SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Review
Article
Hand
and
wrist
surgery
without
suspending
warfarin
or
oral
antiplatelet
–
systematic
review
夽
Trajano
Sardenberg
∗,
Francisco
Simões
Deienno,
Raffaello
de
Freitas
Miranda,
Denis
Varanda,
Andréa
Christina
Cortopassi,
Paulo
Roberto
de
Almeida
Silvares
UniversidadeEstadualPaulista(Unesp),FaculdadedeMedicinadeBotucatu,Botucatu,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received10May2016 Accepted19May2016 Availableonline14July2017
Keywords: Hand/surgery Anticoagulants Warfarin
a
b
s
t
r
a
c
t
Toassess,throughasystematicliteraturereview,whetherornotitisnecessarytosuspend antithromboticmedications(warfarin,aspirin,andclopidogrel)toperformelectivewrist andhandsurgeries.Thesearchforarticleswasperformedusingacombinationofkeywords inthedatabasesavailable,withoutscientificdesignconstraints,beingselectedserieswith fiveormoresurgeries;theselectedarticleswereanalyzedregardingserious(needfor surgi-caltreatment)andmildcomplications(withoutsurgery).Sevenarticleswereretrievedand analyzed;410wristandhandsurgerieswereperformedinpatientsonwarfarinoraspirin andclopidogrel,withthreeseriouscomplications(0.7%)and38mild(9.2%);2023surgeries wereperformedinpatientswithoutuseofantithrombotics,withzeroseriousand18(0.8%) minorcomplications.Patientsusingwarfarinororalantiplatelet(aspirin,clopidogrel,and aspirinassociatedwithclopidogrel)neednotsuspendthemedicationtoundergowristand handsurgery.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Cirurgia
da
mão
e
do
punho
sem
suspender
varfarina
ou
antiplaquetários
orais
–
Revisão
sistemática
Palavras-chave: Mão/cirurgia Anticoagulantes Varfarina
r
e
s
u
m
o
Avaliar,pormeioderevisãosistemáticadaliteratura,seháounãonecessidadedesuspender medicamentosantitrombóticos(varfarina,AASeclopidogrel)paraarealizac¸ãode proced-imentoseletivosdecirurgiadopunhoedamão.Abuscadeartigosfoifeitapormeioda combinac¸ãodepalavras-chavenasbasesdedadosdisponíveis,semrestric¸õesdedesenho científico,sendoselecionadassériescomcincooumaiscirurgias;osartigosselecionados foramanalisadosemrelac¸ãoàscomplicac¸õesgraves(necessidadedetratamentocirúrgico)
夽
StudyconductedatUniversidadeEstadualPaulista(Unesp),FaculdadedeMedicinadeBotucatu,Botucatu,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](T.Sardenberg).
http://dx.doi.org/10.1016/j.rboe.2017.07.001
rev bras ortop.2017;52(4):390–395
391
eleves(semnecessidadedetratamentocirúrgico).Seteartigosforamencontradose anal-isados;410cirurgiasdopunhoedamãoforamfeitasempacientesemusodevarfarinaou AASeclopidogreleobservoutrêscomplicac¸õesgraves(0,7%)e38leves(9,2%);2.023cirurgias foramfeitasempacientessemusodosantitrombóticos,apresentaramzerocomplicac¸ões gravese18leves(0,8%).Pacientesemusodevarfarinaouantiplaquetáriosorais(AAS, clo-pidogreleAASassociadoaclopidogrel)nãonecessitamsuspenderamedicac¸ãoparaser submetidosacirurgiasdopunhoedamão.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The indication of continuous use of oral antithrombotic drugsforthetreatmentorpreventionofcardiovascularand cerebrovasculardiseaseshasincreasedinrecentdecades.1,2 Antithromboticdrugsaredistributedintwogroups: anticoag-ulants,warfarinbeingthemostused,andantiplatelets,with acetylsalicylicacid(ASA)andclopidogrelaloneorin combina-tion,commonlyusedinthepreventionofthromboticdiseases. Theadjustment ofwarfarin dosageto keep the patient in an anticoagulated state, prevent thrombotic diseases, and avoidcausingserious bleedingisacomplextreatmentthat requires control through regular International Normalized Ratio(INR)testing;warfarin suspensionandreintroduction areevenmoredifficult,andmayleadtothedevelopmentof newthromboticeventsorhyperanticoagulationwithbleeding risk.Suspensionandreintroductionoforalantiplateletagents (ASAandclopidogrel)alsopresentahighriskofthrombotic diseases,aswellasofthrombosisorbleeding.3–6
Patients takingantithrombotic medications that require surgeryputphysiciansinadilemma:stoppingantithrombotic medicationtoavoidexcessivebleeding,butincreasingtherisk ofthromboembolic disease, or maintaining the antithrom-boticmedicationtopreventthromboembolism,butincreasing theriskofbleeding.Clinicalexperiencesand meta-analysis studiesindicatetwogroupsofsituations:surgeriesand inva-siveprocedureswithalowriskofbleeding(e.g.,endoscopy, cataractsurgery,arthrocentesis,and dermatological surger-ies)donotrequirediscontinuationofantithrombotictherapy, andsurgerieswithincreasedriskofbleedingrequirethe sus-pensionoforalantithromboticmedicationand,dependingon theriskofthrombosis,atransitionperiodwithheparin.4,7,8 Thepresentstudyaimedtoassesswhetheritisnecessaryto suspendantithromboticdrugs(warfarin,aspirin,and clopid-ogrel)forelectivesurgicalproceduresofthewristandhand, throughasystematicreview.
Material
and
methods
The search strategy for the databases used the terms hand surgery and anticoagulant or anticoagulants or indi-rectthrombininhibitorsorplateletaggregationinhibitorsor blood platelet antiaggregants or platelet antiaggregants or bloodplateletaggregationinhibitorsorplateletinhibitorsor antiplateletagentsorantiplateletdrugsorplateletantagonists
or blood platelet antagonists or warfarin or clopidogrel or ticlopidineoraspirinoracetylsalicylicacid.Thestrategywas adapted to search in MEDLINE (PubMed), Embase, Scopus, LILACS, SciELO, and Cochrane Library (Reviews and Trials) databases.
Therewasnoperiodlimitationforthestudy;thesearches werecarriedoutuntilDecember2015.
Articlesthatdirectlyaddressedthestudytopic,i.e.,wrist andhandsurgeryandtheuseorsuspensionofanticoagulants orantiplateletagents,wereselectedthroughtheanalysisof theirtitlesand,whennecessary,abstractsretrievedthrough thesearchstrategiesindatabases.
Therewere norestrictionsregardingstudy design. How-ever, only articles with samplesize (patients or surgeries) equaltoorgreaterthanfivepatientsoperatedonusing war-farinorantiplateletdrugs(ASAandclopidogrel)wereselected. Thebibliographicreferencesoftheselectedarticleswere analyzedinsearchofotherstudiesthatmaynothavebeen previouslyretrieved.
The articles were analyzed and the following charac-teristics were recorded: sample size (number of surgeries or patients); type of surgery; use of tourniquet; type of antithromboticmedication(warfarin,antiplateletassociated withwarfarin,ASA,clopidogrel,orASAassociatedwith clo-pidogrel);andnumberandseverityofcomplications.
Thecomplicationsassessedwerethosedirectlyrelatedto theeffectsofwarfarinandantiplateletagents(clopidogreland ASA)onbloodcoagulationduringsurgeryanduptotwoweeks postoperatively:excessive bleedingandbruising. Complica-tionsthatweretreatedonlywithconservativemethodswere consideredasmild;thosethatrequiredreoperationwere con-sideredassevere.
Results
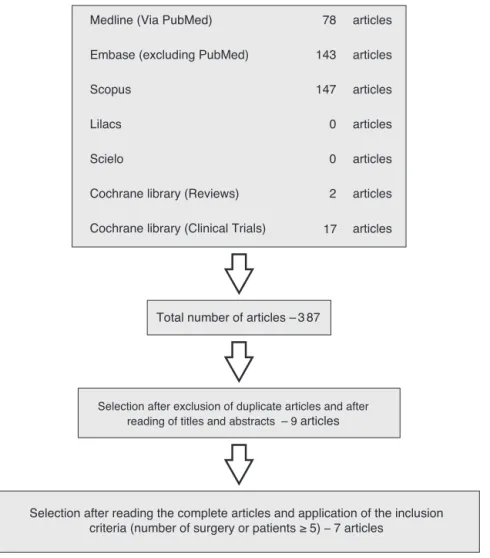
A total of 387 articles were selected. After analyzing the titlesandabstractsandexcludingduplicatestudies,nine arti-cles were selected. Afterreading their full texts, twowere excluded,asthesamplesizewaslessthanfivesurgeriesor patients. Theanalysisofthereferencesofthe ninearticles didnotretrieveanynewpapers.Thefinalnumberofarticles includedforanalysiswasseven(Fig.1).
articles 78
Medline (Via PubMed)
articles 143
Embase (excluding PubMed)
articles 147
Scopus
Lilacs 0 articles
Scielo 0 articles
Cochrane library (Reviews) articles
articles 2
17 Cochrane library (Clinical Trials)
Total number of articles – 3 87
Selection after exclusion of duplicate articles and after reading of titles and abstracts – 9 articles
Selection after reading the complete articles and application of the inclusion criteria (number of surgery or patients ≥ 5) – 7 articles
Fig.1–Studiesretrievedonhandandwristsurgeryinpatientsusingantithromboticdrugs(warfarin,aspirin,and
clopidogrel).
tunnelsyndrome[CTS]and 527forDupuytrencontracture); 22inuseofwarfarininpatientswithINR<3(nineforCTSand 13forDupuytrencontracture);andoneinuseofclopidogrel (Dupuytren contracture). The patient in use of clopidogrel whounderwentsurgeryforDupuytrencontracturepresented excessivebleedingtreatedconservatively,thuscharacterized asamildcomplication.Allotherpatientsoperatedon(1370 withoutantithromboticmedicationand22withwarfarin)did notpresentexcessivebleedingorbruisingcomplications.
Wallaceetal.10conductedanon-controlledclinical retro-spectiveseries.Allsurgerieswereperformedwiththeuseof atourniquet.Thesample(surgeries)included:55patientsin useofwarfarin(INRbetween1.3and2.9;17forCTS,12for Dupuytren contracture,five fortriggerfinger,and 21 other surgeries).Twopatients(oneoperatedforCTSandonewho underwentatrapeziectomy)developedhematoma,whichwas conservativelytreated,thusindicatingamildcomplication.
Jivanetal.11conductedaretrospectivecase-controlstudy. Thepatientswereoperatedwiththeuseofatourniquet.All patientsunderwent surgeryforCTS, 48 withoutthe use of antithromboticmedicationand48usingASA.Nobleedingor bruisingcomplicationswereobservedinbothgroups.
Edmunds and Avakian12 conducted a non-controlled, prospectiveclinicalseries.Thepatientswereoperatedwith
the use of a tourniquet. The sample (surgeries) consisted of57 patientsusingwarfarin (INRbetween1.4and 3.2),40 using clopidogrel, and 24 using clopidogrel and ASA. The surgeries performed were: 59 for CTS, 12 for Dupuytren contracture, five for trigger finger, and 45 other surgeries. Six patients (five using clopidogreland oneusing clopido-grel and ASA) presented excessive bleeding conservatively treated,thuscharacterizingamildcomplication;onepatient onclopidogrelwithadiagnosisofVaughan-Jacksonsyndrome, who underwent resection of the distal ulna, tenosynovec-tomy, and tendon transfer, presented a hematoma that required surgical treatment, thus characterizing a severe complication.
rev bras ortop.2017;52(4):390–395
393
Bogunovicet al.5 conducted aprospective cohort study. The patients were operated with the use of a tourniquet. Thesample(surgeries)included107patientswhodidnotuse antithromboticmedication(39forCTS,23fortriggerfinger, and45forothersurgeries)and107operatedonwhileusing antiplateletmedication(48forCTS,21fortriggerfingerand 38forothersurgeries).Amongthepatientsusingantiplatelet agents,76usedASA,fiveusedclopidogrel,and11used clo-pidogreland ASA.Noserious complicationswere observed inpatientswhodidnotuseantiplateletmedication.Oneof thepatientsusingantiplateletmedication presentedsevere bleedingrequiringreoperation(thepatienthadrheumatoid arthritisandwasusingahighdoseofASA,andunderwent arthrodesis of the wrist and tenosynovectomy). The rates of conservatively treated bruisings (which did not require surgeryandwerecharacterizedasmildcomplications)were 14% for patients who did not use medication and 17% in thosewhousedantiplateletagents;this differencewasnot statistically significant. No infection or dehiscence of sur-gical wound was observed in the group of patients using antiplateletagents.Theecchymosis size,digitalsensitivity, andQuick-Dashpresentedstatisticallysimilarresultsin oper-atedpatientsusingantiplateletagentsvs.thosewhowerenot. Bogunovicet al.6 conducted another prospectivecohort studyonthisissue,thistimeaddressingwarfarin.Thesample included50surgeriesinpatientsusingwarfarinalone(32)or associatedwithASA(18;27forCTS,twofortriggerfinger,five formassorsynovialcystsresection,fourfortendonsurgeries, and12forbonesurgeries)and50surgeriesinpatientswhodid notuseantithromboticmedication(21forCTS,eightfortrigger finger,threetendonsurgeries,threefordeQuervain tenosyn-ovitis,onewristarthroscopy,threesofttissuesurgeries,and11 bonesurgeries).ThemeanINRinpatientsusingwarfarinwas 2.3.Allsurgeriesweremadewiththeuseofatourniquetand localanestheticwasinjectedwithoutepinephrineatthe sur-gicalsite.Noseriouscomplicationswereobservedinpatients whodidnotuseantithromboticmedication.Inpatientsusing warfarin,oneseriouscomplicationrequiringanewsurgical interventionwasobserved(patientsubmittedtocarpectomy ofthefirstrowwhodevelopedhematomaandcompression ofthemediannervefourdaysaftersurgery).Regardingmild complicationsthatdidnotrequirehospitalizationor reope-ration, patients using warfarin had a higher incidence of bruisingsonlyattwoweekspostoperatively,whichpairedwith thegroupthatdidnotuseantithromboticmedicationatfour weeks.Therewerenorelevantclinicaldifferencesbetweenthe groupsregardingpain,edema,andupperlimbdysfunction.
Tables1and2presentsummariesoftheresultsfromthe sevenarticlesincluded.
The indicationfor the use ofwarfarin and antiplatelet agents in the seven studies analyzed were atrial fib-rillation, cardiomyopathy, mitral valve prosthesis, coarc-tation of the aorta, venous thromboembolism, valvular prosthesis, atrioventricular communication, primary pre-vention of coronary disease, secondary prevention of coronary disease,combined secondary prevention of coro-naryand cerebrovascular diseases, pulmonary thrombosis, deepvenousthrombosis,thromboticdisorders, cardiovascu-lardisease,peripheral vascular disease,and neurovascular disease.
Discussion
The analysis of the results of the seven selected studies addressed handand wrist surgeries inpatients using war-farinororalantiplateletagents(ASAandclopidogrel)indicates thatthefrequencyofseverecomplications,definedas bleed-ing orbruisingrequiringsurgicaltreatment, wasextremely low – three in410 (0.7%). Thethree serious complications occurredinpatientsundergoingcomplexsurgicalwrist pro-cedures(wristarthrodesisassociatedwithtenosynovectomy; resectionofthedistalulnaassociatedwithtenosynovectomy andtendontransfer;andfirst-rowcarpectomy);onepatient used high-dose ASA, one used clopidogrel, and one used warfarin.5,6,12Bogunovicetal.5emphasizethesimilarityofthe situationofpatientsusingantiplateletagents,inwhich seri-ouscomplicationswereobservedinthosewithrheumatoid arthritisundergoingboneprocedures.Inthe184surgeries per-formedonpatientsusingwarfarin,oneseriouscomplication wasobserved.6
Mild complications,definedas bleedingorbruising that did not require surgical treatment, occurred in 35 out of 410 surgeries (8.5%). Theprospective studies byBogunovic etal.5,6 includingacontrolgroup(patientswhodidnotuse antiplateletagentsorwarfarin)presentedthelargestamount ofmildcomplications,buttheauthorsadoptedabroad def-inition ofthe term hematoma (“any bulging withpalpable fluidcollection,regardlessofsize”)EdmundsandAvakian12 reportedsixminorcomplicationsinpatientsusing clopido-grelandASA,subjectivelydefinedas“excessiveintraoperative bleeding.”Stoneet al.14analyzedthe resultsofover10,000 patientsundergoingmajorarterialsurgeryinuseof clopid-ogrel alone or in combination with ASA, and did not find evidenceofexcessiveintraoperativebleeding.
The four studies reporting surgery in patients using warfarin6,9,10,12adoptedINRequaltoorlessthanthreeasa parametertoperformthesurgerywithoutsuspending anti-coagulant; apparently, the selection of the INR value was determined subjectively. The four studies showed an INR variationfrom1.3to3.2.Wallaceetal.10reportedtwomild complications,andtheINRrangedfrom1.3to2.9.Thestudy byBogunovietal.6presentedacasewithseriouscomplication inwhichtheINRwas2.1preoperativelyand5.4onthefourth dayaftertheoperation,whenthecomplicationwasdetected. AlthoughtheINRparameteroflessthanorequalto3or3.5is subjective,theobservedresultssuggestthatthislimitissafe. Thesevenstudiesanalyzedhadlowlevelsofevidence,as onlythreewereprospectivestudiespresentingbetter detail-ingandcareindesignandexecution;thesestudiesreported morecasesofmildandseverecomplications,probablydueto thefactthatthedefinitionsofthecomplicationsweremore precise.5,6,12
r
e
v
b
r
a
s
o
r
t
o
p
.
2
0
1
7;
5
2(4)
:390–395
Table1–Characteristicsandsummaryofresultsofthesevenarticles.
Authors Typeofstudy Tourniquetuse AT Numberofsurgeries Mildcomplications Severecomplications Totalcomplications
WithAT WithoutAT WithAT WithoutAT WithAT WithoutAT
Smitand Hooper9
(2004)
Cohortstudy (retrospec-tive)
Yes Warfarin
(INR≤3)and
clopidogrel
23(22with warfarinand 1with clopidogrel)
1.370 1 (Bleed-ing/clopidogrel)
Zero Zero Zero 1(4.3%)(WithAT)
Wallace etal.10(2004)
Non-controlled clinicalseries (retrospec-tive)
Yes Warfarin(INR 1.3–2.9)
55 Doesnot
refer
2(hematoma) Doesnot refer
Zero Zero 2(3.6%)(WithAT)
Jivanetal.11
(2008)
Case-control studies (ret-rospective)
Yes ASA 48 48 Zero Zero Zero Zero Zero(withand
withoutAT)
Edmundsand Avakian12
(2010)
Non-controlled clinicalseries (prospective)
Yes Warfarin(INR 1.4–3.2) clopidogrel and
ASA+clopidogrel 121(57 warfarin,40 with clopidogrel, and24with clopido-grel+ASA)
Doesnot refer
6(bleeding;5 clopidogrel and1with ASA+clopidogrel)
Doesnot refer
1(hematoma/ clopidogrel)
Zero 7(5.8%)(WithAT)
Boogaarts etal.13(2010)
Cohortstudy (retrospec-tive)
No(local anesthesia with epinephrine)
ASA 6 448 Zero Zero Zero Zero Zero(withand
withoutAT)
Bogunovic etal.5(2013)
Cohortstudy (prospective)
Yes clopidogrel, ASA,and ASA+clopidogrel
107 107 15
(hematoma) 13
(hematoma)
1 (bleed-ing/highdose ofASA)
Zero 16(15%)withAT 13(12.1%) withoutAT Bogunovic
etal.6(2015)
Cohortstudy (prospective)
Yes Warfarin
(meanINR 2.3);18 war-farin+ASA
50(32 warfarinand 18with war-farin+ASA)
50 14
(hematoma)
5(hematoma) 1
(hematoma+ mediannerve compression)
Zero 15(30%)withAT 5(10%)without AT
Total 410 2023 38(9.2%) 18(0.8%) 3(0.7%) Zero 41(10%)withAT
18(0.8%)without AT
rev bras ortop.2017;52(4):390–395
395
Table2–Summaryandaggregationoftheresultsofthe
sevenarticles.
Surgeriesusingwarfarin,warfarin+ASA,orantiplateletagents (AAS;clopidogrel;AAS+clopidogrel):410
Mildcomplications:38(9.2%) Severecomplications:three(0.7%)
Surgeriesusingwarfarin:184 Mildcomplications:16(8.6%) Severecomplications:one(0.5%)
Surgeriesusingantiplateletagents(AAS;clopidogrel; AAS+clopidogrel):226
Mildcomplications:22(9.7%) Severecomplications:two(0.9%)
Surgerieswithouttheuseofantithrombotics(warfarin, warfarin+ASA,ASA,clopidogrel,ASA+clopidogrel):2023 Mildcomplications:18(0.8%)
Severecomplications:zero
physiciansshouldbeextremelycautiousbeforesuspending
theuseofthesemedications.2–4,7
Theidealstudy,whichwasnotretrievedintheliterature, would prospectively compare the results ofpatients using antithromboticdrugswiththoseofpatientswhohadtheuse ofthesedrugssuspended.
Thelimitationsof thepresent study,due inpart tothe methodological restrictions ofthe articles selected, hinder moreemphaticconclusionsregardingthe needtosuspend antithromboticdrugsforwristandhandsurgeries.However, thestudiesanalyzedsuggestthatwristand handsurgeries withlowriskofbleeding,involvingsoftparts,fingerjoints,and tubularbones,canbeperformedwithoutsuspendingwarfarin orantiplateletagents(ASAandclopidogrel).Furthermore,the studiessuggestthefollowingpracticesinthesurgical man-agement of patients taking antithrombotic drugs: in order nottodiscontinue warfarin,patients should haveINR less thanorequaltothreeontheeveofsurgery,andpatientson antiplateletagents(ASAandclopidogrel)maypresentgreater intraoperativebleedingandrequiregreaterhemostasiscare.
Morerandomizedandcontrolledstudies,especiallywith groupswithandwithoutantithromboticsuspension,are nec-essarytoelucidatethistheme.Moreover,theintroductionof antithrombotictreatmentwithanticoagulantandantiplatelet association,aswellastheadventofnewanticoagulants,also requiresnewstudiesonwristandhandsurgerywithoutthe suspensionofthesedrugs.16,17
Final
considerations
Patientstakingwarfarinororalantiplateletagents(ASA, clo-pidogrel,andASAassociatedwithclopidogrel)donotneedto discontinuethemedicationtoundergohandandwrist surger-ies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TothelibrarianEnilzedeSouzaNogueiraVolpatoforthehelp onthearticlessearchandreferencescitation.
r
e
f
e
r
e
n
c
e
s
1.PignoneM,AndersonGK,BinnsK,TilsonHH,WeismanSM. Aspirinuseamongadultsaged40andolderintheUnited States:resultsofnationalsurvey.AmJPrevMed. 2007;32(5):403–7.
2.KeelingD,BaglinT,TaitC,WatsonH,PerryD,BaglinC,etal. Guidelinesonoralanticoagulationwithwafarin:fourth edition.BrJHaematol.2011;154(3):311–24.
3.DunnAS,TupierAG.Perioperativemanagementofpatients receivingoralanticoagulants:systematicreview.ArchIntern Med.2003;163(8):901–8.
4.LindsleyRC.Perioperativemanagementofsystemicoral anticoagulantsinpatientshavingoutpatienthandsurgery.J HandSurgAm.2008;33(7):1205–7.
5.BogunovicL,GelbermanRH,GoldfarbCA,BoyerMI,CalfeeRP. Theimpactofantiplateletmedicationonhandandwrist surgery.JHandSurg.2013;38(6):1063–70.
6.BogunovicL,GelbermanRH,GoldfarbCA,BoyerMI,CalfeeRP. Theimpactofuninterruptedwarfarinonhandandwrist surgery.JHandSurg.2015;40(11):2133–40.
7.JafferAK,BrotmanDJ,ChukwumerijeN.Whenpatientson warfarinneedsurgery.CleveClinJMed.2003;70(11): 973–84.
8.JamulaE,AndersonJ,DouketisJD.Safetyofcontinuing warfarintherapyduringcataractsurgery:asystematicreview andmeta-analysis.ThrombRes.2009;124(3):292–9.
9.SmitA,HooperG.Electivehandsurgeryinpatienttaking warfarin.JHandSurgBr.2004;29(3):204–5.
10.WallaceDL,LatimerMD,BelcherHJ.Stoppingwarfarinis unnecessaryforhandsurgery.JHandSurgBr.
2004;29(3):201–3.
11.JivanS,SouthernS,MajumberS.Re:theeffectsofaspirinin patientsundergoingcarpaltunneldecompression.JHand SurgEur.2008;33(6):813–4.
12.EdmundsI,AvakianZ.Handsurgeryonanticoagulated patients:aprospectivestudyof121operations.HandSurg. 2010;15(2):109–13.
13.BoogaartsHD,VerbeekAL,BartelsRH.Surgeryforcarpal tunnelsyndromeunderantiplatelettherapy.ClinNeurol Neurosurg.2010;112(9):791–3.
14.StoneDH,GoodneyPP,ShanzerA,NolanBW,AdansJE,Powell RJ,etal.Clopidogrelinnotassociatedwithmajorbleeding complicationsduringperipheralarterialsurgery.JVascSurg. 2011;54(3):779–84.
15.BellCM,BajcarJ,BiermanAS,LiP,MandaniMM,UrbachDR. Potentiallyunintendeddiscontinuationoflong-term
medicationuseafterelectivesurgicalprocedures.ArchIntern Med.2006;166(22):2525–31.
16.PaikinJS,WrightDS,EikelboomJW.Effectivenessandsafety ofcombinedantiplateletandanticoagulanttherapy:acritical reviewoftheevidencefromrandomizedcontrolledtrials. BloodRev.2011;25(3):123–9.