www.jped.com.br
ORIGINAL
ARTICLE
Association
between
socioeconomic
and
biological
factors
and
infant
weight
gain:
Brazilian
Demographic
and
Health
Survey
---
PNDS-2006/07
夽
,
夽夽
Jonas
Augusto
C.
Silveira
a,∗,
Fernando
Antônio
B.
Colugnati
b,
Ana
Paula
Poblacion
a,
José
Augusto
A.C.
Taddei
aaDepartmentofPediatrics,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bNúcleoInterdisciplinardeEstudosePesquisasemNefrologia(NIEPEN),NephrologyDivision,
UniversidadeFederaldeJuizdeFora(UFJF),JuizdeFora,MG,Brazil
Received30April2014;accepted27August2014 Availableonline13February2015
KEYWORDS
Child; Weightgain;
Nutritionaldisorders; Surveys;
Brazil
Abstract
Objective: To examine the associations between socioeconomic and biological factors and
infantweightgain.
Methods: All infants (0-23 months of age) with available birth and postnatal weight data
(n=1763) wereselectedfromthelastnationally representativesurveywith complex
prob-abilitysamplingconductedinBrazil(2006/07).Theoutcomevariablewasconditionalweight
gain(CWG), which represents howmuch anindividualhas deviatedfrom his/herexpected
weightgain,giventhebirthweight.Associationswereestimatedusingsimpleandhierarchical
multiplelinearregression,consideringthesurveysamplingdesign,andpresentedinstandard
deviationsofCWGwiththeirrespective95%ofconfidenceintervals.Hierarchicalmodelswere
designedconsideringtheUNICEFConceptualFrameworkforMalnutrition(basic,underlyingand
immediatecauses).
Results: The poorest Brazilian regions (-0.14 [-0.25;-0.04]) andrural areas (-0.14
[-0.26;-0.02])wereinverselyassociatedwithCWGinthebasiccausesmodel.However,thisassociation
disappearedafteradjustingformaternalandhouseholdcharacteristics.Inthefinalhierarchical
夽 Pleasecitethisarticleas:SilveiraJA,ColugnatiFA,PoblacionAP,TaddeiJA.Associationbetweensocioeconomicandbiologicalfactors andinfantweightgain:BrazilianDemographicandHealthSurvey---PNDS-2006/07.JPediatr(RioJ).2015;91:284---91.
夽夽
StudyconductedatDepartamentodePediatria,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](J.A.C.Silveira). http://dx.doi.org/10.1016/j.jped.2014.08.013
WeightgainamongBrazilianinfants 285
model,lowereconomicstatus(-0.09[-0.15;-0.03]),humancapitaloutcomes(maternal
edu-cation<4thgrade(-0.14[-0.29;0.01]),highermaternalheight(0.02[0.01;0.03])),andfeverin
thepast2weeks(-0.13[-0.26;-0.01])wereassociatedwithpostnatalweightgain.
Conclusion: The results showed thatpoverty and lowerhuman capital arestill key factors
associatedwithpoorpostnatalweightgain.Theapproachusedintheseanalyseswassensitive
tocharacterize inequalities amongdifferentsocioeconomiccontextsandtoidentify factors
associatedwithCWGindifferentlevelsofdetermination.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Crianc¸a; GanhodePeso; Distúrbios Nutricionais; Inquéritos; Brasil
Associac¸ãoentrefatoressocioeconômicosebiológicoseoganhodepesode lactentes:PesquisaNacionaldeDemografiaeSaúde(PNDS)de2006/07
Resumo
Objetivo: Examinarasassociac¸ões entrefatoressocioeconômicos ebiológicoseoganhode
pesodelactentes.
Métodos: Foramselecionadostodososlactentes(0-23mesesdeidade)comdadosdepesoao
nascerepós-natalavaliadosnaúltimapesquisacomrepresentatividadenacionalrealizadano
Brasil(2006/07)poramostragemprobabilísticacomplexa.AvariávelderesultadofoioEvoluc¸ão
PonderalCondicional(CWG),querepresentaquantoumindivíduodesvioudeseuganhodepeso
esperado,considerandoopesoaonascer.Asassociac¸õesforamestimadasutilizandoregressão
linearsimplesemúltiplahierárquica,considerandooplanoamostaldapesquisaeapresentadas
emdesviospadrãodoCWGcomseusrespectivosintervalosdeconfianc¸ade95%.Osmodelos
hierárquicosforamestruturadosconsiderandooModeloConceitualdeDesnutric¸ãodaUNICEF
(causasbásicas,inerenteseimediatas).
Resultados: Asregiõesbrasileirasmaispobres(-0,14[-0,25;-0,04])eaárearural
(-0,14[-0,26;-0,02]) foraminversamenteassociadas ao CWG nomodelo decausasbásicas.Contudo,essa
associac¸ãodesapareceuapósoajustepelascaracterísticasmaternasedoambientefamiliar.
Nomodelohierárquicofinal,abaixacondic¸ãoeconômica(-0,09[-0,15;-0,03]),asvariáveisde
capitalhumano(escolaridadematerna<5◦ano(-0,14[-0,29;-0,01])),maiorestaturamaterna
(0,02[0,01;0,03]))efebrenasduassemanasanterioresàpesquisa(-0,13[-0,26;-0,01])foram
inversamenteassociadasaoganhodepesopós-natal.
Conclusão: Osresultadosmostraramqueapobrezaebaixocapitalhumanoaindasãofatores
fundamentaisassociadosaoganhodepesopós-natalabaixodeesperado.Aabordagemutilizada
emnossasanálisesfoisensívelaocaracterizardesigualdadesentrediferentescontextos
socioe-conômicoseaoidentificarfatoresassociadosaoCWGemdiferentesníveisdedeterminac¸ão.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Nutritionaldisordersarecyclicallydeterminedbycultural, social,economic,andbiologicalfactorsatdifferentlevels, fromthemost proximal,suchasfoodavailabilityand the occurrenceof diseases,todistalfactorssuchasaccessto informationandtheculturalsuperstructure.1,2
The first twoyears of life are characterized by accel-erated growth and development, which require high nutritional intake and define infants as a group with high biological vulnerability, especially considering that, by this time, growth and development are more strongly determined by environmental factors than by genetic characteristics.3,4 Nutritional disorders beginning in this
period areassociated with increased mortality, increased susceptibilitytoinfectiousdiseases,impairedpsychomotor development,academicunderachievement,andlower pro-ductivecapacityinadulthood.1,4---6
InBrazil,thepredominantnutritionandhealthpolicies and programs, such as the exclusive breastfeeding cam-paign, immunization and supplementation programs, and the food fortification initiative, address infants and their mothers. The main Brazilian social support programs are knownas ‘‘FomeZero’’ and ‘‘Plano Brasil Sem Miséria’’, whichaimtopromotehouseholdfoodsecurityandautonomy forlow-incomefamiliesbymeansofconditionalcash trans-fers,thefundingoffamilyfarming,andaid forpurchasing goodsandservices.7,8
Nationalhealthsurveysareimportanttoolstoevaluate suchpublicpoliciesbecausetheydescribethe healthand nutritionprofileofthepopulation,identifyingriskfactors, toallow comparisonsamongregionsandcountriesaswell astheplottingoftrendsovertime.9,10Therefore,giventhe
significance of children’s growthin the first twoyears of life3 and using data from the last Brazilian National
(PNDS-2006/07),thisstudyaimed toexaminethe associa-tionsbetweensocioeconomicandbiologicalconditionsand postnatalweightgain.
Materials
and
methods
Studydesignandsettings
ThePNDS-2006/07wasanationalsurveyconductedbetween Novemberof2006andMayof2007,focusedonthehealth andnutritionofwomenofreproductiveage(15-49yearsold) andchildrenunder5yearsofage,includingsocial,economic andculturalfactors.ThePNDS-2006/07usedcomplex prob-abilitysamplingintwostages:theprimarysamplingunitwas thecensusarea,andthesecondary samplingunitwasthe household.The studygroupcomprisedonlyprivate house-holds (includingslums).Eligible households wereselected atrandom,takingintoaccountthenumberofcensusareas ineachregionandtheurban/ruralareas.Furtherdetailson methodology,includingsamplingdesignanddatacollection, havebeenreportedelsewhere.11
Eligibilityandselectioncriteria
The households considered eligible included at least one womanofreproductive age.Data werecollectedfromall childrenunder59monthsforeacheligiblemother.Forthe purposeofthisstudy,theauthorsselectedthesubgroupof infants(0---23monthsofage)livinginthesamehouseastheir mothers.
Datacollectionandvariablesdefinition
Datawerecollectedbypairsoftrainedfemalefield work-ers in the children’s residence. Children were weighed usingan electronic portable scale (Y60) withprecision of 100g(Dayhome®,SãoPaulo,SP,Brazil).11 Birthweightwas
collected from the child’s maternity card, and when not available,bymother’srecall.Weight-for-ageZ-score(WAZ) wascalculatedusingmacrosoftheWorldHealth Organiza-tion(WHO)AnthroSoftwareversion3.2.2forStataandthe WHOChildGrowthStandardswereusedforanthropometric classification.12
Conditionalweightgain (CWG) ---the outcome variable ---representsachild’sdeviationfromtheexpectedweight gain,givenhis/herbirthweight,andisexpressedinstandard deviations(SD).CWGisderivedfromthestandardized resid-ualsobtainedfromasex-specificlinearregressionadjusted forWAZatbirthandageatsurvey,whereWAZatsurveyis thedependentvariable.
It is important to consider this approach in longitudi-nal analysisof individuals’growth, sinceit: 1)overcomes the statistical phenomenon of regression to the mean, whereextreme values tend tomove closertothe sample mean;2) incorporatesthedifferentagesatsurvey’sdate; and, 3) deals with the collinearity of dependent weight measures.13,14Forexample,ifachildwithhighbirthweight
reduceshisorherWAZ,likewisefortherestofthechildren inthe sample whowere born withhigh birth weight,the CWGwouldbe∼0SD;but,inacounterfactualperspective,
ifthischildkeepsthesameWAZwhentherestofthe sam-ple’sWAZtendstoreduce,hisorherCWGwouldbegreater thanzeroSD.
Therationalefortheselectionoftheexposurevariables wasbasedonUNICEF’sConceptualFrameworkof Malnutri-tion,whichconsidersthebasic,underlying,andimmediate determinants.TheConceptualFrameworkofMalnutritionis ausefultoolthathelpstoorganizepossiblecausesof nutri-tionaldisordersandidentifysituationswhereinvestigations orinterventionsarerequired.2
Twovariableswereincluded asbasiccauses:children’s areaofresidence(urban/rural)andregions, dichotomized asSouthandSoutheastorasNorth,Northeast,andMidwest; this approach wasused to contrastsocioeconomic differ-ences,thelatterregionsbeingmoredeprived.
Asunderlyingcauses,somehouseholdandmaternal fac-tors were considered. Economic statuswas assessed by a validatedasset-basedquestionnaire,whichclassifies house-holds into eight mean family income categories,15 which
werereducedtofourcategories(A1-C1/C2/D/E);the cat-egories A1-C1(richest) weremerged toproducebalanced cellsizes in eachcategory.Household foodinsecuritywas assessedusingtheBrazilianFoodInsecurityScale (EBIA,in Portuguese)atranslatedandvalidatedversionoftheUSDA FoodSecurityModule,knowncurrentlyastheUSHousehold FoodSecuritySurveyMeasure---whichclassifiesthe house-hold’s in food security level asmild, moderate or severe foodinsecurity.16,17Humancapitaloutcomes(maternal
edu-cationlevel[<4thgrade]andheight[cm]),ageatbirth(<18 years),parity(numberofdeliveries),prenatalcare(number ofvisits),andtypeofdelivery(vaginal/caesarean)werealso included.
Lastly,feverordiarrheaintheprevioustwoweeks; hos-pitalization due to diarrhea, pneumonia, or bronchitis in theprevious 12 months;durationofexclusive breastfeed-ing(<1month/1-4months/>4months);age;andsexwere consideredasbasiccauses.
Dataanalysis
DataweremergedandanalyzedusingStatasoftware (Stat-aCorp.2011.StataStatisticalSoftware:Release12.College Station,TX:StataCorpLP,USA),consideringthe stratifica-tionandclusteringeffectsofthecomplexsamplingdesign. Sampleweightswereonlyappliedtothedescriptive statis-ticstoavoidoverestimatingsubgroups.10
In the analytical approach, simple and multivariable linearregression analyses wereperformed. The multivari-able regression was conducted by applying a hierarchical structuretotheanalysis,18consideringtheUNICEF’s
Frame-work for Malnutrition.2 Initially, all variables were tested
byasimplelinearregressionandthosewithp-value<0.20 wereconsideredeligibleformultivariableanalyses,within eachlevelofdetermination.Then,amultivariableanalysis wasperformedforvariablesconsideredinthebasiccauses
(Model 1), adjusted for age and sex. This procedure was repeatedforthesetofunderlying(Model2)andimmediate causes(Model3).
WeightgainamongBrazilianinfants 287
WAZ, weight-for-age Z-score.
Total records from children born after Jan/2001
(n=6,011)
Exclusion criteria:
Older than 24 months (n=3,870) Died before the survey (n=99) Not living with mother (n=140)
An
alys
is
Infant national sample (n=1,902)
Exclusion criteria:
Missing birth’s or survey’s weight data or biologically implausible WAZ (n=139)
Analyzed (n=1,763)
S
am
ple
S
el
ec
ti
on ♦
♦ ♦
♦
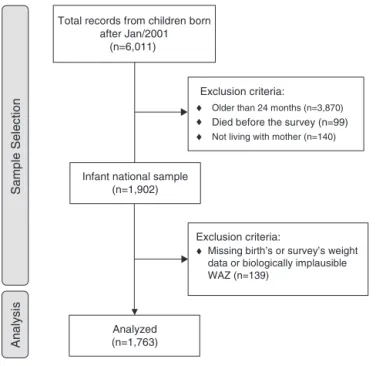
Figure1 Flowdiagramoffinalsampleselection.
WAZ,weight-for-ageZ-score.
Model2 and1.Model3wasalsocontrolledforthesource of birth weight data (maternity card or mother’s recall). ThecoefficientswerereportedastheSDofCWGwiththeir respective95%confidenceintervals(inparenthesisorsquare bracketsthroughthetext).Followingthetechnical litera-turerecommendations,estimateswereinterpretedinterms oftheirrelevancetowardthesubject,effectsize,and inher-entuncertainties,representedhereinasthe95%confidence intervals,avoidingtheusualaccept/rejectapproachbased onthep-value<0.05cut-off.19
EthicalAspects
All procedures involving human subjects in the
PNDS-2006/07wereapprovedbytheResearchEthicsCommittee oftheCenterofReferenceandTrainingonSTD/HIVofSão Paulo’sStateHealthDepartment.Thepresentresearchwas approvedbytheResearchEthicsCommitteeofthe Univer-sidadeFederaldeSãoPaulo---CEP/UNIFESP.
Results
Of the 6,011 children born after January 2001 who were availableinthedataset,1,763wereinfants(0-23monthsof age)livinginthesamehouseastheirmothers,having biolog-icallyplausibleWAZdata(-6to+5SD)atbirthandatsurvey date(Fig.1).Thesample’scharacteristicsaredescribedin
Table1.
Diarrhea in the past two weeks, duration of exclusive breastfeedingandhospitalizationfordiarrhea,pneumonia, andbronchitisin thepast12 monthswerenotconsidered formultivariableanalyses(p-value>0.20).Sexwaskeptin themodelstoadjustforpotentialsex-relatedconfounding.
SamplelossesoccurredintheModels2and3duetomissing valuesinthedataset(Table2).
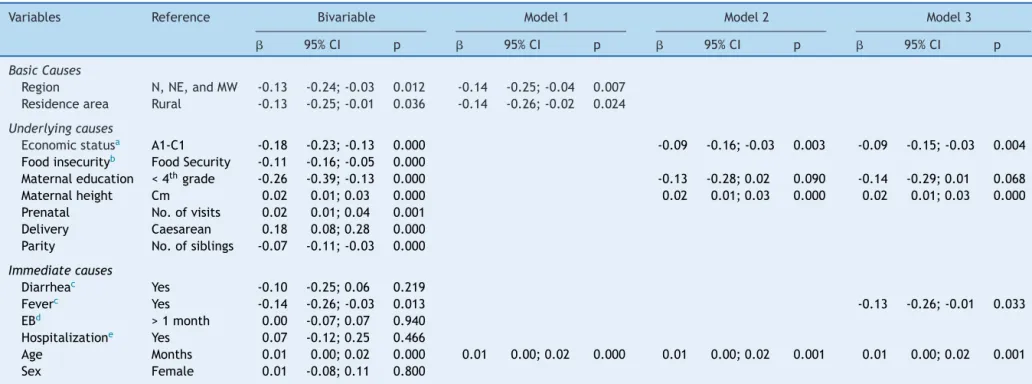
BothbasiccauseswereinverselyassociatedwiththeCWG (Table2---Model1).However,thisassociationwaslostafter adjustingthemodelforunderlyingcauses(Model2).When adjustedforimmediatecauses(Model3),economicstatus (-0.09[-0.15; -0.03]),maternal education(-0.14 [-0.29; -0.01]),andfeverinthepasttwoweeks(-0.13[-0.26;-0.01]) wereinverselyassociatedwithchildren’sweightgain. How-ever,each1cmincrementinmaternalheightwasassociated withanincreaseof0.02SD(0.01;0.03)inchildren’s post-natalweightgain.
Discussion
UsingdatafromthePNDS-2006/07,themostrecentsurvey withnationalrepresentativenessconductedinBrazil,itwas possibletoidentifythelevel ofassociation betweenaset offactors--- indifferenthierarchicallevelsofdetermination --- andpostnatalweightgainamongBrazilianinfants.Itwas foundthatlowereconomic statusandmaternal education andfeverinthepasttwoweekshadanegativeimpacton postnatalweightgain,andthatmaternal heightwas posi-tivelyassociatedwithCWG.
Although geographical factors were highly associated
withCWG in Model 1, when the maternal and household
characteristics were introduced in the hierarchicalmodel (Model2),theassociationbetweengeographicalfactorsand CWGdisappeared,andwasreplacedbyeconomicstatusand highermaternalheight;lowmaternal educationpresented onlyamoderateassociation.However,whenthethirdlevel (immediatecauses)wasintroducedintotheanalysis,fever remainedassociatedwithCWGandthelevelofassociation betweenlowmaternaleducationandCWGincreased.
Thetrajectoryofgrowthismediatedbyacomplex net-workofnon-mutuallyexclusivefactors,actingatdifferent levels of causation, from social, economic, and political determinants;followed byaccesstohealth services,food security,income,andeducationallevel;toindividualfactors relatedtotheburdenofdisease,eating/feedingpractices, metabolicprogramming,andgeneticfactors.2,3,20
The presentresults demonstratedthatlowincomeand maternaleducationallevelsarestillkeyfactorstoweight faltering. However, contrary to expected, geographical characteristics were not independent factors associated withCWG.This lackof associationmaybea consequence ofthecoverageexpansionofthepublicprimaryhealthcare systeminBrazil8and/ortheintensemigratoryprocessfrom
thepooresttotherichest regionsandfromruraltourban areas.21However,thisstatementmaynotholdtruefor
geo-graphicaldisparitieswithinneighborhoodsorcities.22,23
Besides geographicalfactors,thelack ofassociation of CWGanddiarrhea can alsobeexplained by the improve-ment of health and sanitation systems. The increased access to health services enables the provision of ade-quaterehydrationandantibiotictherapy toinfants,which prevents important acute weight loss and/or promotes faster recovery.8,24,25 Moreover, oneof the componentsof
Silveira
JA
et
al.
Table1 CharacteristicsofBrazilianinfantsfromtheBrazilianChildren’sandWomen’sDemographicandHealthSurvey---PNDS---2006/07.
Characteristics na orPb 95%CI Characteristics na orPb 95%CI
Biologicalcharacteristics Maternalheight(cm) 1,754 157.7 157.1;158.3
Age(months) 1,763 11.2 10.6;11.7 Prenatal(No.ofvisits)e 1,707 7 6;9
Gender(%) 1,763 Delivery(%) 1,762
Boys 928 52.4 47.8;57.0 Caesarean 772 45.3 40.1;50.6
Girls 835 47.6 43.0;52.2 Other 990 54.7 49.4;59.9
Birthweight(kg) 1,763 3.25 3.21;3.30 Parity(No.ofdeliveries)e 1,763 2 1;3
WAZatbirth 1,763 -0.13 -0.22;-0.03 FoodandNutritionSecurity(%) 1,710
WAZatsurvey 1,763 0.17 0.08;0.25 Security 879 53.8 48.7;58.8
Nutritionalstatusatsurvey(%) 1,763 Mildinsecurity 473 28.4 24.1;33.0
Underweight(WAZ<-2) 61 2.9 1.9;4.5 Moderateinsecurity 230 13.1 9.8;17.3 Normalweight(WAZ±2) 1,604 93.3 91.3;94.8 Severeinsecurity 128 4.7 3.6;6.2 Overweight(WAZ>2) 98 3.8 2.7;5.2
BasicCauses ImmediateCauses
Region(%) 1,763 Diarrhea(%)c 1,760
SandSE 647 54.2 48.9;59.4 Yes 233 12.2 9.8;15.1
N,NE,andMW 1,116 45.8 40.6;51.1 No 1,527 87.8 84.9;90.2
Residencearea(%) Fever(%)c 1,761
Urban 1,200 83.2 78.4;87.0 Yes 450 26.2 22.8;29.8
Rural 563 16.8 12.9;21.6 No 1,311 73.8 70.2;77.2
Hospitalizationd 1,763
UnderlyingCauses Yes 139 7.8 5.7;10.6
Economicstatus(%) 1,550 No 1,624 92.2 89.4;94.3
A1-C1(richest) 486 34.6 29.0;40.7 Exclusivebreastfeeding(%) 1,477
C2 356 23.5 19.0;28.6 <1month 502 31.8 27.2;36.8 D 446 29.1 24.4;34.2 1-4months 484 33.6 28.9;38.6 E 265 12.9 10.3;16.0 >4months 491 34.6 30.4;39.1
Maternaleducation(%)
<4thgrade 378 17.7 14.6;21.3 ≥4thgrade 1,379 82.3 78.6;85.4
,mean;P,prevalence;CI,confidenceinterval;WAZ,weight-for-ageZ-score;S,South;SE,Southeast;N,North;NE,Northeast;MW,Midwest. a Numberofsubjectsindatabase.
b Meanorprevalencebasedontheweightedsample. c Inthepasttwoweeks.
W
eight
gain
among
Brazilian
infants
289
Table2 Linearmodelsofassociationbetweenenvironmentalandindividualfactorsandconditionalweightgain(CWG)amongBrazilianinfants--- PNDS-2006/07.
Variables Reference Bivariable Model1 Model2 Model3
 95%CI p  95%CI p  95%CI p  95%CI p
BasicCauses
Region N,NE,andMW -0.13 -0.24;-0.03 0.012 -0.14 -0.25;-0.04 0.007
Residencearea Rural -0.13 -0.25;-0.01 0.036 -0.14 -0.26;-0.02 0.024
Underlyingcauses
Economicstatusa A1-C1 -0.18 -0.23;-0.13 0.000 -0.09 -0.16;-0.03 0.003 -0.09 -0.15;-0.03 0.004
Foodinsecurityb FoodSecurity -0.11 -0.16;-0.05 0.000
Maternaleducation <4thgrade -0.26 -0.39;-0.13 0.000 -0.13 -0.28;0.02 0.090 -0.14 -0.29;0.01 0.068
Maternalheight Cm 0.02 0.01;0.03 0.000 0.02 0.01;0.03 0.000 0.02 0.01;0.03 0.000 Prenatal No.ofvisits 0.02 0.01;0.04 0.001
Delivery Caesarean 0.18 0.08;0.28 0.000 Parity No.ofsiblings -0.07 -0.11;-0.03 0.000
Immediatecauses
Diarrheac Yes -0.10 -0.25;0.06 0.219
Feverc Yes -0.14 -0.26;-0.03 0.013 -0.13 -0.26;-0.01 0.033
EBd >1month 0.00 -0.07;0.07 0.940
Hospitalizatione Yes 0.07 -0.12;0.25 0.466
Age Months 0.01 0.00;0.02 0.000 0.01 0.00;0.02 0.000 0.01 0.00;0.02 0.001 0.01 0.00;0.02 0.001 Sex Female 0.01 -0.08;0.11 0.800
Model1:n=1,763---adjustedforageandsex;Model2:n=1,448---adjustedforModel1,householdfoodinsecurity,prenatal,typeofdelivery,andparity;Model3:n=1,447---adjusted forModel2andsourceofbirthweightdata(maternitycard/mother’srecall).
EB,exclusivebreastfeeding. a Ordinalvariable:A1-C1,C2,D,E.
b Ordinalvariable:foodsecurity,mildfoodinsecurity,moderatefoodinsecurity,severefoodinsecurity. c Inthepasttwoweeks.
Brazil has substantially reduced nutritional disorders and mortalityratesfromacuteinfections.8,25
The associations found here depict a society in transi-tion,wheregeographicalcharacteristics or acutediseases areno longer major determinants of negativenutritional disorders, but low socioeconomic status and educational attainment still are. It contrasts with high-income coun-tries,where weightfaltering is most attributedtohigher parity, low appetite, weaning/feeding/eating difficulties, or lack of positive interactions between infants and parents.26 This study also observed an inverse and
sig-nificant association between parityand CWG;however, it was not sustained after adjusting for the other factors. This may have occurred due tothe relationship between higherparity and lower incomeand educationallevels in Brazil.27
Although food insecurity and incomelevel are related variables,inthepresentanalysiseconomicstatusperformed betterasexplanatoryvariableofCWG.Theauthorsattribute thistothefactthatthequestionsintheEBIAarerelatedto anyeventoffoodinsecurityinthepastthreemonths, with-outconsidering thefrequencyofevents; furthermore,the processforafamilytoimprovetheireconomic statusmay requireconsiderabletime(evengenerations).TheCWGwas sensitivetosuchdifferenceand,therefore,itisreasonable toconsiderthatinfants wereexposedtothesameor sim-ilareconomicenvironmentdescribedatsurveysincebirth, considering that thoseliving in less privileged households experiencedpoorerpostnatalweightgaincomparedtothose fromwealthyfamilies.
The variation in the effect size and the level of asso-ciation between low maternal educationand CWG in the bivariate and multivariate analyses was noteworthy. The samerationaledescribedpreviouslycanbeusedtoexplain suchvariation,sinceeconomicstatusandeducationallevel arerelatedvariables.However,therewassome effecton CWGthatwasnotfullyexplainedbyeconomicstatus,and after addingthe occurrence of fever in the previous two weeks,thelevelofassociationbetweenlowmaternal edu-cationandpoorweightgainincreased.
Lack of maternal educationis a recognized risk factor for negative health outcomes28 and, in this context, this
resultwasinterpretedasthematernal inabilitytoprovide adequatecare,eitherduetotheinabilitytorecognizethe developmentofan infectious process,or delay inseeking health services. The impact on weight gain is a conse-quenceofincreasedenergyexpenditureandreducedfood intake, due to the anorectic effect of pro-inflammatory cytokinesonappetiteregulatoryhormones(i.e.leptin)and neuropeptides(i.e.neuropeptideY)duringtheacutephase response.29Consideringthefamily’ssocioeconomicstatusin
thisequation---thatis,livinginanunhealthyenvironment ---these infants mayhave experienced multiple infectious eventsduringtheirlives.
Finally,thepositiveassociationbetweenmaternalheight andchildweightgainshouldnotbeinterpretedsolelyasa consequenceofsharedgeneticcharacteristics,butalsoasa milieuofinadequatehealthandnutritionduringawoman’s childhood (compromising her growth and, consequently, reproductive organ size) and pregnancy (insufficient pro-vision of nutrients impairing intrauterine growth).3 This
relationshiphighlightstheimportanceofimprovingnotonly
infants’ butalso women’shealthand nutritionalstatusto breakthiscycle.
Using data from the ALSPAC cohort, Din et al.30
com-paredthepatternsofweightgainamongchildrenwhohad ‘‘early weight faltering’’ (< 5th percentile of weight gain at 8 weeks),‘‘late weight faltering’’(< 5th percentile of weight gain at 9 months), and a control group. Similarly tothe present study,theyobserveda positiveassociation betweenageandCWG.Thepatternofweightgainwas dif-ferentdependingonwhentheweightfalteringoccurred,but bytheageof13yearsthesechildrensubstantiallyrecovered weight;however,theirstandardizedmeanweightandheight wasstatisticallydifferentfromthecontrolgroup.
Such findings highlight the importance of preventing nutritionaldisordersduringthefirst1,000daysoflife---from conceptionto2yearsofage---becausedamagesthatoccurin thisperiodwillbereflectedinlong-termhealthandhuman capitaloutcomes.3
Themainstrengthsofthisstudyincludeitsbasisonthe most recent representative sample of the Brazilian popu-lation,designed andconductedby ateamof experienced researchers,whousedCWGtoevaluatechildren’sgrowth; thus,theseresultshavenotonlyinternalvalidity,butalso canbegeneralizedtoallBrazilianinfantsand,althoughthe PNDSdatesfrom2006/07,itisconsideredthatthefindings arestillvalid,sincenomajorpoliticalorstructuralchanges haveoccurredinBraziliansocietyinthelastseveralyears. However,anewPNDS isneeded toupdatethe knowledge about the current children’snutritional and health status inBrazil, allowingcomparisonswithprevious nationaland internationalhealthsurveys.
It is important to consider two limitations in the interpretation of this study. First, although the PNDS-2006/07 included slums in the household sample, it did notconsideredinstitutionalized(i.e.hospitalororphanage), homeless,orchildrenlivinginsettlements;second,the mor-tality bias,which is related tothedeath ofchildren who werebornunderinadequateconditionsorwereexposedto adverseconditionsduringthegestationalperiod.Therefore, thesefindingscannotbegeneralizedtochildrenlivingunder thedescribedcircumstances,andfurthermore,these limi-tationsmayhave underestimatedthemagnitudeandlevel ofassociationoftheresults.
Contrarytothe attainednutritionalstatus (i.e.,WAZ), theCWGisgenerated consideringthe birthweight,which allowsfortheanalysisofhowmuchachild deviatedfrom his/her expected weight gain, considering his/her peers, providingabettermeasureofenvironmentalinfluencesof growth.However,thisis ameasureexclusive toacademic research,andcannotfeasiblybeusedinaclinicalsetting.
WeightgainamongBrazilianinfants 291
Theseresultsshowedthatpovertyandlowerhuman capi-talarestillkeyfactorsassociatedwithpoorpostnatalweight gain. The approach used was sensitive in characterizing inequalities among different socioeconomic contexts and in identifying factors at different levels of determination associatedwithCWG.
Funding
The Brazilian Children’s and Women’s Demographic and
HealthSurvey2006/07wasfundedbytheMinistryofHealth andexecutedbytheBrazilianCenterforAnalysisand Plan-ning (CEBRAP).The authorJSreceiveda scholarshipfrom
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo
(FAPESP)protocolno.2011/17736-4.TheauthorAPreceived ascholarshipfromCoordenac¸ãodeAperfeic¸oamentode Pes-soalde Nível Superior (CAPES). The authorJT is partially fundedbyConselhoNacionaldeDesenvolvimentoCientífico eTecnológico(CNPq).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.World Health Organization. Physical status: the use and interpretationofanthropometry-reportofaWHOExpert Com-mittee.WHOTechnicalReportSeries:WHOLibrary;1995. 2.UnitedNationsChildren’s,Fund.,Strategyforimproved
nutri-tionofchildrenandwomenindeveloping,countries.NewYork: UNICEF;1990.
3.Martorell R, Zongrone A. Intergenerational influences on childgrowthand undernutrition. PaediatrPerinatEpidemiol. 2012;26:S302---14.
4.Victora CG,de Onis M,Hallal PC, Blossner M, ShrimptonR. Worldwidetimingofgrowthfaltering:revisitingimplicationsfor interventions.Pediatrics.2010;125:e473---80.
5.BlackRE,AllenLH,BhuttaZA,CaulfieldLE,deOnisM,Ezzati M,etal.Maternalandchildundernutrition:globalandregional exposuresandhealthconsequences.Lancet.2008;371:243---60. 6.VictoraCG,AdairL,FallC,HallalPC,MartorellR,RichterL, etal.Maternalandchildundernutrition:consequencesforadult healthandhumancapital.Lancet.2008;371:340---57.
7.Brasil,MinistériodaSaúde.PolíticaNacionaldeAlimentac¸ãoe Nutric¸ão.Brasília:MinistériodaSaúde;2012.
8.VictoraCG,AquinoEM,doCarmoLealM,MonteiroCA,Barros FC,SzwarcwaldCL.MaternalandchildhealthinBrazil:progress andchallenges.Lancet.2011;377:1863---76.
9.RamalingaswamiV.Newglobalperspectivesonovercoming mal-nutrition.AmJClinNutr.1995;61:259---63.
10.HeeringaSG,WestBT,BerglundPA.Appliedsurveydataanalysis. 1stedBocaRaton:ChapmanandHall/CRC;2010.
11.BerquóE,GarciaS,LagoT.Aspectosmetodológicos-Pesquisa NacionaldeDemografiaeSaúdedaCrianc¸aedaMulher---PNDS
2006.[cited04Apr2014].Availablefrom:http://bvsms.saude. gov.br/bvs/pnds/img/MetodologiaPNDS2006.pdf
12.WorldHealth,Organization.,WHO.,Child GrowthStandards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and, development. Geneva: The World Health Organization; 2006.
13.ColeTJ.Conditionalreferencechartstoassessweightgainin Britishinfants.ArchDisChild.1995;73:8---16.
14.ColeTJ.Presentinginformationongrowth distanceand con-ditionalvelocityinonechart:practicalissuesofchartdesign. StatMed.1998;17:2697---707.
15.Associac¸ão Brasileira de Empresas de Pesquisa (ABEP).
Critério de Classificac¸ão Econômica Brasil (CCEB). 2009.
[cited 04 Apr 2014]. Available from: http://www.abep.org/
novo/FileGenerate.ashx?id=251
16.Brasil,MinistériodaSaúde.PesquisaNacionaldeDemografiae
SaúdedaCrianc¸aedaMulher---PNDS2006:dimensõesdo
pro-cessoreprodutivoedasaúdedacrianc¸a.MinistériodaSáude:
Brasília, 2009. [cited04 Apr 2014]. Available from: http://
bvsms.saude.gov.br/bvs/publicacoes/pndscriancamulher.pdf 17.Kepple AW,Segall-CorreaAM.Conceptualizingandmeasuring
foodandnutritionsecurity.CienSaudeColet.2011;16:187---99. 18.VictoraCG,HuttlySR, FuchsSC,OlintoMT.Theroleof con-ceptualframeworksinepidemiologicalanalysis:ahierarchical approach.IntJEpidemiol.1997;26:224---7.
19.GardnerMJ,AltmanDG.ConfidenceintervalsratherthanP val-ues:estimationratherthanhypothesistesting.BrMedJ(Clin ResEd).1986;292:746---50.
20.BlackRE, Victora CG, WalkerSP, BhuttaZA, ChristianP, de Onis M, et al. Maternal and child undernutrition and over-weight in low-income and middle-income countries. Lancet. 2013;382:427---51.
21.Brito F.Thedisplacementof theBrazilianpopulation tothe metropolitanareas.EstudAv.2006;20:221---36.
22.CarterMA,DuboisL,TremblayMS,TaljaardM.Theinfluence ofplaceonweightgainduringearlychildhood:a population-based,longitudinalstudy.JUrbanHealth.2013;90:224---39. 23.SprayAL,EddyB,HippJA,IannottiL.Spatialanalysisof
under-nutritionofchildreninléogâneCommune.HaitiFoodNutrBull. 2013;34:444---61.
24.MelliLC,WaldmanEA.Temporaltrendsandinequalityin under-5mortalityfromdiarrhea.JPediatr(RioJ).2009;85:21---7. 25.VictoraCG.Diarrheamortality:whatcantheworldlearnfrom
Brazil?JPediatr(RioJ).2009;85:3---5.
26.ShieldsB,WacogneI,WrightCM.Weightfalteringandfailureto thriveininfancyandearlychildhood.BMJ.2012;345:e5931. 27.Huttly SRA, BarrosFC,Victora CG,Lombardi C,Vaughan JP.
Subsequentpregnancies:whohasthemandwhowantsthem? ObservationsfromanurbancenterinSouthernBrazil.RevSaude Publica.1990;24:212---6.
28.ChenY,LiH.Mother’seducationand childhealth:istherea nurturingeffect?JHealthEcon.2009;28:413---26.
29.ShilsME, Shike M,RossAC,CaballeroB,Cousins RJ.Modern nutritioninhealthanddisease.10thed.Baltimore:Lippincott
Williams&Wilkins;2005.