w w w . r b o . o r g . b r
Original
Article
Length
of
preoperative
hospital
stay:
a
risk
factor
for
reducing
surgical
infection
in
femoral
fracture
cases
Hoberdan
Oliveira
Pereira
a,∗,
Edna
Maria
Rezende
a,
Bráulio
Roberto
Gonc¸alves
Marinho
Couto
baDepartmentofNursing,FederalUniversityofMinasGerais(UFMG),BeloHorizonte,MG,Brazil
bInstituteofEngineeringandTechnology,UniversityCenterofBeloHorizonte(UNIBH),BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23September2014 Accepted14November2014 Availableonline23October2015
Keywords:
Infectionoftheoperativewound Femoralfractures
Riskfactors
a
b
s
t
r
a
c
t
Objective:Toanalyzeinfectionsofthesurgicalsiteamongpatientsundergoingclean-wound surgeryforcorrectionoffemoralfractures.
Methods:Thiswasahistoricalcohortstudydevelopedinalarge-sizedhospitalinBelo Hor-izonte.DatacoveringtheperiodfromJuly2007toJuly2009weregatheredfromtherecords inelectronicmedicalfiles,relatingtothecharacteristicsofthepatients,surgicalprocedures andsurgicalinfections.Theriskfactorsforinfectionwereidentifiedbymeansofstatistical testsonbilateralhypotheses,takingthesignificanceleveltobe5%.Continuousvariables wereevaluatedusingStudent’sttest.Categoricalvariableswereevaluatedusingthe chi-squaretest,orFisher’sexacttest,whennecessary.Foreachfactorunderanalysis,apoint estimateandthe95%confidenceintervalfortherelativeriskwereobtained.Inthefinal stageofthestudy,multivariatelogisticregressionanalysiswasperformed.
Results:432patientswhounderwentclean-woundsurgeryforcorrectingfemoralfractures wereincludedinthisstudy.Therateofincidenceofsurgicalsiteinfectionswas4.9%and theriskfactorsidentifiedwerethepresenceofstroke(oddsratio,OR=5.0)andlengthof preoperativehospitalstaygreaterthanfourdays(OR=3.3).
Conclusion:Topreventsurgicalsiteinfectionsinoperationsfortreatingfemoralfractures, measuresinvolvingassessmentofpatients’clinicalconditionsbyamultiprofessionalteam, reductionofthelengthofpreoperativehospitalstayandpreventionofcomplications result-ingfrominfectionswillbenecessary.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](H.O.Pereira). http://dx.doi.org/10.1016/j.rboe.2015.09.006
Tempo
de
internac¸ão
pré-operatório:
um
fator
de
risco
para
reduzir
a
infecc¸ão
cirúrgica
em
fraturas
de
fêmur
Palavras-chave:
Infecc¸ãodaferidaoperatória Fraturasdofêmur
Fatoresderisco
r
e
s
u
m
o
Objetivo:Analisarasinfecc¸õesdesítiocirúrgicoempacientessubmetidosacirurgiaslimpas paracorrec¸ãodefraturasdefêmur.
Métodos: EstudotipocoortehistóricadesenvolvidoemumhospitaldegrandeportedeBelo Horizonte.Acoletadosdadosfoifeitanosregistrosdosprontuárioseletrônicos,dejulho de2007ajulhode2009.Foramcoletadosdadosreferentesàscaracterísticasdospacientes, dosprocedimentoscirúrgicosedasinfecc¸õescirúrgicas.Osfatoresderiscoparainfecc¸ão foramidentificadospormeiodetestesestatísticosdehipótesesbilaterais,considerando níveldesignificânciade5%.AsvariáveiscontínuasforamavaliadasportestetdeStudent. Asvariáveiscategóricasforamanalisadaspormeiodetestedequi-quadradoouexatode Fisher,quandonecessário.Paracadafatorsobanálise,foiobtidaumaestimativapontual eporintervalosdeconfianc¸ade95%paraoriscorelativo.Naúltimaetapadotrabalho,foi feitaumaanálisemultivariada(regressãologística).
Resultados: Foramincluídosnesteestudo432pacientessubmetidosacirurgiaslimpasde correc¸ãodefraturadefêmur.AtaxadeincidênciadeISCfoide4,9%eosfatoresderisco identificadosforamapresenc¸adeacidentevascularcerebral(razãodaschances–OR=5)e períododeinternac¸ãoatéacirurgiaacimadequatrodias(OR=3,3).
Conclusão:Paraaprevenc¸ãodasinfecc¸õesdesítiocirúrgico(ISC)dascirurgiasdefraturasde fêmurserãonecessáriasmedidasqueenvolvamaequipemultiprofissionalnaavaliac¸ãodas condic¸õesclínicasdospacientes,reduc¸ãodotempodeinternac¸ãoatéacirurgiaeprevenc¸ão dascomplicac¸õesdecorrentesdasinfecc¸ões.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Surgicalsiteinfection(SSI)isadisastrousadverseeventfor bothpatients andsurgeons, especiallyin clean surgeryfor open reductionoffractures ofthe femurand hip. InLatin America,thefinancialcostsinvolvedinfracturesofthe prox-imalfemurwereassessedbetween1980and2003andwere foundtorangefromUS$4500toUS$6000perpatient.InBrazil, theseamountsmayreachUS$5500perpatient.1Everyyear,
theBrazilianNationalHealthSystem(SistemaÚnicodeSaúde, SUS)undertakesgreaternumbersoftreatmentsonfemoral fractures in elderly patients. In 2009, the expenditure was approximatelyR$57.61milliononadmissionsversusR$24.77 milliononmedicationsfortreatingosteoporosis,whichisan importantcauseoffemoralfractures.In2006,these expendi-tureshadbeenR$49millionandR$20million,respectively. Hannanetal.,2 statedthatthesocialandeconomiccostof
femoralfracturesbecomesevengreaterbecauseafteraperiod of hospitalization, elderly patients need intensive medical careandlongperiodsofrehabilitation,andalsopresentahigh mortalityrate.Thetreatmentformostfemoralfracturesis sur-gical.Inusingnewmaterialsforreplacingprostheses,lower complicationratesthroughbettertechnologyanddesignare sought.Accordingtothepotentialofsurgicalproceduresfor woundcontamination,theycanbeclassifiedasclean, poten-tiallycontaminated,contaminatedorinfected.Arrowsmith3
notedthatcleansurgicalproceduresoughttohavelower inci-denceofsurgicalsiteinfection(SSI)becausetheypresented
lowerriskofcontaminationthanothercategories.Such pro-ceduresareconsideredtobemarkersofservicequalityand presentbetterexecution(elective,non-traumatic,tissuesthat areeasilydecontaminatedandintactskin).Therateof inci-denceofSSIshouldbelessthan2%.
Several risk factors relating to the patient and to the surgicalprocedure havebeen correlatedwiththeincidence ofSSIinfemoralfractures.Theintrinsicfactors relatingto elderlypatientscompriseinadequatenutritionalstatus, dia-betes mellitus (DM), use of tobacco, obesity, surgical site infection,colonizationoftheskin,immuneresponseand pro-longedperiodofpreoperativehospitalization.1Theextrinsic
factors associatedwiththeoperationandthe patient com-priseskinpreparation,appropriateclothes,preparationofthe surgicalteam’shands,durationoftheoperation,surgical tech-nique,processingofmaterialsandarticles,preparationofthe antibioticand preparationofthesurgicalsite. Controlover thesefactorsisessentialforminimizingthecontamination ofthesurgicalsite.4Studieshaveemphasizedtheneedto
pri-oritizecareforpatientswithfemoralfractures,especiallyin relationtothetimethatelapsedbetweenthefractureandthe surgicalprocedure.5
increasethepatient’sriskofdeathafterthesurgery?(4)Does SSIincreasethepatient’slengthofhospitalstay?and(5)What aretheriskfactorsassociatedwithSSIafteropenreductionof femoralfractures?
Materials
and
methods
ThiswasaprospectivecohortstudyconductedtoanalyzeSSI andits riskfactorsamongpatientswho underwent correc-tionoffracturesofthehipandfemur,betweenJuly2007and July2009.Thestudy wasconductedinalarge-sized hospi-tal,withacapacityforaround350beds,whichisareferral centerforaccidentsandemergenciesinthestateofMinas Gerais, Brazil. The sample was composed of 432 patients whounderwentelectivesurgerytocorrectfemoralfractures. Theresponsevariablescomprisedsurgicalsiteinfectionand hospitaldeath. Thepreoperativeand operativeparameters weredividedintocategoricalandcontinuousvariables.The continuous variables studied were age, duration of preop-erative hospitalization and duration of the operation. The categoricalvariableswere sex,typeofsurgery, shiftduring whichtheoperationwasperformed(morning,afternoonor night),typeofanesthesia,preoperativeassessmentscoreof the American Societyof Anesthesiology(ASA),Nosocomial InfectionSurveillance index, fracture classification, typeof injury, typeofosteosynthesis and typeofsurgery (elective oremergency).Thecomorbiditiesstudiedwerediabetes mel-litus(DM), congestive heart failure (CHF), systemic arterial hypertension(SAH), chronicobstructive pulmonarydisease (COPD),heartdiseases,hypercholesterolemia,alcoholabuse, psychiatricdisorders,cancerofmetabolicdisease,strokeand anemia.Thetypeofanesthesiawasclassifiedaccordingtothe combinationoftwoormoreprocedureswithorwithout seda-tion.Hospitalizationbeforesurgerywasdefinedasuptofour daysbeforeitormorethanfourdaysbeforeit.6Theduration
ofthesurgerywasstratifiedaslessthanorequalto138minof morethanthisduration.TheASAscorewascategorizedinto levelsI,II,IIIandIV:ASAIforhealthypatients;IIforpatients withmoderatesystemicdisease;IIIforpatientswithsevere preexistingsystemicdiseases thatwere notincapacitating; andIVforpatientswithlife-threateningsystemicdisease. Cat-egoryV-5,forindividualswithlifeexpectancyofamaximum of24h,wasnotidentifiedinanyofthepatientsofthisstudy. Fortheindexofsurgicalriskofinfection,thescorezerowas usedandthegroupedscoreof1or2wasusedonlyforclean surgery.Theprophylacticantibioticwastestedforusebefore orduringthesurgery.
Theclassificationoffemoralfractureswasbasedonregions of the femur: fractures of the femoral neck,7 trochanteric
fractures8 orsubtrochantericfractures.9 Forfracturesofthe
diaphysis,theAOclassificationwasused.10Forsome
opera-tions,theclassificationwasnotshown.WeusedtheICD-10 tocodeandgroupthisvariable.11Fivetypesofosteosynthesis
wereused:plate,nail,screw,cementandothers.Thepatients includedwerehospitalizedandunderwentcleansurgical cor-rectionoffemoralfracturesbetweenJuly2007andJuly2009.
Riskfactorsandprotectivefactorsforinfectionwere iden-tified bymeans ofstatistical testson bilateral hypotheses, inwhichthesignificancelevelwastakentobe5%(˛=0.05).
ContinuousvariableswereevaluatedusingStudent’sttestor anonparametrictest,andcategoricalvariableswereanalyzed using thechi-square orFisherexact test(whennecessary). Foreachfactorunderanalysis,apointanalysisand95% con-fidenceinterval(95%CI)fortherelativeriskwereobtained. Inthelastphaseofthestudy,multivariateanalysiswas con-ductedusinglogisticregression.Thevariablestestedinthe logisticmodelwereselectedwhentheunivariateanalysis gen-eratedavalueofp≤0.25.
Thisstudywasapprovedbythehospitalinvolved,under report no.18 and bythe researchethics committee,under CAEEreportno.0108.0.203.000-11,whichwasapprovedonMay 5,2011,inconformitywithresolution196/96.
Results
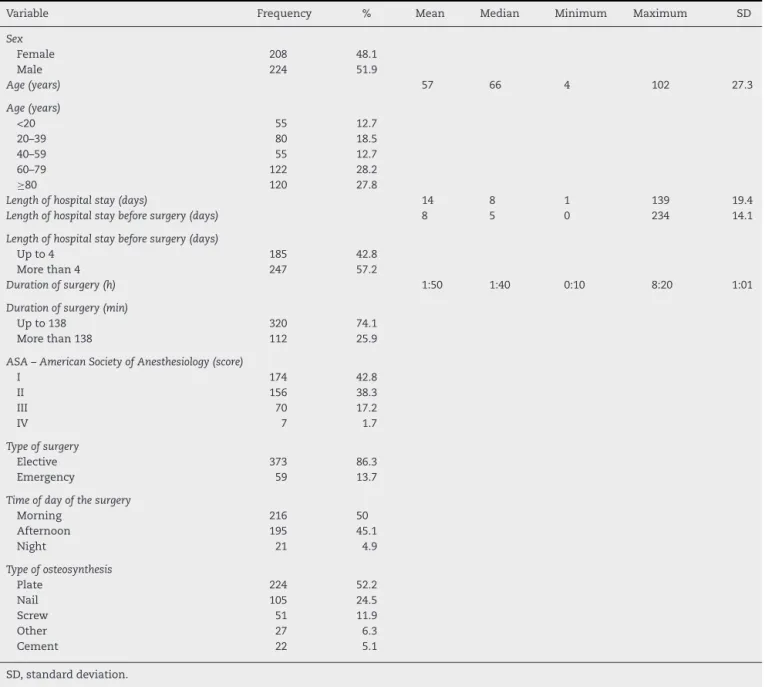
Thisstudyincluded432patientswhounderwentopen reduc-tion offemoral fractures between July 2007and July 2009. Fallingfromastandingposition,fallingfromabedandfalling from a staircase were the most frequent types of trauma amongthepatientswithfemoralfractureswhowere evalu-ated.Thesepatientsaccountedfor59%ofthecasesandwere followed bythose involvedinmotorcycleaccidents(15.5%). Thepatients’lengthofhospitalstayrangedfromoneto139 days,withamedianofeightdays.Themeantimespentin hos-pitalbeforethesurgerywasfivedaysand43%ofthepatients wereinhospitalforuptofourdays.Thepatients’meanlength ofstayinthesurgicalcenterwassixhours.Themean dura-tionoftheoperationwasonehourand50minandmorethan 70%oftheoperationslastedfornotmorethan138min.Most ofthepatientswereovertheageof60years;36%cametothe hospitalviaanemergencyunit;and5%presentedmorethan twodiagnosesatthetimeofhospitaladmission(Tables1–3).
Amongthe432patientswhounderwentcorrectionofclean fracturesofthefemur,21patientswererecordedaspresenting SSI.Theriskofinfectionwas4.9%.
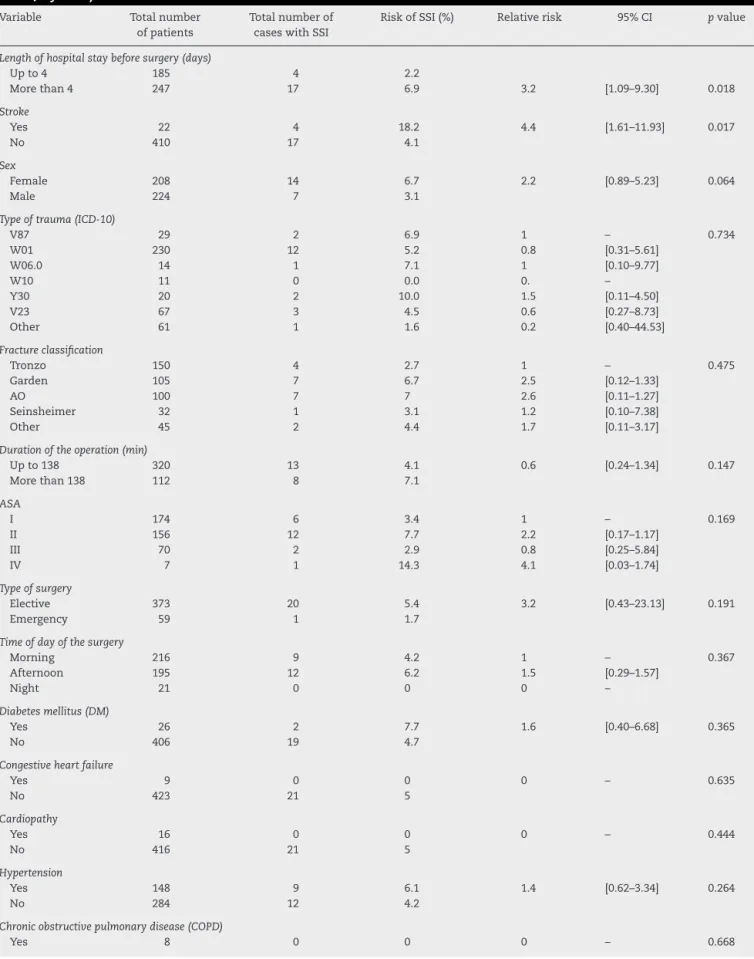
Strokeandlengthofstaygreaterthanfourdayspresented statisticallysignificantassociationswithSSI(Table4).
Itwasfoundthatforthepatientswithstrokewhoremained inhospitalformorethanfourdays,theexpectedriskof acquir-ing infection was almost threetimes greater than the risk amongthosewhohadthisdiseasebutwereinhospitalfornot morethanfourdays.Strokeandlengthofhospitalstayuntil thesurgerywerethevariablesassociatedwithSSI(Table5).
Regardinghospitalmortalityaftersurgicalcorrectionofthe femoralfracture,SSIwasnotassociatedwiththechanceof death(p=0.125)(Table6).
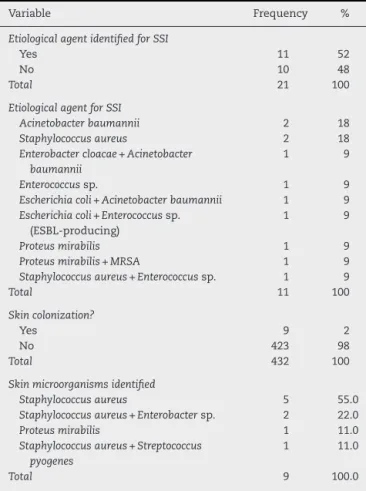
In10ofthe21casesofinfectionregistered,theetiological agentremainedunidentified.Staphylococcusaureusand Acine-tobacterbaumanniiwerethemicroorganismsmostfrequently identified.Only2%ofthe432patientspresentedpreoperative colonization,whichwasmostlydetectedbymeansofnasal andaxillaryswabs(Table7).
Discussion
Table1–Opensurgeryforcorrectingfemoralfracturesinatertiary-levelhospital:patients’characteristicsandsurgical characteristics(July2007–July2009).
Variable Frequency % Mean Median Minimum Maximum SD
Sex
Female 208 48.1
Male 224 51.9
Age(years) 57 66 4 102 27.3
Age(years)
<20 55 12.7
20–39 80 18.5
40–59 55 12.7
60–79 122 28.2
≥80 120 27.8
Lengthofhospitalstay(days) 14 8 1 139 19.4
Lengthofhospitalstaybeforesurgery(days) 8 5 0 234 14.1
Lengthofhospitalstaybeforesurgery(days)
Upto4 185 42.8
Morethan4 247 57.2
Durationofsurgery(h) 1:50 1:40 0:10 8:20 1:01
Durationofsurgery(min)
Upto138 320 74.1
Morethan138 112 25.9
ASA–AmericanSocietyofAnesthesiology(score)
I 174 42.8
II 156 38.3
III 70 17.2
IV 7 1.7
Typeofsurgery
Elective 373 86.3
Emergency 59 13.7
Timeofdayofthesurgery
Morning 216 50
Afternoon 195 45.1
Night 21 4.9
Typeofosteosynthesis
Plate 224 52.2
Nail 105 24.5
Screw 51 11.9
Other 27 6.3
Cement 22 5.1
SD,standarddeviation.
emphasizingthattherateofSSIincleansurgeryinthis hos-pitaloverthesameperiodofJuly2007toJuly2009,takinginto accountallbodyareasandspecialties,suchasorthopedics, plasticsurgery,generalsurgeryandneurosurgery,was approx-imately2.2%.ItisnecessarytoinvestigatetheratesofSSIper surgeonandtomonitortheriskfactorsrelatingtopatientsand tothe surgicalprocedure.Efficientmonitoringsystemsand informationforsurgeonsregardingtheirinfectionrateshave demonstratedbetterpreventionofSSI.Theinfectionratescan bereducedbymorethanonethirdthroughprogramsand per-sonnelwhoaretrainedinmonitoringandinfectioncontrol.13
Thestudypopulationwascomposedofpatientswhowere mostlymale,includingadolescents,youngadultsandelderly individualsovertheageof60years,perhapsbecausethisisa referralhospitalforattendingtoemergencies.However,many authorsconsiderthatwomenarethegroupmostsubjectto femoralfractures,1andthatstudyshowedagreaterriskofSSI.
Pereira14studiedgroupsofelderlypeopleandfoundthatthe
rateofincidenceofhipfracturesamongwomenwas72.76%. The classification for the femoral fractures was estab-lishedinaccordancewiththeregionaffected:femoralneck, trochanterorsubtrochantericdiaphysis.Munizetal.15showed
thatthemaintypesoffractureweretranstrochanteric(58.73%) and femoralneck(38.20%),whichare consideredtobedue to low-energy trauma. In the present study, trochanteric fractureshadhigherfrequency,butdiaphysealfractures pre-sentedhigherriskofSSI,albeitwithoutstatisticalsignificance. The length of hospital stay after the operation (four days)wasstatisticallysignificant inourunivariateanalysis (p=0.018).Thisassociationwasmaintainedinthe multivari-ateanalysis,thusconfirmingthepresenceofthisriskfactorfor SSI.Prolongedpreoperativehospitalstayhasbeencorrelated withariskofSSI.6Thedurationoftheoperationwasassessed
Table2–Univariateanalysisonthecategoricalvariables:lengthofpreoperativehospitalstaygreaterthanfourdaysand strokewereriskfactorsforSSI,aftersurgerytocorrectfemoralfractures,atthe5%significancelevel(p<0.05)(July 2007–July2009).
Variable Totalnumber ofpatients
Totalnumberof caseswithSSI
RiskofSSI(%) Relativerisk 95%CI pvalue
Lengthofhospitalstaybeforesurgery(days)
Upto4 185 4 2.2
Morethan4 247 17 6.9 3.2 [1.09–9.30] 0.018
Stroke
Yes 22 4 18.2 4.4 [1.61–11.93] 0.017
No 410 17 4.1
Sex
Female 208 14 6.7 2.2 [0.89–5.23] 0.064
Male 224 7 3.1
Typeoftrauma(ICD-10)
V87 29 2 6.9 1 – 0.734
W01 230 12 5.2 0.8 [0.31–5.61]
W06.0 14 1 7.1 1 [0.10–9.77]
W10 11 0 0.0 0. –
Y30 20 2 10.0 1.5 [0.11–4.50]
V23 67 3 4.5 0.6 [0.27–8.73]
Other 61 1 1.6 0.2 [0.40–44.53]
Fractureclassification
Tronzo 150 4 2.7 1 – 0.475
Garden 105 7 6.7 2.5 [0.12–1.33]
AO 100 7 7 2.6 [0.11–1.27]
Seinsheimer 32 1 3.1 1.2 [0.10–7.38]
Other 45 2 4.4 1.7 [0.11–3.17]
Durationoftheoperation(min)
Upto138 320 13 4.1 0.6 [0.24–1.34] 0.147
Morethan138 112 8 7.1
ASA
I 174 6 3.4 1 – 0.169
II 156 12 7.7 2.2 [0.17–1.17]
III 70 2 2.9 0.8 [0.25–5.84]
IV 7 1 14.3 4.1 [0.03–1.74]
Typeofsurgery
Elective 373 20 5.4 3.2 [0.43–23.13] 0.191
Emergency 59 1 1.7
Timeofdayofthesurgery
Morning 216 9 4.2 1 – 0.367
Afternoon 195 12 6.2 1.5 [0.29–1.57]
Night 21 0 0 0 –
Diabetesmellitus(DM)
Yes 26 2 7.7 1.6 [0.40–6.68] 0.365
No 406 19 4.7
Congestiveheartfailure
Yes 9 0 0 0 – 0.635
No 423 21 5
Cardiopathy
Yes 16 0 0 0 – 0.444
No 416 21 5
Hypertension
Yes 148 9 6.1 1.4 [0.62–3.34] 0.264
No 284 12 4.2
Chronicobstructivepulmonarydisease(COPD)
Table2–(Continued)
Variable Totalnumber ofpatients
Totalnumberof caseswithSSI
RiskofSSI(%) Relativerisk 95%CI pvalue
No 424 21 5
Hypercholesterolemia
Yes 3 0 0 0 – 0.860
No 429 21 4.9
Alcoholabuse
Yes 19 1 5.3 1.1 [0.15–7.68] 0.620
No 413 20 4.8
Psychiatricdisorders
Yes 18 1 5.6 1.2 [0.16–8.10] 0.599
No 414 20 4.8
Metabolicdisorders
Yes 9 0 0 0 – 0.635
No 423 21 5
Cancer
Yes 12 0 0 0 – 0.545
No 420 21 5
Typeofosteosynthesis
Plate 224 15 6.7 1 – 0.246
Nail 105 2 1.9 0.3 [0.82–15.09]
Screw 51 1 2 0.3 [0.46–25.27]
Other 27 1 3.7 0.6 [0.03–8.14]
Cement 22 2 9.1 1.4 [0.04–4.20]
Anesthesia:spinalanesthesiawithsedation
Yes 224 14 6.3 1.9 [0.76–4.71] 0.120
No 208 7 3.4
Surgicalinfectionriskindex
Score0 246 11 4.5 0.7 [0.31–1.66] 0.585
Scoreupto2 161 10 6.2
Anemia
Yes 178 10 5.6 1.4 [0.59–3.43] 0.288
No 228 9 3.9
Hematocritlessthan36mg/dL
Yes 259 15 5.8 2.1 [0.72–6.29] 0.120
No 147 4 2.7
Skincolonization
Yes 17 1 5.9 1.2 [0.17–8.57] 0.578
No 415 20 4.8
Generalanesthesia
Yes 41 2 4.9 1 [0.24–4.16] 0.620
No 391 19 4.9
ASA,AmericanSocietyofAnesthesiology;95%CI,95%confidenceinterval;SSI,surgicalsiteinfection;RR,relativerisk;ICD-10,international classificationofdiseases.
whichthenumberofminutesdefinedforthistypeofoperation was138.Althoughthisisavariableclassicallyassociatedwith SSI,itwasnotassociatedwithsurgicalinfectioninthepresent study.Longdurationofanoperationinacontaminated envi-ronment favors surgical contamination and, consequently, developmentofinfection.17
TheASAvariable,whichassessesthepatient’s preopera-tiveclinicalstatewasnotconsideredtobeariskfactorfor SSI in the present study. Although the patients were pre-dominantly gradedas ASAI, those withASA IVpresented ariskofSSIthatwasfourtimeshigher.Manyauthorshave considered that the ASAscore isa risk factor forSSI that
relatesdirectlytotheseverityofthepatient’sconditionand the risk of infection.18 Plates were the synthesis material
mostused,in224cases(51%).Sakakietal.,1 statedthatthe
treatment forthe majority of femoral fractures should be surgical.Conservativetreatmentshouldbereservedonlyfor someincompleteornon-displacedfractures.Theaimofthe surgeryistoreducethefractureandfixitinastablemanner, using avarietyofosteosynthesis methods.Spinal anesthe-siawithsedationistheanestheticproceduremostusedand theriskofinfectioninrelationtopatientsforwhomthiswas not usedhasbeen found tobe1.9%. Ercoleand Chianca19
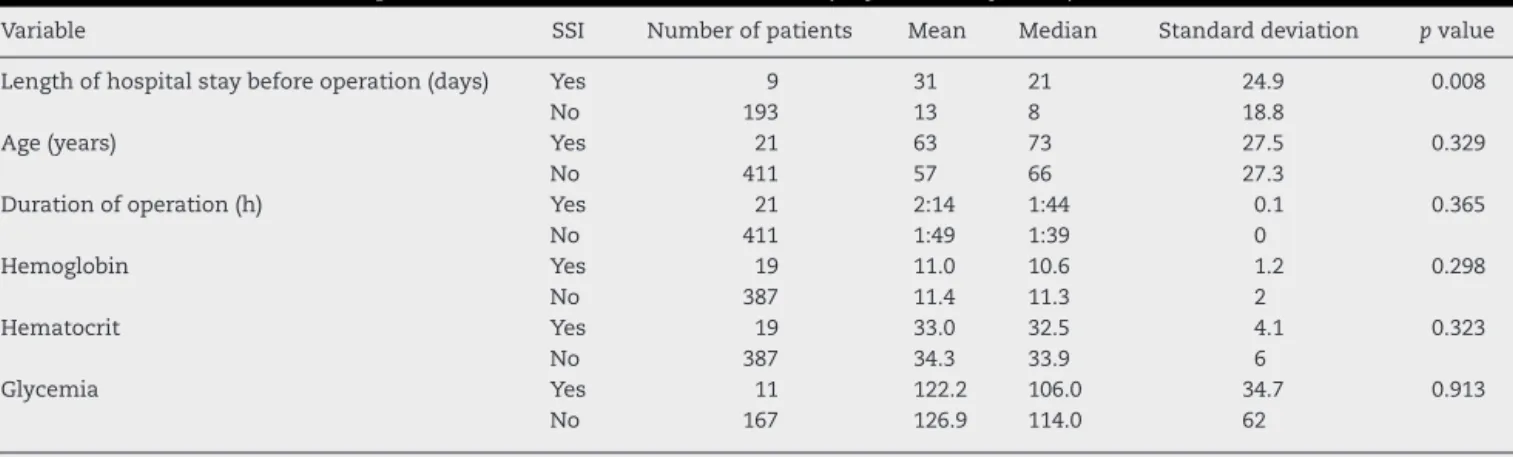
Table3–Univariateanalysisonthecontinuousvariables:onlythelengthofhospitalstaybeforetheoperation(days)was associatedwithSSIaftertheoperationtocorrectfemoralfractures(July2007–July2009).
Variable SSI Numberofpatients Mean Median Standarddeviation pvalue
Lengthofhospitalstaybeforeoperation(days) Yes 9 31 21 24.9 0.008
No 193 13 8 18.8
Age(years) Yes 21 63 73 27.5 0.329
No 411 57 66 27.3
Durationofoperation(h) Yes 21 2:14 1:44 0.1 0.365
No 411 1:49 1:39 0
Hemoglobin Yes 19 11.0 10.6 1.2 0.298
No 387 11.4 11.3 2
Hematocrit Yes 19 33.0 32.5 4.1 0.323
No 387 34.3 33.9 6
Glycemia Yes 11 122.2 106.0 34.7 0.913
No 167 126.9 114.0 62
SSI,surgicalsiteinfection.
Table4–Analysisofvariance:inthefinalmodel,thelengthofhospitalstaybeforetheoperationandstrokewere independentlyassociatedwithsurgicalsiteinfectionaftertheoperationtocorrectfemoralfractures.Preoperativelength ofhospitalstaygreaterthanfourdaysincreasedthechancethatapatientwouldbeinfectedalmostthreefold(OR=3.3; p=0.037)(July2007–July2009).
Variable Regressioncoefficient Standarderrorofthe regressioncoefficient
Oddsratio pvalue
Preoperativelengthofhospital staygreaterthan4days
1.19 0.57 3.3 0.037
Stroke 1.60 0.62 5 0.009
Constant −3.96 0.52
Table5–SimulationofriskofSSI:lengthofhospitalstaybeforethesurgeryandstroke.
Typeofpatient Expectedrisk
ofSSI(%)
Numberof patients
ObservedSSI Observedrisk ofSSI(%)
Nostrokeandlengthofstayupto4days 1.9 177 2 1.1
Nostrokeandlengthofstaymorethan4days 5.9 233 15 6.4
Previousstrokeandlengthofstayuptofourdaysa 8.6 8 – –
Previousstrokeandlengthofstaymorethanfourdaysa 23.6 14 – –
a Smallsamplesize.
Table6–Hospitalmortalityaftersurgerytocorrectfemoralfractures:surgicalsiteinfectionwasnotassociatedwiththe chanceofdeath(p=0.125)(July2007–July2009).
SSI Numberofpatients Hospitalmortality Riskofhospitaldeath(%) Relativerisk 95%confidenceinterval pvalue
Yes 21 3 14.3 2.6 [0.83–7.83] 0.125
No 411 23 5.6
Total 432 26 6
presented3.4timesgreaterriskofinfectionthanthosewho underwentblocking.Thedatafrom thepresent studywere insufficienttocharacterizeantibioticasaprotectionfactor, althoughthesedatasignaledthat therewere patientswho receivedcefazolinandwhopresentedariskofSSIthatwas aroundfourtimeslower.Inameta-analysis,itwasobserved thatinsurgerytofixclosedfractures,prophylaxiswitha sin-gledoseofantibioticsreduced theseverityofdeep-wound, surface-wound,urinary-tractandrespiratory-tractinfections. That analysis alsoshowed multiple-doseprevention had a similar effecton the size ofdeep-wound infection,but no significant effect on urinary or respiratory infections was confirmed.20
TheetiologicalagentsidentifiedinSSIcaseswere Staphylo-coccusaureus,AcinetobacterbaumanniiandEnterococcussp.In some cases, more than one microorganism was identified fromcultures.Itshouldbenotedthatetiologicalagentswere onlyidentifiedin11ofthe21casesthatpresentedSSI.Thislow proportionoffindingsfromtheculturesperformedexplains theabsenceoftreatmentsguidedbylaboratoryresults.
Themultivariateanalysisconfirmedthatstrokebeforethe cleansurgicalcorrectionoffemoralfractureswas character-izedasariskfactorforSSI.Inacohortstudyinvolving1379 victimsofproximalfemoralfractures,Fengetal.21reported
Table7–Opensurgerytocorrectfemoralfracturesina tertiary-levelhospital:skincolonizationandetiological agentsofthesurgicalsiteinfection(July2007–July2009).
Variable Frequency %
EtiologicalagentidentifiedforSSI
Yes 11 52
No 10 48
Total 21 100
EtiologicalagentforSSI
Acinetobacterbaumannii 2 18
Staphylococcusaureus 2 18
Enterobactercloacae+Acinetobacter baumannii
1 9
Enterococcussp. 1 9
Escherichiacoli+Acinetobacterbaumannii 1 9
Escherichiacoli+Enterococcussp. (ESBL-producing)
1 9
Proteusmirabilis 1 9
Proteusmirabilis+MRSA 1 9
Staphylococcusaureus+Enterococcussp. 1 9
Total 11 100
Skincolonization?
Yes 9 2
No 423 98
Total 432 100
Skinmicroorganismsidentified
Staphylococcusaureus 5 55.0
Staphylococcusaureus+Enterobactersp. 2 22.0
Proteusmirabilis 1 11.0
Staphylococcusaureus+Streptococcus pyogenes
1 11.0
Total 9 100.0
ESBL, extended-spectrum beta lactamase; MRSA, methicillin-resistantStaphylococcusaureus;SSI,surgicalsiteinfection.
ormorecomorbidities,lowercognitivecapacity,weaker pre-fracture outpatient status, longer hospital stay and higher mortalityrate.
Inthe present study,patients with previousstroke pre-sentedfourtimesgreaterriskofdevelopingSSI.Aprospective studyforevaluatingtheeffectoftheanteriorpassageafter occurrences of femoral neck or intertrochanteric fractures showedthatpatientswithhistoriesofstrokeweremorelikely tobe male, haveASA gradesIIIor IV, havethree or more comorbidities,belimitedtomovingaroundathomeandbe dependentinactivitiesofdailyliving(ADLs)and instrumen-talactivities, beforethetimeofthe fracture.Thelengthof hospitalstaywassignificantlygreaterforthesepatients.22
Thelimitationofthepresentstudywasthatitwas retro-spective,withlackofinformationonthepatients’evolution overthecourseofadministrationoftheprophylactic antibi-oticsand lack ofdefinition and adherence criteria for the clinicalevaluationanddetailedhistory-taking.
Conclusion
TheriskfactorsforSSIincasesofcorrectionoffemoral frac-turesthroughcleansurgerythatwereidentifiedinthepresent study were the presence of stroke before the surgery and lengthofhospitalstaybeforetheoperationofmorethanfour
days.Thecombinedactionofthesetwofactorscontributed towardraisingtherateofSSIamongthepatientswho under-went surgerytothreetimestheexpectedrisk.Controlover the risk factors and thetime that elapses untilthe opera-tion ishighlydesirableforreducing theriskofinfectionin thesepatients.TheincidenceofSSIidentifiedincasesofclean surgery on femoralfractures presentedlevels greater than theinfectionraterecordedinthehospital.Cleansurgery per-formedon thefemurshouldbemonitoredand keptunder surveillancebecausethisisamarkerforinfectionassociated withqualitycontrolinhealthcareservices.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.SakakiMH,OliveiraRA,CoelhoFF,GarcezELL,SuzukiI, AmatuzziMM.Estudodamortalidadenafraturadofêmur proximalemidosos.ActaOrtopBras.2004;12(4):242–9. 2.HannanEL,MagazinerJ,WangJJ,EastwoodEA,Silberzweig
SB,GilbertM,etal.Mortalityandlocomotion6monthsafter hospitalizationforhipfracture:riskfactorsandrisk-adjusted hospitaloutcomes.JAMA.2001;285(21):2736–42.
3.ArrowsmithM.Surgicalsiteinfection.In:EmmersonAM, ArrowsmithM,editors.Infectioncontrolpractices.Germany: 3MMedicalMarketsLaboratory;1998.p.60–9.
4.AndersonDJ,KayeKS,ClassenD,AriasKM,PodgornyK, BurstinH,etal.Strategiestopreventsurgicalsiteinfections inacutecarehospitals.InfectControlHospEpidemiol. 2008;29Suppl1:S51–61.
5.MoranCG,WennRT,SikandM,TaylorAM.Earlymortality afterhipfracture:isdelaybeforesurgeryimportant?JBone JointSurgAm.2005;87(3):483–9.
6.ErcoleFF,FrancoCML,MacieiraRGT,WenceslauCCL,Resende NIH,ChiancaMCT.Riscoparainfecc¸ãodesítiocirúrgicoem pacientessubmetidosacirurgiasortopédicas.RevLatino-Am Enfermagem.2011;19(6):1362–8.
7.GardenRS.Thestructureandfunctionoftheproximalendof thefemur.JBoneJointSurgBr.1961;43(3):576–89.
8.TronzoRG.Symposiumonfracturesofthehip.Special considerationsinmanagement.OrthopClinNorthAm. 1974;5(3):571–83.
9.SeinsheimerF.Fraturassubtrocantéricasdofêmur.JBone JointSurgAm.1978;60(3):300–6.
10.MüllerME.AOMullerElectronicLongBoneFracture Classification;2003.Availablein:www.aopublishing.org [accessed25.02.12].
11.Organizac¸ãoMundialdaSaúde/OMS.CID-10.Classificac¸ão estatísticainternacionaldedoenc¸aseproblemas
relacionadosàsaúde.3a.ed.SãoPaulo:OMS;1996.
12.CamargoFGC.Urgênciasclínicasecirúrgicas.RiodeJaneiro: Atheneu;2001.
13.AsturCD,ArlianiGG,BalbachevskyD,FernandesAJH,ReisBF. Fraturasdaextremidadeproximaldofêmurtratadasno HospitalSãoPaulo/UNIFESP:estudoepidemiológico.RBM:Rev BrasMed.2011;68:11–5(númeroespecial).
15.MunizFC,ArnautCA,YoshidaM,TrelhaSC.Caracterizac¸ão dosidososcomfraturadefêmurproximalatendidosem hospital-escolapúblico.RevEspac¸oSaúde.2007;8(2):33–8. 16.CentersforDiseaseControlandPrevention/CDC.The
NationalHealthcareSafetyNetwork(NHSN)manual:patient safetycomponentprotocol.Atlanta:DivisionofHealthcare QualityPromotion,NationalCenterforPreparedness, DetectionandControlofInfectiousDiseases;2009,210p. Availablein:http://www.cdc.gov/nhsn/library.html#psc [accessed20.09.09].
17.LewDP,PittetD,WaldvogelFA.Infectionsthatcomplicatethe insertionofprostheticdevices.In:MayhallCG,editor. Hospitalepidemiologyandinfectioncontrol.3rded. Philadelphia:LippincottWillians&Wikins;2004. p.1181–205.
18.OliveiraAC,BrazNJ,RibeiroMM.Incidênciadainfecc¸ãodo sítiocirúrgicoemumhospitaluniversitário.CiencCuid Saúde.2007;6(4):486–93.
19.ErcoleFF,ChiancaTCM.Infecc¸ãodesítiocirúrgicoem pacientessubmetidosaartroplastiasdequadril.Rev Latino-AmEnfermagem.2002;10(2):157–65.
20.GillespieWJ,WalenkampG.Antibioticprophylaxisforsurgery forproximalfemoralandotherclosedlongbonefractures. CochraneDatabaseSystRev.2010;3:CD000244.
21.FengM,ZhangJ,ShenH,HuH,CaoL.Predictorsofprognosis forelderlypatientswithpoststrokehemiplegiaexperiencing hipfractures.ClinOrthopRelatRes.2009;467(11):2970–8. 22.YoumT,AharonoffG,ZuckermanJD,KovalKJ.Effectof