Abst ract
Submitted: April 1, 2016 0RGL¿FDWLRQ-XO\ Accepted: August 14, 2016
Short- t erm t ranscut aneous elect rical
nerve st im ulat ion reduces pain and
im proves t he m ast icat ory m uscle
act ivit y in t em porom andibular
disorder pat ient s: a random ized
cont rolled t rial
St udies t o assess t he effect s of t herapies on pain and m ast icat or y m uscle funct ion are scarce. Obj ect ive: To invest igat e t he short- t erm effect of t ranscut aneous elect rical nerve st im ulat ion ( TENS) by exam ining pain int ensit y, pressure pain t hreshold ( PPT) and elect rom yography ( EMG) act ivit y in pat ient s w it h t em porom andibular disorder ( TMD) . Mat erial and Met hods: Fort y pat ient s wit h m yofascial TMD were enrolled in t his random ized placebo-cont rolled t rial and were divided int o t w o groups: act ive ( n= 20) and placebo ( n= 20) TENS. Out com e variables assessed at baseline ( T0) , im m ediat ely aft er ( T2) and 48 hour s aft er t r eat m ent ( T1) w er e: pain int ensit y w it h t he aid of a visual analogue scale ( VAS) ; PPT of m ast icat ory and cervical st r uct ur es; EMG act ivit y dur ing m andibular r est posit ion ( MR) , m axim al volunt ary cont ract ion ( MVC) and habit ual chew ing ( HC) . Two- way ANOVA IRUUHSHDWHGPHDVXUHVZDVDSSOLHGWRWKHGDWDDQGWKHVLJQL¿FDQFHOHYHO was set at 5% . Result s: There was a decrease in t he VAS values at T1 and T2 w hen com pared w it h T0 values in t he act ive TENS group ( p< 0.050) . The 337 EHWZHHQJURXS GLIIHUHQFHV ZHUH VLJQL¿FDQW DW 7 DVVHVVPHQW RI WKH ant erior t em poralis and st ernocleidom ast oid ( SCM) and T2 for t he m asset er DQGWKH6&0S$VLJQL¿FDQW(0*DFWLYLW\UHGXFWLRQRIWKHPDVVHWHU and ant erior t em poralis was present ed in t he act ive TENS during MR at T1 assessm ent when com pared wit h T0 ( p< 0.050) . The EMG act ivit y of t he DQWHULRUWHPSRUDOLVZDVVLJQL¿FDQWO\KLJKHULQWKHDFWLYH7(16GXULQJ09& at T1 and T2 when com pared w it h placebo ( p< 0.050) . The EMG act ivit y RIWKHPDVVHWHUDQGDQWHULRUWHPSRUDOLVPXVFOHZDVVLJQL¿FDQWO\KLJKHULQ t he act ive TENS during HC at T1 w hen com pared w it h placebo ( p< 0.050) . Conclusions: The short - t erm t herapeut ic effect s of TENS are superior t o t hose of t he placebo, because of report ed facial pain, deep pain sensit ivit y and m ast icat ory m uscle EMG act ivit y im provem ent .
Ke yw or ds: Tem porom andibular j oint disorders. Transcut aneous elect ric nerve st im ulat ion. Pain t hreshold. Elect rom yography.
Ana Paula de Lima FERREIRA1
Dayse Regina Alves da COSTA2
Ana Izabela Sobral de OLIVEIRA3
Elyson Adam Nunes CARVALHO4
Paulo César Rodrigues CONTI5
Yuri Martins COSTA6
Leonardo Rigoldi BONJARDIM6
1Universidade Federal de Pernambuco, Departamento de Fisioterapia, Recife, PE, Brasil. 2Universidade Federal de Sergipe, São Cristóvão, SE, Brasil.
3Universidade Federal de Pernambuco, Programa de Pós-Graduação em Neuropsiquiatria e Ciências
do Comportamento, Recife, PE, Brasil.
4Universidade Federal de Sergipe, Departamento de Engenharia Elétrica, São Cristóvão, SE, Brasil. 5Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Prótese, Bauru,
SP, Brasil.
6Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Ciências
Biológicas, Seção de Fisiologia da Cabeça e da Face, Bauru, SP, Brasil.
Corresponding address: Yuri Martins Costa Seção de Fisiologia da Cabeça e da Face
I nt roduct ion
Transcut aneous Elect rical Nerve St im ulat ion ( TENS)
has been used t o cont rol pain in pat ient s w it h chronic
t em por om andibular disor der s ( TMD) . How ever, t he
LQÀXHQFHRIWKLVWKHUDS\RQWKHWRQXVRIPDVWLFDWRU\
m uscles should be furt her invest igat ed, considering
t hat t he evidence regarding t he im provem ent of clinical
param et ers, e.g., report ed pain, j aw m ovem ent and
elect rom yography ( EMG) act ivit y, are divergent and
cont roversial4,6,18,22.
I t is w ell est ablished t hat TENS can reduce pat ient -r epo-r t ed pain in t en sit y in acu t e pain con dit ion s1 3, EXWLWVHI¿FDF\LVFRQWURYHUVLDOLQFKURQLFSDLQ2,15. On
t he ot her hand, t o t he best of our know ledge, t here is no published st udy on t he effect s of TENS on t he pressure pain t hreshold ( PPT) of m ast icat ory m uscles.
1RQHWKHOHVV ¿QGLQJV IURP WKH FHUYLFDO UHJLRQ KDYH
sh ow n t h at TENS did n ot affect t h e PPT of u pper t rapezius t rigger point s11.
One st udy show ed t hat t he m ain effect s of TENS on t he m uscular t onus of pat ient s w it h TMD w ere: 1) r educt ion in m uscle act iv it y of t he ant er ior por t ion of t h e an t er ior t em por alis m u scle, du r in g r est in g post ure of t he j aw, and 2) increased m uscle act ivit y of t he m asset er m uscles, during m axim al volunt ary cont ract ion ( clenching)222WKHUVWXG\DOVRFRQ¿UPHG
TENS as effect ive in reducing t he EMG act ivit y of t he an t er ior t em por alis an d m asset er m u scles du r in g rest ing post ure of t he j aw19.
Ma n d i b u l a r k i n e m a t i cs m a y b e su b j e ct e d t o changes t hat m ay com prom ise t he m uscle and art icular funct ions in TMD pat ient s16. Ther efor e, in addit ion
t o pain assessm ent , ident ify ing dy sfunct ional EMG behaviors w ill also be useful in providing t herapeut ic m an ag em en t an d p r ev en t i n g t h e p r og r essi on of signs and sym pt om s16. Furt herm ore, pain reduct ion
and im proved funct ion are com m only t he proposed g oals f or t r eat in g ch r on ic m u scu losk elet al p ain1 2.
Nev er t h eless, pain an d m u scle f u n ct ion ar e of t en evaluat ed separat ely, and st udies t o assess t he effect s of t herapies on pain and m ast icat ory m uscle funct ion are scant in t he lit erat ure.
Based on t he above, t he aim of t his st udy was t o invest igat e t he short- t erm effect of TENS by exam ining pain int ensit y, PPT and EMG param et ers in subj ect s wit h m yofascial TMD. Our init ial hypot hesis was t hat TENS is as effect ive in reducing facial pain as it is in im proving m ast icat ory m uscle EMG act ivit y of TMD pat ient s.
Mat erial and Met hods
Part icipant s and design
Academ ic st aff and under graduat e st udent s of bot h genders from t he Federal Universit y of Sergipe w ere eligible. They underw ent clinical evaluat ion for ex am inat ion of signs and sy m pt om s of TMD and, aft er t he inclusion and exclusion crit eria assessm ent , part icipant s w ere divided int o t w o groups: ( 1) TENS placebo ( n= 20) and ( 2) TENS act ive ( n= 20) . The st udy design w as a random ized placebo- cont r olled t r ial. One invest igat or ( R1) w ho did not part icipat e in dat a collect ion perform ed t he random izat ion w it h t he aid of com put ed- generat ed com binat orial analysis, w hich was used t o generat e t he random sequence. A second invest igat or ( R2) perform ed t he eligibilit y assessm ent and t he gr oup allocat ion was m ade by sealed and opaque envelopes ( concealed allocat ion) . Operat ional issu es pr eclu ded m ask in g of t h e r esear ch er w h o applied t he t reat m ent . Then, t he sam e invest igat or ( R2 ) w h o p e r f o r m e d t h e g r o u p a l l o ca t i o n a l so perform ed t he t reat m ent . A t hird invest igat or ( R3) , blinded for group allocat ion, conduct ed t he out com e assessm ent s. Finally, a fourt h invest igat or ( R4) carried out t he int er pr et at ion and analysis of r esult s. I t is im port ant t o not e t hat t he part icipant s of t his st udy w ere also blinded regarding t he t ype of t reat m ent .
Sam ple size of at least 20 subj ect s per group was det erm ined based on pilot evaluat ions, w hich w ould be suit able t o det ect a pressure pain t hreshold ( PPT) difference of 1.02 kgf/ cm2, st andard deviat ion ( SD)
of 1.12 kgf/ cm2FRQVLGHULQJWKHVLJQL¿FDQFHOHYHORI ĮDQGVDPSOHSRZHURIǃ
The Et hics Com m it t ee of t he Federal Univer sit y of Ser gipe appr ov ed t h e st u dy an d t h e in f or m ed consent from each part icipant was obt ained aft er full explanat ion of t he research purposes and procedures.
I nclusion and exclusion crit eria
The inclusion crit eria was t he diagnost ic of chronic painful TMD ( at least six m ont hs of pain com plaint ) accor din g t o t h e Resear ch Diagn ost ic Cr it er ia f or Tem porom andibular Disorders ( RDC/ TMD) , cat egories I a ( m yofascial pain w it hout lim it ed m out h opening) or I b ( m yofascial pain w it h lim it ed m out h opening)10.
The exclusion crit eria w ere: a) a hist ory of facial or head t raum a, rheum at ic and ort hopedic pat hologies, surgical procedures perform ed in t he craniocervical region and neurological diseases; b) diagnost ic of ot her
chronic pain disorders, such as prim ary headaches,
FHUYLFDO SDLQ GLVRUGHUV RU ¿EURP\DOJLD XVH RI RUDO
cont racpt ive; c) regular int ake of m edicat ions, such as m uscle relaxant s, ant iconvulsant s, ant idepressant s and anxiolyt ics; d) any TMD t reat m ent perform ed in t he last t hree m ont hs; e) int ake of any painkiller or oral cont racept ive 24 h prior t o t he assessm ent . A det ailed m edical int erview and clinical exam inat ion was carried out t o evaluat e inclusion and exclusion crit eria. Also, t he invest igat or r esponsible for t he eligibilit y assessm ent ( R2 ) w as an or ofacial pain specialist , t rained and calibrat ed in t he RDC/ TMD exam inat ion t echnique.
Out com es
Repor t ed facial pain int ensit y and PPT ( pr im ar y o u t co m es) , as w el l as EMG act i v i t y ( seco n d ar y out com e) , w ere assessed.
Pain int ensit y
Visual analogue scale ( VAS) was used t o assess t he int ensit y of current pain. VAS m easures t he painful experience using a st raight line of 100 m m , w it h t he left m argin anchored by t he t erm “ no pain”, and t he right , by t he t erm “ w orst im aginable pain”3.
Pressure Pain Threshold ( PPT)
PPT was conduct ed using an algom et er ( Krat os®, &RWLD63%UD]LOFRQWDLQLQJDURGZLWKDFLUFXODUÀDW
surface of 1 cm2 coat ed w it h soft rubber. The pat ient
was posit ioned com fort ably in a sit t ing posit ion, w it h m uscles relaxed. The evaluat or t hen placed t he end of t he circular surface of t he algom et er perpendicular t o t he skin and applied a st eadily increasing pressure of 0.5 kg/ cm2/ second. The pat ient was inst ruct ed t o
v er balize t he m om ent w hen t he pr essur e ex er t ed caused a painful sensat ion. The follow ing sit es w ere assessed: m asset er m u scles, an t er ior t em por alis m uscle, and st er nocleidom ast oid ( SCM) and upper t r apeziu s ( bilat er ally ) m u scles, in addit ion t o t h e lat eral pole of t he j aw. The average of t w o t rials was considered t he PPT. There was a t w o- m inut e int erval
EHWZHHQWKH¿UVWDQGVHFRQGPHDVXUHPHQWVDWWKH VDPHPXVFOHVLWHDQGD¿YHVHFRQGLQWHUYDOEHWZHHQ
t he m easurem ent s of one m uscle sit e and t he ot her7.
Elect rom yography ( EMG)
Th e su r f ace EMG r eco r d w as o b t ai n ed u si n g a Miot ec®, m odel Miot ool 4 0 0 4 - ch an n el sy st em ,
w h i ch a cq u i r e s t h e EMG si g n a l s ( 1 4 - b i t ) , w i t h elect r ical isolat ion of 3,000 volt s, high EMG signal r epr esent at ion acr oss all channels ( 2000 sam ples/ second per channel) , r ej ect ion of 110 dB com m on
PRGH DQG ORZ QRLVH OHYHO /6% /RZ 6LJQL¿FDQW
Bit ) . The acquisit ion of EMG signals was perform ed using Miograph soft war e w it h a 2000 Hz sam pling
IUHTXHQF\+]EDQGSDVV¿OWHUZLWKLQWHUIHUHQFH
elim inat ed by t he Not ch Filt er25. I n perform ing t he dat a
analysis, t he aut hors considered t he am plit ude of t he elect rical pot ent ial in m icrovolt s ( uV) , expressed by t he root m ean square ( RMS)1. Disposable and circular
elect rodes by Medit race® w ere used, w it h a 20 m m
dist ance bet w een t he poles. The gr ound elect r ode was placed in t he lat eral epicondyle of t he left elbow of all volunt eers.
A m uscle funct ion t est perform ed before placing t he elect rodes served t o ident ify t he cent er of t he m uscles t o be analyzed. The elect rodes w ere placed parallel t o
WKHPXVFOH¿EHURIWKHVHPXVFOHVHTXLGLVWDQWIURP
t he m uscle or igin and inser t ion. Befor e t he ex am it self, subj ect s w ere asked t o perform a m axim um
YROXQWDU\ FRQWUDFWLRQ 09& VXSSRUWHG E\ D ¿YH
second isom et ric cont ract ion of t he m asset er m uscles and ant erior t em poralis m uscle, in order t o conduct norm alizat ion of t he dat a, int erpret ed subsequent ly w it h t he MATLAB.
EMG signal was capt ured in t hree t asks: in t he m andibular rest posit ion ( MR) , during MVC and during habit ual chewing ( HC) . I n m easuring HC, Trident® gum
was used for 20 chew ing cycles1.
Assessm ent s
All evaluat ions w er e m ade in t hr ee assessm ent t im es: baseline ( T0) , im m ediat ely aft er ( T1) and 48 hour s aft er ( T2) t r eat m ent . The par t icipant s w er e assessed according t o t he group allocat ion ( int ent ion-t o- ion-t reaion-t analysis) .
Treat m ent ( Act ive TENS)
The volunt eer was posit ioned in dorsal decubit us w it h knees support ed on a t riangular pillow placed bet w een t he volunt eer ’s chest and head. Elect rodes w er e p laced on b ot h t h e m asset er m u scles an d t he ant er ior t em poralis m uscle beam s, consider ing t he sam e r efer ences t hat w er e used for elect r ode placem ent of t he elect rom yography surface exam .
t est ed in t he research and of t he perceived sensat ion of par est h esia f r om t h e elect r odes, r an gin g f r om unnot iceable t o hardly not iceable or very not iceable. The TENS device used was m odel Neurodyn Sapphire Com pact Lin e, by I br am ed®, w it h t w o pr ev iou sly
calibrat ed channels, and circular adhesive elect rodes by Valut rode®, 3 cm in diam et er. The param et ers used
in t his st udy w ere: pulse durat ion only up t o sensory act ivat ion ( < 100 us) and high int ensit ies, but w it h an est ablished lim it t o pr event m uscle cont ract ion and allow m axim um com fort during t he 50 m inut es of t herapy.
The t ot al t im e of t r eat m ent w as 50 m in using variat ions of low and high frequency ( VHF) , w it h a
VZHHS RI +] ¿UVW PLQ DQG +] ODVW
m in) . This applicat ion prot ocol was based on previous evidence, w hich report different and com plem ent ary analgesic m echanism w hen adopt ing high and low frequencies9,20,24,26. The TENS device was connect ed
t o a placebo dev ice w it h a select or k ey t hat w as sw it ched off, w it hout t he volunt eers know ing t his, in such a way not t o allow t hem t o dist inguish bet w een t est procedure and placebo.
Treat m ent ( placebo TENS)
Placebo dev ice w as dev eloped in t he Elect r ical Engineering Laborat ory of t he Federal Universit y of Ser gipe ( GPRUFS) , Robot ics Resear ch Gr oup. The placebo equipm ent allow ed t he passage of cur r ent t o t he part icipant for only a short period of t im e ( 40 seconds) . The current was gradually reduced in such a way t hat t he receiver would not be able t o perceive t he int errupt ion in t he st im ulus. The placebo device had an int ernal resist ance wit h values close t o hum an body resist ance. This syst em did not allow t he elect rical st im ulat ion device t o recognize t hat t he current was not going t hrough t he individual, t hus avoiding a false recording of non- cont act elect rodes.
Placebo procedure was perform ed wit h t he placebo group posit ioned in t he sam e way as t he t est group ( act ive TENS) , and w it h t he sam e current param et ers used for t he t est group. All t he pat ient s w ere t old was t hat t hey w ere part icipat ing in a st udy involving t he possibilit y of a placebo t reat m ent .
St at ist ical analysis
Qu an t i t at i v e v ar i ab l es, i . e., ag e, b o d y m ass index – body m ass divided by t he square of t he body height – ( BMI ) , VAS, PPT and EMG at different t asks
w er e pr esen t ed as m ean an d st an dar d dev iat ion ( SD) . Var iables w er e t est ed for dat a nor m alit y by t he Kolm ogorov- Sm irnov t est , and present ed norm al dist ribut ion ( p> 0.050) .
The effect of TENS on VAS, PPT and EMG act ivit y at different t asks ( MR, MVC and HC) w it hin and bet w een t he groups over t im e ( before, im m ediat ely aft er and 48 hours aft er applicat ion of TENS) was com put ed using t wo- way ANOVA for repeat ed m easures followed by Tukey’s postWHVW7KHVLJQL¿FDQFHOHYHOZDVVHW
at 5 % . I n ad d it ion , t h e ef f ect size of sig n if ican t com par ison s w as com pu t ed accor din g t o Coh en ’s
NDSSDFRHI¿FLHQWG&XWRIISRLQWVFDQLQGLFDWHVPDOO
( d= 0. 20) , m oderat e ( d= 0. 50) and lar ge ( d= 0. 80) effect s5. Missing dat a in consequence of dropout s were H[FOXGHGIURPWKH¿QDODQDO\VLV
Result s
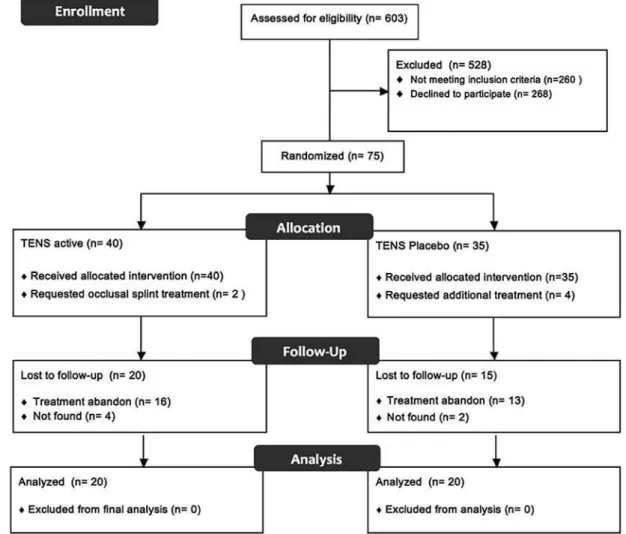
7KHÀRZRISDUWLFLSDQWVLVGHVFULEHGLQ)LJXUH,Q
addit ion, Table 1 describes t he general charact erist ics of
WKHSDUWLFLSDQWVZKRZHUHLQFOXGHGLQWKH¿QDODQDO\VLV 1RVLJQL¿FDQWGLIIHUHQFHZDVREVHUYHGEHWZHHQWKH
groups for gender, age and BMI ( p< 0.050) . Moreover, no bet w een- group difference was found in t he VAS values at any assessm ent t im e ( p> 0.050) . How ever,
WKHUHZDVDVLJQL¿FDQWGHFUHDVHLQWKH9$6YDOXHVDW
T1 ( d= - 0.79) and T2 ( d= - 0.92) w hen com pared w it h T0 values ( wit hin- group differences) only in t he act ive TENS group ( Figure 2) .
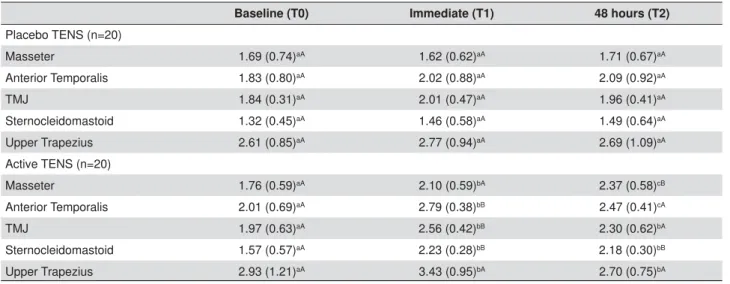
PPT values of t he ant erior t em poralis ( d= 1.13) ,
70-G DQG6&0G ZHUHVLJQL¿FDQWO\
higher in t he act ive TENS and at T1 w hen com pared w it h placebo, but also for t he m asset er ( d= 1. 05) and SCM ( d= 1.38) at T2 ( p< 0.050) ( Table 2) . There
ZDVQRVLJQL¿FDQWLQFUHDVHLQWKH337YDOXHVLQDQ\
of t h e assessm en t t im es con sider in g t h e placebo
JURXS S! +RZHYHU WKHUH ZDV D VLJQL¿FDQW
incr ease in t he PPT values of m asset er ( d= 0. 57) , ant er ior t em poralis ( d = 0.68) , TMJ ( d= 1.10) and SCM ( d= 1.46) at T1 w hen com pared w it h T0, and of m asset er ( d= 0.46) at T2 com pared w it h T1 in t he act ive TENS group ( p< 0.050) ( Table 2) .
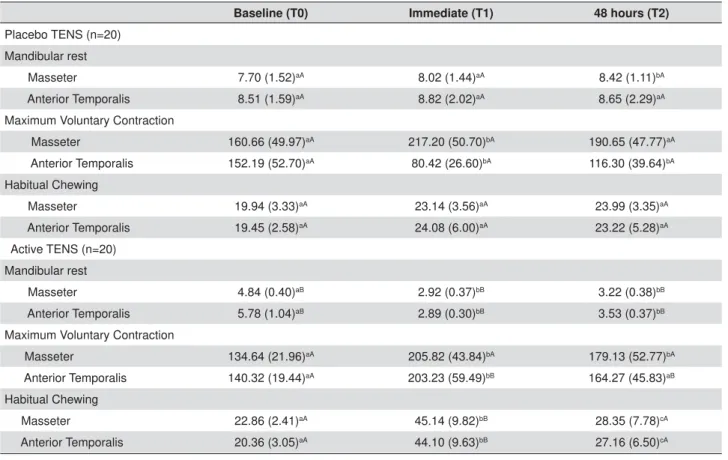
EMG act ivit y of t he m asset er ( T0, d= - 2.57, T1, d= - 4.58 and T2, d= - 6.26) and ant er ior t em poralis ( T0, d = - 2.03, T1, d= - 3.69 and T2, d= - 3.12) w ere
VLJQL¿FDQWO\ ORZHU LQ WKH DFWLYH 7(16 GXULQJ 05 DW
all assessm ent t im es w hen com pared w it h placebo ( p < 0 . 0 5 0 ) ( Tab le 3 ) . Nev er t h eless, a sig n if ican t EMG act iv it y r educt ion of t he m asset er ( d= - 4. 98)
and ant erior t em poralis ( d= - 3.77) was present ed in t he act ive TENS during MR at T1 assessm ent w hen com pared w it h T0 ( p< 0.050) , w hereas t he placebo increased MR EMG act ivit y of t he m asset er ( T0, d= 0.37 and T1, d= 0.22) at T2 assessm ent w hen com pared
w it h T0 and T1 ( p< 0.050) ( Table 3) .
EMG act ivit y of t he ant erior t em poralis ( T1, d= 2.66
DQG7G ZDVVLJQL¿FDQWO\KLJKHULQWKHDFWLYH
TENS during MVC at T1 and T2 w hen com pared w it h
SODFHERS7DEOH,QDGGLWLRQDVLJQL¿FDQW
Placebo TENS (n=20)
Active TENS (n=20)
p-value
Gender - n(%) ns
Female 15 (75%) 15 (75%)
Male 5 (25%) 5 (25%)
Age (years) - Mean (SD) 24.15 (3.01) 25.10 (3.87) ns BMI (Kg/m2) - Mean (SD 23.29 (2.28) 24.45 (5.80) ns
Axis I RDC/TMD - n(%)
IA 12(60%) 11(55%)
IA/IIA 7(35%) 8(40%)
IB 1 (5%) 0(0%)
IB/IIB 0 (0%) 1(5%)
QV QRQVLJQL¿FDQWS!
RDC/TMD=Research Diagnostic Criteria for temporomandibular disorders.
IA=myofascial pain; IIA=disk displacement with reduction; IB= myofascial pain without mouth opening limitation ;IIB=myofascial pain with mouth opening limitation
BMI= body mass index
Table 1- Baseline characteristics of the sample
increase in t he EMG act ivit y of t he m asset er ( TENS act iv e, d = 2 . 0 5 an d TENS p laceb o, d = 1 . 1 2 ) an d ant erior t em poralis ( TENS act ive, d= 1.42) was also observed in t he act ive TENS and placebo during MVC at T1 w hen com pared w it h T0 ( p< 0.050) , w hereas a
VLJQL¿FDQWUHGXFWLRQLQWKH(0*DFWLYLW\RIWKHDQWHULRU
t em poralis ( d= - 1.71) in t he placebo was obser ved during MVC at T1 w hen com pared w it h ( p< 0.050) T0 ( Table 3) .
EMG act ivit y of t he m asset er ( d= 2.97) and ant erior
WHPSRUDOLVG PXVFOHZDVVLJQL¿FDQWO\KLJKHULQ
t he act ive TENS during HC at T1 w hen com pared w it h
SODFHERS7DEOH0RUHRYHUDVLJQL¿FDQW
incr ease in t he EMG act iv it y of t he m asset er ( T1, d= 3.11 and T2, d= 0.95) and ant erior t em poralis ( T1, d= 3.32 and T2, d= 1.33) was observed only in t he act ive TENS during HC at T1 and T2 w hen com pared w it h T0 ( p< 0.050) ( Table 3) .
Baseline (T0) Immediate (T1) 48 hours (T2)
Placebo TENS (n=20)
Masseter 1.69 (0.74)aA 1.62 (0.62)aA 1.71 (0.67)aA
Anterior Temporalis 1.83 (0.80)aA 2.02 (0.88)aA 2.09 (0.92)aA
TMJ 1.84 (0.31)aA 2.01 (0.47)aA 1.96 (0.41)aA
Sternocleidomastoid 1.32 (0.45)aA 1.46 (0.58)aA 1.49 (0.64)aA
Upper Trapezius 2.61 (0.85)aA 2.77 (0.94)aA 2.69 (1.09)aA
Active TENS (n=20)
Masseter 1.76 (0.59)aA 2.10 (0.59)bA 2.37 (0.58)cB
Anterior Temporalis 2.01 (0.69)aA 2.79 (0.38)bB 2.47 (0.41)cA
TMJ 1.97 (0.63)aA 2.56 (0.42)bB 2.30 (0.62)bA
Sternocleidomastoid 1.57 (0.57)aA 2.23 (0.28)bB 2.18 (0.30)bB
Upper Trapezius 2.93 (1.21)aA 3.43 (0.95)bA 2.70 (0.75)bA
'LIIHUHQWVPDOOOHWWHUVLQWKHVDPHURZUHSUHVHQWVLJQL¿FDQWZLWKLQJURXSGLIIHUHQFHVS 'LIIHUHQWFDSLWDOOHWWHUVLQWKHVDPHFROXPQUHSUHVHQWEHWZHHQJURXSGLIIHUHQFHVS
Table 2- Mean (SD) of the pressure pain threshold (PPT) values (Kgf/cm2) of masticatory muscles, temporomandibular joint (TMJ) and
cervical muscles
VAS=visual analogue scale, T0=baseline, T1=immediately after treatment and T2=48 hours after treatment. Error-bars indicate the standard deviation of the mean
Figure 2- Mean of the pain intensity at all assessment times
Discussion
Th is st u dy dem on st r at ed t h at m ost ly of TENS h y p oalg esic p r op er t ies an d im p r ov em en t in EMG act iv it y in su bj ect s w it h m y of ascial TMD ar e n ot
SODFHERHIIHFWV7KHPDLQ¿QGLQJVZHUHDVKRUW
t er m ( T1 an d T2 ) r edu ct ion in pain in t en sit y ; b) short- t erm increase in PPT values; ( b) im m ediat e ( T1) reduct ion in MR EMG act ivit y and short - t erm increase in MVC and HC EMG act ivit y.
The evidence is cont roversial regarding t he TENS effect s of pain r educt ion in chr onic pain disor der s, t h ou g h elect r ical n er v e st im u lat ion m od alit ies in general ar e consider ed an effect iv e t r eat m ent for ch r on ic m u scu losk elet al pain . I n par t icu lar, TENS seem s t o be effect ive on reducing pain in TMD pat ient s. However, posit ive out com es are generally not report ed im m ediat ely aft er t he applicat ion, but rat her t hey are proposed as cum ulat ive effect s. Our st udy present ed bot h, im m ediat e ( T1) and cum ulat ive effect s of TENS applicat ion ( T2) , w hich could be part ially explained by t he use of high frequency TENS. Previous evidence has report ed im m ediat e effect s on TMD pain w hen applying only high frequency TENS. How ever, as far
as w e know, t here is no published st udy com paring high and low frequency TENS in TMD pat ient s, w hich warrant s furt her researches.
A pr oper TMD evaluat ion w ould include m uscle t enderness invest igat ion, which can be done by m anual palpat ion or w it h t he aid of m ore st andardized and reliable t echniques, e.g., PPT assessm ent21. Previous
evidence has shown inconsist ent result s of TENS effect on m uscle t enderness in TMD pat ient s, w it h report s of no effect s on m asset er and ant er ior t em poralis pain upon palpat ion aft er four w eeks14, but also w it h
posit iv e ef f ect s on per icr an ial m u scle t en der n ess scor e ( PTS) aft er 10 w eek s8. I nt er est ingly, t his is WKH¿UVWVWXG\WRUHSRUWWKDW7(16FDQLQFUHDVH337
of m ast icat ory m uscles, w hich reinforce t he claim ed posit ive effect s of elect rical t herapy on m uscle pain.
The pain adapt at ion m odel17 advocat es t hat chronic
m uscle pain can reduce agonist m uscle cont ract ion a n d a n i n cr e a se a n t a g o n i st m u scl e a ct i v i t y, i n or der t o pr ot ect t he agonist fr om new inj ur ies19,23. 2XU ¿QGLQJV IRU (0* DFWLYLW\ UHGXFWLRQ DW 05 DQG
increase at MVC and HC m ay point out TENS as an im port ant cont ribut ion t o lowering energy expendit ure in m aint aining j aw rest , and t o im proving t he pow er
Baseline (T0) Immediate (T1) 48 hours (T2)
Placebo TENS (n=20) Mandibular rest
Masseter 7.70 (1.52)aA 8.02 (1.44)aA 8.42 (1.11)bA
Anterior Temporalis 8.51 (1.59)aA 8.82 (2.02)aA 8.65 (2.29)aA
Maximum Voluntary Contraction
Masseter 160.66 (49.97)aA 217.20 (50.70)bA 190.65 (47.77)aA
Anterior Temporalis 152.19 (52.70)aA 80.42 (26.60)bA 116.30 (39.64)bA
Habitual Chewing
Masseter 19.94 (3.33)aA 23.14 (3.56)aA 23.99 (3.35)aA
Anterior Temporalis 19.45 (2.58)aA 24.08 (6.00)aA 23.22 (5.28)aA
Active TENS (n=20) Mandibular rest
Masseter 4.84 (0.40)aB 2.92 (0.37)bB 3.22 (0.38)bB
Anterior Temporalis 5.78 (1.04)aB 2.89 (0.30)bB 3.53 (0.37)bB
Maximum Voluntary Contraction
Masseter 134.64 (21.96)aA 205.82 (43.84)bA 179.13 (52.77)bA
Anterior Temporalis 140.32 (19.44)aA 203.23 (59.49)bB 164.27 (45.83)aB
Habitual Chewing
Masseter 22.86 (2.41)aA 45.14 (9.82)bB 28.35 (7.78)cA
Anterior Temporalis 20.36 (3.05)aA 44.10 (9.63)bB 27.16 (6.50)cA
'LIIHUHQWVPDOOOHWWHUVLQWKHVDPHURZUHSUHVHQWVLJQL¿FDQWZLWKLQJURXSGLIIHUHQFHVS 'LIIHUHQWFDSLWDOOHWWHUVLQWKHVDPHFROXPQUHSUHVHQWEHWZHHQJURXSGLIIHUHQFHVS
HI¿FLHQF\ RI MDZ IXQFWLRQV LQ SDWLHQWV ZLWK 70'
However, previous report s showed t hat high frequency
7(16 GRHV QRW LQÀXHQFH (0* DFWLYLW\ RI PDVVHWHU
an d an t er ior t em p or alis m u scles at clen ch in g in TMD pat ient s22. Discrepancy in t he TENS applicat ion
prot ocol could explain such differences, considering t hat variat ions in t he st im ulat ion frequency of TENS could be considered im port ant t o obt ain unlikeness at MR or MVC22,QDGGLWLRQVLQFHWKLVLVWKH¿UVWVWXG\WR GHPRQVWUDWH7(16HI¿FDF\RQPXVFOHSDLQZLWKWKHDLG
of evaluat ion of m uscle EMG act ivit y at t hree different t asks, m ore researches are required t o support our
¿QGLQJVPDLQO\LQWKHORQJWHUPDVVHVVPHQW
Su ch p osi t i v e sh or t - t er m ef f ect s of TENS on m uscle pain and funct ion could be relat ed w it h t he alt ernat e frequencies prot ocol adopt ed in our st udy. Th is ap p licat ion p r ot ocol w as b ased on p r ev iou s evidence, w hich report different and com plem ent ary analgesic m echanism w hen adopt ing high and low f r e q u e n ci e s9 , 2 6. Hi g h f r e q u e n cy TENS h a s b e e n
associat ed w it h segm ent al pain inhibit ion at neurons locat ed in t he dorsal horn and it can reduce nocicept ive su b st a n ce s r e l e a se d i n p e r i p h e r a l t i ssu e s2 4. I n
addit ion, low frequency TENS has been associat ed wit h
UHOHDVHRIHQNHSKDOLQVDQGǃHQGRUSKLQVZLWKLQWKH
descending pain m odulat ion syst em24. Nevert heless, LWLVLPSRUWDQWWRQRWHWKDWWKLVLVWKH¿UVWUHSRUWLQ
t he lit erat ure on t he use of alt ernat e frequencies in TMD pat ient s. Consider ing t hat t her e is no sound con clu sion s r egar din g t h e opt im al TENS pr ot ocol, furt her invest igat ion is required not only t o det erm ine
VXSHULRUHI¿FDF\RIDOWHUQDWHIUHTXHQF\7(16WKHUDS\
for m yofascial TMD but rat her t o est ablish guidelines for TENS applicat ion.
The st rengt hs of t his st udy are m ainly relat ed w it h t he syst em at ic assessm ent of m yofascial TMD pain and m uscle funct ion using valid and reliable m et hods. On t h e ot h er h an d, som e lim it at ion s t h at can be highlight ed in t his st udy w ere: a) lack of a long- t erm assessm ent ; b) lack of a cont rol group w it hout any
WUHDWPHQWVLQFHDVSHFWVUHODWHGWRÀXFWXDWLRQSHULRGV
and pain rem ission in TMD pat ient s m ust be considered b e f o r e a n y f i n a l j u d g m e n t i s m a d e r e g a r d i n g
WKHUDSHXWLFHI¿FDF\DOWKRXJKHWKLFDOLPSOLFDWLRQVRI
such pr ocedur e should be consider ed; c) lack of a cont rol group w it hout TMD, w hich could also elucidat e t he effect s of TENS on asym pt om at ic m uscles; d) risk of t reat m ent bias, because t he researcher who applied t he t reat m ent was aware about t he group allocat ions.
Conclusions
Short- t erm t herapeut ic effect s of TENS are superior t o t h ose of t h e placebo, becau se of t h e r epor t ed facial pain , deep pain sen sit iv it y an d m ast icat or y m uscle EMG act ivit y im provem ent . Accordingly, w e recom m end t he use of TENS as an effect ive opt ion for short- t erm m anagem ent of m ast icat ory m yofascial pain. How ever, furt her invest igat ions are required t o
GHWHUPLQHLIWKLVHI¿FDF\LVDOVRSUHVHQWLQWKHORQJ
t erm effect s.
&RQÀLFWRILQWHUHVW
1RFRQÀLFWWRGHFODUH
Acknow ledgm ent s
The authors would like to thank CAPES – Coordination for t he I m provem ent of Higher Educat ion Personnel and São Paulo Research Foundat ion ( FAPESP) , grant # 2015/ 09913- 4.
References
1- Ardizone I , Celem in A, Aneiros F, del Rio J, Sanchez T, Moreno
I . Elect rom yographic st udy of act ivit y of t he m asset er and ant erior
t em poralis m uscles in pat ient s w it h t em porom andibular j oint ( TMJ)
dysfunct ion: com parison w it h t he clinical dysfunct ion index. Med Oral
Pat ol Oral Cir Bucal. 2010; 15: e14- 9.
2 - Aw an KH, Pat il S. The r ole of t ranscut aneous elect r ical ner v e
st im ulat ion in t he m anagem ent of t em porom andibular j oint disorder.
J Cont em p Dent Pract . 2015; 16: 984- 6.
3- Carlsson AM. Assessm ent of chronic pain. I . Aspect s of t he reliabilit y
and validit y of t he visual analogue scale. Pain. 1983; 16: 87- 101. &DVWURÀRULR7%UDFFR3)DULQD'6XUIDFHHOHFWURP\RJUDSK\LQWKH assessm ent of j aw elevat or m uscles. J Oral Rehabil. 2008; 35: 638- 45.
5 - Cohen J. The concept s of pow er analy sis. I n: _ _ _ _ _ _ , edit or.
St at ist ical pow er analysis for t he behavioral sciences. New Jersey:
Hillsdale; 1988. p 1- 17.
6- Cooper BC, Kleinber g I . Est ablishm ent of a t em por om andibular
phy siological st at e w it h neur om uscular or t hosis t r eat m ent affect s
reduct ion of TMD sym pt om s in 313 pat ient s. Cranio. 2008; 26: 104- 17.
7- Cost a DR, Lim a Ferreira AP, Pereira TA, Porporat t i AL, Cont i PC, Cost a
YM, et al. Neck disabilit y is associat ed w it h m ast icat ory m yofascial
pain and regional m uscle sensit ivit y. Arch Oral Biol. 2015; 60: 745- 52. 'H *LRUJL , &DVWURÀRULR 7 6DUWRULV % 'HUHJLEXV $ 7KH XVH RI convent ional t ranscut aneous elect r ical ner ve st im ulat ion in chr onic
facial m yalgia pat ient s. Clin Oral I nvest ig. 2016. Epub ahead of print .
9- Desant ana JM, Sant ana- Filho VJ, Sluka KA. Modulat ion bet w een
high- and low- fr equency t ranscut aneous elect r ic ner ve st im ulat ion
delays t he developm ent of analgesic t olerance in art hrit ic rat s. Arch
Phys Med Rehabil. 2008; 89: 754- 60.
1 0 - D w o r k i n SF, LeResch e L. Resea r ch d i a g n o st i c cr i t er i a f o r
11- Gem m ell H, Hilland A. I m m ediat e effect of elect ric point st im ulat ion
( TENS) in t reat ing lat ent upper t rapezius t rigger point s: a double blind
random ised placebo- cont rolled t rial. J Bodyw Mov Ther. 2011; 15:
348-54.
12- Gourlay DL, Heit HA, Alm ahrezi A. Universal precaut ions in pain
m edicine: a rat ional approach t o t he t reat m ent of chronic pain. Pain
Med. 2005; 6: 107- 12.
1 3 - Joh n son MI , Paley CA, How e TE, Slu k a KA. Tr an scu t an eou s
elect rical nerve st im ulat ion for acut e pain. Cochrane Dat abase Syst
Rev. 2015: CD006142.
14- Kat o MT, Kogawa EM, Sant os CN, Cont i PC. TENS and low- level
laser t herapy in t he m anagem ent of t em porom andibular disorders. J
Appl Oral Sci. 2006; 14: 130- 5.
15- Khadilkar A, Odebiyi DO, Brosseau L, Wells GA. Transcut aneous
elect rical nerve st im ulat ion ( TENS) versus placebo for chronic low- back
pain. Cochrane Dat abase Syst Rev. 2008: CD003008.
16- Lobbezoo F, van Selm s MK, Naeij e M. Mast icat ory m uscle pain
and disordered j aw m ot or behaviour: lit erat ure review over t he past
decade. Arch Oral Biol. 2006; 51: 713- 20.
17- Lund JP, Donga R, Widm er CG, St ohler CS. The pain- adapt at ion
m odel: a discussion of t he relat ionship bet ween chronic m usculoskelet al
pain and m ot or act ivit y. Can J Physiol Pharm acol. 1991; 69: 683- 94.
1 8 - Mon aco A, Sgolast r a F, Ciar r occh i I , Cat t an eo R. Ef f ect s of
t ranscut aneous elect rical nervous st im ulat ion on elect rom yographic and
kinesiographic act ivit y of pat ient s w it h t em porom andibular disorders:
a placebo- cont rolled st udy. J Elect rom yogr Kinesiol. 2012; 22: 463- 8.
19- Monaco A, Sgolast ra F, Piet ropaoli D, Giannoni M, Cat t aneo R.
Com par ison bet w een sensor y and m ot or t ranscut aneous elect r ical
nervous st im ulat ion on elect rom yographic and kinesiographic act ivit y
of pat ient s wit h t em porom andibular disorder: a cont rolled clinical t rial.
BMC Musculoskelet Disord. 2013; 14: 168.
20- Oost erhof J, Sam wel HJ, de Boo TM, Wilder- Sm it h OH, Oost endorp
RA, Crul BJ. Predict ing out com e of TENS in chronic pain: a prospect ive,
random ized, placebo cont rolled t rial. Pain. 2008; 136: 11- 20.
2 1 - Par k G, Kim CW, Par k SB, Kim MJ, Jan g SH. Reliabilit y an d
usefulness of t he pressure pain t hreshold m easurem ent in pat ient s
w it h m yofascial pain. Ann Rehabil Med. 2011; 35: 412- 7.
22- Rodrigues D, Siriani AO, Bérzin F. Effect of convent ional TENS on
pain and elect rom yographic act ivit y of m ast icat ory m uscles in TMD
pat ient s. Braz Oral Res. 2004; 18: 290- 5.
5RGUtJXH])HUQiQGH]$/*DUULGR6DQWR¿PLD9*HLWD5RGUtJXH] J, Fer nández- de- Las- Peñas C. Effect s of bur st - t ype t ranscut aneous
elect rical nerve st im ulat ion on cervical range of m ot ion and lat ent
m y ofascial t r igger poin t pain sen sit iv it y. Ar ch Phy s Med Reh abil.
2011; 92: 1353- 8.
24- Sluka KA, Walsh D. Transcut aneous elect rical nerve st im ulat ion:
b a si c sci e n ce m e ch a n i sm s a n d cl i n i ca l e f f e ct i v e n e ss. J Pa i n .
2003; 4: 109- 21.
2 5 - Tar t ag lia GM, Lod et t i G, Paiv a G, De Felicio CM, Sf or za C.
Surface elect rom yographic assessm ent of pat ient s w it h long last ing
t em por om an dibu lar j oin t disor der pain . J Elect r om y ogr Kin esiol.
2011; 21: 659- 64.
2 6 - To n g KC, Lo SK, Ch e i n g GL. Al t e r n a t i n g f r e q u e n ci e s o f
t ranscut aneous elect r ic ner ve st im ulat ion: does it pr oduce gr eat er
analgesic effect s on m echanical and t herm al pain t hresholds? Arch