Detection of multi drug resistant bacteria in major hospitals in Kano,
North-West, Nigeria
I. Yusuf
1, A.H. Arzai
1, M. Haruna
2, A.A. Sharif
3, M.I. Getso
3 1Department of Microbiology, Faculty of Science, Bayero University, Kano, Nigeria.
2
Department of Biology, Kano University of Science and Technology, Wudil, Kano, Nigeria.
3
Department of Microbiology and Parasitology, Faculty of Medicine, Bayero University, Kano, Nigeria.
Submitted: January 26, 2013; Approved: March 14, 2014.
Abstract
Two major hospitals in Kano, North West Nigeria have recorded increasing resistance of clinical pathogens to broad spectrumblactams, mediated by extended spectrumb- lactamase (ESbL) and non ESBLs. A study was therefore undertaken to determine the occurrence and prevalence of plasmid and chromosomal mediated AmpC bL and carbapenemase in addition to already known ESBL due to increasing resistance of pathogens from the two hospitals to carbapenems, cephamycins and flouroquinolones. Antibiogram tests and ESBL, AmpC and carbapenemase production tests were performed on all the isolates. AmpC and carbapenemase producers were further screened for AmpC inducibility and metallo beta lactamase production respectively. Majority of the isolates (> 80%) were resistant to bothb-lactam and nonb-lactam antibiotics. Reduced susceptibility to levofloxacin, nitrofurantoin, nalidixic acid and ofloxacin among the isolates were observed with the exception ofP. aeruginosawhich is totally resistant to imipenem and levofloxacin. An overall preva-lence of 14.4%, 11.9% and 11.9.3% for ESbL, AmpC and carbapenemase was observed respectively. About 7.9% of the AmpC producers can over expressed the chromosomally mediated AmpC and 85.8% of the carbapenemase producers require metal for their action. Co-production of either of two and/or all of the enzymes was observed inE. coli, P. mirabilisandP. aeruginosa. Antibiotic resis-tance among isolates from the two hospitals is increasing and the major cause of this resisresis-tance in the pathogens studied are production of AmpC, carbapenemase (especially Metallob- lactamase) in ad-dition to already known ESBL enzymes by the pathogens. Some of the isolates also possess the ca-pacity to elaborate two or more of the enzymes concurrently, which would renders them resistant to a multitude of antibiotics.
Key words:AmpCb-lactamases, extended spectrumb-lactamases, coexistence, prevalence, Gram negative bacteria.
Introduction
b-lactamases are enzymes produced by some bacteria and are responsible for their resistance tob-lactam antibiot-ics like penicillins, cephamycin and carbapenem (Bushet al., 1995).b-lactamase deactivates the molecular antibacte-rial properties ofb-lactam antibiotics there by breaking and opening the common element in their molecular structure
b-lactam (Bushet al., 1995). Some of these enzymes
in-clude extended spectrumb-lactamase (ESBL), AmpCbL, and carbapenemase.
ESBLs are plasmid-mediatedb-lactamase that are ca-pable of efficiently hydrolyzing penicillin, narrow and broad spectrum cephalosporins and monobactams (Aztreo-nam), but they do not hydrolyze cephamycin or carba-penems (imipenem, meropenem) (Emery and Weymouth, 1997). b-Lactamase, inhibitors such as clavulanic acid, sulbactam and tazobactam generally inhibit ESBL
produc-Brazilian Journal of Microbiology 45, 3,791-798(2014) Copyright © 2014, Sociedade Brasileira de Microbiologia
ISSN 1678-4405 www.sbmicrobiologia.org.br
Send correspondence to I. Yusuf. Department of Microbiology, Faculty of Science, Bayero University, P.M.B. 3011, Kano, Nigeria. E-mail: [email protected].
ing strains (Naumorskil and Palzkill, 1999). ESBL produc-ing isolates are most commonly found in Klebsiella pneumoniae and Escherichia coli (Winokur and Brueggemann-Desalvo, 2005).
AmpC b-lactamase is primarily chromosomal and plasmid-mediated and are resistant tob-lactamase inhibi-tors such as clavulanic acid but can hydrolyze cephamycin (Livermore and Woodford, 2000). Carbapenems are one of the antibiotics of last resort for many bacterial infections such asE. coli andK. pneumoniaeproducing AmpC and extended spectrum b-lactamase but the emergence of carbapenemase which have versatile hydrolytic capacities have the ability to hydrolise pencillins, cephalosporins, monobactams and carbapenems (Fernandoet al., 2009).
Infection caused by organisms producing such en-zymes have resulted in poor outcomes, reduced rate of clin-ical and microbiologclin-ical responses, longer hospital stays and greater hospital expenses (Patersonet al., 2004). Physi-cal contact is the most likely mode of transmission and the gastrointestinal tract of colonized or infected patients is the most frequent reservoir while transient carriage of bacteria on the hands of healthcare workers may lead to transmis-sion to patients (Patersonet al., 2004).
The spread of these resistant bacteria in hospitals all over the world, conferring multiple antibiotic resistances in the treatment and management of life threatening infec-tions necessitate this study. The routine susceptibility tests performed by clinical laboratories in Nigeria, fail to detect bacteria harboring these enzymes, which have led to inap-propriate and unsuccessful therapy of patient and unneces-sary use of drugs. This study was therefore aimed at deter-mining the antibiotic susceptibility of the commonly isolated pathogens in Aminu Kano Teaching Hospital, Kano (AKTH) and Murtala Muhammad Specialist Hospi-tal, Kano (MMSH), North-west Nigeria to commonly pre-scribed antibiotics and relates the gross antibiotic resis-tance to production of AmpC, carbapenemase and ESBL and their co-production in different isolates.
Materials and Methods
Collection of clinical isolates
A total of six hundred and thirty three (633) consecu-tive non repeticonsecu-tive Gram negaconsecu-tive clinical bacterial isolates derived from samples of urine, catheter tips, stool, semen, urogenitals, and abscesses were collected from pathology department of AKTH and MMSH over a period of 12 months. The isolates included E. coli (278), Klebsiella pneumoniae(128),Proteus mirabilis(89),P. vulgaris(32), Pseudomonas aeruginosa (83), Salmonella typhi (4), Serratia mercesens (1), Morganella spp (2) and Enterobacter spp(16). Isolates were obtained from both outpatients and inpatients. However, attention were given to 17 isolates from inpatients admitted into intensive care unit (ICU) and Special Care Baby Unit (SCBU) which
in-cluded 7E. coli, 4K. pneumoniae, 1P. mirabilisand 5P. aeruginosathat were totally resistant to all the antibiotics tested against them in the laboratory.
Antimicrobial susceptibility testing
An antibiotic susceptibility test was performed on all the isolates by disc diffusion method (CLSI, 2005). The zone diameters of each of the antibiotics were interpreted as per Clinical Laboratory Standards Institute (CLSI) recom-mendations (CLSI, 2005). Sixteen different antibiotic discs commonly prescribed by clinicians in the two hospitals ex-cept cefoxitin were used. These included: gentamicin (10 mg), co-trimoxazole (25 mg), ciprofloxacin (5 mg), cefpodoxime (30 mg), ceftazidime (30 mg), ceftriaxone (30mg), cefoxitin (30mg), imipenem (10mg), nalidixic acid (30 mg), amoxycillin (20 mg), ofloxacin (30 mg), levo-floxacin (30 mg), nitrofurantoin (300 mg), tetracycline (30mg), chlorampenicol (30mg) and augmentin (30 mg) (Oxoid, UK). Escherichia coli ATCC 25922 strain was used as a control culture.
Beta lactamase detection, presumptive and confirmatory test for ESBL
The types ofb-lactamase produced by the clinical iso-lates were investigated by phenotypic based methods.
All the clinical isolates collected were tested for po-tential ESBL producers using the cefpodoxime (10 mg) ceftazidime (30mg) and the ceftriaxone (30mg) antibiotic discs (Oxoid, UK). Results were interpreted based on the CLSI criteria (CLSI, 2005). Organisms showing a zone of inhibition of £ 21 mm to cefpodoxime or £ 20 mm to ceftazidime and ceftriaxone were subjected to confirmatory test using the double discs synergy test as described by CLSI guidelines (CLSI, 2005). In the method, a suspension of the test organism was inoculated on Mueller- Hinton agar (MHA) (Oxoid, UK). A disc containing 30 mg amoxicillin plus clavulanic acid was placed centrally on the plate. Discs containing cefpodoxime (10 mg) and ceftriaxone (30mg) were placed on the agar at a distance of 15 mm from the amoxicillin + clavulanic acid disk. The plates were incubated over night at 35 °C. A³5 mm in-crease in zone diameter for either antimicrobial agent com-bination compared to its zone when tested alone signified a positive ESBL.
AmpC screening and confirmatory test
The susceptibility of the isolates to cefoxitin disc 30mg (Oxoid, UK) was determined and all isolates that yielded a zone diameter less than 18 mm were tested for AmpC enzyme production by AmpC disk test according to the method of Blacket al.(2005).
UK) plate. A 30mg cefoxitin (Oxoid, UK) disc was placed on the inoculated surface of the agar. A sterile plain disc in-oculated with 2-3 pure colonies of the test organism was placed beside the cefoxitin disc 2 mm away from the edge, with the inoculated disk face in contact with the agar sur-face. The plates were incubated at 37 °C for 24 h. After in-cubation, the plates were examined for either an indentation or a flattening of the zone of inhibition, indicating enzy-matic inactivation of cefoxitin (positive result), or the ab-sence of a distortion, indicating no significant inactivation of cefoxitin (negative result).
Detection of inducible AmpC production (Disc antagonism test)
Screening for the inducible AmpCb-lactamase was done by the method of Sanderset al.(1996). This was done by placing cefoxitin disc (Oxoid, UK) at a distance of 20 mm from ceftazidime (Oxoid, UK) on the surface of MHA inoculated with the test organism.b-lactamase inducibility was recognized by blunting of the ceftazidime (Oxoid, UK) zone adjacent to cefoxitin (Oxoid, UK).
Screening and confirmatory test for carbapenemase
The bacterial isolates were screened for carbape-nemase production according to CLSI guidelines (CLSI, 2005). In this method, carbapenem antibiotics-meropenem (MEM) and imipenem (IPM) discs (10mg, each) (Oxoid, UK) were used. The antibiotic discs were placed on the sur-face of MHA plates using sterile forceps. The discs were placed about 30 mm apart and the plates were incubated for 24 h at 37 °C after which zones of inhibitions were read. Isolates that showed a zone of inhibition£21 mm in diame-ter for meropenem were considered as suspected carba-penemase producers and were subjected to confirmatory test by the Modified Hodges Test (MHT).
Modified hodges test
A Mcfarland suspension ofE. coliATCC 25922 was streaked with a sterile cotton swab on surface of MHA plates. Two discs of meropenem and imipenem (10mg) were placed on the surface of MHA 30 mm apart lying di-agonally opposite to each other. In a straight line, by means of a sterilized wire loop, the test organisms were streaked from the edge of one disc meropenem to edge of the other imipenem disc. Up to four organisms were tested on the same MHA plate. The plates were incubated at 37 °C for 24 h.
They were examined for a clover leaf type indentation or flattening at the intersection of the test organism andE. coli ATCC 25922 within the zone of inhibition of the carbapenem susceptibility disc as described by Andersonet al.(2007).
Screening of carbapenemase producers for Metallo b-Lactamases (MBLs)
EDTA-disc synergy test was used as described by Walshet al.(2005) and CLSI, (2005). A carbapenemase producing isolate was streaked on the surface of the MHA using a sterile wire loop. Two meropenem discs, one con-taining EDTA and the other without EDTA were placed on the surface of the MHA using a sterile forceps at a distance of about 30 mm apart. The EDTA disc was prepared by adding 250mL of neutral EDTA to MEM. The plates were incubated for 24 h at 37 °C. Zones of inhibition were re-corded after 24 h of incubation. Control disc containing EDTA alone was used to determine the activity of the EDTA to ensure that it does not cause false-positive results by inhibiting the test isolate. Organisms that showed differ-ence in diameter of zone of inhibition by³4 mm on the MEM containing EDTA and MEM alone is confirmed for the production of MBLs.
Results
Antimicrobial susceptibility testing
Antibacterial susceptibility of clinical isolates from the two hospitals to the commonly prescribed antibiotics in the hospitals showed that majority of the isolates were re-sistant tob-lactam antibiotics such amoxicillin, augmentin, cefpodoxime, ceftriaxone and nonblactam antibiotics such as chlorampenicol, co-trimoxazole and tetracycline. Major-ity of the isolates showed reduced susceptibilMajor-ity to levo-floxacin, nitrofurantoin, nalidixic acid and ofloxacin with the exception ofP. aeruginosawhich is totally resistant to imipenem and levofloxacin but showed enhanced sensitiv-ity to cefoxitin (Table 1).
ESBL, AmpC and carbapenemase producing isolates
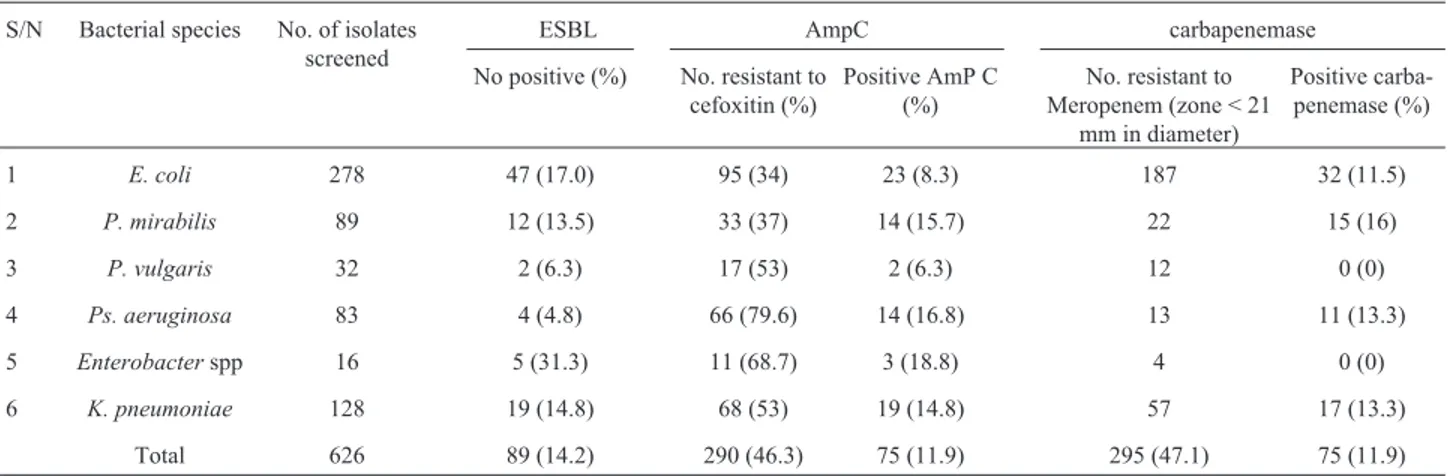
Out of the 633 isolates screened for ESBL produc-tion, 91 were confirmed to produce ESBL giving an overall prevalence of 14.4%. The highest prevalence of ESBLs was found inEnterobacter spp(31.3%), followed byE. coli (17%), K. pneumoniae (14.8%), P. mirabilis (13.5%) P. vulgaris (6.3%) and Ps. aeruginosa had the least ESBL prevalence of 4.8% (Table 2). No ESBL production was de-tected in Serratia mercenses but one out of the two M. morganiiproduces ESBL.
The susceptibility of the isolates to cefoxitin disc showed that 291 isolates equivalent to (46.3%) were found to be either resistant or showed reduced susceptibility to cefoxitin while 342 (54%) were susceptible (Table 3). The overall prevalence of AmpCb-lactamases was 11.9%. Sim-ilar to ESBL,Enterobacter spphad the highest prevalence of (18.8%), followed by Ps. aeruginosa (16.8%), P. mirabilis(15.7%),K. pneumoniae(14.4%),E. coli(8.3%) andP. vulgaris(6.3%).
Yusuf
et
al.
No. of susceptible bacteria to common antibiotics and their percentages
Antibiotics E. coli
N = 278
K. pneumoniae N = 128
Enterobacter spp N = 1
Salmonellaspp. N = 4
Ps. aeruginosa N = 83
P. mirabilis N = 89
P. vulgaris N = 32
No. % No. % No. % No. % No. % No. % No. %
Amoxycillin 6.0 2.2 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1.0 3.1
Augmentin 29.0 10.4 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 6.0 18.7
Cefoxitin 95.0 34.2 68.0 53.1 11.0 68.8 0.0 0.0 66.0 79.5 33.0 37.1 17.0 53.1
Cefpodoxime 59.0 21.2 0.0 0.0 2.0 8.3 0.0 0.0 0.0 0.0 0.0 0.0 3.0 9.4
Ceftriazone 88.0 31.7 0.0 0.0 2.0 8.3 0.0 0.0 0.0 0.0 0.0 0.0 5.0 15.6
Ceftazidime 0.0 0.0 0.0 0.0 4.0 25.0 2.0 50.0 0.0 0.0 0.0 0.0 3.0 9.4
Ciprofloxacin 54.0 19.4 35.0 33.0 4.0 25.0 0.0 0.0 41.0 49.4 52.0 58.4 11.0 34.4
Chloramphenicol 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Cotrimaxazole 41.0 14.7 52.0 50.0 3.0 18.7 0.0 0.0 0.0 0.0 0.0 0.0 3.0 9.4
Gentamycin 60.0 21.6 23.0 22.1 5.0 31.3 0.0 0.0 76.0 91.6 0.0 0.0 18.0 56.3
Imipenem 237.0 85.3 73.0 70.2 9.0 56.3 4.0 100.0 0.0 0.0 77.0 86.5 15.0 46.9
Levofloxacin 184.0 66.2 47.0 45.2 5.0 31.3 2.0 50.0 0.0 0.0 0.0 0.0 12.0 37.5
Nitrofurantoin 212.0 76.3 47.0 45.2 8.0 50.0 0.0 0.0 54.0 65.1 63.0 70.8 8.0 25.0
Nalidixic acid 119.0 42.8 8.0 7.6 10.0 62.5 2.0 50.0 35.0 42.2 0.0 0.0 6.0 18.8
Ofloxacin 151.0 54.5 33.0 31.7 7.0 43.7 0.0 0.0 71.0 85.5 73.0 82.0 9.0 28.1
Among the AmpC producers, 57.1% showed indenta-tion (high producindenta-tion of AmpC enzyme) while 42.1% showed flattening (low production of AmpC enzyme) (Ta-ble 3).
In addition to plasmid mediated AmpCb-lactamase, the chromosomal expressions of the AmpC among the plasmid mediated strains were investigated. Out of the 77
AmpC producing isolates, inducible AmpC b-lactamase was detected in 6 (7.8%). Highest was recorded among the Ps. aeruginosa(26.7%),P. mirabilis(3.2%).
Furthermore, sixty five out of the six hundred and thirty three isolates (10.3%) produces carbapenemase. The highest prevalence of carbapenemase producers was in Proteus mirabilis (16.0%), then Ps. aeruginosa, K. pneumoniae(13.3% each) andE. coli(11.5%) (Table 2).
Majority of the carbapenemase producers produces MBLs (85.5%) a type carbapenemase requiring Zn+ for ac-tivity (Sinha et al., 2008).
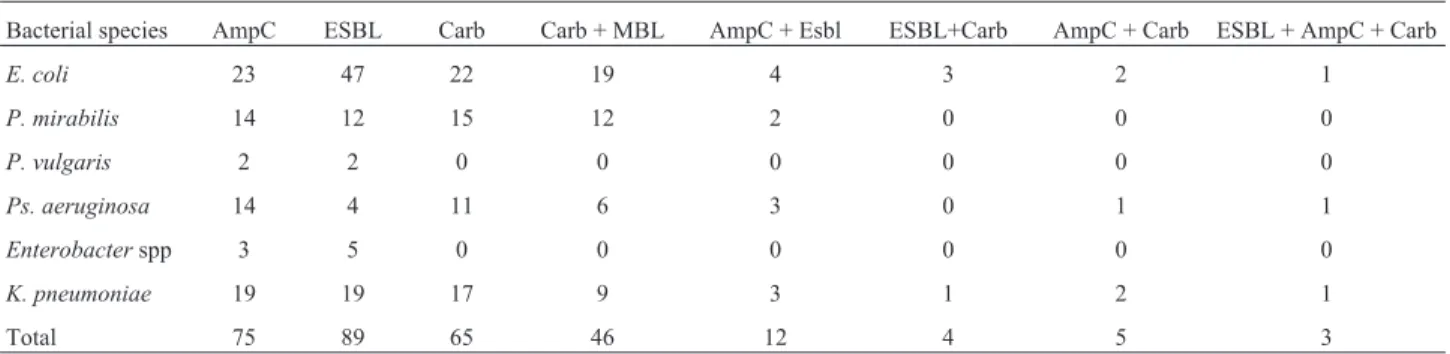
Co-Production of ESBL, AmpC, MBL and carbapenemase
The co-production of carbapenemase, MBL AmpC and ESBL was also observed among the isolates. Various combinations of different types of enzymes were found particularly inE. coliandK. pneumoniae(Table 4).
Discussions
The distribution of antibiotic resistance tob-lactams in our study was very similar to that described by Stéphane et al.(2003) with nearly all of the isolates being resistant or slightly susceptible to commonly prescribed antibiotics in the two hospitals, and many of the isolates showing a de-creased susceptibility or resistance to promising antibiotics such as imipenem, levofloxaxin, cefoxitin, cefpodoxime and ceftriaxone (Table 1). This could be linked to the un-controlled consumption of antimicrobials in Kano such as underuse through lack of access, inadequate dosing, poor adherence, widespread of substandard antibiotics and sales of antibiotics in open markets play an important role. Inap-propriate consumption of antimicrobials in Kano may be stimulated by marketing practices such as
direct-to-con-Emergence of superbugs in N-W Nigeria 795
Table 2- Prevalence of ESBL, AmpC and carbapenemase producers among Gram negative clinical isolates. S/N Bacterial species No. of isolates
screened
ESBL AmpC carbapenemase
No positive (%) No. resistant to cefoxitin (%)
Positive AmP C (%)
No. resistant to Meropenem (zone < 21
mm in diameter)
Positive carba-penemase (%)
1 E. coli 278 47 (17.0) 95 (34) 23 (8.3) 187 32 (11.5) 2 P. mirabilis 89 12 (13.5) 33 (37) 14 (15.7) 22 15 (16)
3 P. vulgaris 32 2 (6.3) 17 (53) 2 (6.3) 12 0 (0)
4 Ps. aeruginosa 83 4 (4.8) 66 (79.6) 14 (16.8) 13 11 (13.3) 5 Enterobacterspp 16 5 (31.3) 11 (68.7) 3 (18.8) 4 0 (0) 6 K. pneumoniae 128 19 (14.8) 68 (53) 19 (14.8) 57 17 (13.3)
Total 626 89 (14.2) 290 (46.3) 75 (11.9) 295 (47.1) 75 (11.9)
Note: figures in parenthesis are percentages.
Table 3- Confirmation of Amp Cb-lactamases (Amp C disc test).
S/N Bacterial species No of isolates screened Positive AmpC No distortion
indentation flattening
1 E. coli 95 14 10 71
2 P. mirabilis 33 9 5 39
3 P. vulgaris 17 0 2 15
4 Ps. aeruginosa 66 6 8 52
5 M. morganii 2 1 0 1
5 Enterobacterspp 11 1 2 8
6 K. pneumoniae 68 13 6 49
Total 290 44 (57.1) 33 (43.4) 235
sumer advertising which allows pharmaceutical companies to market medicines directly to the public via television, ra-dio, print media, and the internet.
High prevalence of ESBL, AmpC and carbapene-mase among the clinical bacterial isolates in the two major hospitals has negative health implications. The prevalence of ESBL is high when compared with the findings of Yushauet al.(2007) who first reported 9.3% prevalence in Kano, Nigeria in 2007. From then, higher reports of these enzymes among clinical isolates in Kano have been made even among the immune-compromised patients such as tu-berculosis and cancer patients (Eyitayoet al., 2009; Yusuf et al., 2011). The high prevalence of ESBL among Enterobacterspp,E. coliandK. pneumoniaein this study is of clinical important as these species are among the most frequent Gram-negative bacteria involved in hospital-acquired infections and nosocomial outbreaks in Kano, Ni-geria. Reports of ESBL inEnterobacterin Nigeria is not new, as it spread across the geo political zones of the coun-try. For instance, Aibinu et al. (2003) recorded 20% in Lagos South West-Nigeria and Akujobi and Ewuru (2010), in Nnewi, Anambra, South East Nigeria.
Initially is was ESBL that was suspicious to be re-sponsible forb-lactam resistance among our isolates from their initial reports in 2007 among some of their isolates, but due to (i) increased rates of resistance to cefpodoxime, ceftriaxone, ceftazidime in association with clavulanate (ii) decreased susceptibility or resistance to cefoxitin and/or carbapenem, plasmid/chromosomal mediated AmpCb -lac-tamases and carbapenemase were thought to pose new clin-ical threat because these enzymes confer resistance to cephamycins and they are not affected byb-lactamase in-hibitors, and can, in strains with loss of outer membrane porins, provide resistance to carbapenems. In view of the above, the isolates were further screened for other beta lactamase enzymes such as AmpC and carbapenemase beta lactamases.
The prevalence of AmpC production was 11.9%. This prevalence rate is higher than that reported from some parts of the world. For instance, Singhalet al.(2005) reported 8% in India, Eyitayo et al. (2009) however reported a
higher prevalence (23%) in Lagos-Nigeria among cancer patients.
Phenotypic detection of AmpC inE. colias used in this study does not indicate if the enzyme is chromosomal or plasmid mediated. Chromosomal AmpC b-lactamase was not detected in E. coli in this study meaning that plasmid mediated AmpC which are faster to spread to other bacteria are the cause of their wide spread in the hospitals. Initially, moderate resistance of some of the isolates to mul-tiple drugs was used to suggest a chromosomal AmpC (Kenneth, 2010), and resistance to multiple drugs shown my most of theE. coliis suggestive of plasmid-mediated AmpC production, but even the moderately resistant ones showed no chromosomal expression.
Out of the 291 (46%) of the isolates showing resis-tance to cefoxitin in the present study, only 76 (26.1%) were AmpC producers. Cefoxitin resistance in this type of AmpC negative isolates could be due to a decreased perme-ability of porins (Clark, 1996; Leeet al., 2003).
Carbapenemase-producing isolates have not been de-scribed to date in Nigeria. Here, we report the emergence of carbapenemase producing clinical isolates in two major hospitals in Kano, Nigeria. Although, carbapenem usage in Kano, Nigeria is low because of their cost. The origin or source of these carbapenemase-producing isolates is un-known, but genotypic studies of the isolates could answer questions about whether the strains were imported or they emerged locally and spread by gene transfer. This is be-cause one of the patients from AKTH has a history of travel to India for treatment. Equally important is that patients from MMSH are usually being referred to AKTH when their conditions deteriorate, this will facilitate their spread to other hospitals. The MHT used for carbapenemase con-firmation in the study does not distinguish between carba-penemase types and lacks sensitivity for MBLs detection (Leeet al., 2003). Specific MBLs confirmatory test involv-ing EDTA (chelatinvolv-ing agent) was used (Walshet al., 2005).
The total resistance of P. aeruginosa to imipenem raise suspicious of carbapenemase production initially as carbapenemase-producingP. aeruginosastrains is known to exhibit reduced susceptibility to imipenem (Queenan and Bush, 2007). In addition, some after showing negative Table 4- Co-existence of ESBLs, AmpC, MBL and Carbapenemase.
Bacterial species AmpC ESBL Carb Carb + MBL AmpC + Esbl ESBL+Carb AmpC + Carb ESBL + AmpC + Carb
E. coli 23 47 22 19 4 3 2 1
P. mirabilis 14 12 15 12 2 0 0 0
P. vulgaris 2 2 0 0 0 0 0 0
Ps. aeruginosa 14 4 11 6 3 0 1 1
Enterobacterspp 3 5 0 0 0 0 0 0
K. pneumoniae 19 19 17 9 3 1 2 1
ESBL and AmpC, but still showed reduced or no sensitivity to carbapenem, this also raises suspicious of MBLs produc-tion from the isolates. The detecproduc-tion of carbapenemase and MBLs type among the isolates from the hospitals is danger-ous for hospitals that lack information of their existence talk less of their detection and if result in nosocomial outbreaks can be disastrous to the hospital and the community at large. Carbapenem resistance in non carbapenemase producing strains as observed may be as a result of modifications in outer membrane proteins (Clark, 1996) or penicil-lin-binding proteins (Fernandoet al., 2009).
Mechanisms of resistance tob-lactam by producing ESBL, AmpC and carbapenemase were also noticed as some of the isolates produce different combinations of the enzymes. Similar co-production of enzymes have been re-ported by different researchers. For instance, Sinhaet al. (2008) reported 8% co-existence inE. coli. A prevalence of 1.25% (1/80) was demonstrated by Mathur et al. (2002) amongE. coliin India. These co-productions among some isolates as observed in this study is indicative of the exis-tence of multi-drug resistant bacteria pathogens which may be responsible for treatment failure and/or outbreaks of in-fections caused by resistant organisms. Longer hospital stays as often observed in the hospitals and resulting higher treatment costs as well as disease complications are other likely consequences of these co-productions of enzymes. Interestingly, 4 of theE. coliand 2 of theP. aeruginosaof totally resistant isolates were found to produce all the three enzymes. However, 2 out of the remainingE. coliproduced AmpC and carbapenemase together and 1K. pneumoniae produces ESBL and carbapenemase after repeated experi-ment. This may result in their associated resistance to aminoglycosides and trimethoprin sulfamethotazole, as well as high frequency of fluroquinolone resistance because many bacteria carrying genes for AmpC, ESBL or carbapenemase production on their plasmids may also carry genes responsible for resistance to other nonb-lactam anti-biotics (Mathuret al., 2002).
Conclusion
From the findings of the study the following conclu-sions were drawn:
• Antibiotic resistance among isolates from the two hospitals increases at an alarming.
• Resistance to cephamycins, carbapenems are on in-crease despite their low availability and low prescriptions.
• Carbapenemase, AmpC and Extended spectrum
b-lactamases are believe to be major cause ofb-lactam re-sistance in the two hospitals
• Co-production of two or more of the enzymes oc-curred among some of the isolates raising fears of resistance to a multitude of antibiotics in the treatment of clinical in-fections.
Acknowledgments
We are indebted to Dr Nasiru Magaji of the Microbi-ology Department, Aminu Kano Teaching Hospital, Kano-Nigeria for providing the control strain and logistics for the smooth conduct of the research. We also wish to thank University research Grant Committee, Bayero Uni-versity, Kano-Nigeria for providing the fund.
References
Aibinu I, Odugbemi P, Brian JM (2003) Extended-spectrum
b-lactamases in isolates ofKlebsiellaspp andEscherichia colifrom Lagos. Nig J Health Biomed Sci 2:53-60. Akujobi CN, Ewuru CP (2010) Detection of extended spectrum
b-lactamases in Gram negative bacilli from clinical speci-mens in a teaching hospital in South eastern Nigeria. Niger Med J 51:141-146.
Anderson KF, Lonsway DR, Rasheed JK, Biddle J, Jensen B, McDougal LK (2007) Evaluation of methods to identify the
Klebsiella pneumoniae carbapenemase in
Enterobacteriaceae. J Clin Microbiol 45:2723-2725. Arakawa Y, Shibata N, Shibayama K, Kurokawa H, Yagi T,
Fujiwara H (2000) Convenient test for screening metallo-b-lactamase-producing gram-negative bacteria by using thiol compounds. J Clin Microbiol 38:40-43. Black JA, Moland ES, Thomson KC (2005) AmpC disk test for
detection of plasmid-mediated AmpC b-lactamases in Enterobacteriaceae lacking chromosomal AmpC
b-lactamases. J Clin Microbiol 43:3110-3113.
Bush K, Jacoby GA, Medeiros AA (1995) A functional classifi-cation scheme forb-lactamases and its correlation with mo-lecular structure. Antimicrob Agents Chemother 39:1211-1233.
Clark RB (1996) Imipenem resistance among Acinetobacter baumannii: Association with reduced expression of a 33-36 kDa outer membrane protein. Journal of Antimicrobial Chemotherapy 38:245-251.
Clinical Laboratory Standards Institute (CLSI) (2005) Perfor-mance standards for antimicrobial disk susceptibility test. 8th ed. Approved standards, M2-A8, Wayne, Pa, USA. Emery CL, Weymouth LA (1997) Detection and clinical
signifi-cance of extended-spectrumb-lactamases in a tertiary-care medical center" J Clin Microbiol 35:2061-2067.
Eyitayo O, Adenipekun I, Aibinu E, Oluwole D, Afolabi A, Aderemi T (2009) Occurrence ofb-lactamase resistance among isolates from cancer patients in Lagos, Nigeria. Aca-demia Arena 1(5):1553-992.
Fernando P, Tania M, Leonor G, Melina R, Alejandra C (2009) Sensitive Screening Tests for Suspected Class A Carba-penemase Production in Species of Enterobacteriaceae. J Clin Microbiol 47(6):1631-1639.
Kenneth ST (2010) Extended-Spectrum-b-Lactamase, AmpC, and Carbapenemase issues. J Clin Microbiol 48(4):1019-1025.
Lee K, Lim YS, Yong D, Yum JH, Chong Y (2003) Evaluation of the Hodge test and the imipenem-EDTA double-disk syn-ergy test for differentiating metallo-beta-lactamase-producing isolates ofPseudomonas spp. andAcinetobacter
spp. J Clin Microbiol 41:4623-4629.
Livermore DM, Woodford N (2000) Carbapenemases a problem in waiting? Current Opinion in Microbiology 3 (5):489-495. Mathur P, Kapil A, Das B, Dhawan B (2002) Prevalence of ESBL
producing Gram negative bacteria in a tertiary care hospital. India J Med Res 115:153-157.
Naumorskil L, Palzkill T (1999) Outbreak of ceftazidime resis-tance due to moral extended spectrumb-lactamases in iso-lates from cancer patients. Antimicrob agents chemother 36(4):91-95.
Paterson DL, WC KO, Goossens H (2004) Antibiotic therapy for
Klebsiella pneumoniaebacteremia. Implication of produc-tion of Extended spectrumb- Lactamases. J Clin Microbiol 39(5):50-57.
Queenan AM, Bush K (2007). Carbapenemases: The versatile beta-lactamases. Clin Microbiol Rev 20:440-458.
Sanders WE, Tenney JH, Kessler RE (1996) Efficacy of cefepime in the treatment of infections due to multiply resistant
Enterobacterspecies. Clin Infect Dis 23:454-461.
Singhal S, Mathur T, Khan S, Upadhyay DJ, Chugh S, Gaind R (2005) Evaluation of Methods for AmpCb-Lactamase in Gram Negative Clinical Isolates from Tertiary Care Hospi-tals. Indian J Med Microbiol 23:120-124.
Sinha P, Rajni S, Suman R, Raman S, Smita S, Deepali P (2008) Prevalence of extended spectrumb- lactamase and AmpCb -lactamase producers amongE. coliisolates in a tertiary care
hospital in jaipur. Indian J of pathol and Microbiol 51(3):367-369.
Stéphane C, Nathalie C, Eric E, Cécile G, Henri D, Alain R (2003) AmpC cephalosporinase hyperproduction inAcinetobacter baumannii clinical strains. J Antimicrob Chemother 52(4):629-635.
Walsh TR, Toleman MA, Poirel L, Nordmann P (2005) Metallo-beta-lactamases: The quiet before the storm? Clin Microbiol Rev 18:306-325.
Winokur PL, Brueggemann-Desalvo DL (2005) Animal and hu-man multidrug-resistant cephalosporin-resistant Salmonella isolates expressing a plasmid-mediated CMY-2, AMP-C
b-lactamases. Antimicrob Agents Chemother 44:2777-2783.
Yusha’u M, Olonitola SO, Aliyu BS (2007) Prevalence of Ex-tended-Spectrum b- lactamases (ESBLs) among members of the Enterobacteriaceae isolates obtained from Moham-med Abdullahi Wase Specialist Hospital, Kano, Nigeria. Internl J Pure and App Sci 1(3):42-48.
Yusuf I, Arzai AH, Umar A, Magaji N, Salisu N, Tukur A, Hamid KM, Haruna M (2011) Prevalence of Extended Spectrumb -Lactamases (ESBL) producing Escherichia coli and
Klebsiella pneumoniaein Tuberculosis patients in Kano, Ni-geria. Bayero J of Pure App Sci 4(2):182-185.