www.jped.com.br
ORIGINAL
ARTICLE
Prenatal,
perinatal
and
postnatal
factors
associated
with
autism
spectrum
disorder
夽
Imen
Hadjkacem
a,∗,
Héla
Ayadi
a,
Mariem
Turki
a,
Sourour
Yaich
b,
Khaoula
Khemekhem
a,
Adel
Walha
a,
Leila
Cherif
a,
Yousr
Moalla
a,
Farhat
Ghribi
aaUniversityofSfax,HédiChakerHospital,DepartmentofChildandAdolescentPsychiatry,Sfax,Tunisia
bUniversityofSfax,HédiChakerHospital,DepartmentofCommunityMedecineandEpidemiology,Sfax,Tunisia
Received19September2015;accepted27January2016 Availableonline12August2016
KEYWORDS Autismspectrum disorder; Child; Riskfactors; Prenatal; Perinatal; Postnatal
Abstract
Objective: Toidentifyprenatal,perinatalandpostnatalrisk factorsinchildren withautism spectrumdisorder(ASD)bycomparingthemtotheirsiblingswithoutautisticdisorders.
Method: Thepresentstudyiscrosssectionalandcomparative.Itwasconductedoveraperiod ofthreemonths(July---September2014).Itincluded101children:50ASD’schildrendiagnosed accordingtoDSM-5criteriaand51unaffectedsiblings.TheseverityofASDwasassessedbythe CARS.
Results: Ourstudyrevealedahigherprevalenceofprenatal,perinatalandpostnatalfactorsin childrenwithASDincomparisonwithunaffectedsiblings.Itshowedalsoasignificant associa-tionbetweenperinatalandpostnatalfactorsandASD(respectivelyp=0.03andp=0.042).In thisgroup,perinatalfactorsweremainlyastypeofsufferingacutefetal(26%ofcases),long durationofdeliveryandprematurity(18%ofcasesfor eachfactor),whilepostnatalfactors wererepresentedprincipallybyrespiratoryinfections(24%).Asforparentalfactors,no corre-lationwasfoundbetweenadvancedageofparentsatthemomentoftheconceptionandASD. Likewise,nocorrelationwasobservedbetweentheseverityofASDanddifferentfactors.After logisticregression,theriskfactorsretainedforautisminthefinalmodelwere:malegender, prenatalurinarytractinfection,acutefetaldistress,difficultlaborandrespiratoryinfection.
Conclusions: Thepresentsurveyconfirmsthehighprevalenceofprenatal,perinataland post-natalfactorsinchildrenwithASDandsuggeststheinterventionofsomeofthesefactors(acute fetal distressanddifficultlabor, amongothers),asdeterminantvariablesfor thegenesisof ASD.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:HadjkacemI,AyadiH,TurkiM,YaichS,KhemekhemK,WalhaA,etal.Prenatal,perinatalandpostnatalfactors associatedwithautismspectrumdisorder.JPediatr(RioJ).2016;92:595---601.
∗Correspondingauthor.
E-mail:[email protected](I.Hadjkacem). http://dx.doi.org/10.1016/j.jped.2016.01.012
PALAVRAS-CHAVE Transtornodo espectrodoautismo; Crianc¸a;
Fatoresderisco; Pré-natal; Perinatal; Pós-natal
Fatorespré-natais,perinataisepós-nataisassociadosaotranstornodoespectro doautismo
Resumo
Objetivo: Identificar fatores de risco pré-natal, perinatal e pós-natal em crianc¸as com transtornodoespectrodoautismo(TEA)aocompará-lasairmãossemtranstornosdeautismo.
Método: Esteestudoétransversal ecomparativo.Ele foiconduzidoem umperíodo detrês meses(julhoasetembrode2014).Incluiu101crianc¸as:50crianc¸ascomTEAsdiagnosticadas deacordocomoscritériosdoDSM-5e51irmãosnãoafetados.AgravidadedoTEAfoiavaliada pelaEscaladeAvaliac¸ãodoAutismonaInfância(CARS).
Resultados: Nossoestudorevelouumaprevalênciamaiordefatorespré-natais,perinataise pós-nataisemcrianc¸ascomTEAemcomparac¸ãoairmãosnãoafetados.Tambémmostrouuma associac¸ãosignificativaentrefatoresperinataisepós-nataiseTEA(respectivamentep=0,03 ep=0,042).Nessegrupo,osfatoresperinataisforamprincipalmentedotiposofrimentofetal agudo(26%doscasos),longadurac¸ãodopartoeprematuridade(18%doscasosemcadafator), aopassoquefatorespós-nataisforamrepresentadosprincipalmenteporinfecc¸õesrespiratórias (24%).Noquedizrespeitoafatoresdospais,nenhumacorrelac¸ãofoiencontradaentreaidade avanc¸adadospaisnomomentodaconcepc¸ãoeoTEA.Damesmaforma,nenhumacorrelac¸ão foiestabelecidaentreagravidadedoTEAefatoresdiferentes.
Apósregressãologística,osfatoresderiscodeautismoencontradosnomodelofinalforam: sexomasculino, infecc¸ãopré-nataldotrato urinário,sofrimento fetalagudo,partodifícile infecc¸ãorespiratória.
Conclusões: Estapesquisaconfirmaaaltaprevalênciadefatorespré-natais,perinataise pós-nataisemcrianc¸ascomTEAesugereaintervenc¸ãodealgunsdessesfatores(sofrimentofetal agudo,partodifícil...)comovariáveisdeterminantesparaagênesedoTEA.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Autismspectrum disorder (ASD) is a complex neurodevel-opmentalcondition.Basedonthe5theditionofDiagnostic StatisticalManualofMentalDisorders(DSM-5),specific diag-nosticcriteriaforchildhoodautismincludesocialskillsand communicationdeficitassociatedwithrestrictiveand repet-itivebehaviors,interests,oractivities.1ASDiscurrentlyone
of themost common childhoodmorbidities, presenting in variousdegreesofseverity.The mostrecentglobal preva-lenceofautismwasestimatedat0.62%.2
This disorder has grown into a constant challenge for manycountriessuchasTunisia,asithasasevereimpacton boththeaffectedindividualsandtheirfamilies.The finan-cialburden,whichhasbecomemoreacutesincetheTunisian revolution,alongwiththelackofscientificknowledgeabout theepidemiology,etiology,andnaturalcourseofthis condi-tion,haverenderedthesituationmorecomplex.3---5
The spectrum of symptomsand the extreme complex-ityinthedevelopmentalandassociatedmedicalconditions withinASDdonotnecessarilymeanasingleetiology. Sev-eral hypotheses concerning the pathogenesis have been proposed,including theinteraction of environmental fac-torsandvariousgeneticpredispositions.5,6Studiesbasedon
concordance rates amongmonozygotic twins and families suggesta possibleroleof bothgeneticandenvironmental factorsintheetiologyofASD.7
A recent study suggests that genetic factors account for only 35---40% of the contributing elements.8,9 The
remaining60---65% arelikelyduetoother factors, suchas
prenatal, perinatal, and postnatal environmental factors. SinceASDs areneurodevelopmentaldisorders, neonatally-observed complications that are markers of events or processesthatemergeearlyduringtheperinatalperiodmay beparticularlyimportanttoconsider.8
To thebestof our knowledge,in Tunisia, thereareno studiesthathaveconsideredtherelationshipbetween pre-natal,perinatal,andpostnatalriskfactorsandASD.
Thus,theaimofthepresentstudywastoidentifythe pre-,peri-,andpostnatalfactorsassociatedtoASDbycomparing childrenwithASDtotheirsiblingswhodonotpresent any autisticdisorders.
Methods
Study
Thiswasacrosssectionalandcomparativestudy.Itwas con-ductedoveraperiodofthreemonthsfromJulytoSeptember 2014.
Population
Participants
Thesampleincluded101childrendividedintotwogroups:
HospitalofSfax(Tunisia).Thesepatientscamefrom dif-ferentregionsof Tunisia,asthereareonlythreechild psychiatry departments in the entire country. Subject agesrangedbetween3and7years.
2. Thesecondgroupwascomposedof51non-autistic chil-dren,agedbetween3and12years.
Inclusionandexclusioncriteria
Inclusioncriteria.
- Forthefirstgroup,thestudyincludedchildrenwhoboth metthe DSM-5 criteriafor ASDand whose scoreat the ChildAutisticRatingScale(CARS)was≥30.
- For the second group, the unaffected siblings were includedascontrols.
Inbothgroups,thechildrenwereagedatleast3years. ThiscriterionforageselectionisbasedonthefactthatASD isidentifiedwithahighdegreeofcertaintyattheageof3. Exclusioncriteria. Exclusioncriteria:knownneurogenetic conditions(e.g.,tuberoussclerosis,neurofibromatosis, frag-ileXsyndrome,Downsyndrome).
Thecontrolgroupsharedthesameexclusioncriteria.
Tools
DSM-5diagnosticcriteriaforASD
InDSM-5,ASDencompassesthepreviousDSM-IVautistic dis-order(autism),Asperger’sdisorder,childhooddisintegrative disorder,and pervasivedevelopmentaldisordernot other-wisespecified.1
CARS
CARSassessestheintensityofASDsymptomatology.It evalu-atestheseverityofautisticbehaviorsin14functionalareas by assigning a score from1 to 4.An overall score is cal-culated by addingall thegrades, to stratifypatients into three levels: ‘‘severely autistic’’ (score between 37 and 60),‘‘mildlytomoderatelyautistic’’(scorebetween30and 36.5),and‘‘absenceofASD’’(scorelessthan30).10Thetime
foradministeringthisquestionnaireisaround20---30min.
Procedures
Allstudyprocedureswereapprovedby thelocalResearch EthicsCommittee.
Informalconsentfromparentsorlegalguardiansof par-ticipants wasobtained afterthenatureof theprocedures hadbeenfullyexplained.
The interviews wereconductedwithmothers in78%of the cases,withfathersin 4% of thecases, andwithboth parents in 18% of the cases, by a properly trained child psychiatrist.
Parentscompletedamedicalhistoryquestionnairewitha combinationofclosedandopen-endedquestionsregarding pregnancy,labor,andcomplicationsduringandafterbirth. Additionally,datawerecollectedwithreferencetomedical recordandmedicalbirthbook.
The studied variables were designed according to the probable risk factors of ASDfrom existingliterature. The followingvariables,whichwereconsideredforbothgroups,
wereclassified as parental factors,pre-, peri-, and post-natalcharacteristics andwerecodifiedasbinaryvariables (yes/no).
Parentalfactors:Advancedmaternalandpaternalageat
thetimeofchildbirth(≥35years),consanguinity.
Prenatalfactors:Theseconsistedofconditionsthatarose
duringpregnancy,suchasgestationaldiabetes,which usu-ally develops in the second half of pregnancy; high and lowbloodpressure;gestationalinfections;andfetaldistress inducing threatened abortion conditions, such as amni-otic fluid loss, bleeding during gestation, and suboptimal intrauterineconditions.Perinatalfactors:delivery charac-teristics,suchastermbirth(prematureorpost-termbirth); deliverytypes,includingforcepsorcesareansection;acute fetaldistress;andbirthweight(lowbirthweight[<2500g] andmacrosomia[>4000g])
Postnatalfactors:Allconditionsoccurringinthefirstsix
weeksafterbirth,suchasrespiratoryandurinaryinfections; auditorydeficit(alossof 30dB);andblood disorderssuch asanemiaandthrombopenia.
The diagnosis of respiratoryand urinaryinfections was achievedduringhospitalizationsinpediatricservices.
Statisticalanalysis
Statisticalanalysis wasdone usingSPSS softwarefor Win-dows, release 20.0 (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, version 20.0, USA). The analysis includedadescriptivestudy,observingthefrequenciesfor thequantitativevariables and meansand standard devia-tionsforthequalitativevariables,aswellasananalytical study, using Pearson’s correlation coefficient to establish correlationsbetweenthetwogroups.Thelevelofstatistical significancewassetatp<0.05(alphalevelof5%).
In the multivariable analysis, logistic regression was performed to identify risk factors for autism, taking into accountconfoundingfactorsandusingthedownmethodof Wald.
Initially, all the variables significantly associated with autismwereincludedintheunivariableanalysis,aswellas thosefoundasriskfactorsintheliterature.Thesignificance levelwassetat20%.Thefinalmodelaccuracywasverified andcalculatedaccordingtotheHosmerandLemeshowtest. Theresultswereexpressedbytheadjustedoddsratio(ORa) withtheirconfidenceintervals,95%CI(ORa).
Results
ClinicalprofileofchildrenwithASD
Thisstudyincluded 50children.Amalepredominance(37 boys and 13 girls) was observed, as well as a moderate socioeconomiclevel in90% of cases, anda predominance ofthemildtomoderate formofASDattheCARS(62%vs. 38%forthesevereform).
Parentalfactors
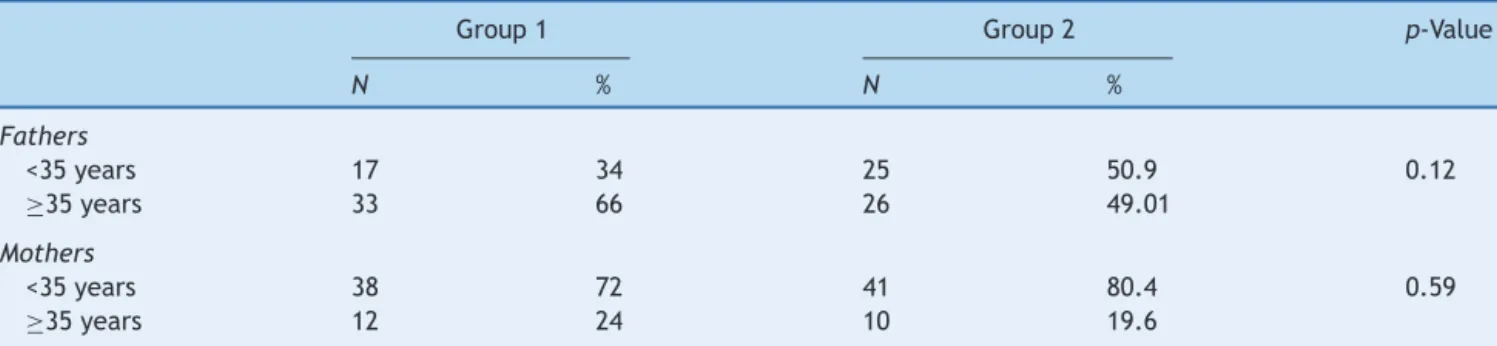
Table1 Parentalageatthetimeofconceptioninbothgroups.
Group1 Group2 p-Value
N % N %
Fathers
<35years 17 34 25 50.9 0.12
≥35years 33 66 26 49.01
Mothers
<35years 38 72 41 80.4 0.59
≥35years 12 24 10 19.6
rate of advanced age (≥35 years) among parents at the momentofconceptionwashigherinchildrenwithASDthan in their siblings (66% vs. 49.01% for fathers and 24% vs. 19.6%formothers),butthedifferencewasstatistically non-significant.
Inthepresentstudy,therateofconsanguinitywas28% (firstdegreein31%ofcases,seconddegreein26%ofcases, andthirddegreein43%ofcases).
Prenatal,perinatal,andpostnatalfactors(Table2)
Table2 displays a comparisonof prenatal, perinatal,and postnatal factors between both groups. Despite the fact that nostatistically significant differences were observed betweenprenatalfactorsinthegroups(p=0.13),the preva-lencewashigherinthefirstgroup(50%vs.35.3%).Table2
showsthatperinatalfactorsweremorefrequentinthefirst
group,witharateof60%vs.11.8%inthesecondgroup,a sta-tisticallysignificantdifference(p=0.03).Themostfrequent perinatalfactorsfound inthe ASDgroupwereacutefetal distress(26%),prematurity,anddifficultlaborobserved in 18%ineachcase.
As for postnatal factors, they were associated with ASD (40% in thefirst group vs. 9.8% in the second group, p=0.042);thesepostnatalfactorswereprimarilyatypeof respiratoryinfection(24%ofthecasesinthefirstgroup).
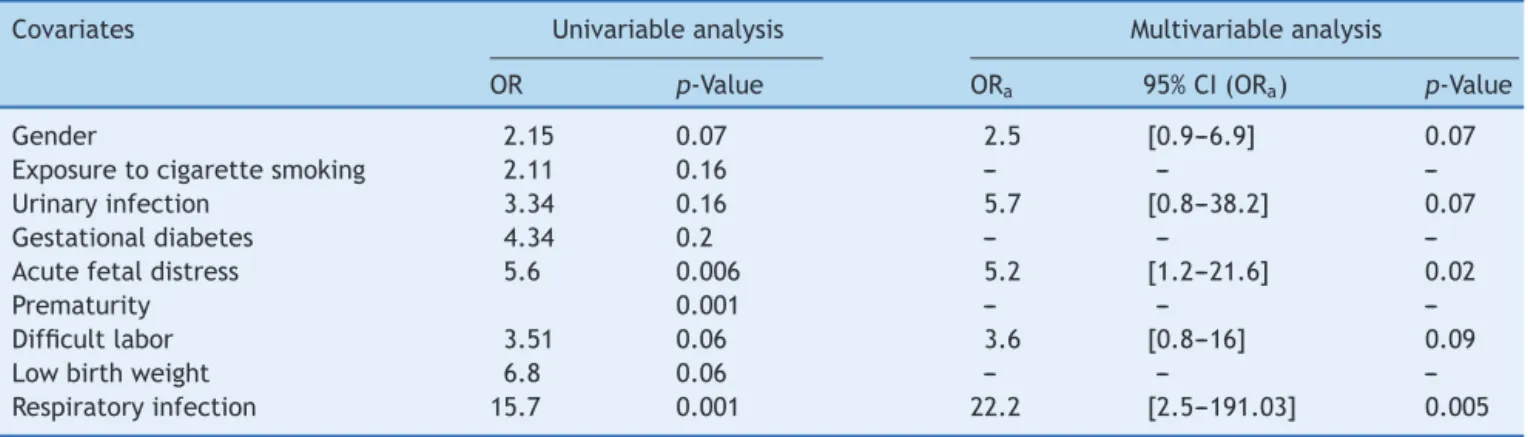
Table3showsthatafterlogisticregression,therisk fac-torsforautismthatremainedinthefinalmodelwere:male gender,prenatalurinarytractinfection,acutefetaldistress, difficultlabor,andrespiratoryinfection.
Fig.1showsthedistributionofprenatal,perinatal,and postnatalfactorsaccordingtotheseverityofautism.
No association was observed between the severity of autismandtheprenatal,perinatal,andpostnatalfactors.
Table2 Correlationbetweenpre-,peri-,andpostnatalfactorsinbothgroups.
Group1(n=50) Group2(n=51) p-Value
N % N %
Prenatalfactors 25 50 18 35.3 0.13
Exposuretocigarettesmoking 11 22 6 11.8 0.16
Urinaryinfection 6 12 2 3.9 0.16
Hypertensioninpregnancy 5 10 3 5.9 0.48
Threatenedabortion 5 10 3 5.9 0.48
Gestationaldiabetes 4 8 1 2 0.2
Hypotension 1 2 0 0 0.49
Perinatalfactors 30 60 6 11.8 <0.01
Acutefetaldistress 13 26 3 5.9 0.006
Prematurity 9 18 0 0 0.001
Exceedingtheterm 1 2 1 2 1
Difficultlabor 9 18 3 5.9 0.06
Lowbirthweighta 6 12 1 2 0.06
Macrosomiab 3 6 1 2 0.36
Postnatalfactors 20 40 5 9.8 <0.01
Respiratoryinfection 12 24 1 2 0.001
Urinaryinfection 3 6 1 2 0.36
Auditorydeficitc 2 4 0 0 0.24
Blooddiseased 1 2 2 3.9 1
aLowbirthweight<2500g. b Macrosomia>4000g.
c Auditorydeficit(alossof30dB).
Table3 AdjustedanalysisofriskfactorsofASD.
Covariates Univariableanalysis Multivariableanalysis
OR p-Value ORa 95%CI(ORa) p-Value
Gender 2.15 0.07 2.5 [0.9---6.9] 0.07
Exposuretocigarettesmoking 2.11 0.16 --- ---
---Urinaryinfection 3.34 0.16 5.7 [0.8---38.2] 0.07
Gestationaldiabetes 4.34 0.2 --- ---
---Acutefetaldistress 5.6 0.006 5.2 [1.2---21.6] 0.02
Prematurity 0.001 --- ---
---Difficultlabor 3.51 0.06 3.6 [0.8---16] 0.09
Lowbirthweight 6.8 0.06 --- ---
---Respiratoryinfection 15.7 0.001 22.2 [2.5---191.03] 0.005
Light to moderate autism
P=.16 P=.5
64% 67%
60%
65%
P=.2
58% 45%
Prenatal factors Perinatal factors Postnatal factors
Severe autism
Figure 1 Distributionof prenatal,perinatal, andpostnatal factorsaccordingtotheseverityofASD(atotalof50cases).
Discussion
Thepresentstudydiscussesprenatal,perinatal,and postna-talcomplications,aswellassomeparentalcharacteristics, thatcouldbeconsideredasriskfactorsforASD.
Parentalfactors
Previousstudieshavelinkedadvancedmaternaland pater-nalagetoincreasedriskforASDs.11,12
In the present study, the chose 35 years as the age cut-off for both parents. This choice was based the rec-ommendationsof manyauthors.11---13 Despitethefact that
acorrelationbetweenadvancedageatthemomentofthe conceptionofbothparentsandASDwasnotobserved,the frequencyofparentsagedover35yearswashigherin chil-drenwithASDthantheirsiblings(respectively24%vs.19.6% formaternalageandtwo-thirdsvs.almost50%forpaternal age).
Theories advocating the association between parental age and increased risk for ASDs include the potential for moregeneticmutationsinthegametesofolderfathersand mothers,aswellasalessfavorableinuteroenvironmentin oldermothers,withmoreobstetricalcomplicationssuchas lowbirthweight,prematurity,andcerebralhypoxia.11
Moreover,accordingtosomestudies,highprevalenceof chronic diseases among older women could contribute to
expandthe risk of adverse birthoutcomes.12,14 Data from
theliteraturetryingtoexplaintheincreasedriskforASD’s among older mothers have incriminated the high risk of obstetriccomplicationsobservedinthesemothers.11,12,14
Furthermore,congenitalanomalies arealsomore com-moninthefetusesandinfantsofoldermothers,andthese conditionscontributeinincreasingtheriskofASD.
Inthepresentstudy,arateof28%ofconsanguinitywas observed.Intheliterature, itisstated thatconsanguinity increases the chances of inheriting a bad DNA fit, which willdefinitelyresultinabirthdefect.Inbreddisordersmay causeotherabnormalities,andASDcanalsobebroughton byotherconditions.15Sincethecontrolgroup,inthepresent
study,wasrepresentedbythesiblings conceivedandborn fromthesame biologicalparents,consanguinitycouldnot beevaluatedasariskfactorforASD.
Prenatal,perinatalandpostnatalfactors
Inthepresentsurvey,nocorrelationwasobservedbetween theseverityof ASDandprenatal,perinatal,andpostnatal factors. The present results are in agreement with some recentstudies.16,17Conversely,somehypothesis havebeen
raised,indicatingthatthelightformofautismwouldshow weakerornoassociationwithobstetricriskfactors.
Prenatalfactors
Inthepresent study,theoccurrenceofmaternalinfection washigheramongcaseswhencomparedtocontrols(12%for thefirstgroupvs.3.9%forcontrols).
Accordingtomanystudies,adverseintrauterine environ-mentresultingfrommaternalbacterialandviralinfections during pregnancy is a significant risk factor for several neuropsychiatricdisordersincludingASD.15 Theassociation
between intrauterine inflammation, infection, and ASD is basedonbothepidemiologicalstudiesandcasereports.This associationisapparentlyrelatedtomaternalinflammatory process;hence,maternalimmuneactivationmayplayarole inneuro-developmentalperturbation.
Amongtheprenatalfactorsidentifiedinthisstudy, expo-sure to cigarettetobacco (passive smoking) wasnoted in 22% of cases. Retrospective epidemiological studies have observed, amongmothers of children with ASD,a signifi-cantlyincreasedpercentageof womenwhowereexposed totobaccoduring theconception of thechild. Therefore, maternal smokingwasconsidered asapotential maternal confoundingfactor,aswellasothertoxicchemicals.6
Someauthorshavedemonstratedthatmaternalcigarette smokingduringpregnancymayhaveacommutativeimpact onthelineageofherreproductivecells;itisalsoassociated withanincreased rateof spontaneousabortions,preterm delivery,reducedbirthweight,amongothers.19Thefindings
regardingitsrelationwithASDarestillcontroversial.20---22
The presentstudyshowedthat thefrequencyof gesta-tionaldiabeteswashigherinthefirstgroup(8%vs.2%inthe secondgroup).
Accordingtosomeauthors,gestationaldiabetesismainly associatedwithdisturbedfetalgrowthandincreasedrate of a variety of pregnancy complications.23 It also affects
fine and gross motor developmentand increasesthe rate oflearningdifficultiesandof attentiondeficit hyperactiv-itydisorder,acommoncomorbidneurobehavioralproblem inASD. The negativeeffects of maternal diabetes onthe brainmayresultfromintrauterineincreasedfetaloxidative stressandepigenetic changesintheexpression ofseveral genes.Theincreasedriskobservedmightberelatedtoother pregnancycomplications thatarecommonin diabetes, or toeffectsonfetalgrowthratherthantocomplicationsof hyperglycemia.Itisalsounknownwhetheroptimalcontrol ofdiabeteswillfurtherdecreasethisassociation.23
Because of its rising incidence, maternal diabetes has been considered, byseveral studies, asan obvious candi-datetobeassociatedwithASD,whereasothershavefailed todemonstratesuchassociations.15,20,23
In the current survey, hypertension, hypotension, and threatenedabortionweremorefrequentinthefirstgroup (respectively10%vs. 5.9%,2%vs. 0%,and10%vs.5.9%in thesecondgroup).Theseconditionsaregenerallyrelatedto fetallossandadverseinfantoutcomes,suchasprematurity, intrauterine growth retardation, still birth, and neonatal deathindicatingfetaldistress.Likewise,fetalhypoxiaisone ofthemanifestationsoffetaldistressandhasbeenreported toinduceconditionssuchasplacentalabruption,threatened prematuredelivery, emergency cesarean section, forceps delivery,spontaneousabortion,andvaryingdegreesof cere-braldamage.4,5Accordingly,ASDwaslinkedtofetaldistress:
oxygendeprivationcoulddamagevulnerableregionsinthe brain,suchasthebasalganglia,hippocampus,andlateral ventricles.Some neuroimagingstudies havedemonstrated abnormalitiesintheseregionsamongpatientswithASD com-paredwithcontrols.5,14
Perinatalfactors
In the present series, perinatal factors were very sig-nificantly associated with ASD (p=0.03). This result is consistent with the literature.4,24 In fact, complications
occurringduringlaboraffecttheneurodevelopmentofthe fetusandinfantinlaterstages,andcancontributetoward theriskofASD.
The current research also suggests that obstetric fac-tors occur more frequently in ASD children than in their unaffectedsiblings. The presentresults corroborateother studies reportingan association betweenperinatalfactors andASD.
Perinatal factors were represented by a long duration of delivery and prematurityin 18% of thecases each one and suffering acute fetal in 26% of the cases. Therefore, it isadmittedthattheseconditionsmayleadtofetal dis-tressandasphyxia,resultinginbraindamage.Fetaloxygen deprivationhasbeenproposedtoincreasetheriskforASD. Recently, researchhashighlightedthe occurrenceof ASDs in very preterm infants, in addition to already identified developmentaldisorders.4,14,24
Postnatalfactors
The presentfindings arein agreementwithprevious stud-iessuggesting thatpostnatal eventsmay increasethe risk for ASDs in some children.4 In fact, a significant
associa-tionbetweenpostnatalfactorsandASD(p=0.042)hasbeen observed.
In the present study, an association was observed between both urinaryand respiratory infections andASD. Thesefindingscouldbeexplainedbythereleaseofcytokines asimmuneresponsesofthebabytotheseinfections,which can affect neural cell proliferation and differentiation. TheseimpairmentsareknowntobeassociatedwithASD.5,25
Hearingdeficitsweremorecommoninthefirstgroup(4% vs.0%inthesecondgroup).Thepresentresultscorroborate thoseofFombonne,26whoreported,inameta-analysis,that
theprevalenceofsensorydeficitsinautismvaryfrom0.9% to5.9%.
Rosenhalletal.,27 inastudyconductedon199children
and adolescentswithASD, estimated that theprevalence ofhearingimpairmentinautismistentimeshigherthanin generalpopulation (11%).Theyalsoobservedthat7.9% of thepatientshadanmoderatehearingloss,3.5%were pro-foundly deaf, and18% had hyperacusis in the audiogram, even after controlling for the age factor. More recently, Kielinenetal.28 observed,inapopulationofchildrenwith
autism, that8.6% hadamild hearingloss, 7%a moderate deficit,and1.6%severedeficiency(hearinglossinmorethan 60dBataudiometry).
Thestrengthofthepresentstudyliesinitsprecise confir-mationoftheASD,theactiveparticipationofparents,and resortingtounaffectedsiblingsascontrols.Thislastfeature mayhelptoidentifyriskfactorsandtocontrolforhereditary background,familyenvironment,andmaternal predisposi-tion tocomplications in pregnancy or birth. Nonetheless, therearesomelimitations, namelythelimited numberof samples. Therefore, the present results should be com-pleted by epidemiological studies witha larger scale and inlargerpopulations.TofacetheissueofASDand consan-guinity,alargerpopulationwithandwithoutconsanguinity shouldbeevaluated.
Prenatal,perinatal,andpostnatalfactorsforASDshould be considered in the broadestsense: theseevents of the fetal,newborn, and infant environment couldinteract or contribute in combination with other co-factors (environ-mental and genetic, among others) to characterize ASD. Scoresindicatethatratherthanfocusingonasinglefactor, futurestudiesshouldinvestigatethecombinationofseveral factors.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.American Psychiatric Association. Autism spectrum disorder [FactSheet].AmericanPsychiatricAssociation;2013.Available from: http://www.dsm5.org/Documents/Autism%20Spectrum %20Disorder%20Fact%20Sheet.pdf[cited05.12.13].
2.ElsabbaghM,Divan G,KohYJ,KimYS,KauchaliS,MarcínC, etal.Globalprevalenceofautismandotherpervasive devel-opmentaldisorders.AutismRes.2012;5:160---79.
3.ZahorodnyW,ShenoudaJ,HowellS,RosatoNS,PengB,Mehta U.IncreasingautismprevalenceinmetropolitanNew Jersey. Autism.2014;18:117---26.
4.GomesPT,LimaLH,BuenoMK,AraújoLA,SouzaNM.Autism inBrazil:asystematicreviewoffamilychallengesandcoping strategies.JPediatr(RioJ).2015;91:111---21.
5.GardenerH,SpiegelmanD,BukaSL.Perinatalandneonatalrisk factorsforautism:acomprehensivemeta-analysis.Pediatrics. 2011;128:344---55.
6.TchaconasA,AdesmanA.Autismspectrumdisorders:apediatric overviewandupdate.CurrOpinPediatr.2013;25:130---44. 7.Mamidala MP, Polinedi A, PTV PK, Rajesh N, Vallamkonda
OR, Udani V, et al. Prenatal, perinatal and neonatal risk factors of autism spectrum disorder: a comprehensive epi-demiologicalassessmentfromIndia.ResDevDisabil.2013;34: 3004---13.
8.Froehlich-SantinoW,LondonoTobonA,ClevelandS,TorresA, PhillipsJ,CohenB,etal. Prenataland perinatalriskfactors inatwinstudyofautismspectrumdisorders.JPsychiatrRes. 2014;54:100---8.
9.HallmayerJ,ClevelandS,TorresA,PhillipsJ,CohenB, Tori-goe T, et al. Genetic heritability and shared environmental factors among twin pairs withautism. Arch Gen Psychiatry. 2011;68:1095---102.
10.Schopler E, ReichlerRJ, DeVellis RF, Daly K. Toward objec-tiveclassificationofchildhoodautism:ChildhoodAutismRating Scale(CARS).JAutismDevDisord.1980;10:91---103.
11.ParnerET,Baron-CohenS,LauritsenMB,JørgensenM,Schieve LA,Yeargin-AllsoppM,etal.Parentalageandautismspectrum disorders.AnnEpidemiol.2012;22:143---50.
12.Sandin S, Hultman CM, Kolevzon A, Gross R, MacCabe JH, Reichenberg A. Advancing maternal age is associated with increasingriskfor autism:a reviewandmeta-analysis.JAm AcadChildAdolescPsychiatry.2012;51:477---86.
13.JollyM,SebireN,HarrisJ,RobinsonS,ReganL.Therisks asso-ciatedwithpregnancyinwomenaged35yearsorolder.Hum Reprod.2000;15:2433---7.
14.Polo-Kantola P, Lampi KM, Hinkka-Yli-Salomäki S, Gissler M, BrownAS,SouranderA.Obstetricriskfactorsandautism spec-trumdisordersinFinland.JPediatr.2014;164:358---65. 15.GuinchatV,ThorsenP,LaurentC,CansC,BodeauN,CohenD.
Pre-,peri-and neonatalrisk factorsfor autism.Acta Obstet GynecolScand.2012;91:287---300.
16.Haglund NG, Källén KB. Risk factors for autism and Aspergersyndrome. Perinatalfactors and migration.Autism. 2011;15:163---83.
17.GlassonEJ,BowerC,PettersonB,deKlerkN,ChaneyG, Hall-mayerJF.Perinatalfactorsandthedevelopmentofautism:a populationstudy.ArchGenPsychiatry.2004;61:618---27. 18.DoddsL,FellDB,SheaS,ArmsonBA,AllenAC,BrysonS.Therole
ofprenatal,obstetric,andneonatalfactorsinthedevelopment ofautism.JAutismDevDisord.2011;41:891---902.
19.Kiechl-KohlendorferU,RalserE,PuppPeglowU,ReiterG, Gries-maierE,TrawögerR.Smokinginpregnancy:a riskfactor for adverseneurodevelopmentaloutcomeinpreterminfants?Acta Paediatr.2010;99:1016---9.
20.HultmanCM,SparenP,CnattingiusS.Perinatalriskfactorsfor infantileautism.Epidemiology.2002;13:417---23.
21.Larsson M, Weiss B, Janson S, Sundell J, Bornehag CG. Associations between in door environmental factors and parental-reportedautisticspectrumdisordersinchildren6---8 yearsofage.Neurotoxicology.2009;30:822---31.
22.LeeBK,GardnerRM,DalH,SvenssonA,GalantiMR,RaiD,etal. Briefreport: maternalsmoking duringpregnancy andautism spectrumdisorders.JAutismDevDisord.2012;42:2000---5. 23.OrnoyA,RatzonN,GreenbaumC,WolfA,DulitzkyM.
School-age children born to diabetic mothersand to mothers with gestational diabetes exhibit a high rate of inattention and fineandgrossmotorimpairment.JPediatrEndocrinolMetab. 2001;14:681---9.
24.MannJR,McDermottS,BaoH,HardinJ,GreggA.Pre-eclampsia, birthweight,andautismspectrumdisorders.JAutismDev Dis-ord.2010;40:548---54.
25.AshwoodP,KrakowiakP,Hertz-PicciottoI,HansenR,PessahI, VandeWaterJ.Elevatedplasmacytokinesinautismspectrum disordersprovideevidenceofimmunedysfunctionandare asso-ciatedwithimpairedbehavioraloutcome.BrainBehavImmun. 2011;25:40---5.
26.Fombone E. Prevalence of childhood disintegrative disorder. Autism.2002;6:149---57.
27.RosenhallU,NordinV,SandströmM,AhlsénG,GillbergC.Autism andhearingloss.JAutismDevDisord.1999;29:349---57. 28.KielinenM,RantalaH,TimonenE,LinnaSL,MoilanenI.