v e l s e x p e r i e n ce d p r o f e ssi o n a l s ex pect ed f r om r ecen t gr adu at es w it h t h e act u ally observed levels at t he st art of professional pract ice. The authors call attention to the im portance of these f in d in g s t o assess t h e q u alit y of n u r sin g sch ools’ products when considering the perform ance of recently graduat ed st udent s. They also alert t o t he need for cau t ion w it h h y p ot h et ical est im at es ab ou t r ecen t graduat es’ com pet ence( 15).
Th e se f i n d i n g s a l so d e m o n st r a t e t h a t r et u r n in g t o t h e t r ain in g in st it u t ion t o solv e t h e difficult ies graduat es face is not a pract ice used by nurses as a strategy to overcom e difficulties, nor has it been a space t o obt ain updat ed knowledge.
FI NAL CONSI DERATI ONS
Put t ing in pract ice a series of charact erist ics d esi r a b l e f o r h i g h - q u a l i t y p r en a t a l ca r e d i d n o t co n st i t u t e a so u r ce o f d i f f i cu l t i es f o r t h e st u d y part icipant s at t he st art of t heir professional career. However, t hey report ed different levels of difficult ies in ot her act ivit ies. This indicat es t he need for furt her st udies t o ident ify t heir origin and nat ure.
The ident ified difficult ies allow for reflect ions about t he r ole of t he t eaching inst it ut ion in t hese professionals’ t raining, so as t o cont ribut e t o bet t er perform ance at t he st art of professional life, as well as t o achieve sat isfact ion in t erm s of knowledge and k now - how .
The Brazilian curricular guidelines established a n e w , co m p e t e n cy - b a se d p r o f i l e f o r h e a l t h p r o f e ssi o n a l s, i n cl u d i n g n u r se s. A co m p e t e n cy cur r iculum for nur sing r equir es int egr at ion bet w een t heory and pract ice. St udent s need t o have cont act
w it h r eal sit uat ions fr om pr act ice since t he st ar t of t heir t raining, so as t o reflect , t heorize and develop know- how in different cont ext s, t hus est ablishing t he t eaching/ lear ning pr ocess.
I f nurses want t o deliver prenat al care wit h com pet ence, t hey need t o dev elop count less sk ills ( know - how ) w hich, in t ur n, r equir e vast know ledge ( knowing) to allow them to assum e an attitude ( know-how- t o- be) when t hey are faced wit h risk sit uat ions in pregnant wom en.
REFERENCES
1. Enk in M, Keir se MJNC, Neilson J, Cr ow t her C, Duley L, Hodnet t E, et al. Guia para at enção efet iva na gravidez e no part o. Rio de Janeiro ( RJ) : Guanabara Koogan; 2005. 2. Trevisan MR, De Lorenzi DRS, Araúj o NM, Ésber K. Perfil da assist ência pré- nat al ent re usuárias do Sist em a Único de Saú de em Cax ias do Su l. Rev Br as Gin ecol Obst et 2 0 0 2 j unho; 24( 5) : 293- 9.
3. World Healt h Organizat ion. [ hom epage on t he I nt ernet ] . Geneva: WHO; [ cit ed 20 March 2004] Abouzahr C, Wardlaw T. Mat ernal m ort alit y in 2000: est im at es developed by WHO, UNI CEF and UNFPA. 2003. [ 5 t elas] . Av ailable on: ht t p: / / w w w . w h o . i n t / r e p r o d u c t i v e - h e a l t h / p u b l i c a t i o n s / m at er nal_m or t alit y _2000/ m at er nal_m or t alit y _2000. pdf. 4. MacDonald M, St arrs A. La at ención calificada durant e el par t o. Un cuader no infor m at iv o par a salv ar la v ida de las m uj eres y m ej orar la salud de los recién nacidos. New York ( USA) : Fam ily Car e I nt er nacional; 2003.
5. World Healt h Organizat ion. Making pregnancy safer: t he cr it ical r ole of t he sk illed at t endant : a j oint st at em ent by WHO, I CM, and FI GO. Geneva: WHO; 2004.
6. Perrenoud P. Ensinar: Agir na urgência, decidir na incert eza. Port o Alegre ( RS) : Art es Médicas Sul; 2001.
7 . Wor t h - Bu t ler M, Mu r p h y RJL, Fr aser DM. To w ar d s an int egrat ed m odel of com pet ence in m idwifery. Midwifery 1994 Decem ber ; 1 0 ( 4 ) : 2 2 5 - 3 1 .
8. Perrenoud P. Dez novas com pet ências para ensinar. Port o Alegre ( RS) : Art es Médicas Sul; 2000.
9. Kak N, Burkhalt er B, Cooper MA. Measuring t he com pet ence of healt hcar e pr ov ider s. Oper at ions Res I ssue Paper 2001 [ ser ial on lin e] Ju ly [ cit ed 1 0 Apr il 2 0 0 6 ] ; 2 ( 1 ) : 1 - 2 8 . [ 1 2 scr e e n s] . Av a i l a b l e o n : w w w . q a p r o j e ct . o r g / p u b s/ PD F/ com pet ence. pdf
10. Hager P, Gonczi A, At hanason J. Topicos generales sobre la ev aluación de la com pet encia. Asses Ev aluat ion Higher Educ 1 9 9 4 j unio; 1 9 : 3 2 7 - 3 9 .
11. Perrenoud P. Const ruir as com pet ências desde a escola. Port o Alegre ( RS) : Art es Médicas Sul; 1999.
1 2 . Schim er J, Par ras AP, Leocádio E, For m iga JFN Filho, Faj ar do ML, Cost a Net o MM, et al. Assist ên cia pr é- n at al. Manual Técnico. 3r d ed. Br asília ( DF) : Minist ér io da Saúde
Secret aria de Polít icas de Saúde; 2000.
13. I nt er nat ionalm idw iv es.or g [ hom epage on t he I nt er net ] Ma n i l a : I n t e r n a t i o n a l Co n f e d e r a t i o n o f Mi d w i v e s. Com pet encies; c2005 [ updat e Febr uar y 22 2005; cit ed 20 Se p t e m b e r 2 0 0 4 ] . Av a i l a b l e f r o m : h t t p : / / www.int ernat ionalm idwives.org
1 4 . Co n sel h o Fed er a l d e En f er m a g em ( BR) . Reso l u çã o COFEN- 271. Regulam ent a ações do enferm eiro na consult a, prescrição de m edicam ent os e requisição de exam es. Rio de Janeiro ( RJ) : Conselho Federal de Enferm agem ; 2002. 15. O’ Connor SE, Pearce J, Sm it h RL, Voegeli D, Walt on P. An evaluat ion of t he clinical perform ance of newly qualified nurses: a com pet ency based assessm ent . Nurse Educ Today 2 0 0 1 Ap r il; 2 1 : 5 5 9 - 6 8 .