JPediatr(RioJ).2015;91(3):213---233
www.jped.com.br
REVIEW
ARTICLE
Application
of
tactile/kinesthetic
stimulation
in
preterm
infants:
a
systematic
review
夽
,
夽夽
Vanessa
C.
Pepino
a,∗,
Maria
Aparecida
Mezzacappa
baPrograminChildandAdolescentHealthScience,UniversidadeEstadualdeCampinas(UNICAMP),SãoPaulo,SP,Brazil
bDivisionofNeonatology,DepartmentofPediatrics,FacultyofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),
SãoPaulo,SP,Brazil
Received19September2014;accepted6October2014 Availableonline9February2015
KEYWORDS
Preterminfants; Massage; Review; Weightgain; Tactile/kinesthetic stimulation
Abstract
Objective: Toverifythemethodsused bytheclinicaltrialsthatassessedtheeffectof tac-tile/kinestheticstimulationonweightgaininpreterminfantsandhighlightthesimilaritiesand differencesamongsuchstudies.
Sources: Thisreviewcollectedstudiesfromtwodatabases,PEDroandPubMed,inJulyof2014, inadditiontobibliographies.Tworesearchersassessedtherelevanttitlesindependently,and thenchosewhichstudiestoreadinfullandincludeinthisreviewbyconsensus.Clinicaltrials thatstudiedtactilestimulationormassagetherapywhetherornotassociatedwithkinesthetic stimulation ofpreterm infants;thatassessedweight gainafter theintervention;thathada controlgroupandwerecomposedinEnglish,Portuguese,orSpanishwereincluded.
Summaryofthefindings: Atotalof520titleswerefoundand108wereselectedformanuscript reading.Repeatedstudieswereexcluded,resultingin40differentstudies.Ofthese,31met alltheinclusioncriteria.Thereweremanydifferencesintheapplicationoftactile/kinesthetic stimulationtechniquesamongstudies,whichhinderedtheaccuratereproductionofthe proce-dure.Also,manystudiesdidnotdescribetheadverseeventsthatoccurredduringstimulation, thecourseofactiontakenwhensucheventsoccurred,andtheireffectontheoutcome.
Conclusions: Thesestudiesmadearelevantcontributiontowardsindicatingtactile/kinesthetic stimulation asapromisingtool.Nevertheless,therewas nostandardforapplicationamong them.Futurestudiesshouldraisethelevelofmethodologicalrigoranddescribetheadverse events. Thismay permitotherresearchersto bemoreawareofexpectedoutcomes, anda standardtechniquecouldbeestablished.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:PepinoVC,MezzacappaMA.Applicationoftactile/kinestheticstimulationinpreterminfants:asystematic
review.JPediatr(RioJ).2015;91:213---33.
夽夽
StudyconductedatDepartmentofPediatrics,FacultyofMedicalSciences,UniversidadeEstadualdeCampinas(UNICAMP),SãoPaulo,
SP,Brazil
∗Correspondingauthor.
E-mail:[email protected](V.C.Pepino). http://dx.doi.org/10.1016/j.jped.2014.10.005
214 PepinoVC,MezzacappaMA
PALAVRAS-CHAVE
Neonatosprematuros; Massagem;
Análise; Ganhodepeso; Estimulac¸ão tátil-cinestésica
Aplicac¸ãodaestimulac¸ãotátil-cinestésicaemneonatosprematuros:análise sistemática
Resumo
Objetivo: Verificar quaismetodologiasforamutilizadasporensaios clínicosqueavaliaramo efeitodaestimulac¸ãotátil-cinestésicasobreoganhodepesodeneonatosprematurosedestacar asdiferenc¸asesemelhanc¸asentreessesestudos.
Fontesdosdados: Estaanálisecoletouestudosdeduasbasesdedados,PEDroePubMed,em julhode2014,alémdebibliografias.Doispesquisadoresavaliaramostítulosrelevantes indepen-dentementee,então,escolheramconsensualmentequaisestudosseriamlidoscompletamente eincluídosnestaanálise.Foramincluídososensaiosclínicosqueestudaramaestimulac¸ãotátil ouamassagemterapêuticaassociadaounãoàestimulac¸ãocinestésicaemneonatosprematuros eavaliaramoganhodepesoapósaintervenc¸ão,tiveramumgrupodecontroleeforamescritos eminglês,portuguêsouespanhol.
Síntesedosdados: Foram encontrados 520 títulos no total, e foram selecionados 108 para leitura.Osestudosrepetidosforamexcluídos,resultando em40estudosdiferentes.Destes, 31atenderamatodososcritériosdeinclusão.Hámuitasdiferenc¸asnaaplicac¸ãodastécnicas deestimulac¸ãotátil-cinestésicaentreosestudos,oqueprejudicaareproduc¸ãoprecisado pro-cedimento.Alémdisso,muitosestudosnãodescreviamoseventosadversosocorridosdurante aestimulac¸ão,oprocedimentorealizadoquandoesseseventosocorriameseuefeitosobreo resultado.
Conclusões: Essesestudosfizeramumacontribuic¸ãorelevanteaoincluiraestimulac¸ão tátil-cinestésicacomoumaferramentapromissora.Contudo,nãohouvepadrãodeaplicac¸ãoentre eles.Estudosfuturospodemaumentaroníveldorigormetodológicosedescreveroseventos adversos.Issopodepermitirqueoutrospesquisadorestenhammaisciênciadoqueesperare assimestabelecerumatécnicapadrão.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Preterm infants (PI) are exposed daily to many stressors intheneonatalintensive care unit(NICU)inherenttothe criticalcaretheyneedtosurvive.Themannerandintensity of exposure vary according tothe individual PI condition andresponse. It has alreadybeen shown that such expo-sureleads tostructuraland functionalchangesin specific areas of the brain, affecting its development,1 language, andsocial-emotionalandadaptivebehavior.2
Tactilestimulation(TS)ormassagetherapy(MT), some-timesassociatedwithkinestheticstimulation(KS),is used in PI along withthe standard clinical treatment. TS have beentheobjectof clinicalstudiessincethe1960s,3when it was proposed as a means of encouraging PI growth and development.3---10 Additionally, recent studies have shown thatinterventionssuch astactile/kinesthetic stim-ulation(TKS)havetheaddedbenefitofreducingbehavioral manifestationsofstress.11
The objective of this systematic review was to verify whichmethodologieswereusedbyclinicaltrialsthatstudy theeffects ofsome types ofTS/MT, whether or not asso-ciatedwith KS, on weight gain of PI. Clinicaltrials were selectedthatstudiedtheeffectsonweightgain,asthisisa determinantvariablefordischargefromtheNICU.The dif-ferencesandsimilaritiesbetweenthemethodsusedbythe reviewedclinical trials werehighlighted in an attempt to improvethemethodologicalqualityoffuturetrials.
Methods
Twodatabasesweresearchedforthissystematicreview:the PhysiotherapyEvidenceDatabase(PEDro)12 andtheUnited StatesNationalLibraryofMedicineoftheNationalInstitutes ofHealth(PubMed).13Allstudieslistedonthedateofsearch wereaccessed.
The PEDro database was searched by specifying the following fields in the advanced search option: therapy (stretching, mobilization,manipulation, massage); subdis-cipline(pediatrics),andmethod(clinicaltrial).
PubMedwassearchedusingsixkeywordcombinations,as follows:
--- Search1:massageprematurenewborn
--- Search2:tactilekinestheticstimulationpremature --- Search3:tactilestimulationpremature
--- Search4:massageprematuregrowth
--- Search5:kinestheticstimulationprematuregrowth --- Search6:tactilekinestheticstimulation
prematuregrowth
Tactilekinestheticstimulationinpreterminfants 215
Inclusion
criteria
Two independent researchers preselected the articles accordingtotheirtitles.In caseof doubt,the articlewas included in the selection processby consensus.The pres-elected titles were then stored in a file according to the databasetheywerefound,andtheirabstractsortextswere downloadedforassessment.Oncedownloaded,thearticles werethoroughlyreadtoselectthosethatmettheinclusion criteriadetailedbelow.
Thepresentreviewincludedallclinicaltrialsthatstudied theprovision of TSor MT,whether or notassociatedwith KS, for PI in the NICU, assessed PI weightgain after the intervention,hadacontrolgroupthatdidnotreceive any interventioninadditiontothestandardtreatmentprovided bytheNICU,andwerecomposedinEnglish,Portuguese,or Spanish.
Results
A total of 508 articles werefound in the two abovemen-tioneddatabases.Seventeenarticleswerefullyreadamong the 206 articles found in the PEDro database, of which eightmettheinclusioncriteria.ThefirstsearchonPubMed resultedin126titles,ofwhich30wereselectedand18met theinclusioncriteria.ThesecondsearchonPubMedresulted in16titles,ofwhichtenwereselectedandeightmetthe inclusioncriteria. The third searchonPubMed resultedin 86titles,ofwhich14wereselectedandtenmetthe inclu-sioncriteria. The fourth searchonPubMed resulted in 49 titles, of which 23 were selected and 16 met the inclu-sion criteria. The fifth search on PubMed resulted in 14 titles,ofwhichninewereselectedandsixmettheinclusion criteria. ThesixthsearchonPubMedresulted in11titles, of which eight were selected and five met the inclusion criteria.
However,another12titlesfoundinthereferencesofthe articlesthatmettheinclusioncriteriawereanalyzed,and ofthese,fourwereincluded,fivewereexcluded,andthree were notfound. Table 1 shows the titles and where they werefound.
In summary, 520 titles werefound; the repeated stud-ieswereeliminated,resultingin31thatmettheinclusion criteriaofthepresentreview(Table1).
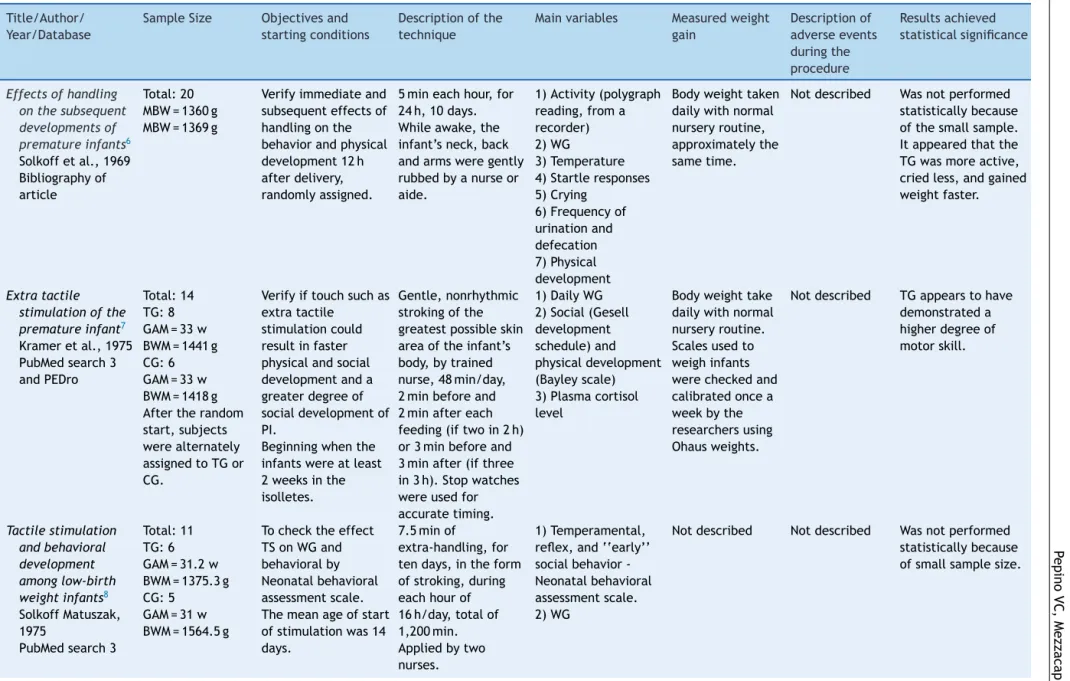
TS/MTwasdoneinmanydifferentways,3,9,10,14---18andthe mostof thestudiesdid notprovideadetaileddescription ofhowtoproceedduringthestimulationifadverseevents occur, nor of the possible effects of these events on the outcomes.
Analysis of the techniques used by different studies showedthatolder studies,suchasSolkoffetal.,6 Kramer etal.,7andSolkoff&Matuszak8didnotspecifywhichparts of the body were stimulated or how often. The pressure usedduringtheinterventionanditsdurationvariedgreatly betweenthesestudies.
White&Labarba3werethefirsttocombineTSandKS.In 1981,Rausch9dividedTKSintothreephasesoffiveminutes eachandappliedTKSonlywhenthePIwereawake,without changingtheirpositionintheincubator.BothLee19and Fer-reira& Bergamasco20 followed these procedures.Rausch9
suggestedthatnewstudiesshouldprovidetheintervention forat leasttendays,becauseweightgainincreasedafter thisperiod.Rausch’s9studywasthefirsttoshowsignificantly fasterweightgaininPIsubmittedtoTKSandtodescribethe techniqueusedindetail.
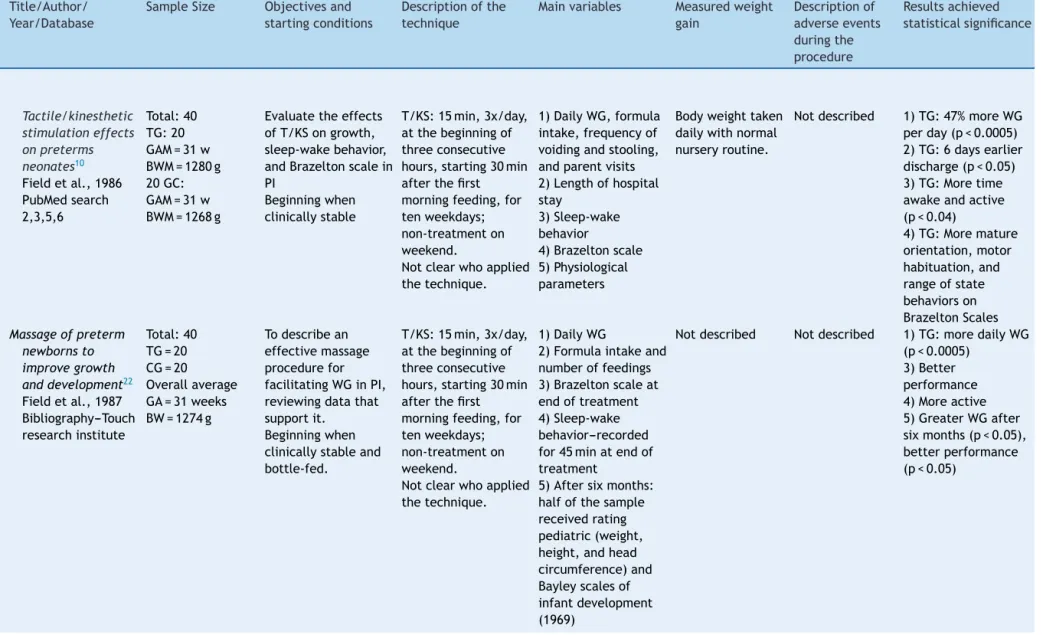
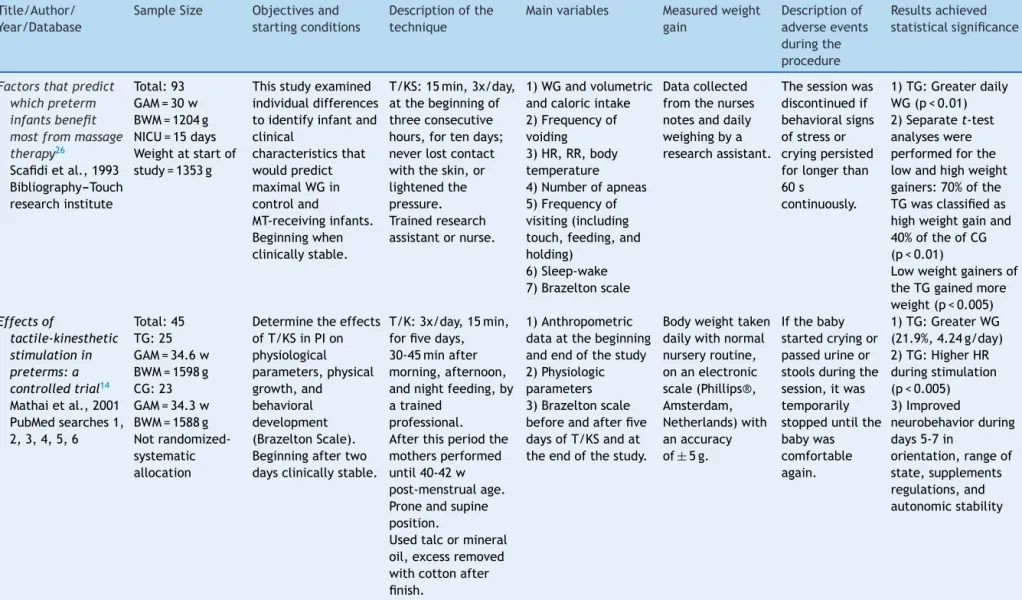
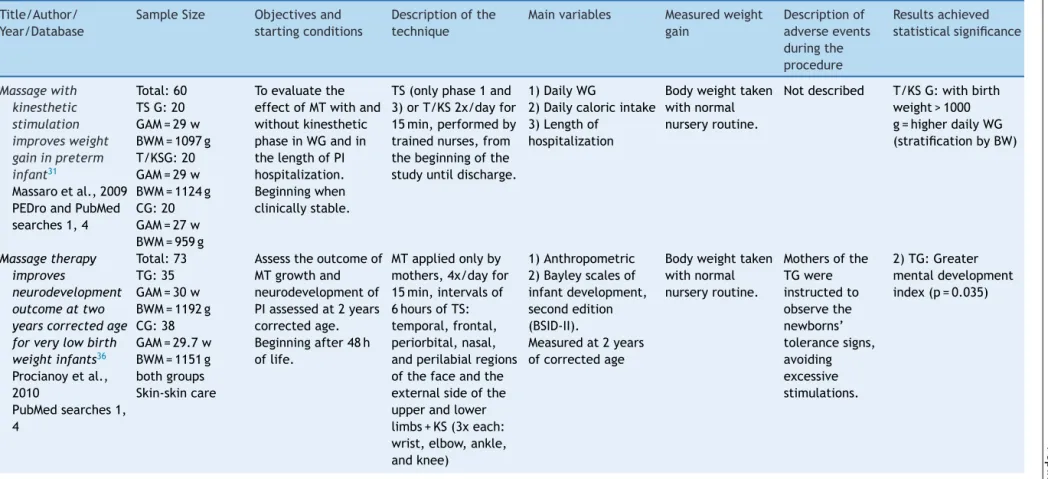
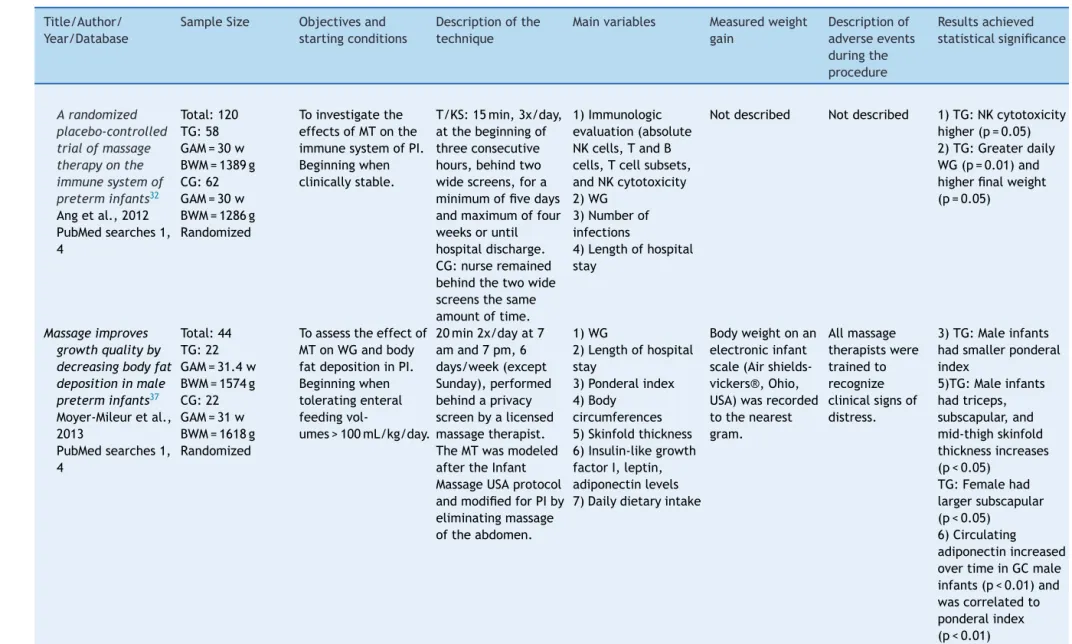
Scafidietal.21standardizedthethreefive-minutephases proposedby Rausch9 intoprone TS+supine KS+proneTS. Fourteen of the 31 studies that met the inclusion crite-ria for the present review used the technique described by Field et al. 10 in 1986; 11 of the 14 were conducted by Field’s team10,21---30 in the same institution and three wereperformedby other researchers,namelyLee,19 Mas-saro et al.,31 and Ang et al. 32 The intervention was usuallyperformed after the first feeding in the morning. In1990, Field& Schanberg24 provided theintervention at thebeginningofthreeconsecutivehours,afterthemidday feeding.
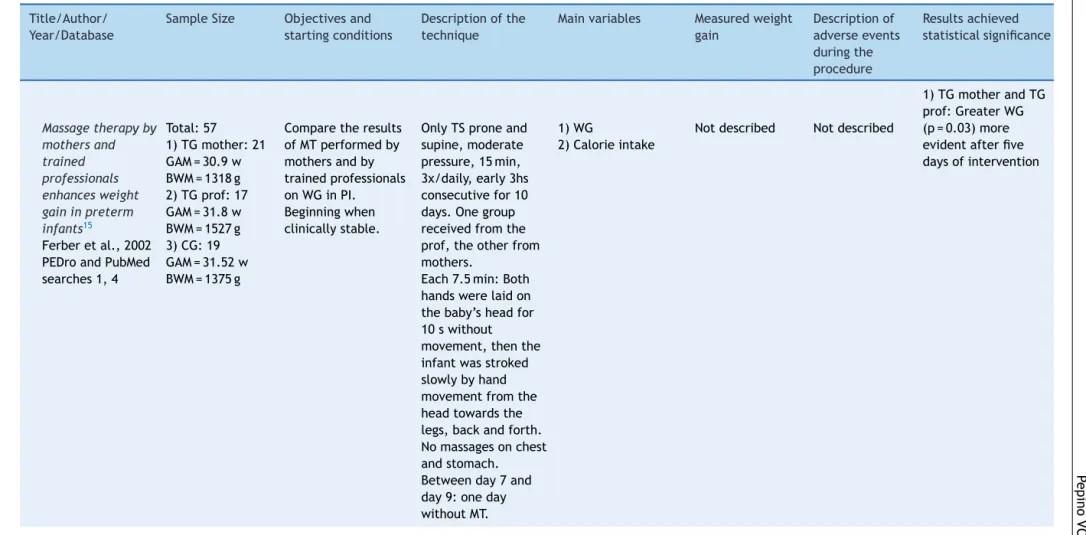
Mathai et al. 14 introduced a new way of providing TKS,asfollows:theinterventionwasdoneafterthe morn-ing,midday,andeveningfeedingintheprone(TS)+supine (TS)+supine (KS) positions, which was repeatedby Arora etal.33Likeotherstudies,theyalsousedsometypeofoil toreducefrictiononthePI’sskin.14,17,33---35Insomestudies, onlythemothersprovidedKTS.16,35,36
Ferberetal.15suggestedthatduringthefirsttenseconds of TS, the caregiver should only rest his hand on the PI, avoidingmovements.
Dieteretal.27 wasthefirsttoprovideTKSforonlyfive days,showingthatthiswasenoughtoincreasetherateof weightgainsignificantlycomparedwiththecontrolgroup.
Diego et al. 28 demonstrated that moderate KTS pres-surepromotedbetteroutcomesthantheplacebogroupwho receivedlightKTSpressure.Also,inanothertime,traineda fewtherapistsandsuggestedthatthetechniquewas effec-tive,regardlessoftherapist.29
Massaroetal.31testedKTSandTSseparatelyindifferent groupsofinfantsandfoundthatKTSappearstobebetter, butthedifferencewasnotsignificant.
Fucile & Gisel18 used the same trained researcher to provide the intervention and introduced oral stimulation (OS)inadditiontoKTS.TheyfoundthatOSdidnotincrease the rate of weightgain and attributed this result to the shorterperiod dedicated toeach intervention, suggesting thatthedurationofthesensoriomotor inputiscriticalfor improvingdefinedoutcomes.
Ferreira&Bergamasco20 usedgentletechniqueswithno rigidsequence,onlywhenthePIwasawake.
Moyer-Mileuretal.37 usedtheInfantMassageUSA pro-tocol,buttheymodifiedforPI,eliminatingmassageofthe abdomen.
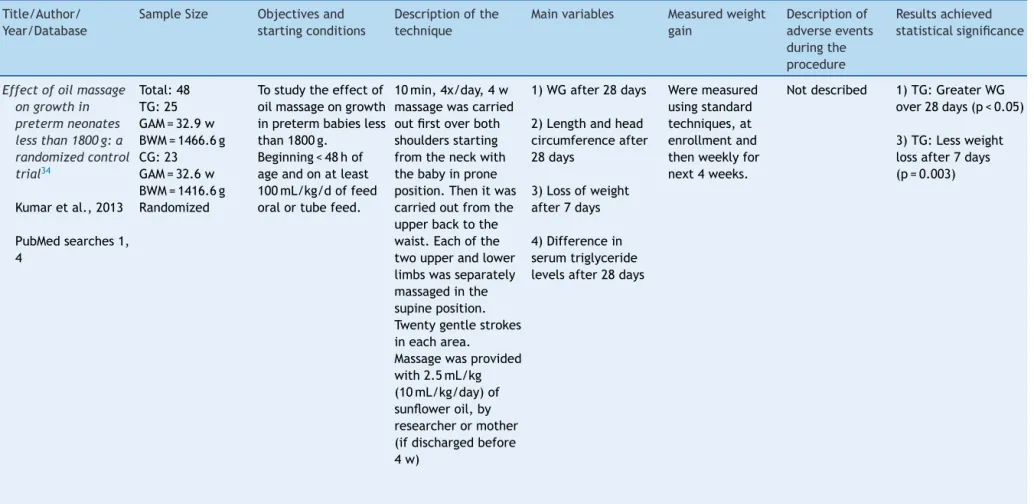
Kumar etal. 34 demonstratedthat PI who receivedoil massage soon after birth had less weight loss in the first week,probablyduetoundetectablewaterlossthroughthe skinduetoblockageofporesandsweatglands.Also,early oilapplication probablyleadstobettertemperature regu-lationandlesscaloricexpenditureduetocoldstress.
216
P
epino
VC,
Mezzacappa
MA
Table1 Descriptionsoftheincludedstudies.
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Effectsofhandling onthesubsequent developmentsof prematureinfants6 Solkoffetal.,1969 Bibliographyof article
Total:20 MBW=1360g MBW=1369g
Verifyimmediateand subsequenteffectsof handlingonthe behaviorandphysical development12h afterdelivery, randomlyassigned.
5mineachhour,for 24h,10days. Whileawake,the infant’sneck,back andarmsweregently rubbedbyanurseor aide.
1)Activity(polygraph reading,froma recorder) 2)WG
3)Temperature 4)Startleresponses 5)Crying
6)Frequencyof urinationand defecation 7)Physical development
Bodyweighttaken dailywithnormal nurseryroutine, approximatelythe sametime.
Notdescribed Wasnotperformed statisticallybecause ofthesmallsample. Itappearedthatthe TGwasmoreactive, criedless,andgained weightfaster.
Extratactile stimulationofthe prematureinfant7 Krameretal.,1975 PubMedsearch3 andPEDro
Total:14 TG:8 GAM=33w BWM=1441g CG:6 GAM=33w BWM=1418g Aftertherandom start,subjects werealternately assignedtoTGor CG.
Verifyiftouchsuchas extratactile
stimulationcould resultinfaster physicalandsocial developmentanda greaterdegreeof socialdevelopmentof PI.
Beginningwhenthe infantswereatleast 2weeksinthe isolletes.
Gentle,nonrhythmic strokingofthe greatestpossibleskin areaoftheinfant’s body,bytrained nurse,48min/day, 2minbeforeand 2minaftereach feeding(iftwoin2h) or3minbeforeand 3minafter(ifthree in3h).Stopwatches wereusedfor accuratetiming.
1)DailyWG 2)Social(Gesell development schedule)and physicaldevelopment (Bayleyscale) 3)Plasmacortisol level
Bodyweighttake dailywithnormal nurseryroutine. Scalesusedto weighinfants werecheckedand calibratedoncea weekbythe researchersusing Ohausweights.
Notdescribed TGappearstohave demonstrateda higherdegreeof motorskill.
Tactilestimulation andbehavioral development amonglow-birth weightinfants8 SolkoffMatuszak, 1975
PubMedsearch3
Total:11 TG:6 GAM=31.2w BWM=1375.3g CG:5
GAM=31w BWM=1564.5g
Tochecktheeffect TSonWGand behavioralby Neonatalbehavioral assessmentscale. Themeanageofstart ofstimulationwas14 days.
7.5minof extra-handling,for tendays,intheform ofstroking,during eachhourof 16h/day,totalof 1,200min. Appliedbytwo nurses.
1)Temperamental, reflex,and‘‘early’’ socialbehavior -Neonatalbehavioral assessmentscale. 2)WG
Tactile
kinesthetic
stimulation
in
preterm
infants
217
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Theeffectsoftactile andkinesthetic stimulationon neonatal
developmentinthe prematureinfant3 WhiteLabarba,1976 PubMedsearches2, 3,5,6
Total:12 TG:6 GAM=34.3w BWM=1910g CG:6 GAM=34.2w BWM=1911g
Investigatesome immediateeffects suchasWGandthe developmentoflow birthweightinfants thatreceivedT/KSin atypicalhospital nursery.
Beginningafter48hof age.
15minperiodsevery hourforfour
consecutivehours,for tendays.Rubbingthe infant’sneck, shoulder,arms,legs, chest,andback;and KS.Performedby researcher.
1)WG,numberof feedings,amountof formulaintake. 2)Bodytemperature 3)HR,RR
4)Frequencyof voidingandstooling.
Allinfantswere routinelyweighed threedayseach weekbythe nurserystaff.
Notdescribed 1)TG:MoreWG stimulationeffect (p<0.05)and stimulationxdays interaction(p<0.001) TG:Greateramountof formulaintake (p<0.025)
TG:Fewernumberof feedings/day(p<0.05)
Effectsoftactileand kinesthetic stimulationon prematureinfants9 Rausch,1981 PubMedsearches2, 3,5,6
Total:40 TG:20 CG:20
BW=1000-2000g Notrandomized
Todeterminethe effectsofa10-day regimenofT/KSon caloricintake, stooling,andWG. Beginningat24-48hof age.
15min,3x/day,atthe beginningofthree consecutivehours, starting30minafter thefirstmorning feeding,forten weekdays; non-treatmenton weekend.Performed byresearcher. Withtheinfantawake andkeepingthebaby inposition.
1)WG
2)Frequencyof stooling 3)Caloricintake
Bodyweighttaken dailywithnormal nurseryroutine.
Notdescribed 2)TG:Increaseof formulaintakeondays 6-10(p<0.0001) 3)TG:Increase stoolingfrequency (p<0.004)
Effectsof
tactile/kinesthetic stimulationonthe clinicalcourseand sleep/wake behaviorofpreterm neonates21
Scafidietal.,1986 PEDro
Total:40 TG:20 GAM=31w BWM=1280g CG:20 GAM=31w BWM=1268g
Itwasdesignedto complementthe alreadyexisting literatureofthe effectsofT/KSinPI. Beginningwhen clinicallystable.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,starting30min afterthefirstmorning feeding,forten weekdays; non-treatmenton weekend. Performedby researcher.
Phase1and3inprone positionandphase2in supine.
1)DailyWG 2)Formulaintake, frequencyofvoiding, stooling
3)HR,RR,body temperature 4)Numberofapneic episodes
5)Parentsvisitingand touch
6)Brazeltonscale 7)Sleep-wake behavioral(Thomas Scaleof1975) 8)Lengthofhospital stay
Bodyweighttaken dailywithnormal nurseryroutine.
218
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Tactile/kinesthetic stimulationeffects onpreterms neonates10 Fieldetal.,1986 PubMedsearch 2,3,5,6
Total:40 TG:20 GAM=31w BWM=1280g 20GC: GAM=31w BWM=1268g
Evaluatetheeffects ofT/KSongrowth, sleep-wakebehavior, andBrazeltonscalein PI
Beginningwhen clinicallystable
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,starting30min afterthefirst morningfeeding,for tenweekdays; non-treatmenton weekend.
Notclearwhoapplied thetechnique.
1)DailyWG,formula intake,frequencyof voidingandstooling, andparentvisits 2)Lengthofhospital stay
3)Sleep-wake behavior
4)Brazeltonscale 5)Physiological parameters
Bodyweighttaken dailywithnormal nurseryroutine.
Notdescribed 1)TG:47%moreWG perday(p<0.0005) 2)TG:6daysearlier discharge(p<0.05) 3)TG:Moretime awakeandactive (p<0.04)
4)TG:Moremature orientation,motor habituation,and rangeofstate behaviorson BrazeltonScales
Massageofpreterm newbornsto improvegrowth anddevelopment22 Fieldetal.,1987 Bibliography---Touch researchinstitute
Total:40 TG=20 CG=20 Overallaverage GA=31weeks BW=1274g
Todescribean effectivemassage procedurefor facilitatingWGinPI, reviewingdatathat supportit.
Beginningwhen clinicallystableand bottle-fed.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,starting30min afterthefirst morningfeeding,for tenweekdays; non-treatmenton weekend.
Notclearwhoapplied thetechnique.
1)DailyWG
2)Formulaintakeand numberoffeedings 3)Brazeltonscaleat endoftreatment 4)Sleep-wake behavior---recorded for45minatendof treatment
5)Aftersixmonths: halfofthesample receivedrating pediatric(weight, height,andhead circumference)and Bayleyscalesof infantdevelopment (1969)
Notdescribed Notdescribed 1)TG:moredailyWG (p<0.0005)
Tactile
kinesthetic
stimulation
in
preterm
infants
219
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Effectsofearly multimodal stimulationon pretermnewborn infants39
Benavides-González etal.,1989 PubMedsearches2, 5,6
Total:18 GAM=31.5w BWM=1296g GC:
GAM=32.4w BWM=1211g
Tostudyifthe supplemental stimulationofPI responsesimproves neurobehavioral organization, achievinggreaterWG andareductionin lengthofhospital stay.
IntrahospitalT/KS: 15min,2x/day,for tendays,
non-treatmenton weekend. Period1:TS, vestibularand proprioceptive (15min) Period2:lateral wedge-shaped crescent(15min) Performedbythree trainedpeople, 30minbeforefeeding at7amand10am. Extra-hospital: T/KS+visual,auditory stimulationfor5min
1)DailyWG 2)Formulaintake 3)Lengthofhospital stay
4)Posturalreflexes andneurobehavioral performancewere assessedatthetime thechildleftthe hospitalandone monthafterwards.
Bodyweighttaken dailywithnormal nurseryroutine. Onlyonescalewas used.
Notdescribed 1)TG:3.2g/daymore 3)TG:3daysless 4)Better neurobehavioral performanceand posturalreflexes
Massagestimulates growthinpreterm infants:a replication23 Scafidietal.,1990 PEDro
Total:40 TG:20 GAM=30w BWM=1179g CG:20 GAM=30w BWM=1180g Stratification: <or>30weeksGA <or>1100gBW <or>20daysNICU <or>1300gat beginningofstudy
Designedtocorrect previous
methodological weaknessesand provideareplication ofthepreviousstudy. Notrandomized, alternativeweeks. Beginningwhen clinicallystable.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,starting60min afterthenoon feeding,for10 weekdays; non-treatmenton weekends.
Notclearwhoapplied thetechnique. Neverlostcontact withtheinfant’sskin duringstroking motions.
1)DailyWG 2)Formulaintake, frequencyofvoiding andstooling 3)HR,RR,body temperature 4)Numberofapneic episodes
6)Parentsvisitingand touch
7)Brazeltonscale (day1and10) 8)Sleep/wake behavior---videotaped during
stimulation/no-stimulationperiod 9)Lengthofhospital stay
Theinfantwas weigheddailyby theexperimenter orresearch assistant
immediatelyprior tothe3pm feeding.
220
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Massagealtersgrowth andcatecholamine productionin pretermnewborns24 FieldSchanberg, 1990
Bibliography---Touch researchinstitute
Total:40 BWM=1176g GAM=30w NICU=14days Randomized
Toreplicatethe stimulationprocedure andfindingsofthe earlierstudy,andto addseveral under-the-skin variablessuchas growthhormone, cortisol,and
cathecolamineactivity thatmightprovide moreinformationon therelationship betweenTSandWG.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,starting60min afterthenoon feeding,forten weekdays; non-treatmenton weekends.
Notclearwhoapplied thetechnique.
1)Formulaintake, dailyWG
2)Frequencyof urination 3)Frequencyof stooling 4)HR,RR,body temperature 5)Numberofapneic episodes
6)Parentsvisiting(and iftouching,holding, andfeeding) 7)Sleep---wake behavior 8)Plasmagrowth hormoneandcortisol 9)
Urine-norepinephrine, epinephrine,
dopamine,cortisol, andcreatinine 10)Lengthofhospital stay
Notdescribed Notdescribed 1)TG:21%greaterWG (p=0.003).
3)Betterperformance onthehabituation clusterfollowingthe treatmentperiod,less timeinactivesleep, andlessfacial grimacing, mouthing/yawning, andclenchedfists 10)5daysless hospitalization
Massageeffectson cocaine-exposed pretermneonates25 Wheedenetal., 1993
PEDroandPubMed searches1,4
Total:30 TG
GAM=29.7w BWM=1158.3g CG
GAM=30.8w BWM=1265.4g
Toobservetheeffects ofMTinWGof cocaine-exposedPI. Beginningwhen clinicallystable.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,fortendays.All performedbythe sametrained researcher.
DuringTSphasenever lostcontactwiththe skin,keepingpressure eveniftherewassome reactionfromthe infant,suchastickle.
1)DailyWG 2)Formulaintake, frequencyofvoiding andstooling 3)HR,RR,body temperature 4)Numberofapneic episodes
5)Parentsvisitingand touch
6)BrazeltonScale 7)Postnatal complications
Bodyweighttaken dailywithnormal nurseryroutine.
Notdescribed
1)TG:28%greaterWG 2)MoredailyWG, p<0.01
Tactile
kinesthetic
stimulation
in
preterm
infants
221
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Factorsthatpredict whichpreterm infantsbenefit mostfrommassage therapy26
Scafidietal.,1993 Bibliography---Touch researchinstitute
Total:93 GAM=30w BWM=1204g NICU=15days Weightatstartof study=1353g
Thisstudyexamined individualdifferences toidentifyinfantand clinical
characteristicsthat wouldpredict maximalWGin controland
MT-receivinginfants. Beginningwhen clinicallystable.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,fortendays; neverlostcontact withtheskin,or lightenedthe pressure. Trainedresearch assistantornurse.
1)WGandvolumetric andcaloricintake 2)Frequencyof voiding 3)HR,RR,body temperature 4)Numberofapneas 5)Frequencyof visiting(including touch,feeding,and holding)
6)Sleep-wake 7)Brazeltonscale
Datacollected fromthenurses notesanddaily weighingbya researchassistant.
Thesessionwas discontinuedif behavioralsigns ofstressor cryingpersisted forlongerthan 60s
continuously.
1)TG:Greaterdaily WG(p<0.01) 2)Separatet-test analyseswere performedforthe lowandhighweight gainers:70%ofthe TGwasclassifiedas highweightgainand 40%oftheofCG (p<0.01)
Lowweightgainersof theTGgainedmore weight(p<0.005)
Effectsof
tactile-kinesthetic stimulationin preterms:a controlledtrial14 Mathaietal.,2001 PubMedsearches1, 2,3,4,5,6
Total:45 TG:25 GAM=34.6w BWM=1598g CG:23 GAM=34.3w BWM=1588g Not randomized-systematic allocation
Determinetheeffects ofT/KSinPIon physiological parameters,physical growth,and behavioral development (BrazeltonScale). Beginningaftertwo daysclinicallystable.
T/K:3x/day,15min, forfivedays, 30-45minafter morning,afternoon, andnightfeeding,by atrained
professional. Afterthisperiodthe mothersperformed until40-42w post-menstrualage. Proneandsupine position.
Usedtalcormineral oil,excessremoved withcottonafter finish.
1)Anthropometric dataatthebeginning andendofthestudy 2)Physiologic parameters 3)Brazeltonscale beforeandafterfive daysofT/KSandat theendofthestudy.
Bodyweighttaken dailywithnormal nurseryroutine, onanelectronic scale(Phillips®, Amsterdam, Netherlands)with anaccuracy of±5g.
Ifthebaby startedcryingor passedurineor stoolsduringthe session,itwas temporarily stoppeduntilthe babywas comfortable again.
1)TG:GreaterWG (21.9%,4.24g/day) 2)TG:HigherHR duringstimulation (p<0.005) 3)Improved
neurobehaviorduring days5-7in
222
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Massagetherapyby mothersand trained professionals enhancesweight gaininpreterm infants15
Ferberetal.,2002 PEDroandPubMed searches1,4
Total:57 1)TGmother:21 GAM=30.9w BWM=1318g 2)TGprof:17 GAM=31.8w BWM=1527g 3)CG:19 GAM=31.52w BWM=1375g
Comparetheresults ofMTperformedby mothersandby trainedprofessionals onWGinPI. Beginningwhen clinicallystable.
OnlyTSproneand supine,moderate pressure,15min, 3x/daily,early3hs consecutivefor10 days.Onegroup receivedfromthe prof,theotherfrom mothers.
Each7.5min:Both handswerelaidon thebaby’sheadfor 10swithout movement,thenthe infantwasstroked slowlybyhand movementfromthe headtowardsthe legs,backandforth. Nomassagesonchest andstomach. Betweenday7and day9:oneday withoutMT.
1)WG
2)Calorieintake
Notdescribed Notdescribed
Tactile
kinesthetic
stimulation
in
preterm
infants
223
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Stablepreterm infantsgainmore weightandsleep lessafterfivedays ofmassage therapy27
Dieteretal.,2003 PubMedsearches1, 4
Total:32 TG:16 GAM=30.1w BWM=1359g CG:16 GAM=31.1w BWM=1421g
Toevaluatetheeffect offivedaysofMTin WGandsleep-wake behaviorinPI. Beginningwhen clinicallystable.
T/KS:15minforfive days,3x/day. Performedbya trainedtherapist.
1)DailyWG 2)Formulaintake, kilocalories,stooling 3)Sleep-wake behavior
DailyWGwas measuredinthe earlymorningby nursesonthe precedingnight shift.
Atthesignof physiologic distress(HR greaterthan200 bpm),massage wasdiscontinued for15s,oruntil areturnto baselinelevels wasobserved. Massagewas thenresumed. Theoccurrence offiveperiodsof physiologicover reactivitywas arbitrarily chosenasthe criterionfor discontinuingan infantfromthe study.Noinfant discontinued.
1)TG:53%greater dailyWG(p=0.001) 3)TG:Lesssleeping time(p=0.04)and drowsylonger (p=0.007)
Effectofoilmassage ongrowthand neurobehaviorin verylowbirth weightpreterm neonates33 Aroraetal.,2005 PEDroandPubMed searches1,4
Total:62 1)TGwithoil:20 GAM=33.9w BWM=1280.2g 2)TGwithoutoil: 19
GAM=34.6w BWM=1298.6g 3)CG:23 GAM=34.7w BWM=1327.1g
Studyingtheeffectof MTwithoilongrowth andbehaviorPIwith BW<1500g. Beginningassoonas theyreceivedenteral feedsofatleast 100mL/kg/day, providedtheywere lessthan10daysof age.
20gentlestrokesin eacharea,by professionalsand mothers.
Proneposition:both shouldersstarting fromtheneck,upper backtothewaist. Supineposition:the limbs.
28days,4x/dayfor 10min.
Afterdischarge performedby mothers.
Usedsunfloweroil.
1)WG
2)Anthropometric data
3)Serumtriglyceride levels
Bodyweighttaken withnormal nurseryroutineat thetimeof registrationand weeklyforthe nextfourweeks.
Temporary interruptionin thetrial:apnea, sepsis,andIVH. Minorproblems: oralthrush, pyoderma,and hyperbilirubine-mia
224
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Vagalactivity,gastric motility,and weightgainin massagedpreterm neonates28 Diegoetal.,2005 PubMedsearches1, 4
Total:48 1)TG:16 GAM=29.8w BWM=1091g 2)Gsham:16 GAM=30.3w BWM=1184g 3)CG:16 GAM=29.6w BWM=1265g
Assesswhetherthere alterationinVA,GM, andWGinresponse toMT.
Beginningwhen clinicallystable.
T/KS:15min3x/day forfivedays,1hafter feeding.
Appliedbyvarious professionals. TheGshamreceived thesamesequenceof T/KSwithlight pressure.
1)WG 2)Daysof hospitalization 3)VAandGMonday1 (15minbefore, duringthe15minof treatment,and 15minafterT/KS)
Datacollectedby ablinded researcher. Bodyweighttaken withnormal nurseryroutine
Notdescribed 1)GMgreaterWG(p< 0.01),withnogreater caloricintake. 3)IncreasedVAand GMduringandshortly afterMT.
Theeffectofinfant massageonweight gain,physiological andbehavioral responsesin premature infants19 Lee,2005
PubMedsearches1, 2,3,4,5
Total:26 TG:13
GAM=224.2days BWM=1508.5g CG:13
GAM=217.4days BWM=1377.7g
Evaluatetheresponse ofinfantswho receivedMTinWG, including
physiologicaland behavioral parameters. Beginningwhen clinicallystable,two daysafterstartof enteralfeeding.
T/KS:15min2x/day fortendays,1hafter feedinginthe morningand afternoon,with infant’seyesopen. Datacollected10min beforeand10min aftertheT/KSdaily. Useofoiltoreduce friction.
Performedbynurses. 1)WG
2)Physiologicaldata 3)Behavioral responses: 10minevaluation pre-andpost-MT -videotaped
4)Electrocardiogram
Nursesonthe precedingnight shiftmeasured dailyWGinthe earlymorning.
Studywouldbe discontinuedfor atleastonehour if:HRlessthan 100bpmor greaterthan200 bpmfor12sor more,orblood oxygen
saturationlevels lessthan90%for longerthan30s. Infantshowedno signsofstress duringthestudy.
1)HigherinVAinTG: days1,2,6,7,8,and 9
2)IncreasedO2Sat onthe9thdayinTG 3)Significantincrease inalertnessand motoractivity 4)Therewasa significanteffectfor days(p=0.001)both groupsincreasedin WG,ontheaverage, overtheten-day experimentalperiod
Preterminfant massageelicits consistent increasesinvagal activityandgastric motilitythatare associatedwith greaterweight gain29
Diegoetal.,2007 PubMedsearches1, 4
Total:70
TG:34 CG:36
Determinewhether theMTinPIisrelated totheincreaseinVA andGMandifit interfereswithWG. Beginningwhen clinicallystableand gavage-fed.
T/KS:15min3x/day forfivedays,one hourafterfeeding, earlyof3hs consecutive Performedby professional
1)DailyWG 2)Caloricintake 3)ECGsandEGGs collectedondayone anddayfive,15min before,duringthe 15min,and15min aftertheprocedure. MTwasperformedat 12am.
Bodyweighttaken withnormal nurseryroutine.
Notdescribed 1)TG:IncreasedWG (30%more)
Tactile
kinesthetic
stimulation
in
preterm
infants
225
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Insulinandinsulin-like growthfactor1 increasedin pretermneonates followingmassage therapy30 Fieldetal.,2008 PubMedsearches1, 4
Total:42 TG:95 GAM=29.3w BWM=1178.5g CG:42 GAM=2.8w BWM=1292.5g
DetermineiftheMT increasedserum insulinandinsulin-like growthfactor1 (IGF-1)inPI. Beginningwhen clinicallystable.
T/KS:15min3x/day forfivedays,onehour afterthemorning feeding(12am),early of3hsconsecutive. Conductedbya therapist.
1)DailyWG
2)Dailycaloricintake 3)Vitalsignsbefore, during,andafterthe MT
4)Seruminsulinand IGF-1ondaysoneand five
5)VAmeasuredat intervals
Bodyweighttaken withnormal nurseryroutine (weigheddaily priortothe8am feeding)
Notdescribed 1)TG:GreaterWG (p=0.02)
4)TG:Increasein insulin(p=0.001)and greaterincreasein IGF-1(p=0.05) 5)TG:greaterVA (p<0.001)
Massagetherapy reduceshospital stayandoccurrence oflate-onsetsepsis inverypreterm neonates16 MendesProcianoy, 2008
PubMedsearch1
Total:104 TG:52 GAM=29.7w BWM=1186.8g CG:52 GAM=29.4w BWM=1156.7g
Studyingtheeffectsof massageonmaternal hospitalstayinvery lowbirthweight (VLBW)whowere alreadysubmittedto skin-to-skincare. Beginningafter 48hoursoflife.
MTappliedonlyby mothers,4x/dayfor 15mineachtime, intervalsof6h.TS: temporal,frontal, periorbital,nasal,and perilabialregionsof thefaceandthe externalsideofthe upperandlower limbs+KS(3xeach: wrist,elbow,ankle, andknee)
1)Lengthofhospital stay
2)Growth 3)Ageofstartof partialortotalenteral feeding
4)Agewhichpartial andtotaloralfeeding started
5)Occurrenceoflate onsetsepsis---clinical andbloodand or/cerebrospinalfluid 6)Presenceof necrotizing enterocolitisand 7)Bronchopulmonary dysplasia
Bodyweighttaken withnormal nurseryroutine, alwaysverifiedbya blindedresearcher, intheafternoon andusingthesame digitalbabyscale equipment
Notdescribed 1)TG:Fewerdaysof hospitalization (p=0.084)
2)TG:Lesserrateof late-onsetsepsis (p<0.01)
Weightgainin preterminfants following parent-administered Vimalamassage:a randomized controlledtrial17 Gonzalezetal., 2009
PEDroandPubMed searches1,4
Total:60 TG:30 GAM=31.4w BWM=1235g CG:30 GAM=31.7w BWM=1220g
EvaluatetheWGinPI receivingMT,correlate withlengthofhospital stayandcheckfor othereffects. Beginningwhen clinicallystable,with orogastrictube feeding.
Vimalamassage 2x/dayfortendays, 1hafterfeeding. Conductedbythe motherorfather, trainedand supervised:face, upperlimbs,chest, abdomen,lower limbs,andback, withouteverlosing touch,evenincases ofPIdiscomfort. Usedoilorcream.
1)DailyWG
2)Dailycaloricintake 3)Lengthof
hospitalization
Bodyweighttaken withnormal nurseryroutine withadigitalscale, (Seca®,Hamburg, Germany).At8am everyday,1h beforethenext scheduledfeeding. Thenursewas blinded.
226
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Massagewith kinesthetic stimulation improvesweight gaininpreterm infant31
Massaroetal.,2009 PEDroandPubMed searches1,4
Total:60 TSG:20 GAM=29w BWM=1097g T/KSG:20 GAM=29w BWM=1124g CG:20 GAM=27w BWM=959g
Toevaluatethe effectofMTwithand withoutkinesthetic phaseinWGandin thelengthofPI hospitalization. Beginningwhen clinicallystable.
TS(onlyphase1and 3)orT/KS2x/dayfor 15min,performedby trainednurses,from thebeginningofthe studyuntildischarge.
1)DailyWG
2)Dailycaloricintake 3)Lengthof
hospitalization
Bodyweighttaken withnormal nurseryroutine.
Notdescribed T/KSG:withbirth weight>1000 g=higherdailyWG (stratificationbyBW)
Massagetherapy improves
neurodevelopment outcomeattwo yearscorrectedage forverylowbirth weightinfants36 Procianoyetal., 2010
PubMedsearches1, 4
Total:73 TG:35 GAM=30w BWM=1192g CG:38 GAM=29.7w BWM=1151g bothgroups Skin-skincare
Assesstheoutcomeof MTgrowthand neurodevelopmentof PIassessedat2years correctedage. Beginningafter48h oflife.
MTappliedonlyby mothers,4x/dayfor 15min,intervalsof 6hoursofTS: temporal,frontal, periorbital,nasal, andperilabialregions ofthefaceandthe externalsideofthe upperandlower limbs+KS(3xeach: wrist,elbow,ankle, andknee)
1)Anthropometric 2)Bayleyscalesof infantdevelopment, secondedition (BSID-II).
Measuredat2years ofcorrectedage
Bodyweighttaken withnormal nurseryroutine.
Mothersofthe TGwere instructedto observethe newborns’ tolerancesigns, avoiding excessive stimulations.
Tactile
kinesthetic
stimulation
in
preterm
infants
227
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Sensorimotor interventions improvegrowth andmotorfunction inpreterm infants18
Fucile&Gisel,2010 PubMedsearches1, 2,3,4,5,6
Total:75 OSG:19 T/KSG:18 OS+T/KSG:18 CG:20
Toevaluatetheeffect ofOSandT/KSalone onWGandmotor functioninPIandif OS+T/KShave greaterinfluenceon theseparameters. Beginningwhen clinicallystable, receivingallfeedings bytube.
OS:15min2x/dayfor tendays(7min: cheek,chin,lips, 5minongumand tongue,and3minof non-nutritivepacifier sucking).
T/KSfor15min 2x/day.TS:Proneand supine,strokingthe bodystartingfrom thehead,followedby theneck,shoulders, back,legs,and arms+KS. Performedby researcher.
1)DailyWG (g/kg/day) 2)MotorFunction. TestofInfantMotor Performance-1969 (TIMP)
Bodyweighttaken withnormal nurseryroutine, nursewasblinded andalwaysused thesamescale.
Stopprocedure: iffussing, vomiting, growingoxygen demand, frequent episodesof apnea, bradycardia,or desaturationin the24hthat precededthe intervention;or interventions suchassightor hearingtests performed30min beforeT/KS.
1)OSGand T/KSG:greaterWG (p=0.014)
2)T/KSGandOS+ T/KSG:greaterTIMP scores(p<0.003)
Behavioralanalysisof pretermneonates includedinatactile andkinesthetic stimulation programduring hospitalization20 Ferreira
Bergamasco,2010 PubMedsearches2, 3
Total:32 TG:16 GAM=33.4w BWM=1910.3g CG:16 GAM=33.3w BWM=1872.8g Notrandomized
Toevaluatetheeffect ofT/KSevolution behavioraland clinicalnewbornPI during
hospitalization. Beginningwhen clinicallystable.
8min/weekfilming untildischarge: behavioral evaluation. TS:performed 4-5x/weekfor 5-15min,focusingon alertness.Soft touches,slowand continuous,norigid sequence,with cerebrospinalflow directiononthe trunk,and proximal-distal directiononthe limbs,supineor lateralposition. KS:flexionand extensionofthe limbs.
Conductedby researcher.
1)DailyWG 2)Lengthof hospitalization 3)Behavioral evaluation:adapted fromtheManualfor theNaturalistic Observationof NewbornBehavior (Pre-termand Full-term)
Bodyweighttaken withnormal nurseryroutine.
Notdescribed. Citessome internalevents inherenttothe nurserythatcan interferewith behavioral responses,such astimeafterthe lastfeeding, sleep,pain, noise,light,and temperature.
3)TG:Greater%time with:
Regularrespiration (p=0.002)
Stateactivewarning (p=0.036)
Posturesmixed (p=0.013) Balancedtone (p<0.001)
228
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Arandomized placebo-controlled trialofmassage therapyonthe immunesystemof preterminfants32 Angetal.,2012 PubMedsearches1, 4
Total:120 TG:58 GAM=30w BWM=1389g CG:62 GAM=30w BWM=1286g Randomized
Toinvestigatethe effectsofMTonthe immunesystemofPI. Beginningwhen clinicallystable.
T/KS:15min,3x/day, atthebeginningof threeconsecutive hours,behindtwo widescreens,fora minimumoffivedays andmaximumoffour weeksoruntil hospitaldischarge. CG:nurseremained behindthetwowide screensthesame amountoftime.
1)Immunologic evaluation(absolute NKcells,TandB cells,Tcellsubsets, andNKcytotoxicity 2)WG
3)Numberof infections
4)Lengthofhospital stay
Notdescribed Notdescribed 1)TG:NKcytotoxicity higher(p=0.05) 2)TG:Greaterdaily WG(p=0.01)and higherfinalweight (p=0.05)
Massageimproves growthqualityby decreasingbodyfat depositioninmale preterminfants37 Moyer-Mileuretal., 2013
PubMedsearches1, 4
Total:44 TG:22 GAM=31.4w BWM=1574g CG:22 GAM=31w BWM=1618g Randomized
Toassesstheeffectof MTonWGandbody fatdepositioninPI. Beginningwhen toleratingenteral feeding
vol-umes>100mL/kg/day.
20min2x/dayat7 amand7pm,6 days/week(except Sunday),performed behindaprivacy screenbyalicensed massagetherapist. TheMTwasmodeled aftertheInfant MassageUSAprotocol andmodifiedforPIby eliminatingmassage oftheabdomen.
1)WG
2)Lengthofhospital stay
3)Ponderalindex 4)Body
circumferences 5)Skinfoldthickness 6)Insulin-likegrowth factorI,leptin, adiponectinlevels 7)Dailydietaryintake
Bodyweightonan electronicinfant scale(Air shields-vickers®,Ohio, USA)wasrecorded tothenearest gram.
Allmassage therapistswere trainedto recognize clinicalsignsof distress.
3)TG:Maleinfants hadsmallerponderal index
5)TG:Maleinfants hadtriceps, subscapular,and mid-thighskinfold thicknessincreases (p<0.05)
TG:Femalehad largersubscapular (p<0.05)
Tactile
kinesthetic
stimulation
in
preterm
infants
229
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
Effectofoilmassage ongrowthin pretermneonates lessthan1800g:a randomizedcontrol trial34
Kumaretal.,2013
PubMedsearches1, 4
Total:48 TG:25 GAM=32.9w BWM=1466.6g CG:23 GAM=32.6w BWM=1416.6g Randomized
Tostudytheeffectof oilmassageongrowth inpretermbabiesless than1800g.
Beginning<48hof ageandonatleast 100mL/kg/doffeed oralortubefeed.
10min,4x/day,4w massagewascarried outfirstoverboth shouldersstarting fromtheneckwith thebabyinprone position.Thenitwas carriedoutfromthe upperbacktothe waist.Eachofthe twoupperandlower limbswasseparately massagedinthe supineposition. Twentygentlestrokes ineacharea. Massagewasprovided with2.5mL/kg (10mL/kg/day)of sunfloweroil,by researcherormother (ifdischargedbefore 4w)
1)WGafter28days
2)Lengthandhead circumferenceafter 28days
3)Lossofweight after7days
4)Differencein serumtriglyceride levelsafter28days
Weremeasured usingstandard techniques,at enrollmentand thenweeklyfor next4weeks.
Notdescribed 1)TG:GreaterWG over28days(p<0.05)
230
P
epino
VC,
Mezzacappa
MA
Table1 (Continued)
Title/Author/ Year/Database
SampleSize Objectivesand startingconditions
Descriptionofthe technique
Mainvariables Measuredweight gain
Descriptionof adverseevents duringthe procedure
Resultsachieved statisticalsignificance
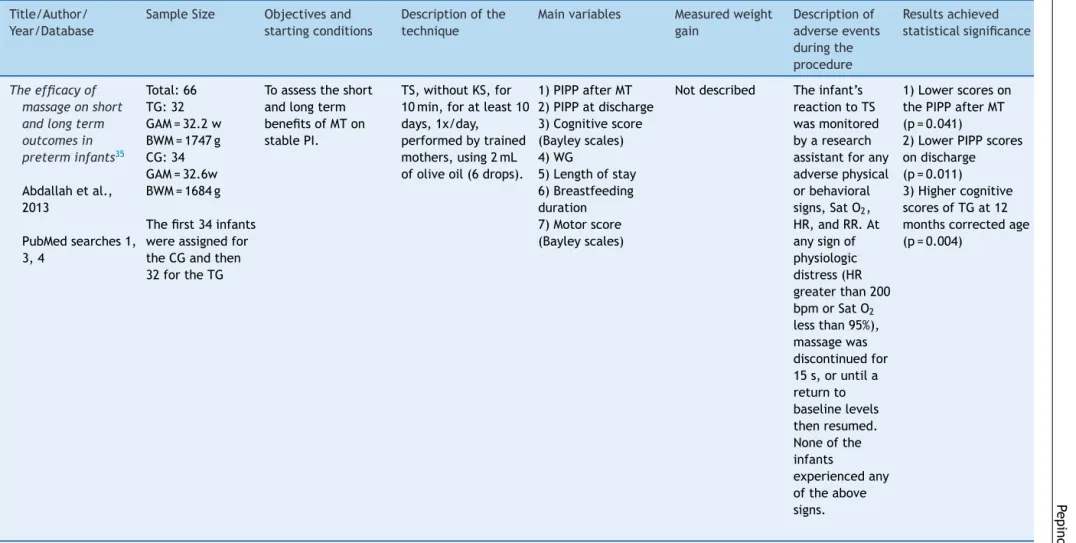
Theefficacyof massageonshort andlongterm outcomesin preterminfants35
Abdallahetal., 2013
PubMedsearches1, 3,4
Total:66 TG:32 GAM=32.2w BWM=1747g CG:34 GAM=32.6w BWM=1684g
Thefirst34infants wereassignedfor theCGandthen 32fortheTG
Toassesstheshort andlongterm benefitsofMTon stablePI.
TS,withoutKS,for 10min,foratleast10 days,1x/day, performedbytrained mothers,using2mL ofoliveoil(6drops).
1)PIPPafterMT 2)PIPPatdischarge 3)Cognitivescore (Bayleyscales) 4)WG
5)Lengthofstay 6)Breastfeeding duration 7)Motorscore (Bayleyscales)
Notdescribed Theinfant’s reactiontoTS wasmonitored byaresearch assistantforany adversephysical orbehavioral signs,SatO2, HR,andRR.At anysignof physiologic distress(HR greaterthan200 bpmorSatO2 lessthan95%), massagewas discontinuedfor 15s,oruntila returnto baselinelevels thenresumed. Noneofthe infants
experiencedany oftheabove signs.
1)Lowerscoreson thePIPPafterMT (p=0.041)
2)LowerPIPPscores ondischarge (p=0.011) 3)Highercognitive scoresofTGat12 monthscorrectedage (p=0.004)
TS,tactilestimulation;T/KS,tactileandkinestheticstimulation;KS,kinestheticstimulation;HR,heartrate;RR,respiratoryrate;BW,birthweight;BWM,birthweight-mean;GAM,
gestationalage-mean;GA,gestationalage;NICU,Neonatalintensivecareunit;MT,massagetherapy;prof,professional;VA,vagalactivity;GM,gastricmotility;ECGs,electrocardiograms;
Tactilekinestheticstimulationinpreterminfants 231
Discussion
Tactilestimulationhastheadvantagesofbeingnoninvasive, inexpensive,andsafe,aswasdemonstrated byLivingston etal.38 basedonphysiological stabilityand nochangein agitation/painscoresoftheinfantsreceivingmassage.The majority oftheclinical trialsstudied herein(20 ofthe 31 studies)3,10,14,15,17---19,21---32,34 described asignificantlybenefit onweightgain in the PI groupthat received theTS/TKS. ThisinformationplacesTSasapromisingadjunctivetoolin addressingPIintheNICU.Someofthestudiesdidnotassess thedatastatistically;partofthemjustifiedthisbecauseof smallsamplesize.6---8
Some correlations have been suggested to justify the faster weight gain of PI submitted to TKS, such as greatervagalstimulationandgastricactivity,28,29 relation-shipwithenergyintake,3,10,15,17,22---31,39sleep-wakebehavior andbehavioralscales,6---8,10,14,19---27,36,39seruminsulinand IGF-1levels,30,37anduseofoil.33,40,41TheresultsfoundbyDiego et al. 28 and Field et al. 42 on the effects of mild and moderatepressureshowedthatmoderatepressureprovided greatervagalstimulation.Diegoetal.29alsofoundgreater gastricmotilityamongthePIwhowerestimulatedwith mod-erate pressureand suggested thatgreater gastric activity mayexplaintheirfasterweightgain.Fieldetal.42 added thatthegroupofPIstimulatedwithmoderatepressurewere morerelaxed,characterizedbytheirlowerheartratesand bytheassessmentoftheirwakeandsleepstatus,and behav-ior,asrecommendedby theThomasScaleof1975.21 They thensuggestedthatthemorerelaxedstateofthePIresulted in lower energy expenditure, which would then result in faster weight gain. This was confirmed by Lahat et al.,43 whoused indirectcalorimetry toshow that a groupof PI submittedtostimulationhadlowerenergyexpenditure.
Regarding energy intake, some studies have shown that stimulated infants have higher daily weight gain.10,17,22,23,25---28,31,32,39 Other studies recorded stool-ing frequency and found that it increased significantly, together withan increasedformula intakeon days6-10.9 Rausch9 suggested that increased stooling was a conse-quenceofhigherformulaintake.Ontheotherhand,Scafidi et al. 23 found that the frequency of stooling decreased, even when daily weight gain increased. White Labarba3 reportedthattheamountofformulaconsumedperfeeding increased while the number of daily feedings decreased, whichtheauthorsattributedtothenurseryroutine:PIwho didnot consumethe entire servingwerefed moreoften. Otherstudiesthatreportedfasterweightgaindidnotfind significantdifferencesinenergyintake.
Along with weight gain, other variables, some mentioned above, have been analyzed after appli-cation of TKS in premature. All of the following parameters were analyzed by clinical studies in PI who received TS/MT whether or not associated with KS during their NICU stay: weight gain;3,6---10,14---37,39 length of hospital stay;10,16,17,20,21,23,24,28,31,32,35,37,39 behavioral responses;6---8,10,14,19---23,25,26,36,39 sleep/wake stage;10,21,23,24,26,27stressbehavior;11 energyexpenditure;43 body temperature;3,6,21,23---26,44 variations in stimulation pressure;42 use or non-use of oil;33,40,41 speed of brain maturation;38vagalactivityandgastricmotility;28,29serum insulin and growth factor I levels;30,37 late-onset sepsis;16
bodyfatdeposition;37 effectontheimmunesystem;32 and boneformation.45 The studieshadverysimilarobjectives; thatis,toidentifytheeffectsofTKSontheseparameters andthepossiblecausesofitsbenefits.
Somestudies usingonly KSobtainedresults notonlyin greater weight gain but also in bone mineralization.46---48 As for TKS withor without KS for bone weight gain ana-lyzed herein, they found that there was no ideal level of stimulation47 or optimal duration, frequency, andtype ofexerciseforbone development.49 Furtherevaluationof this intervention (KS) was suggested to indicate for this purpose.50 A more recent study demonstrated a signifi-cantimprovementinboneformationanddecreaseofbone resorption,usingamorerigorousmethodologicaldesign.48
A few studies have described the adverse situations that could occur during the procedure and the parame-ters that should encourage the therapist to interrupt the session.14,18,19,26,33 Certain signs during the application of the TKS, such as stress or uninterrupted crying for more than60seconds,26defecationorurination,14increasedheart rate,19,27orheartrate<100for12secondsanddesaturation formorethan30seconds,19weresomeofthecausesthatled thetherapiststointerrupttheprocedureordiscontinuethe study.Sometherapistsconsideredsomesignsinthe24hours thatprecededthe interventiontosuspendtheprocedure, suchasfussing,vomiting,growingoxygendemand,frequent episodesofapnea,bradycardia,desaturation,or interven-tionsconductedwithinthe30minutesthat precededTKS, suchassightandhearingtests.18 Aroraetal.33 separated theadversesituationsintotemporaryinterruptionandminor problems that neither affected feeding nor required any interruptioninthetrial.
Despitetheinformationabove,themajorityofthe stud-iesdidnotmentionadverseeventsand/ordidnotdescribe acourse ofaction todealwithadverse events duringthe intervention.The studies thatreportedthe occurrenceof eventsthatrequiredtheinterruptionoftheproceduredid notindicatehowtheprocedurewasresumed;forexample, whetheritwasresumedfromthestartofthemassage rou-tineorwhetheritwascontinuedfromwhereithadstopped; also,theydidnotindicatewhethertheprocedureshouldbe resumedonthe sameday or onthenextday, or whether theseinterruptions couldaffect weightgain. The clinical trialsstudiedby thisreview madearelevant contribution to the scope of TS. Nevertheless, adding detailed data highlightedby this review,such asadverse events, would improvemethodologyandreliabilityforfuturestudies.
Limitations
Thissystematicreviewwasperformedusingtwodatabases, inadditionto checkingthebibliographic articles ofthose thatmettheinclusioncriteria;however,thepossibilityof not having included an article relevant to the topic that couldhavebeenfound inotherdatabasescannotberuled out.
Conclusion
232 PepinoVC,MezzacappaMA
TStechniqueor recommendedcourse ofaction ifadverse events occur during the procedure. The effect of these adverseeventsthatcanoccurduringtheTKSproceduremay influencetheresults.
Generally, some kind of benefit associated with TKS, suchasfasterweightgain,shorter hospitalstay,and bet-terbehavior,amongothers,wasreportedbyallstudiesthat usedTSorTKSinPI.NurserieshavemanystressorsandTKS hasbeen shown to behelpful in this context. Therefore, TKSshouldbeconsideredasapossibletherapytobe associ-ated withthe standard medical treatment. Even discrete gains in this population can result in long-term benefits. Futurestudies mayraisethelevelofmethodologicalrigor anddescribetheadverseeventsthatcanoccurduringthe procedure.This maypermit otherresearcherstobemore awareofexpectoutcomes,and astandard TKStechnique couldbeestablished.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Smith GC, Gutovich J, Smyser C, Pineda R, Newnham C, TjoengTH,etal.Neonatalintensivecare unitstressis asso-ciatedwithbraindevelopmentinpreterminfants.AnnNeurol. 2011;70:541---9.
2.FernandesLV,Goulart AL, SantosAM, BarrosMC, GuerraCC, KopelmanBI.Neurodevelopmentalassessmentofverylowbirth weightpreterminfantsat correctedageof18-24months by BayleyIIIscales.JPediatr(RioJ).2012;88:471---8.
3.White JL,LabarbaRC. Theeffectsoftactileand kinesthetic stimulationonneonataldevelopmentintheprematureinfant. DevPsychobiol.1976;9:569---77.
4.FreedmanDG,BovermanH,FreedmanN.Theeffectsof
kines-theticstimulationonweightgainandonsmilinginpremature
infants.PaperpresentedattheannualmeetingoftheAmerican
OrthopsychiatricAssociation.SanFrancisco;1966.
5.HasselmeyerEG.Theprematureneonate’sresponseto hand-ling.AmericanNursingAssociation.1964;11:15---24.
6.SolkoffN,WeintraubD,YaffeS,BlaséB.Effectsofhandlingon thesubsequentdevelopmentofprematureinfants.DevPsychol. 1969;1:765---9.
7.KramerM,ChamorroI,GreenD,KnudtsonF.Extratactile stim-ulationoftheprematureinfant.NursRes.1975;24:324---34.
8.SolkoffN,MatuszakD.Tactilestimulationandbehavioral devel-opmentamonglow-birthweightinfants.ChildPsychiatryHum Dev.1975;6:33---7.
9.Rausch PB. Effects of tactile and kinesthetic stimulation on prematureinfants.JOGNNurs.1981;10:34---7.
10.FieldTM,SchanbergSM,ScafidiF,BauerCR,Vega-LahrN, Gar-ciaR,etal.Tactile/kinestheticstimulationeffectsonpreterm neonates.Pediatrics.1986;77:654---8.
11.Hernandez-Reif M, Diego M, Field T. Preterm infants show reducedstressbehaviorsandactivityafter5daysofmassage therapy.InfantBehavDev.2007;30:557---61.
12.PhysiotherapyEvidenceDatabase(PEDro).[cited17Jul2014].
Availablefrom:www.pedro.fhs.usyd.edu.au
13.United States National Library of Medicine of the National
Institutes of Health. [cited 17 Jul 2014]. Available from:
www.ncbi.nlm.nih.gov/pubmed
14.MathaiS,FernandezA,MondkarJ,KanburW.Effectsof tactile-kinestheticstimulationinpreterms:acontrolledtrial.Indian Pediatr.2001;38:1091---8.
15.Ferber SG, Kuint J, Weller A, FeldmanR, DollbergS, Arbel E,etal.Massagetherapybymothersandtrained profession-alsenhancesweight gaininpreterminfants.EarlyHumDev. 2002;67:37---45.
16.MendesEW,ProcianoyRS.Massagetherapyreduceshospitalstay andoccurrenceoflate-onsetsepsisinverypretermneonates. JPerinatol.2008;28:815---20.
17.Gonzalez AP, Vasquez-Mendoza G, García-Vela A, Guzmán-Ramirez A, Salazar-Torres M, Romero-Gutierrez G. Weight gaininpreterminfantsfollowingparent-administeredVimala massage: a randomized controlled trial. Am J Perinatol. 2009;26:247---52.
18.FucileS,GiselEG.Sensorimotorinterventionsimprovegrowth and motor function in preterm infants. Neonatal Netw. 2010;29:359---66.
19.LeeHK.Theeffectofinfantmassageonweightgain, physio-logicalandbehavioralresponsesinprematureinfants.Taehan KanhoHakhoeChi.2005;35:1451---60.
20.FerreiraAM, BergamascoNH.Behavioral analysisofpreterm neonatesincludedinatactileandkinestheticstimulation pro-gramduringhospitalization.RevBrasFisioter.2010;14:141---8.
21.ScafidiFA,FieldTM,SchanbergSM,BauerCR,VegaLahrN, Gar-ciaR, etal.Effectsoftactile/kinestheticstimulationonthe clinicalcourseandsleep/wakebehaviorofpretermneonates. InfantBehavDev.1986;9:91---105.
22.Field T, Scafidi F, Schanberg S. Massage of preterm new-bornstoimprovegrowthanddevelopment.PaediatricNursing. 1987;13:385---7.
23.ScafidiF,FieldT,SchanbergS,BauerC,TucciK,RobertsJ,etal. Massagestimulates growth inpreterminfants: areplication. InfantBehavDev.1990;13:167---88.
24.FieldT,SchanbergS.Massagealtersgrowthandcatecholamine productioninpretermnewborns.In:FieldT,BrazeltonTB, edit-ors.AdvancesinTouch.Skillman,NJ:Johnson&Johnson;1990. p.96---104.
25.WheedenA,ScafidiFA,FieldT,IronsonG,ValdeonC,Bandstra E.Massageeffectsoncocaine-exposedpretermneonates.JDev BehavPediatr.1993;14:318---22.
26.ScafidiFA,Field T,SchanbergSM.Factors thatpredictwhich preterminfantsbenefitmostfrommassagetherapy.JDevBehav Pediatr.1993;14:176---80.
27.DieterJN, FieldT, Hernandez-Reif M, EmoryEK, RedzepiM. Stablepreterminfantsgainmoreweightandsleeplessafterfive daysofmassagetherapy.JPediatrPsychol.2003;28:403---11.
28.Diego MA, Field T, Hernandez-Reif M. Vagal activity, gastric motility,andweightgaininmassagedpretermneonates.J Pedi-atr.2005;147:50---5.
29.DiegoMA, Field T, Hernandez-Reif M,Deeds O, AscencioA, BegertG.Preterminfantmassageelicitsconsistentincreases invagalactivityandgastricmotilitythatare associatedwith greaterweightgain.ActaPaediatr.2007;96:1588---91.
30.FieldT,DiegoM,Hernandez-ReifM,DieterJN,KumarAM, Schan-bergS,etal.Insulinandinsulin-likegrowthfactor-1increased inpretermneonates followingmassagetherapy.JDevBehav Pediatr.2008;29:463---6.
31.MassaroAN,HammadTA,JazzoB,AlyH.Massagewith kines-theticstimulationimprovesweightgaininpreterminfants.J Perinatol.2009;29:352---7.
32. Ang JY,Lua JL,Mathur A, Thomas R, AsmarBI, Savasan S, etal.Arandomizedplacebo-controlledtrialofmassage ther-apy on the immune system of preterm infants. Pediatrics. 2012;130:e1549---58.
Tactilekinestheticstimulationinpreterminfants 233
34.KumarJ,UpadhyayA,DwivediAK,GothwalS,JaiswalV, Aggar-walS.Effect of oilmassage ongrowth inpretermneonates lessthan1800g:arandomizedcontroltrial.IndianJPediatr. 2013;80:465---9.
35.AbdallahB,BadrLK,HawwariM.Theefficacyofmassageon shortandlongtermoutcomesinpreterminfants.InfantBehav Dev.2013;36:662---9.
36.ProcianoyRS,MendesEW,SilveiraRC.Massagetherapyimproves neurodevelopment outcome at two years corrected age for very low birth weight infants. Early Hum Dev. 2010;86: 7---11.
37.Moyer-MileurLJ,HaleyS,SlaterH,BeachyJ,SmithSL.Massage improvesgrowthqualitybydecreasingbodyfatdepositionin malepreterminfants.JPediatr.2013;162:490---5.
38.LivingstonK,BeiderS,KantAJ,GallardoCC,JosephMH,Gold JI.Touchandmassageformedicallyfragileinfants.EvidBased ComplementAlternatMed.2009;6:473---82.
39.Benavides-González H, Rivera-Rueda MA, Ibarra-Reyes MP, Flores-TamezME,Fragoso-RamirezA,Morán-MartínezN,etal. Effectsof earlymultimodalstimulation onpretermnewborn infants.BolMedHospInfantMex.1989;46:789---95.
40.Vaivre-Douret L, Oriot D, Blossier P, PyA, Kasolter-Péré M, Zwang J. The effect of multimodal stimulation and cuta-neousapplicationofvegetableoilsonneonataldevelopment inpreterminfants:arandomizedcontrolledtrial.ChildCare HealthDev.2009;35:96---105.
41.SankaranarayananK, MondkarJA, ChauhanMM,Mascarenhas BM,MainkarAR,SalviRY.Oilmassageinneonates:anopen ran-domizedcontrolledstudyofcoconutversusmineraloil.Indian Pediatr.2005;42:877---84.
42.Field T, Diego MA, Hernandez-Reif M, Deeds O, Figuereido B. Moderate versus light pressure massage therapy leads to greater weight gain in preterm infants. Infant Behav Dev. 2006;29:574---8.
43.LahatS,MimouniFB,AshbelG,DollbergS.Energyexpenditure ingrowingpreterminfantsreceivingmassagetherapy.JAmColl Nutr.2007;26:356---9.
44.DiegoMA, Field T,Hernandez-Reif M. Temperature increases inpreterminfantsduringmassagetherapy.InfantBehavDev. 2008;31:149---52.
45.AlyH,MoustafaMF,HassaneinSM,MassaroAN,AmerHA,Patel K. Physical activity combined with massage improves bone mineralizationinprematureinfants:arandomizedtrial.J Peri-natol.2004;24:305---9.
46.Moyer-MileurLJ,BrunstetterV,McNaughtTP,GillG,ChanGM. Dailyphysical activityprogramincreases bonemineralization andgrowthinpretermverylowbirthweightinfants.Pediatrics. 2000;106:1088---92.
47.VignochiCM,MiuraE,CananiLH.Effectsofmotorphysical ther-apyonbonemineralizationinprematureinfants:arandomized controlledstudy.JPerinatol.2008;28:624---31.
48.Vignochi CM,Silveira RC, Miura E,Canani LH, ProcianoyRS. Physicaltherapyreducesboneresorptionandincreases bone formationinpreterminfants.AmJPerinatol.2012;29:573---8.
49.LitmanovitzI,DolfinT,ArnonS,RegevRH,NemetD,EliakimA. Assistedexerciseandbonestrengthinpreterminfants.Calcif TissueInt.2007;80:39---43.