Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
w w w . r b h h . o r g
Original
article
Prevalence
of
anemia
in
a
sample
of
elderly
southeastern
Brazilians
Fernando
Callera
a,∗,
Alexandra
Fernandes
Callera
a,
Adriano
Moraes
da
Silva
b,
Evandro
Secchi
Rosa
aaCentrodeHematologiadoVale,SãoJosédosCampos,SP,Brazil bUniversidadePaulista(UNIP),SãoJosédosCampos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received1May2014 Accepted23June2014
Availableonline24November2014
Keywords: Anemia Aging Hematology Erythrocytes
a
b
s
t
r
a
c
t
Objective:Todemonstratetheproportionofanemiaanditsassociationwithdemographic andclinicalcharacteristicsinarepresentativesampleofelderlypeoplefromSãoJosédos Campos,SãoPaulo.
Methods:Demographicdataandbloodsampleswerecollectedfrom398over65-year-old maleandfemaleindividuals.Anemiawasdefinedashemoglobinconcentration<12g/dL inwomenand<13g/dLinmen.Anemicandnon-anemicgroupswerecomparedusingthe chi-squaredtestandamultiplelogisticregressionmodel.
Results:Theprevalenceofanemiawas18.6%(20.8%inmenand17.6%inwomen).The per-centagesofanemiarosesignificantlyacrosstheagegroups>75–80,>85–90and>90–95years (p-value=0.0251).Therewerenosignificantdifferencesingender,ethnicbackground,place ofresidence,yearsofschooling,income,comorbiditiesanduseofmedications. Accord-ingtogender,themeanhemoglobinconcentrationandmeancorpuscularvolumewere 11.5g/dL(range:8.4–11.9g/dL)and90.7fL(range:63.0–111.7fL)forwomenand 11.9g/dL (range:8.6–12.8g/dL)and92.1fL(range:59.8–100.1fL)formen.Thegreatmajorityof ane-miacasesweremildwithlessthan6%havinghemoglobinconcentrationsbelow10.9g/dL. Meancorpuscularvolumewaslowerthan80fLinsixcases(8%),between80and100fLin 65cases(88%)andhigherthan100fLinthreecases(4%).
Conclusion: Atotalof18.6%ofelderlypeoplefromSãoJosédosCamposhadmildanemia withthemajoritybeingnormocytic.Thepercentagesofanemiaroseastheageincreased demonstratinganassociationbetweenageandanemia.
©2014Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:CentrodeHematologiadoVale,RuaEuclidesMiragaia700,Sala75,Centro,12245-820SãoJosédosCampos,SP, Brazil.
E-mailaddress:[email protected](F.Callera). http://dx.doi.org/10.1016/j.bjhh.2014.06.005
Introduction
Ithasbeen demonstratedthatanemiaamongolderpeople isassociatedwithavarietyofadverseoutcomes,including mortality.1,2Estimatesoftheprevalenceofanemiainelderly populationsdependondemographicaspects,locationandthe healthstatusoftheindividuals.3
InBraziltherearefewstudiesinthisfieldofresearch.Tothe bestofourknowledgetheprevalenceofanemiawaswell doc-umentedinelderlyindividualsfromonlytwourbanregions locatedinthenortheastern4andsouthernregions.5
Consideringthe impactof anemiaon the agedand the paucityofcomparativedatainBrazil,itseemsthatadditional studiesfromdifferentregionsareneeded.Thepopulationof SãoJosédosCampos,thelargestcityintheValedoParaíba (State of São Paulo), is aging because of lower birthrates asdemonstratedbytheevolutionaryanalysisofits popula-tionpyramid.6Therefore,theobjectivesofthisstudywereto analyze the prevalenceofanemia and its association with demographic characteristics in a sample of elderly people fromSãoJosédosCampos,southeasternBrazil.
Methods
ThisstudywascarriedoutattheCentrodeHematologiado Vale(CHV)andtheHospitalPioXIIinSãoJosédosCampos. Thestudy wasapprovedbytheResearchEthicsCommittee oftheUniversidade Paulista (#481190)and all participants signedwrittenconsentforms.AccordingtoBrazilianInstitute ofGeographyandStatistics(IBGE,2010)7theestimated num-bersofelderlyresidentswere19,619femalesand17,810males agedfrom60to69yearsand14,416femalesand10,061males olderthan70years.Asamplesizeof398wascalculatedbased onanestimatedprevalenceofanemiainolderpeopleof20%, a95%confidenceintervalandasampleerrorof5%.The inclu-sioncriteriaofthe studywereover 65-year-oldindividuals, bothmalesandfemales,whohadnotbeentransfusedwith redbloodcellswithintheprevious12weeks.Aquestionnaire wasdevelopedbytheCHVregardingdemographicand clin-icalaspects.People wereinvitedtoparticipateinthestudy throughthelocalmediaincludingnewspapers,televisionand socialnetworks. One-day events were organized incentral communitymeetingpointsofallsixurbanareasofSãoJosé dosCampos(north,east,center,southeast,southandwest); intheseplacesstudents,physiciansandhealthprofessionals randomlyappliedthequestionnairetoelderlylocalresidents. Inasecondphase,theparticipantswereinvitedtogiveblood samplesintwoclinicalbiochemistrylaboratoriesinthe Hos-pitalPioXII. Overall,713 people were interviewed and 415 (58.2%)gavebloodsamples.Thesampleswereobtainedfrom themediancubitalveinusinganevacuatedtubesystem. Vol-unteerswhodidnotanswerthequestionnaireorfromwhom aninadequatebloodsamplewascollectedwereexcludedfrom thestudy.Thefinalstudysampleincluded398elderly peo-pleinterviewedbetweenMay2012andNovember2013.The WorldHealthOrganization(WHO)criteriawereusedtodefine anemia(hemoglobin concentration<12g/dLin womenand <13g/dLinmen)andassessseverity.8Anemicandnon-anemic
groupswerecomparedusingthechi-squaredtestanda mul-tiplelogisticregressionmodel;p-valuesoflessthan0.05were consideredsignificant.
Results
Theprevalenceofanemiainthissamplewas 18.6%(20.8%
in menand 17.6% in women).The percentages ofanemia
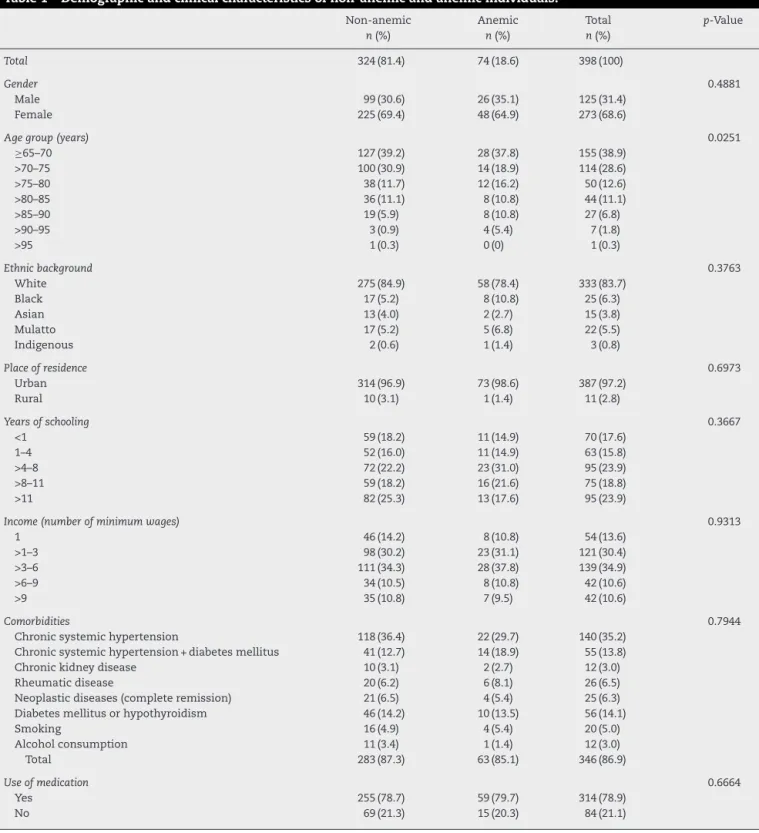
rosesignificantlyacrosstheage groups>75–80,>85–90and >90–95years(p-value=0.0251).Nosignificantdifferenceswere observedfortheothervariablesanalyzedinthisstudy (gen-der,ethnicbackground,placeofresidence,yearsofschooling, income,comorbiditiesanduseofmedications–Table1).
Hemoglobinconcentrationandmeancorpuscularvolume (MCV)oftheanemicgroupaccordingtogenderareshownin Table2.Overall,thegreatmajorityofanemiacasesweremild withlessthan6%havinghemoglobinconcentrationsbelow 10.9g/dL.TheMCV was lower than 80fL in sixcases (8%), between80and100fLin65cases(88%)andhigherthan100fL inthreecases(4%).
Discussion
Thisstudyhaslimitations.Itwascarriedoutbasedon cross-sectional data, and therefore, no cause–effect relationship could beestablished. This is onlya descriptive study that reportstheproportionandseverityofanemiaingeneral.
Theoverallprevalenceofanemiainthisserieswas18.6% with asignificant association beingdemonstrated between ageandanemia.Inaprospectivepopulation-basedstudyofall over64-year-oldresidentsinBiella(Italy),anemiawasfoundin 11.8%withtheprevalenceandincidenceofanemiaincreasing withage.9InastudyperformedinGermany,theprevalence ofanemia ofparticipants aged65 orolder was 4.3%again withtheincidenceincreasingwithage.10Aprospectivestudy conductedinelderlyKoreansdemonstratedthattheoverall prevalenceofanemiawas13.6%andasignificantassociation wasobservedwithage.11 Datafromthe UnitedStates pop-ulationassessedintheThirdNationalHealthandNutrition ExaminationSurvey(NHANESIII)identifiedanemiain10.6% of people aged65 years and older; anemia increasedwith agereachingthehighestprevalenceinthe85yearsandolder agegroup.12Ontheotherhand,datafromlowand middle-incomecountries are sparse.Bryce etal.13 surveyed10,915 peopleaged65yearsand overincatchmentareasinCuba, DominicanRepublic,PuertoRico,VenezuelaandMexicoand foundanemiaprevalenceratesof19.2%,37.3%,32.1%,9.8% and9.2%respectively;inallthesecountriesanemiaincreased withage.Inapopulation-basedstudyperformedamong392 free-living elderlyinsouth Brazil,the overall prevalenceof anemiawas12.8%andthisincreasedwithage.5Moreover,a cross-sectionalstudycarriedoutinCamaragibe(northeastern Brazil)involving284subjectsaged60yearsandovershowed thattheprevalenceofanemiawasaround11%.4
Data regarding the proportion of anemia in men and
women and the relationship between anemia and ethnic
Table1–Demographicandclinicalcharacteristicsofnon-anemicandanemicindividuals.
Non-anemic Anemic Total p-Value
n(%) n(%) n(%)
Total 324(81.4) 74(18.6) 398(100)
Gender 0.4881
Male 99(30.6) 26(35.1) 125(31.4)
Female 225(69.4) 48(64.9) 273(68.6)
Agegroup(years) 0.0251
≥65–70 127(39.2) 28(37.8) 155(38.9)
>70–75 100(30.9) 14(18.9) 114(28.6)
>75–80 38(11.7) 12(16.2) 50(12.6)
>80–85 36(11.1) 8(10.8) 44(11.1)
>85–90 19(5.9) 8(10.8) 27(6.8)
>90–95 3(0.9) 4(5.4) 7(1.8)
>95 1(0.3) 0(0) 1(0.3)
Ethnicbackground 0.3763
White 275(84.9) 58(78.4) 333(83.7)
Black 17(5.2) 8(10.8) 25(6.3)
Asian 13(4.0) 2(2.7) 15(3.8)
Mulatto 17(5.2) 5(6.8) 22(5.5)
Indigenous 2(0.6) 1(1.4) 3(0.8)
Placeofresidence 0.6973
Urban 314(96.9) 73(98.6) 387(97.2)
Rural 10(3.1) 1(1.4) 11(2.8)
Yearsofschooling 0.3667
<1 59(18.2) 11(14.9) 70(17.6)
1–4 52(16.0) 11(14.9) 63(15.8)
>4–8 72(22.2) 23(31.0) 95(23.9)
>8–11 59(18.2) 16(21.6) 75(18.8)
>11 82(25.3) 13(17.6) 95(23.9)
Income(numberofminimumwages) 0.9313
1 46(14.2) 8(10.8) 54(13.6)
>1–3 98(30.2) 23(31.1) 121(30.4)
>3–6 111(34.3) 28(37.8) 139(34.9)
>6–9 34(10.5) 8(10.8) 42(10.6)
>9 35(10.8) 7(9.5) 42(10.6)
Comorbidities 0.7944
Chronicsystemichypertension 118(36.4) 22(29.7) 140(35.2)
Chronicsystemichypertension+diabetesmellitus 41(12.7) 14(18.9) 55(13.8)
Chronickidneydisease 10(3.1) 2(2.7) 12(3.0)
Rheumaticdisease 20(6.2) 6(8.1) 26(6.5)
Neoplasticdiseases(completeremission) 21(6.5) 4(5.4) 25(6.3) Diabetesmellitusorhypothyroidism 46(14.2) 10(13.5) 56(14.1)
Smoking 16(4.9) 4(5.4) 20(5.0)
Alcoholconsumption 11(3.4) 1(1.4) 12(3.0)
Total 283(87.3) 63(85.1) 346(86.9)
Useofmedication 0.6664
Yes 255(78.7) 59(79.7) 314(78.9)
No 69(21.3) 15(20.3) 84(21.1)
Table2–Hemoglobinconcentration(Hb)andmeancorpuscularvolume(MCV)accordingtogenderfortheanemicgroup.
n % Hb(g/dL) MCV(fL)
Male 26 20.8 11.9(8.6–12.8) 92.1(59.8–100.1)
Female 48 17.6 11.5(8.4–11.9) 90.7(63.0–111.7)
Total 74 18.6 11.6(8.4–12.8) 91.1(59.8–111.7)
reported3,10,12–14butdifferenttotwostudiesperformedin dif-ferentregionsofBrazilbyBarbosaetal.4andSgnaolinetal.5 Thisstudyfoundnoassociationwithregardtoethnic back-ground;theethnicbackgroundofpatientswastosomeextent biasedduetothesubjectivityofthequestion.Thisvariable wasstudiedaccordingtothedefinitionofeachpatient with-outanyinterferenceofthehealthprofessionalwhoapplied thequestionnaire.Thus,somepatientsreportedbeingwhite rather than mulattobut this phenomenon was notclearly observedforBlackandAsianclassifications.
Asdescribedbefore,thelackofassociationfortheplace ofresidence,yearsofschooling,incomeandanemiasuggests thatsocioeconomicaspectsdidnotplayaroleinthecurrent sample.3,12,13
With regard to the cause of anemia, the data of this studysuggestahighproportionofpeoplewithunexplained anemia.12,15Therearesomereasonsthatsupportthis hypoth-esis.Mostpeoplehadmildandnormocyticanemia(88%)in contrast tolow proportionsofboth microcytic and macro-cyticanemia.Moreover,bloodsmearsfrompeoplewithhigh
MCVs showed a normal appearance of white cells. These
findingssuggestthat theoccurrenceofanemiamaynotbe associatedwith iron, folate or vitamin B12deficiencies. In addition,consideringthesimilarpercentagesofchronic sys-temic hypertension, diabetes mellitus, rheumatic diseases andkidneydiseasesbetweenanemicandnon-anemicgroups, it is reasonable to believe that the anemia could not be attributedtochronicdisease,inflammationor chronic kid-ney disease.Moreover, sincethe anemia in this series did notpresentwitheitherlowleukocyteorlowplateletcounts (datanotshown), aconcurrentassociationwith myelodys-plasticsyndromeswasnotconsidered.14,16Incomparison,a revisionofclinical,diagnosticandbiologicalissuesrelatedto anemiaand agingasreportedbyCarmel17 demonstrated a higherprevalenceofmildnormocyticanemiaandsmaller pro-portionofmicrocyticanemia;unexplainedanemiaaccounted for14–17%ofthecases.DatafromtheNHANESIIIstudy3,12 indicatedthat most occurrencesofanemia were mild and nutrient deficiency was observed in one-third, anemia of chronic disease was present in one-third and unexplained anemiawasobservedinone-third.TheItalianstudy9found ahigherproportionofnormocyticanemiaandthe underly-ingcauseofmildanemiaremainedunexplainedin26.4%of thecases.AstudyperformedinGermany10showedthatthe majorityoftheanemiacasesweremild withthe following subtypes:microcyticanemiawithirondeficiency(19%), ane-miaofchronicdisease(25%)andunexplainedanemia(44%). Thestudy carried outin Camaragibe(northeastern Brazil)4 reportedthatthemajorcharacteristicsofanemiaweremild,
with normochromia and normocytosis and a lower
preva-lenceofmicrocytosis.Incontrast,theoccurrenceofanemia in older people from southern Brazil was associated with microcytosisandhypochromia.5DatafromCuba,Dominican Republic,PuertoRico,Venezuela and Mexicodemonstrated thatmostcasesofanemiawereassociatedwithmicrocytosis and nutritional deficiency.13 Giventhat anemia isa multi-factorialcondition,amajorproblemwithinterpretingthese reportsisthattheyareextrapolatedfromlocaldatafrom spe-cificregionsandthusmostlikelyreflectingthecharacteristics
ofaparticularpopulation.Tofurtherinvestigatethismatter, studiesincorporatingthemeasurementofserumbiochemical markerssuchasiron,ferritin,folate,vitaminB12and creati-nineshouldbedesignedinthisregion.
Conclusion
Thisstudydemonstratesthat18.6%ofarepresentative sam-pleofcommunity-dwellingelderlypeoplefromSãoJosédos Campos,southeasternBrazilhadmildanemiawiththegreat majoritybeingnormocytic.Thepercentagesofanemiarose acrossthehighestagegroupsandanassociationbetweenage andanemiawasdemonstrated.Withregardtotheprevalence ofanemiaintheelderly,thisserieswassimilartoCubabut higherthandevelopedcountriesandotherregionsofBrazil. Boththeassociationbetweenageandanemiaandthe sub-stantialproportionofmildnormocyticanemiaofunexplained causearesimilartootherstudies.
Finally, consideringthe heterogeneityinthedistribution ofsocialandbiologicalriskfactorsinBrazil,webelievethat anationalsurveyoftheprevalenceofanemiaintheelderly mayshedsomelightonthisimportantissue.Inaddition,a long-termfollow-upoftheagedwithmildandasymptomatic anemiamaybeimportanttoestablishwhetheranemiaisa markerofamoresevereunderlyingcondition.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PatelKV,HarrisTB,FaulhaberM,AnglemanSB,ConnellyJ, BauerDC,etal.Racialvariationintherelationshipofanemia withmortalityandmobilitydisabilityamongolderadults. Blood.2007;109(11):4663–70.
2.CulletonBF,MannsBJ,ZhangJ,TonelliM,klarenbachS, HemmelgarnBR.Impactofanemiaonhospitalizationand mortalityinolderadults.Blood.2006;107(10):3841–6. 3.PatelKV.Epidemiologyofanemiainolderadults.Semin
Hematol.2008;45(4):210–7.
4.BarbosaDL,ArrudaJK,DinizAS.Prevalênciaecaracterizac¸ão daanemiaemidososdoPragramadesaúdedaFamília.Rev BrasHematolHemoter.2006;28(4):288–92.
5.SgnaolinV,EngroffP,ElyLS,SchneiderRH,SchwankeCHA, GomesI,etal.Hematologicalparametersandprevalenceof anemiaamongfree-livingelderlyinsouthBrazil.RevBras HematolHemoter.2013;35(2):115–8.
6.PrefeituraMunicipaldeSãoJosédosCampos.Secretariade DesenvolvimentoSocial.ConselhoMunicipaldeAssistência Social.Planomunicipaldeassistênciasocial2002–2005 [Internet].SãoJosédosCampos;2002.Availablefrom: http://www.sjc.sp.gov.br/sds/downloads/PlanoAssistencia Social.pdf[cited04.04.14].
7.InstitutoBrasileirodeGeografiaeEstatística.Brasília:IBGE. Availablefrom:http://www.ibge.gov.br/cidadesat/topwindow. htm?1[cited03.04.14].
9. TettamantiM,LuccaU,GandiniF,RecchiaA,MosconiP, ApoloneG,etal.Prevalence,incidenceandtypesofmild anemiaintheelderly:thehealthandanemia
population-basedstudy.Haematologica.2010;95(11):1849–56. 10.EiseleL,DürigJ,Broecker-PreussM,DührsenU,ErbelR,
MoebusS,etal.Prevalenceandincidenceofanemiainthe GermanHeinzNixdorfRecallStudy.AnnHematol. 2013;92(6):731–7.
11.ChoiCW1,LeeJ,ParkKH,YoonSY,ChoiIK,OhSC,etal. Prevalenceandcharacteristicsofanemiaintheelderly: cross-sectionalstudyofthreeurbanKoreanpopulation samples.AmJHematol.2004;77(1):26–30.
12.GuralnikJM,EisenstaedtRS,FerrucciL,KleinHG,Woodman R.Prevalenceofanemiainpersons65yearsandolderinthe UnitedStates:evidenceforahighrateofunexplained anemia.Blood.2004;104(8):2263–8.
13.BryceRM,SalasA,AcostaD,Jimenez-VelasquezIZ, Llibre-RodriguezJJ,SosaAL,etal.Theprevalence,correlates andimpactofanaemiaamongolderpeopleinCuba, DominicanRepublic,Mexico,PuertoRicoandVenezuela.BrJ Haematol.2013;160(3):287–398.
14.denElzenWPJ,GusseklooJ.Anaemiainolderpersons.NethJ Med.2011;69(6):260–7.
15.MakipourS,KanapuruB,ErshlerWB.Unexplainedanemiain theelderly.SeminHematol.2008;45(4):250–4.
16.SteensmaDP,TefferiA.Anemiaintheelderly:howshouldwe defineit,whendoesitmatter,andwhatcanbedone?Mayo ClinProc.2007;82(8):958–66.