w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Swiss
ball
exercises
improve
muscle
strength
and
walking
performance
in
ankylosing
spondylitis:
a
randomized
controlled
trial
Marcelo
Cardoso
de
Souza
a,b,
Fábio
Jennings
a,
Hisa
Morimoto
a,
Jamil
Natour
a,∗aUniversidadeFederaldeSãoPaulo(Unifesp),EscolaPaulistadeMedicina(EPM),DisciplinadeReumatologia,SãoPaulo,SP,Brazil bUniversidadeFederaldoRioGrandedoNorte(UFRN),FaculdadedeCiênciasdaSaúdedoTrairí(Facisa),CursodeFisioterapia,
SantaCruz,RN,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12January2016 Accepted28April2016
Availableonline20October2016
Keywords:
Exercises
Resistanceexercises Swissball
Ankylosingspondylitis
a
b
s
t
r
a
c
t
Objective:Thepurposewastoevaluatetheeffectivenessofaprogressivemuscle strength-eningprogramusingaSwissballforASpatients.
Methods:SixtypatientswithASwererandomizedintotheinterventiongroup(IG)orthe controlgroup(CG).EightexerciseswereperformedbytheIGpatientswithfreeweightson aSwissballtwotimesperweekfor16weeks.Theevaluationswereperformedbyablinded evaluatoratbaselineandafter4,8,12and16weeksusingthefollowinginstruments:the one-repetitionmaximumtest(1RM),BASMI,BASFI,HAQ-S,SF-36,6-minutewalktest,time upandgotest,BASDAI,ASDAS,ESRandCRPdosageandLikertscale.
Results:Therewasastatisticaldifferencebetweengroupsfor:strength(1RMcapacity)inthe followingexercises:abdominal,rowing,squat,tricepsandreversefly(p<0.005);6-minute walktest(p<0.001);timedupandgotest(p=0.025)andLikertscale(p<0.001),allofthem withbetterresultsfortheIG.Nodifferenceswereobservedbetweenthegroupswithrespect tothefunctionalcapacityevaluationusingtheBASFI,HAQ-S,BASMI,SF-36,TUG,ASDAS, ESRandCPRdosage.
Conclusions: ProgressivemusclestrengtheningusingaSwissballiseffectiveforimproving musclestrengthandwalkingperformanceinpatientswithAS.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](J.Natour).
http://dx.doi.org/10.1016/j.rbre.2016.09.009
Exercícios
na
bola
suíc¸a
melhoram
a
forc¸a
muscular
e
o
desempenho
na
caminhada
na
espondilite
anquilosante:
ensaio
clínico,
controlado
e
randomizado
Palavras-chave:
Exercícios
Exercíciosresistidos Bolasuíc¸a
Espondiliteanquilosante
r
e
s
u
m
o
Objetivo:Avaliaraefetividadedeumprogramadefortalecimentomuscularprogressivocom ousodeumabolasuíc¸aempacientescomespondiliteanquilosante(EA).
Métodos: SessentapacientescomEAforamrandomizadosemgrupointervenc¸ão(GI)ou grupocontrole(GC).OspacientescomEAfizeramoitoexercícioscompesoslivresemuma bolasuíc¸aduasvezesporsemanadurante16semanas.Asavaliac¸õesforamfeitasporum avaliadorcegonoiníciodoestudoeapósquatro,oito,12e16semanascomosseguintes instrumentos:testedeumarepetic¸ãomáxima(1RM),Basmi,Basfi,HAQ-S,SF-36,testede caminhadadeseisminutos,Timedupandgotest,Basdai,Asdas,dosagemdeVHSePCRe escaladeLikert.
Resultados: Houveumadiferenc¸aestatisticamentesignificativaentreosgruposemrelac¸ão à forc¸a (capacidade no teste de 1 RM) nos seguintes exercícios: abdominal, remada, agachamento,trícepsecrucifixoinvertido(p<0,005);testedecaminhadadeseisminutos (p<0,001);Timedupandgotest(p=0,025);eescaladeLikert(p<0,001),todoscommelhores resultadosnoGI.Nãoforamobservadasdiferenc¸asentreosgruposemrelac¸ãoàavaliac¸ão dacapacidadefuncionalcomBasfi,HAQ-S,Basmi,SF-36,TUG,Asdas,VHSedosagemde PCR.
Conclusões: Ofortalecimentomuscularprogressivocomumabolasuíc¸aéefetivoem mel-horaraforc¸amusculareodesempenhonacaminhadaempacientescomEA.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Ankylosingspondylitis(AS)isaninflammatorydiseasethat affects the axial skeleton and causes low back pain and functionalimpairment.Thediseasecausesinflammationand paininthespineandjoints,whichreducesphysicalactivity andspinalmobilityandcauses fatigue,stiffness,sleep dis-ordersanddepression.1Exercisesareimportanttomaintain
orimprovespinalmobilityandphysicalfitnessaswellasto reducepainandareincludedinevidence-based recommen-dationsforthemanagementofAS.2
Onestudyshowedthatweaknessofperipheralmusclesof thelimbs(speciallythequadriceps)couldbeoneofthemost important determinant of exercise intolerance in patients withAS.Also,thestudyconcludedthatmuscledeconditioning isoneofthemostimportantfactorforthereductioninaerobic capacity, suggesting the importance of muscle strength-ening exercises in these patients, in addition to aerobic training.3
Resistanceexercisesarecurrentlyusedinseveralstudies.4
Theycanbeperformedusingfreeweights,resistancebands orweightmachines.5ExercisethatusetheSwissballdiffered
fromother resistanceexercisebecauseitrecruits the mus-cles responsible for spine stabilization during movement.6
Musculoskeletalandcardiovascularsafetyofresistance train-ing have also been demonstrated, even in the face of co-morbidities.Currently,thereisevidencetojustifytheuse ofthese exercisesforhealth promotion, rehabilitationand therapeuticpurposes.4,7,8
Despitetherecognizedimportanceofexerciseaspartof atreatmentplanforpatientswithAS,thebenefitofspecific exerciseprogramshavenotbeenestablishedintheliterature.9
In a systematic review of the literature, the authors reported difficulty in performing a meta-analysis due to heterogeneity ofthe studies. In this review, it was shown that there is moderate evidence on the effects of exer-cise in improving functional capacity, disease activity and chest expansion when compared toa control group with-out exercise. The authors conclude that literature has not established which exercise protocol is more effective inAS.10
Musclestrengtheningexerciseshavebeenstudiedinfive othertrialsinASpatients.Inthesestudies,thestrengthened muscleswerethelegs,trunk,arms,backandabdominal exer-cises.Mostofthesetrialsfailtonotdescribethemethodology usedtoperformthestrengthening exercisesas:sets, num-berofrepetitions,loadmaximumcalculation,frequencyper week,progressionofloadsanddurationofmuscle strength-eningprogram.11–15
Resistanceexerciseswiththeaidofunstablesurfacessuch asa Swissball arehypothesizedtoimprove the functional capacityofpatientsbecausethisworkoutaffectsotheraspects ofphysicalfitnesssuchasbalanceandproprioception.
Material
and
methods
Population
Thisstudyisarandomizedcontrolledtrialwithablind evalua-torand16weeksoffollow-up.Sixtypatientsofbothgenders, between18and60yearsold,whohadbeendiagnosedwith ASbyarheumatologistaccordingtothemodifiedNewYork criteria16wereselectedbypersonalinvitationduringroutine
visitsinaoutpatientclinicofauniversityhospital (Universi-dadeFederaldeSãoPaulo).Thestudy wasapprovedbythe ethicscommitteeoftheinstitution(CEP0038/11)andwas reg-istered(Clinicaltrials.gov:NCT01351311).
Theinclusioncriteriawereasfollows:anestablished diag-nosisofAS;aSteinbrockerfunctionalclassofI-II;forpatients that were using medication the dosageshould be stable– disease-modifyinganti-rheumaticdrug(DMARD)foratleast threemonthsandNSAIDsand/orcorticosteroidsforatleast fourweeks.Thepatientswhowerenotusinganymedication forAS,shouldbeonthisconditionforatleastthreemonths.
Patientswithuncontrolledhypertension,ahistoryof coro-nary artery disease, a history of syncope or arrhythmias inducedbyexercise,decompensateddiabetesmellitus,severe psychiatricdisorders,fibromyalgia,amoredisablingmedical conditionthan AS, a history ofregular exerciseofatleast 30mintwotimesaweekinthelast3months,andany condi-tionthatcouldpreventthepatientfromperformingexercises inthelastthreemonths,wereexcluded.
Acomputer-generatedrandomizationlistwasutilizedto randomlyallocatepatientsinto intervention (IG)or control (CG)groupsandaconcealedrandomizationwithanopaque sealedenvelopewasperformed.
Intervention
Interventiongroup
TheIGperformedresistanceexercisesonaSwissballingroup ofamaximumof4patientsundersupervisionofatrained physiotherapist.TheexercisesprotocolisdescribedinFig.1. Theballsizewaschosenaccordingtopatientheight.For16 weeks,thesepatientsperformedeightexercisestwiceaweek in50-minutesessions.Theloadswere assessedatbaseline andre-assessedafter4,8,12and16weekstoevaluatethe progressionoftheloads.Theloadswereevaluatedbythe one-repetitionmaximum(1RM)test,where1RMisthemaximum loadsupportableintheexecutionofasinglemovement.
Alltheexerciseswereperformedinthreesetsof10 rep-etitions.Theweightprogressionwasasfollows:inweeks0 through4,theexerciseswereperformedwith50%ofthe1RM; inweeks4through12,theexerciseswereperformedwith60% ofthe1RM;andinweeks12through16,theexerciseswere per-formedwith70%ofthe1RM.Weadopteda2-minuterecovery periodbetweenthesets.4
The IG patients underwent muscle-strengthening exer-cises with the aid of a ball and dumbbells, as described inTable 1. All the exercisesrequired simultaneousmuscle contraction of the latissimus dorsi, abdominal, paraspinal, gluteus,quadricepsandhamstringmusclestomaintain sta-bilityontheball.6
Controlgroup
TheCGremainedwithmedicaltreatmentonly,andthe iden-ticaltreatmentwasofferedtothemaftertheendofthestudy.
Outcomes
The primary outcome is the BASFI (Bath Ankylosing SpondylitisFunctionalIndex).Patientswereevaluatedbefore randomizationatbaseline(T0)after4(T4),8(T8),12(T12)and 16(T16)weeks.Thefollowingoutcomeswereevaluatedbya blindedevaluator:
• BASFI(BathAnkylosingSpondylitisFunctionalIndex);is10 item index that evaluatethe functional capacity in per-formingdailyactivitiesofpatientswithAS.Theaverageof theresultsofthetenscalesistheBASFIscore(0–10),with highervaluesindicatinggreaterimpairmentinfunctional capacity.17
• HAQ-S (Health Assessment Questionnaire for Spondy-loarthritis);toassessthephysicalfunctioning.Themeasure includesitemsconcerningdressing,arising,eating, walk-ing,hygiene, reaching, gripping, and errandsand chores takenfromthe disabilityindexoftheHAQ,and an addi-tional5specificitemsconcerningneckfunctionandstatic posture(drivingacar,usingarear-visionmirror,carrying heavygroceries,sittingforlongperiods,andworkingata desk).Thereare25itemsdividedin10domains.Thefinal scoreistheresultofthesumoftheaveragescoresofthe tendomains,rangingfrom0to3.18
• 6-minutewalkingtest(6MWT)thatisafunctionaltestthat assess distance walked over 6min ina 22-meter indoor track.19
• Timedupand gotest(TUG)thatisafunctionaltestthat aimstoassessmobilityandbalance.Measurethetimein secondsforapersontorisefromsittingfromastandard armchair,walk3m,turn,walkbacktothechair,and sit down.Thepersonwearsregularfootwearandcustomary walkingaid.20
• Onerepetitionmaximumtest(1RM)wasusedforto eval-uatethemusclestrength,1-RMrepresentedthemaximum weightthatthepatientcanliftinonerepetition.8
• BASDAI (Bath Ankylosing Spondylitis Disease Activity Index)isthe goldstandardformeasuringand evaluating diseaseactivityinAS.Patientsanswered6questions per-taining to the 5 major symptoms of AS: fatigue, spinal painandjointpain/swelling,areasoflocalizedtenderness, morning stiffnessduration, and morning stiffness sever-ity.Thefinalscorerangesfrom0to10 withhigherscore suggestingsuboptimalcontrolofdisease.
• BASMI(BathAnkylosingSpondylitisMetrologyIndex)which consists of five steps: cervical rotation, tragus to wall distance,lumbarsideflexion,modifiedSchober’sand inter-malleolar distance.Patients repeated each measurement threetimesandthebest ofthemwasused.Eachis allo-catedonanumericalscalefromzerototenandthefinal scoreofBASMIisthearithmeticmeanofthefivevalues, theendresultmayvaryfrom0to10.21
Fig.1–(A)Biceps–sittingontheball,flexesandextendstheforearmagainstresistanceoffreeweight.Majormuscles acting:biceps,radialbrachiobasilic;(B)triceps–sittingontheball,holdthedumbbellwithbothhands,raiseyourarmsso theyareperpendiculartothegroundandperformsflexionandextensionoftheforearm.Majormusclesacting:triceps, deltoid;(C)rowing–standingposition,withonelegupandovertheballandthecontralaterallimbinextensionandthe upperperformsmotionsimilartorowing.Majormusclesacting:teresmajor,teresminor,rhomboidsandserratusanterior; (D)squat–standingposition,withthesupportoftheballinthelumbar,performssquatmovementwithweightsinhands. Majormusclesacting:quadriceps,hamstrings,gluteusmaximusandmiddle,rectusabdominisandlatissimusdorsi;(E) lateralrise–sittingontheball,makesabductionoftheupperlimbagainstresistance.Majormusclesacting:claviculare acromialdeltoid;(F)crucifix–supineontheball,withthoracicandlumbarspinesontheball,performstheabduction movementoftheupperlimbs.Majormusclesacting:pectoralismajor,longheadofthebiceps;(G)abdominal–supineon theball,withaloadonthepectoralregionandlumbarspineontheball,performsflexionofthetrunk.Majormuscles acting:rectusabdominis,externalandinternaloblique,gluteus;(H)reversecrucifix–proneontheball,kneelingona pillow,performsfullextensionofthearms.Majormusclesacting:posteriordeltoid,teresmajor,teresminor,trapezius.
toinspireandexhalemaximallyusingstandardbreathing instructionsandthegreaterexcursionincmrecorded.22
• TheSF-36HealthSurveywasusedtoevaluatethequalityof life.Withoverallscoresrangingfrom0to100(higherscores denotebettergeneralhealth).23
• TheASDAS-CRP/ESR(AnkylosingSpondylitisDisease Activ-ityScore)theC-ReactiveProtein(CRP)andtheerythrocyte sedimentationrate(ESR)wereusedtoassessthedisease
activity;theASDASdeterminesdiseaseactivity,usingthe scores(onascale ofnumericalmeasureof0–10)ofback pain,durationofmorning stiffness,globalassessmentby thepatient,pain/swellinginperipheraljointsandalsothe PCRdoses(mg/L)orESR(mm/h).Thevaluesareputintoan equationtoobtainthefinalscore.24
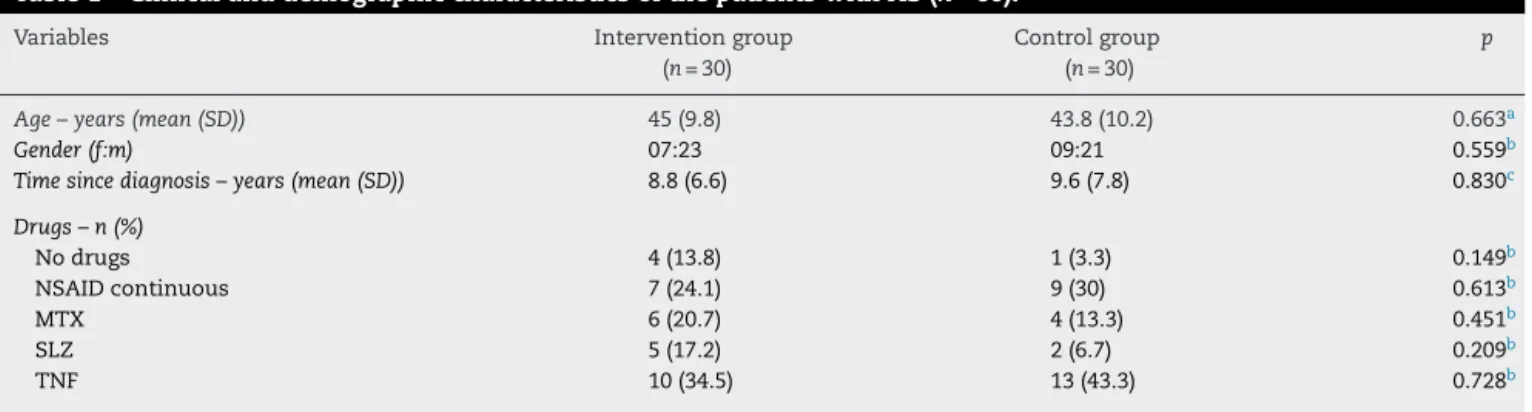
Table1–ClinicalanddemographiccharacteristicsofthepatientswithAS(n=60).
Variables Interventiongroup
(n=30)
Controlgroup (n=30)
p
Age–years(mean(SD)) 45(9.8) 43.8(10.2) 0.663a
Gender(f:m) 07:23 09:21 0.559b
Timesincediagnosis–years(mean(SD)) 8.8(6.6) 9.6(7.8) 0.830c
Drugs–n(%)
Nodrugs 4(13.8) 1(3.3) 0.149b
NSAIDcontinuous 7(24.1) 9(30) 0.613b
MTX 6(20.7) 4(13.3) 0.451b
SLZ 5(17.2) 2(6.7) 0.209b
TNF 10(34.5) 13(43.3) 0.728b
SD,standarddeviation;MTX,methotrexate;SLZ,sulfasalazine;TNF,tumornecrosisfactor. a Student’st-test.
b Chisquaretest.
c Mann–Whitneytest.
andcanchoosebetweenfivesentencesasfollows:1–much worse;2–alittleworse,3–nochange,and4–alittlebetter; 5–muchbetter.25
• Anti-inflammatory andanalgesicintake– theamount of medicationusedduringthestudywasnotedona spread-sheetgiventothepatients.
All instruments ofassessment used in this study were translatedandvalidatedfortheBrazilianversionand follow-ingweexplainedwhentheoutcomeswereevaluatedduring thestudy:1RMwasevaluatedinallevaluationtimes;patient satisfactionwasevaluatedatT4,T8,T12,andT16;BASFI, HAQ-S,6MWT,TUG,BASMI,thoracicexpansion,BASDAIandSF-36 wereevaluatedatT0,T8andT16;ESR,CPRandASDASwere evaluatedatT0andT16andtheanti-inflammatoryand anal-gesicintakewasevaluatedatT16.
Statisticalanalysis
ThesamplesizewascalculatedusingthevariableBASFIas themainvariable ofthe study,andthe standard deviation was2.0points.26Weusedarepeated-measureANOVAasthe
statisticalmethodforthisanalysis.Forthedeterminationof aminimaleffectof2.0points,a5%˛error,20%ˇerrorand SD()of2.0pointswereestablished.Givenapowerof80% anda5%detectablesignificancedifferenceequalto2.0inthe rangethatBASFImeasuredthreetimesovertimeintwo inde-pendentgroups, wefoundasampleof27patients ineach group.Consideringthepossibledropouts,werandomized60 patients.
The data were analyzed by SPSS software version 17.0 (Chicago, IL). The continuous variables between the two groupsatbaselinewerecomparedusingStudent’st-test(for variables withnormaldistribution)and theMann–Whitney test (for the variables with non-normal distribution). The categorical variables were compared using the chi-square test.Toassesstheresponsetointervention,theintentionto treatanalysiswasused,withthelastevaluationcarried for-wardwhennecessary.Theanalysisofvariance(ANOVA)with repeatedmeasureswasusedtoassesstheresponsetotherapy overtime.Theeffectsizewascalculatedbetweengroupsfor variablesthatshoweddifferencesbetweengroupsatanytime,
withthe confidenceintervalof95%.Thelevelofstatistical significancewas5%.
Results
Fig. 2 shows the flowchartof the study. Three patients in the IGand 2patientsin theCG abandonedthe study.The reasons were: loss of contact, pain exacerbation and rup-tureofcalcaneustendonintheIGandlossofcontactinthe CG.
Thepatientswerehomogeneouswithrespecttothe demo-graphicandclinicalcharacteristicsatbaseline(Table1).
Wedidnotfindstatisticaldifferencesbetweenthegroups with respectto the functional capacity assessedby BASFI, HAQSandTUG.Wefoundnodifferencesintheassessmentof
Individuals contacted (n=80)
Individuals excluded (n=3) Did not match criteria (n=5) Refused to participate (n=10)
Not found (n=2)
Randomly selected (n=60)
Interventional group (n=30)
3 abandoned experiment
2 abandoned experiment Control group
(n=30)
n=27 n=28
Intent to treat=60 patients
Table2–Evaluationoffunctionalcapacity,mobility,diseaseactivityandanalgesic/AINEsintakeinbothgroupsof patientswithAS(n=60)atdifferentweeks.
Variables Interventiongroup Controlgroup pinteractiona pintergroupsa CV
Time Mean (SD) Mean (SD)
BASFI 0.023
T0 4.62 (2.49) 4.09 (2.40) 0.410 0.53
T8 3.88 (2.36) 3.99 (2.56) 0.872 0.60
T16 3.36 (2.16) 3.90 (2.6) 0.386 0.64
HAQ-S 0.131
T0 0.79 (0.51) 0.75 (0.53) 0.637 0.64
T8 0.69 (0.46) 0.74 (0.51) 0.637 0.66
T16 0.58 (0.44) 0.70 (0.5) 0.637 0.75
BASMI 0.170
T0 4.94 (2.09) 5.19 (2.04) 0.344 0.42
T8 4.90 (1.86) 5.44 (2.14) 0.344 0.37
T16 4.69 (1.94) 5.37 (2.2) 0.344 0.41
Thoracicexpansion(cm) 0.768
T0 3.33 (1.57) 3.50 (1.90) 0.939 0.47
T8 3.48 (1.83) 3.45 (2.02) 0.939 0.52
T16 3.45 (1.61) 3.41 (1.89) 0.939 0.46
6-minutewalkingtest(m) <0.001
T0 447.43 (54.99) 435.43 (59.44) 0.424 0.12
T8 451.40 (51.52) 440.80 (51.96) 0.435 0.11
T16 464.43 (48.03) 427.20 (49.6) 0.005 0.10
Timeupandgo(s) 0.025
T0 7.36 (1.68) 7.20 (1.60) 0.705 0.22
T8 6.48 (1.13) 6.62 (1.06) 0.621 0.17
T16 6.19 (1.16) 6.76 (1.31) 0.077 0.18
BASDAI 0.828
T0 2.52 (1.65) 2.34 (2.26) 0.885 0.65
T8 2.09 (1.61) 2.01 (2.39) 0.885 0.77
T16 2.08 (1.84) 2.12 (2.4) 0.885 0.88
ASDAS-CRP 0.425
T0 2.20 (0.91) 1.89 (1.00) 0.370 0.41
T16 1.93 (0.84) 1.86 (1.10) 0.43
ASDAS-ESR 0.075
T0 2.23 (0.87) 2.11 (0.97) 0.474 0.39
T16 1.73 (0.70) 2.15 (1.25) 0.40
C-reactiveprotein(mg/dL) 0.351
T0 6.53 (6.00) 4.70 (5.96) 0.063 0.91
T16 9.27 (13.50) 4.51 (6.75) 1.45
ESR(mm/h) 0.104
T0 18.10 (13.23) 18.00 (12.27) 0.356 0.73
T16 13.31 (9.01) 18.71 (14.33) 0.67
NSAIDs
T16 3.17 (5.86) 1.56 (4.88) 0.133b 1.84
Analgesic
T16 1.97 (4.94) 2.19 (5.41) 0.749b 2.50
CV,coefficientofvariationforinterventiongroup;HAQ-S,HealthAssessmentQuestionnaireforSpondyloarthritis;BASFI,BathAnkylosing SpondylitisFunctionalIndex;Basmi,bathankylosingspondylitismetrologyindex;Basdai,BathAnkylosingSpondylitisDiseaseActivityIndex; ASDAS,AnkylosingSpondylitisDiseaseActivityScore;ASDASPCR,ASDASC-ReactiveProtein;ASDASVHS,ASDASerythrocytesedimentation rate.
a ANOVAtest.
b Mann–Whitneytest.
spinalmobilityevaluatedbyBASMIandthoracicexpansion. Statistical differences were found between the groups in the 6-minute walk testat week16 (p=0.005, coefficient of variation=0.10).Regardingthediseaseactivity,wefoundno
Table3–Evaluationofmusclestrengthaccordingtotheexercisesinbothgroups.
Exercise Interventiongroup Controlgroup pinteractiona pintergroups CV
Time Mean (SD) Mean (SD)
Biceps(kg) 0.041
T0 6.47 (2.32) 6.57 (2.66) 0.878 0.35
T4 7.37 (2.60) 7.00 (2.53) 0.586 0.35
T8 7.63 (2.79) 7.20 (2.75) 0.550 0.36
T12 7.97 (2.64) 7.30 (2.56) 0.329 0.33
T16 8.43 (2.78) 7.43 (2.70) 0.166 0.32
Triceps(kg) <0.001
T0 6.90 (2.64) 7.23 (3.20) 0.664 0.38
T4 8.70 (3.28) 7.63 (3.62) 0.240 0.37
T8 9.27 (3.86) 7.93 (3.30) 0.160 0.41
T12 10.17 (4.16) 8.20 (3.39) 0.052 0.40
T16 11.07 (4.46) 8.57 (3.55) 0.021 0.40
Rowing(kg) 0.001
T0 9.63 (3.18) 9.73 (3.04) 0.902 0.33
T4 11.10 (3.76) 10.70 (3.41) 0.670 0.33
T8 12.40 (4.25) 11.17 (3.92) 0.252 0.34
T12 19.47 (31.95) 11.27 (3.89) 0.024 1.64
T16 13.90 (4.03) 11.63 (3.58) 0.026 0.28
Squat(kg) 0.007
T0 13.67 (5.90) 13.67 (6.06) 1.000 0.43
T4 16.53 (6.56) 14.97 (6.12) 0.347 0.39
T8 19.40 (6.78) 16.57 (6.57) 0.109 0.34
T12 20.50 (6.24) 16.97 (6.79) 0.042 0.30
T16 21.27 (7.47) 16.50 (6.89) 0.014 0.35
Lateralrise(kg) <0.001
T0 4.53 (1.84) 4.67 (2.14) 0.798 0.40
T4 4.97 (1.97) 5.00 (2.07) 0.950 0.39
T8 5.37 (1.91) 5.07 (2.20) 0.577 0.35
T12 5.73 (2.06) 5.20 (2.12) 0.332 0.35
T16 6.20 (2.21) 5.23 (2.28) 0.104 0.35
Crucifix(kg) 0.002
T0 4.10 (1.92) 4.33 (2.01) 0.650 0.46
T4 4.73 (1.61) 4.60 (2.14) 0.788 0.34
T8 5.17 (1.88) 4.67 (1.92) 0.316 0.36
T12 5.70 (1.93) 4.70 (2.07) 0.060 0.33
T16 5.90 (2.04) 5.00 (2.38) 0.124 0.34
Abdominal(kg) <0.001
T0 16.63 (8.75) 17.63 (13.15) 0.731 0.52
T4 23.60 (12.10) 20.83 (12.53) 0.392 0.51
T8 28.33 (13.12) 21.67 (13.14) 0.056 0.46
T12 32.33 (15.26) 24.10 (13.08) 0.030 0.47
T16 39.33 (17.21) 26.33 (14.68) 0.003 0.43
Reversecrucifix(kg) 0.002
T0 3.93 (1.44) 4.03 (1.45) 0.791 0.36
T4 4.75 (1.57) 4.27 (1.36) 0.213 0.33
T8 5.12 (1.67) 4.53 (1.59) 0.175 0.32
T12 5.33 (1.72) 4.67 (1.52) 0.120 0.32
T16 5.93 (1.88) 4.87 (1.61) 0.023 0.31
CV,coefficientofvariationforinterventiongroup. a ANOVAtest.
Withregardtomusclestrength,differencesbetweenthe groups were observed, with improvementin the IGin the followingexercises:triceps, rowing,squats, abdominaland reversecrucifix,asshowninTable3.
Table4shows the domains ofthe SF-36, and no differ-encesbetweenthegroupswereobservedinanydomainsof thequestionnaire.
Statisticaldifferencewasobservedbetweenthegroupson theLikertscale(p<0.001).Theinterventiongroupshoweda higherfrequencyofanswers4(alittlebetter)and5(much bet-ter),whereasthecontrolgroupshowedahigherfrequencyof answer3(nochange).
Table4–EvaluationofthegeneralqualityoflifeusingtheSF-36questionnaireinbothgroupsofpatientswithAS.
Domains Interventiongroup Controlgroup pinteractiona pintergroupsa CV
Time Mean (SD) Mean (SD)
Physicalfunctioning 0.189
T0 65.7 (23.2) 67.2 (23.2) 0.926 0.35
T8 69.2 (23.6) 71 (21.9) 0.926 0.34
T16 73 (18.3) 68.2 (26) 0.926 0.25
Role-physical 0.802
T0 54.2 (47.4) 58.3 (47.5) 0.856 0.87
T8 63.3 (47.2) 60 (48.1) 0.856 0.69
T16 67.5 (42.1) 71.7 (42.9) 0.856 0.62
Pain 0.598
T0 61.1 (19.8) 62.4 (25.4) 0.841 0.32
T8 66 (21.7) 61.7 (25.8) 0.841 0.32
T16 65.6 (19.4) 65.6 (27.5) 0.841 0.29
Generalhealth 0.365
T0 44.7 (20.5) 46.2 (23.8) 0.718 0.45
T8 52.3 (21.3) 49.5 (23.5) 0.718 0.40
T16 51.8 (21.5) 47.3 (26.4) 0.718 0.41
Vitality 0.295
T0 62.5 (25.2) 61.3 (33.6) 0.460 0.40
T8 69.5 (18.3) 64.8 (31.6) 0.460 0.26
T16 72.2 (17.8) 3.7 (30.9) 0.460 0.24
Socialfunctioning 0.469
T0 75.3 (24.9) 78.3 (24.2) 0.820 0.33
T8 81.6 (21.9) 78.3 (24.3) 0.820 0.26
T16 81.9 (21.7) 78.7 (26.5) 0.820 0.26
Role-emotional 0.866
T0 60 (49.8) 75.5 (41) 0.161 0.83
T8 68.6 (44.6) 77.7 (40.4) 0.161 0.65
T16 72.2 (43.9) 84.4 (35.8) 0.161 0.60
Mentalhealth 0.236
T0 71.1 (25.9) 73.3 (21.8) 0.807 0.36
T8 73.3 (21.8) 78.4 (25.1) 0.807 0.29
T16 78.4 (18.4) 76.7 (26.6) 0.807 0.23
CV,coefficientofvariationforinterventiongroup. a ANOVAtest.
foundanESof37.2inthe6minwalktest(95%CI11.8to62.7); andinmeasuringthestrengthoftricepsandreversecrucifix exercisestheESwere2.5(95%CI0.39to4.61)and1.07(95% CI0.15to1.98)respectively.InT12andT16,thestrength mea-surementsofrowingexerciseshowedanESof2.5(95%CI0.34 to4.66)and2.27(95%CI0.28to4.25)respectively;thestrength measuredinsquatexerciseshowedanESof3.53(95%CIof 6.93to0.4)inT12and4.77(95%1.02to8.52)inT16.Regarding thestrengthmeasurementofabdominalexercisewefoundan ESof8.23(95%CI0.81to15.65)inT12and13(95%CI4.65to 21.35)inT16.
Discussion
Exercises are widely recommended for the treatment of patientswithAS;however,thereisnoconsensusinthe lit-erature regarding the most efficient type of exercises.27,28
Studiesusingexercisesasatreatmentformanydiseasesfail todescribethenumberofsetsandrepetitions,thetraining
progressionandademonstrationoftheexercisesforthestudy exerciseprotocoltobereproducible.Areviewofexercise pro-grams forASfoundfivestudies withmuscle strengthening exercises,and noneofthesestudiesdescribed theexercise programadequately,thereforeitisdifficulttodefinethe opti-maldose and progressionofexercises.9 Thepresent study
shows an exercise protocol that can be easily reproduced becauseitdescribestheexercises,thenumberofsetsand rep-etitionsandtheprogressionoftrainingloads.Thisprotocol wasshowntobeeffectiveandsafe.
Theexerciseprotocolpresentedinthisstudyisin accor-dancewiththerecommendationsoftheAmericanCollegeof SportsMedicineregardingthemusclestrengthtraining pro-gression, the number ofsets and repetitions,and the rest intervalsbetweensets.8Becausetheserecommendationsare
betweenthegroupsintermsofstrengthimprovementafter 12 weeks.Thestudy ofFernandez de Las Penas et al.was conductedfor16weeks,anditcomparedconventional phys-iotherapywithglobalposturalreeducationanddemonstrated improvement in mobility and functional capacity in both groups.11Otherstudiesusingmuscle-strengtheningexercises
asaninterventionwithshorterdurations,suchas6,8and12 weeks,showedconflictingresults,althoughtheyhadin com-monthelackofadetaileddescriptionoftheload,thenumber ofsetsandthenumberofrepetitionsoftheexercises,ensuring thatitwasdifficulttocomparetheresults.12–14
ThedecisiontoperformtheexercisesonaSwissballwas madebecauseofthebenefitsthistypeofexercisecouldoffer tothe patientduringtheexecutionofmovements,suchas therecruitmentofthestabilizermusclesknownasthe“core”. Exercisesthatactivatethecoremuscleshavebeenthe sub-jectofrecentstudies,andthereisgreateractivationofthese musclesintheexercisesperformedwiththeSwissball.5,6One
studyshowedthatstrengthandcorestabilitywereimportant inimprovingtheperformanceactivitiesofdailylivinginthe elderly.29 Pilatesexercisesthatactivate the corehavebeen
prescribedand areeffectiveinthefunctional improvement ofASpatients.30Thesefindingsjustifyourselectionof
exer-cisesperformedontheSwissball,althoughourgoalwasnot toevaluatetheeffectsofspecificcoreexercises.
Webelievethatthe improvementinperformanceofthe 6-minutewalktesthasadirectrelationshipwithimproved musclestrength,particularlyinthesquatexerciseduringthe last weekof evaluation, which shows that the increase in strengthinthelower limbscoulddeterminetheamountof improvementinthe walking performancein patients with AS.Theseresultscorroboratethefindingsofprevious stud-iesregardingthecorrelationofmusclestrengthwithaerobic capacity.Inthe study byCarteret al.,which evaluatedthe physicalabilities of patients with AS, the authors demon-stratedthat the reductioninaerobiccapacity and exercise intolerance were largely explainedby the weakness ofthe peripheralmuscles,suchasthequadriceps,observedinthese patients.3 Theweakness ofthe lowerlimbsinpatients has
beendocumentedintwostudiesbySahinetal.thatcompared thestrengthandfatigueofthemusclesoftheankleandknee ofASpatientswithhealthycontrols.Theamountoffatigue washigher,andthemusclestrength ofthe plantarflexors, ankleflexorsandkneeextensorswassignificantlylower in patientswithAS.26,31
Inthisstudy,nodifferences wereobservedbetweenthe groups with respect to the functional capacity evaluation usingtheBASFIand HAQ-S.TheBASFIand HAQ-Sare val-idatedinstrumentstomeasurefunctional capacityanduse questionsaboutdailylivingactivitiesinpatientswithAS.Most questionsareaboutsimpleactivitiessuchasdressing,getting upfromachair,andclimbingsteps.Thus,theinstruments donotassessmoreintensephysicalactivitiesandonlydetect changesinlighterphysicaltasks.32Inourstudy,althoughthe
patientsshowedimprovementsofmuscularstrengththeydid notimprovefunctionalcapacity.Itispossiblethattheexercise programwasmoredirectedtoincreasephysicalfitnessand didnotachievetheobjectiveofimprovingfunctionalcapacity. Incontrast,inthestudy byLimetal.,theexercises per-formedonceadayforeightweeksimprovedthefunctional
capacityoftheinterventiongroupcomparedtothecontrol group.26 Arecent study byGunayet al.that evaluated the
effectivenessofbreathingexercisesandposturesinagroup ofpatientswithASdemonstratedimprovementinfunctional capacity,mobility,diseaseactivityandqualityoflifein rela-tiontotheisolatedgroupthatperformedposturalexercises andthecontrolgroup.AstudybyGunayetal.usedasmall sample,andonlyintra-groupcomparisonswereperformed.33
FewstudiesusedtheHAQ-Stoassessthefunctional capac-ityofpatientswithASwhounderwentanexerciseprogram. AstudybySweeneyatalfoundnodifferencesintheHAQ-S betweenthepatientswhodidhomeexercisesversusgroup exercisesfor9months.34
The difference in functional capacity between groups might not havebeen impressivein our study because our patientswerestablewithdrugtreatment,andalmost40%of ourpatientswerestablewiththeuseofanti-TNFtherapy.This mightexplainthelackofdifferencesbetweenthegroupswith respecttodiseaseactivity assessedbyBASDAIand ASDAS-CRP/ESR and the use of analgesics and anti-inflammatory medicationsduringthestudyperiod.
Thisstudy wasthefirsttousetheTimedupandgotest timedupasameasuringtooltoevaluateotherparametersof functionalcapacitysuchasstanding,walkingandsittingin patientswithAS.Thistestiswidelyusedfortheassessment ofbalanceandmobilityintheelderly.35Becausebothgroups
averagedlessthan10sfromtheinitialassessment,bothwere consideredfreelymobile.Itispossiblethatimprovementin thistestwasnotdetectedattheendof16weeksbecausethe patientshad showngoodfunctionalindependenceat base-line.
Nodifferenceswereobservedbetweenthegroupsinterms ofthequality oflifeassessedbythe SF-36,althoughmany studies show improvement inquality oflife asa resultof therapeuticexercises.Itispossiblethattheinstrumentdid nothavesufficientsensitivitytochangestodemonstratethe effectsoftheinterventioninthispopulation.
Althoughtheeffectsonfunctionalcapacity,mobilityand qualityoflifeweremodest,webelievethatourexercise pro-tocol has madea positive impact on patients because the patients’satisfactionregardingthetreatmentwashighforthe interventiongroup,withastatisticaldifferencebetweenthe groups,showingthatpatientsfelt“better”or“muchbetter” withtreatment,asassessedbyaLikertscale.
Adherencetotheexercisetherapyisoneaspectthatshould beobservedinstudieswithexerciseprogramsbecauseitis animportantdeterminantofthebeneficialresponseto inter-vention. In this study, adherence was high,with over 80% attendanceatthetrainingsessions.Moststudieswith physi-calexerciseinASdonotdescribepatientcompliance.Astudy comparingaphysicaltherapygroupwithindividualizedhome exercises reportedadherence of73.5% ofthe patientswho participatedinthesupervisedgroups.15Inthispresentstudy,
theeffectofgrouptherapy,thecontinuoussupervisionbya physiotherapistand no worsening ofinflammatory disease activitywereidentifiedasfactorsthatledtothehigh adher-enceandpatientsatisfaction.
betweenthepatient andthe therapist.Webelievethatthe treatment periodcould have been longer because changes inmusclestrengthwereevidentonlyafter12weeks.Future studiesoflongerdurationthatcomparedifferentexercise pro-tocolsmightshowpromisingresults.
Inconclusion,theprogressivemusclestrengtheningusing theSwissballwaseffectiveinimprovingthemusclestrength, walkingperformanceandpatientsatisfactioninpatientswith AS.Theexerciseprogramhasshowngoodtolerancewithout deleteriouseffectsonthediseaseactivity.
Funding
Clinicaltrials.gov:NCT01351311.
Grant # 2011/03459-9, São Paulo Research Foundation (FAPESP).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. KarapolatH,AkkocY,SariI,EyigorS,AkarS,KirazliY,etal. Comparisonofgroup-basedexerciseversushome-based exerciseinpatientswithankylosingspondylitis:effectson BathAnkylosingSpondylitisIndices,qualityoflifeand depression.ClinRheumatol.2008;27:695–700.
2. ZochlingJ,VanDerHeijdeD,DougadosM,BraunJ.Current evidenceforthemanagementofankylosingspondylitis:a systematicliteraturereviewfortheASAS/EULAR
managementrecommendationsinankylosingspondylitis. AnnRheumDis.2006;65:423–32.
3. CarterR,RiantawanP,BanhamSW,SturrockRD.An investigationoffactorslimitingaerobiccapacityinpatients withankylosingspondylitis.RespirMed.1999;93:700–8.
4. AmericanCollegeofSportsMedicine.AmericanCollegeof SportsMedicinepositionstand.Progressionmodelsin resistancetrainingforhealthyadults.MedSciSportsExerc. 2009;41:687–8.
5. SundstrupE,JakobsenMD,AndersenCH,JayK,AndersenLL. Swissballabdominalcrunchwithaddedelasticresistanceis aneffectivealternativetotrainingmachines.IntJSportsPhys Ther.2012;7:372–80.
6. EscamillaRF,LewisC,BellD,BrambletG,DaffronJ,LambertS, etal.CoremuscleactivationduringSwissballandtraditional abdominalexercises.JOrthopSportsPhysTher.
2010;40:265–76.
7. AmericanCollegeofSportsMedicineChodzko-ZajkoWJ, ProctorDN,FiataroneSinghMA,MinsonCT,NiggCR,etal. AmericanCollegeofSportsMedicinepositionstand.Exercise andphysicalactivityforolderadults.MedSciSportsExerc. 2009;41:1510–30.
8. GarberCE,BlissmerB,DeschenesMR,FranklinBA,Lamonte MJ,LeeIM,etal.,AmericanCollegeofSportsMedicine. Quantityandqualityofexercisefordevelopingand maintainingcardiorespiratory,musculoskeletal,and
neuromotorfitnessinapparentlyhealthyadults:guidancefor prescribingexercise.MedSciSportsExerc.2011;43:1334–59.
9. DagfinrudH,HalvorsenS,VøllestadNK,NiedermannK,Kvien TK,HagenKB.Exerciseprogramsintrialsforpatientswith
ankylosingspondylitis:dotheyreallyhavethepotentialfor effectiveness?ArthritisCareRes(Hoboken).2011;63:597–603.
10.O’DwyerT,O’SheaF,WilsonF.Exercisetherapyfor spondyloarthritis:asystematicreview.RheumatolInt. 2014;34:887–902.
11.Fernandez-de-Las-PenasC,Alonso-BlancoC,
Morales-CabezasM,Miangolarra-PageJC.Twoexercise interventionsforthemanagementofpatientswith ankylosingspondylitis:arandomizedcontrolledtrial.AmJ PhysMedRehabil.2005;84:407–19.
12.AnalayY,OzcanE,KaranA,DiracogluD,AydinR.The effectivenessofintensivegroupexerciseonpatientswith ankylosingspondylitis.ClinRehabil.2003;17:631–6.
13.LimHJ,MoonYI,LeeMS.Effectsofhome-baseddailyexercise therapyonjointmobility,dailyactivity,pain,anddepression inpatientswithankylosingspondylitis.RheumatolInt. 2005;25:225–9.
14.CagliyanA,KotevogluN,OnalT,TekkusB,KuranB.Does groupexerciseprogramaddanythingmoretopatientswith ankylosingspondylitis.JBackMusculoskeletRehabil. 2007;20:79–85.
15.HiddingA,vanderLindenS,BoersM,GielenX,deWitteL, KesterA,etal.Isgroupphysicaltherapysuperiorto individualizedtherapyinankylosingspondylitis.A
randomizedcontrolledtrial.ArthritisCareRes.1993;6:117–25.
16.VanDerLindenS,ValkenburgHA,CatsA.Evaluationof diagnosticcriteriaforankylosingspondylitis.Aproposalfor modificationoftheNewYorkcriteria.ArthritisRheum. 1984;27:361–8.
17.CusmanichKG,KowalskiSC,GallinaroAL,
Goldenstein-SchainbergC,SouzaLA,Gonc¸alvesCR. Cross-culturaladaptationandvalidationofthe Brazilian–PortugueseversionoftheBathAnkylosing SpondylitisFunctionalIndex(BASFI).RevBrasReumatol. 2012;52:733–41.
18.ShinjoSK,GoncalvesR,KowalskiS,Gonc¸alvesCR. Brazilian–PortugueseversionoftheHealthAssessment QuestionnaireforSpondyloarthropathies(HAQ-S)inpatients withankylosingspondylitis:atranslation,cross-cultural adaptation,andvalidation.ClinRheumatol.2007;26:1254–8.
19.ATSCommitteeonProficiencyStandardsforClinical PulmonaryFunctionLaboratories.ATSstatement:guidelines forthesix-minutewalktest.AmJRespirCritCareMed. 2002;166:111–7.
20.PodsiadloD,RichardsonS.Thetimedup&go:atestofbasic functionalmobilityforfrailelderlypersons.JAmGeriatrSoc. 1991;39:142–8.
21.ShinjoSK,GoncalvesR,KowalskiS,Gonc¸alvesCR.
Brazilian–Portugueseversionandapplicabilityquestionnaire ofthemobilityindexforankylosingspondylitis.Clinics. 2007;62:139–44.
22.SieperJ,RudwaleitM,BaraliakosX,BrandtJ,BraunJ, Burgos-VargasR,etal.TheAssessmentofSpondyloArthritis internationalSociety(ASAS)handbook:aguidetoassess spondyloarthritis.AnnRheumDis.2009;68Suppl2:ii1–44.
23.CiconelliRM,FerrazMB,SantosW,MeinaoI,QuaresmaMR. Brazilian–PortugueseversionoftheSF-36.Areliableandvalid qualityoflifeoutcomemeasure.RevBrasReumatol.
1999;39:143–50.
24.MachadoP,LandewéR,LieE,KvienTK,BraunJ,BakerD,etal. AnkylosingSpondylitisDiseaseActivityScore(ASDAS): definingcut-offvaluesfordiseaseactivitystatesand improvementscores.AnnRheumDis.2011;70:47–53.
25.DrinkwaterBL.Acomparisonofthedirection-of-perception techniquewiththeLikertmethodinthemeasurementof attitudes.JSocPsychol.1965;67:189–96.
isokineticdynamometerinpatientswithankylosing spondylitis.ActaReumatolPort.2011;36:252–9.
27.HarperBE,ReveilleJD.Spondyloarthritis:clinicalsuspicion, diagnosis,andsports.CurrSportsMedRep.2009;8:29–34.
28.OzgocmenS,AkgulO,AltayZ,AltindagO,BaysalO,CalisM, etal.,AnatolianGroupfortheAssessmentinRheumatic Diseases.Expertopinionandkeyrecommendationsforthe physicaltherapyandrehabilitationofpatientswith ankylosingspondylitis.IntJRheumDis.2012;15:229–38.
29.GranacherU,GollhoferA,HortobágyiT,KressigRW, MuehlbauerT.Theimportanceoftrunkmusclestrengthfor balance,functionalperformance,andfallpreventionin seniors:asystematicreview.SportsMed.2013;43:627–41.
30.AltanL,KorkmazN,DizdarM,YurtkuranM.EffectofPilates trainingonpeoplewithankylosingspondylitis.Rheumatol Int.2012;32:2093–9.
31.SahinN,OzcanE,BaskentA,KaranA,EkmeciO,Kasikcioglu E.Isokineticevaluationofanklemusclestrengthandfatigue
inpatientswithankylosingspondylitis.EurJPhysRehabil Med.2011;47:399–405.
32.JenningsF,OliveiraHA,deSouzaMC,CruzVG,NatourJ. Effectsofaerobictraininginpatientswithankylosing spondylitis.JRheumatol.2015;42:2347–53.
33.GünayMO,BalS,BayramKB,HarmanE,Dalgıc¸EE,Koc¸yi ˘gitH, etal.Theeffectofbreathingandpostureexerciseonthe clinical,functionalstatusanddiseaserelatedqualityoflifein patientswithankylosingspondylitis.Med-Science.
2012;1:103–17.
34.SweeneyS,TaylorG,CalinA.Theeffectofahomebased exerciseinterventionpackageonoutcomeinankylosing spondylitis:arandomizedcontrolledtrial.JRheumatol. 2002;29:763–6.