www.jped.com.br
ORIGINAL
ARTICLE
Influence
of
breastfeeding
in
the
first
months
of
life
on
blood
pressure
levels
of
preschool
children
夽
Luciana
Neri
Nobre
∗,
Angelina
do
Carmo
Lessa
UniversidadeFederaldosValesdoJequitinhonhaeMucuri(UFVJM),FaculdadedeCiênciasBiológicasedaSaúde, DepartamentodeNutric¸ão,Diamantina,MG,Brazil
Received10September2015;accepted26January2016 Availableonline27May2016
KEYWORDS
Child;
Breastfeeding; Bloodpressure
Abstract
Objective: To investigate whether breastfeeding in early life affects blood pressure of preschoolers.
Methods: Cross-sectionalstudy nestedinacohortfromamunicipalityinthestateofMinas Gerais,Brazil.Allchildreninthecohortwereinvitedforthisstudy.Thus,between2009and 2010,bloodpressureof230preschoolchildrenandtheirmothers,inadditiontoanthropometric variables,previous history, andsocioeconomic statuswere evaluated. Bloodpressure mea-surementwasassessedinthemorning,usingautomaticOmron®HEM-714INTandHEM-781INT devicestomeasurethebloodpressureofpreschoolchildrenandtheirmothers,respectively. Logisticregressionwasusedtostudytheassociationbetweenbreastfeedingandbloodpressure. Thesignificancelevelwassetat5%.
Results: This study identified 19 (8.26%)preschool children with high blood pressure (val-ues abovethe90th percentile). High systolicblood pressurewas associated with lowbirth weight(OR=5.41;95%CI=1.45---20.23)andtotalbreastfeedingdurationoflessthansixmonths (OR=4.14;95%CI=1.40---11.95).Highdiastolicbloodpressurewasnotassociatedwithany vari-able,whereashighsystolicbloodpressure/diastolicbloodpressureratiowasassociatedwith breastfeedingdurationoflessthansixmonths(OR=3.48;95%CI=1.34---9.1).
Conclusion: Theresultsofthisstudyindicatethatpreschoolersbreastfedforaperiodofless thansixmonthsweremorelikelytohavehighbloodpressurewhencomparedtothosebreastfed foralongerperiod,suggestingaprotectiveeffectofbreastfeedingagainsthighbloodpressure inthispopulation.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽
Pleasecitethisarticleas:NobreLN,LessaAC.Influenceofbreastfeedinginthefirstmonthsoflifeonbloodpressurelevelsofpreschool children.JPediatr(RioJ).2016;92:588---94.
∗Correspondingauthor.
E-mail:[email protected](L.N.Nobre).
http://dx.doi.org/10.1016/j.jped.2016.02.011
PALAVRAS-CHAVE
Crianc¸a; Aleitamento materno; Pressãoarterial
Influênciadoaleitamentomaternonosprimeirosmesesdevidanapressãoarterial depré-escolares
Resumo
Objetivo: Investigarsealeitamentonosprimeirosmesesdevidateminfluênciasobreapressão arterialdepré-escolares.
Métodos: Estudotransversalaninhadonumacoortedenascidosnummunicípiomineiro.Foram convidadas para esteestudo todas ascrianc¸asda coorte. Desse modo, entre2009e 2010, foramavaliadospressãoarterial(PA)de230pré-escolaresedesuasmães,alémdevariáveis antropométricasepregressasecondic¸ãosocioeconômica.AmedidadaPAfoifeitademanhã, comosmonitoresautomáticosdebrac¸oOmron®modeloHEM-714INTeHEM-781INTparamedir apressãoarterialdospré-escolaresedesuasmães,respectivamente.Paraoestudodarelac¸ão entrealeitamentomaternoepressãoarterialusou-searegressãologística.Onívelde significân-ciaadotadofoi5%.
Resultados: Foramidentificados19(8,26%)pré-escolarescompressãoarterialelevada(valores acimadopercentil90).Apressãoarterialsistólica(PAS)elevadaseassociouaobaixopesoao nascimento(OR=5,41;IC95%=1,45-20,23)eaoperíodototaldealeitamentomaternoinferior aseismeses(OR=4,14;IC95%=1,40-11,95).Elevadapressãoarterialdiastólica(PAD)nãose associou aqualquer variáveleaPAS/PADelevadasseassociaramaoperíododealeitamento maternoinferioraseismeses(OR=3,48;IC95%=1,34-9,1).
Conclusão: Ospré-escolaresamamentadosporumperíodoinferioraseismeses,quando com-parados comosqueamamentaramporumperíodo superior,apresentaram maiorchancede estarcompressãoarterialelevada,oquesugereefeitoprotetordoaleitamentomaternocontra elevac¸ãodapressãoarterialnapopulac¸ãoestudada.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Somediseasesthatareusuallyobservedinadultshavebeen affectingchildrenatanalarmingrate;amongthem,excess weightandhighbloodpressure(BP)shouldbehighlighted. Excess weight --- overweight/obesity --- has been consid-ereda worldwideepidemic.The HouseholdBudgetSurvey 2008---20091 disclosed that this problemaffected
approxi-mately33.5%ofBrazilianchildrenaged5---9years.According
toFriedman etal.,2 excessweight often accompanies an
increaseinBP.
High BP levels in childhood increase the chance of
systemicarterialhypertension(SAH)inadults,andalso
con-tributetocardiovasculardisease.2Thus,theidentification
andearlytreatmentofhypertensioninchildhoodcan
pre-ventfutureadverseoutcomes.
The Brazilian Society of Cardiology3 recommends that
BPshouldbemeasuredafterthreeyearsof age,annually,
or beforethat,when thereareriskfactors. However,the
complexmethodology establishedto verifyBP inchildren
makesmanyprofessionalsexcludeitfromtheroutine
exam-inationorincorrectlyinterpretthemeasuredvalues,which
mayresultinunderdiagnosisandundesirableconsequences
for these individuals.4 Thus, likely due to these factors,
theprevalence of high BPin the pediatricgroup haslong
been consideredirrelevant.However,severalstudieshave
identifiedthatthisconditionhasbeencommonatthisstage
oflife.5---11
As with most chronic, noncommunicable diseases, the
riskfactors for hypertension includegenetic components,
lifestyle,3,12 and inadequate feeding practices.3,10 Some
studies have suggested that breastfeeding may also be
an importantprotective factor against cardiovascular
dis-eases, hypertension, dyslipidemia, and obesity during
childhood.13
However,theprotectiveeffectofbreastfeedingagainst
highBPisstillcontroversial;whilesomestudieshave
iden-tifiedthiseffect,11,14othershavenot.9,15
ForBalabanandSilva,16nutritionalexperiencesoccurring
duringinfants’firstmonthsoflifecanaffecttheir
suscepti-bilitytochronicdiseasesinadulthood;thishasbeencalled
metabolicimprinting,atermthatdescribesaphenomenon
bywhich an early nutritionalexperience that acts during
acriticalandspecificperiodofdevelopment,whichcould
leadtoregulatorymechanismprogramming,suchasBP
reg-ulationthroughoutlife.17
In this sense, Horta et al.17 mention that different
biologicalmechanismscanhaveaneffectonthis
program-ming, among them the high concentration of long-chain
polyunsaturated fatty acids, which are important
struc-turalcomponentsofcellmembraneincludingthevascular
endothelium.
Considering the abovementioned aspects, this study
aimed to determine whether breastfeeding in the first
Methods
Studysubjectsandsetting
Thiswasacross-sectionalstudynestedinacohortof indi-viduals born in the municipality of Diamantina, state of MinasGerais, Brazil.18 Details about thecohort formation
andof the cross-sectionalstudy were previously reported
inanotherpublication.19 Inthepresentstudy,thechildren
fromtheaforementionedcohortwere5yearsold,ranging
from 4 months older or younger, and were submitted to
anthropometric,socioeconomic,andBPassessments.
Diamantina isamunicipality located inVale do
Jequit-inhonha, in Minas Gerais, Brazil. It has a literacy rate of
83.4% and a human development index of 0.748. Among
households,90.76%aresupplied withtreatedwater,70.7%
haveasewagesystem,and69.67%havegarbagecollection
services.20
The data collectionfor this study took placebetween
2004 and 2005 and between 2009 and 2010. In the first
period,datawerecollectedby anutritionistandstudents
oftheNutritionCourseofUniversidadeFederaldosValesdo
JequitinhonhaeMucuri(UFVJM),andinthesecondperiod,
byfournutritionistsandonestudentoftheaforementioned
UniversityNutrition Course.Beforethestart ofthe study,
theresearchersweretrainedtostandardizethemeasures.
The childrenwere visitedat theirhomesinboth study
periods; in the firstperiod all variables were assessed at
home,while inthesecondstageofthestudyahomevisit
wasconductedinwhichaquestionnairewasappliedtothe
child’sparentorguardian,followedbyascheduleddayand
timeforanthropometricandBPmeasurementsofthe
chil-drenandtheirmothers.
Assessedvariables
Amongthe assessedvariables,the onesusedin thisstudy include the following: body mass index (BMI), waist cir-cumference(WC),householdincome,numberofhousehold members,andBPofthechildrenattheageof5,aswellas oftheirmothers.Additionally,informationonbodyweight atbirthanddurationofbreastfeedinginthefirstmonthsof lifewasalsocollected.
The children’s weight was measured using a portable electronicKratos® digital scale (Kratos®, SP, Brazil), with amaximumcapacityof150kgandprecisionof50g;asfor the height, it was measured using an Altura Exata® sta-diometer(Alturexata®,MG,Brazil)withprecisionof0.1cm. WCmeasurementwascarriedoutwithameasuringtapeat midpointbetweentheiliac crestandthelastrib.21 These
measuresweretakenaccordingtoprotocolsrecommended
byJelliffe,22 onthepremisesofUFVJM,inthemorning.
The cutoff point >1 z-score identified children with
excess weight according to BMI/age.23 The World Health
Organization’s(WHO)Anthro2005version2.0.1andAnthro
2009 Plus version 3 were used to identify the children’s
z-scores.Itisworthmentioningthatthetwosoftware
pro-gramswereused,consideringthatthechildren’sageduring
datacollectionwas 5years, ranging from4 monthsolder
to4 monthsyounger.Foranalysisofthe variableWC,the
riskcategory valuesweredefinedasthoseabovethe75th
percentile.
Theper capitaincomeof thechild’sfamilywas
calcu-latedbasedoninformationabouttotalfamilyincomeand
numberofhouseholdmembers.Duringthestudyperiod,the
minimum wage was R$ 540.00 in Brazil. This information
wasobtained througha structuredquestionnaire
adminis-teredtothechild’smotherorguardianduringthehousehold
interview.
BPwasmeasured onasingleoccasion,withthree
mea-surements made with a 5-min interval between them,
precededby10minofrest.Theaverageofthethree
mea-surements was usedfor the analysis. Automatic HEM-arm
Omron®714INTand781INT(Omron®,Netherlands)monitors
wereusedtoassesstheBPofpreschoolchildrenandtheir
mothers,respectively.Thesemeasurementswereobtained
accordingtothemanufacturer’srecommendations.
BP classificationfollowed the criteriaof the VI
Guide-linesonArterialHypertension,3 which considersBPvalues
for children andadolescents according to the percentiles
ofheightforbothgendersbelowthe90thpercentileas
nor-motensive,aslongastheyare<120/80mmHg;between90th
and95thpercentilesasborderline,andgreaterthanorequal
tothe 95th percentile,ashypertension. In thisstudy,for
preschoolchildren,‘‘highBP’’valueswereconsideredwhen
>the 90thpercentile,andfor themothers,values greater
thanorequalto140/90mmHg.
Maternal breastfeeding was defined according to the
recommendations ofthe WHO.24 Thus,children whowere
breastfeduptosixmonths,regardlessofthe introduction
ofotherfoods,wereconsideredasreceivingbreastfeeding.
Dataonbreastfeedingwereobtainedprospectivelyfromthe
cohortstudy,whenthechildrenwerevisited,aswellasat
home,onamonthlybasis.
This study used data from two larger studies entitled
‘‘Foodandgrowthinthefirstyearoflife:acohortstudy’’18
and‘‘Determinantsofnutritionalstatusofchildrenatfive
years of age in thecity of Diamantina: study of a cohort
assessed in the first year of life.’’25 Both studies were
approvedbytheResearchEthicsCommitteesofUFVJM,with
protocolnumbers011/05and039/08,respectively.The
chil-dren’sparentsorguardianssignedtheinformedconsentto
participateinthestudy.
Statisticalanalysis
Logistic regression analysis was used to determine the influence of breastfeeding on the presence of high BP in preschoolers. Initially, a bivariateanalysis wasperformed andthosevariableswithp-value<20%wereselectedforthe multivariateanalysis.Thelevelofsignificancesettoreject thenullhypothesiswas95%.
Thepowerofthesamplewascalculatedretrospectively usingthestatisticalsoftwareG*Power.26 Forthisanalysis,
the parameters used were the oddsratio (OR) of 2.6 for
highBP(SBP/DBP)accordingtothebreastfeedingduration
obtainedattheunadjustedlogisticregressionanalysis,with
amaximumprobabilityoferrorof5%.Thepoweridentified
Results
Thiswasacross-sectionalstudynestedinabirthcohortand, aspreviouslymentioned,thecohortformationandthe chil-dren’sfollow-uphavebeenpreviouslypublished.19Thus,in
searchofchildrenforthisstudy,itwasdecidedtostudythe
eligiblepreschoolersforthecohortandnotonlythosewho
werefollowedinthefirstyearoflife,inordertoavoid
signif-icantlossesthatwouldinvalidatethepresentstudy,asthere
waslossofsomechildrenduringthefollow-up.Therefore,
therewasalossof49preschoolersinthisstudy.
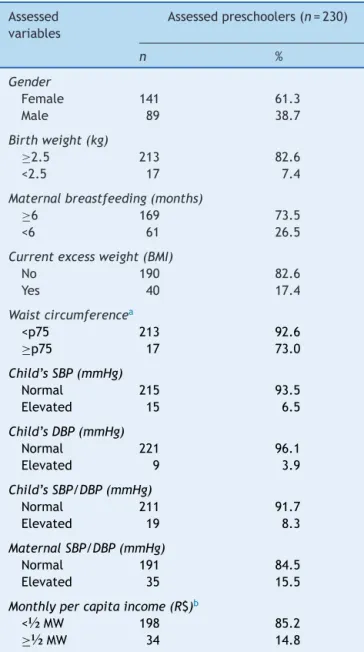
Atotalof230childrenwereevaluated,ofwhom19(8.2%)
wereclassifiedashavinghigh BP, i.e.,SBP/DBP >the90th
percentile,with 6.5%and 3.9% showingelevated SBP and
DBP, respectively. The prevalence of breastfeeding in the
sixthmonthoflifewasapproximately74%(Table1).
Table1 Socioeconomic,maternal,andcurrentandformer characteristicsofpreschoolers.Diamantina,MG-2010.
Assessed variables
Assessedpreschoolers(n=230)
n %
Gender
Female 141 61.3
Male 89 38.7
Birthweight(kg)
≥2.5 213 82.6
<2.5 17 7.4
Maternalbreastfeeding(months)
≥6 169 73.5
<6 61 26.5
Currentexcessweight(BMI)
No 190 82.6
Yes 40 17.4
Waistcircumferencea
<p75 213 92.6
≥p75 17 73.0
Child’sSBP(mmHg)
Normal 215 93.5
Elevated 15 6.5
Child’sDBP(mmHg)
Normal 221 96.1
Elevated 9 3.9
Child’sSBP/DBP(mmHg)
Normal 211 91.7
Elevated 19 8.3
MaternalSBP/DBP(mmHg)
Normal 191 84.5
Elevated 35 15.5
Monthlypercapitaincome(R$)b
<½MW 198 85.2
≥½MW 34 14.8
MW,minimumwage.
a RiskcategorywasdefinedasWCvalues>75thpercentile. b Minimumwageatthetimeofthestudy:R$540.00.
Theresultsofthebivariateanalysisofvariables associ-atedwithelevatedsystolicanddiastolicBP;bothareshown inTable2.Itcanbeobservedthatbirth weightand
dura-tionofbreastfeeding wereassociatedwithSBPlevels.No
variable was associated with DBP; however, birth weight
anddurationofbreastfeedingwereassociatedwithSBP/DBP
(Table2).
In the adjusted model, birth weight and duration of
breastfeedingremainedassociated withelevated SBPand
timeofbreastfeedingwithSBP/DBP(Table3).
Discussion
Amongtheassessedpreschoolers,theprevalenceofhighBP waswithinthenationalstatistics.Thefindingsindicatethat childrenwithlowbirthweightandthosewhowerebreastfed forlessthansixmonthsweremorelikelytohaveelevated systolicBP at 5 yearsof age. Elevated SBPwasnot asso-ciatedwithanymeasuredvariable,andchildrenwhowere breastfedforlessthansixmonths,whencomparedtothose breastfedforlongerperiods,hadhigherSBP/DBP.
InBrazil, therearenonationalstatisticsonthe preva-lenceofhighBPinthepediatricpopulation,whichhinders theknowledgeoftherealproblemfacedbychildren. Fur-thermore,it is believed that high BP is rare in childhood and,thus,itsincidenceendsupbeingunderestimateddue tothedifficultyofdiagnosis,whichrequiresadequate tech-nique, material, and an appropriate environment for BP measurement.4,27Inadditiontobeingconsideredashaving
lowprevalence, the measurementof BPis not performed
duringroutineconsultationsinthepediatricgroup.
However,itisworthmentioningthattheaforementioned
studies5---11,28thatassessedhighBPinchildrenand/or
ado-lescentsidentified prevalence rates ranging from1.7% to
19.9%.Noneofthesestudiesmentionedthetimewhenthe
BPwas measured, and therewasalso variationregarding
themeasurementmethod,i.e.,theequipmentusedranged
from automatic devices to aneroid sphygmomanometers
and the number of measurements and time between the
measurementsalsovaried;therefore,thesevariationsmay
explaindifferencesinthesestatistics.Additionally,the
cut-offpointsusedforhighBPclassificationrangedfromvalues
abovethe90thor95thpercentiles.
Animportantaspectthatshouldbementionedisthe
pos-sibilitythattheBPmeasurementmaybetheresultofwhite
coatsyndrome,asinthisresearchBPwasmeasuredona
sin-gleoccasionand,formostchildren,itwasthefirsttimethat
BPwasbeingmeasured.Thiscomplicatingfactor,however,
mustbesharedbymostofthecross-sectionalstudies.
Itisworthmentioning,however,thatcarefuladherence
tothemeasurementmethodologymayhaveminimizedthis
problem.InthisresearchtheBPwasmeasuredinthe
morn-ing;threepressuremeasurementswereperformed witha
5-minintervalbetweeneachandtheaveragewasusedfor
theanalysis. Moreover,the device usedfor this
measure-menthasanautomaticsystemthatdetectsarrhythmiaand
abodymotionsensorthatwarnstheresearchersaboutthe
possibilityofthissyndrome.
Regarding the association between duration of
breast-feedingandBPlevels,thefindingscorroborateotherstudies
Table2 Crudeodds ratios(OR) andrespectiveconfidenceintervals(CI) oftheanalysisofvariablesassociated withblood pressureinpreschoolers.Diamantina,MG-2010.
Variables SBPd DBPd SBP/DBPd
OR 95%CI p-Value CrudeOR 95%CI p-Value OR 95%CI p-Value
Gender
Male 1 1 1
Female 0.7 0.2---2.2 0.51 0.8 0.2---2.9 0.72 0.7 0.3---1.7 0.42
Birthweight(kg)
≥2.5 1 1 1
<2.5 5.6 1.6---20.2 0.008 3.9 0.7---20.6 0.10 2.6 0.7---10.1 0.16
Totalbreastfeeding(months)a
≥6 1 1 1
<6 4.7 1.6---13.8 0.005 2.3 0.6---8.8 0.23 3.5 1.3---9.0 0.001
Excessweight(kg/m2)
No 1 1
Yes 1.2 0.3---4.5 0.78 --- --- --- 0.9 0.2---3.2 0.85
WC(cm)b
<p75 1 1
≥p75 2.0 0.4---9.9 0.37 --- --- --- 1.5 0.3---7.3 0.58
MaternalSBP/DBP(mmHg)
Normal 1 1 1
Elevated 1.4 0.4---5.2 0.62 1.6 0.3---8.0 0.57 1.5 0.5---4.9 0.48
Percapitaincome(R$)c
≥½MW 1 1
<½MW 0.7 0.2---2.5 0.55 --- --- --- 0.9 0.2---3.3 0.89
aValuereferstothetotalbreastfeedingtime. b Referstowaistcircumference(WC).
c Valuereferstoaminimumwage(MW)ofR$540.00.
d Elevatedvalueswerethose>90thpercentilealone(systolic[SBP]ordiastolic[DBP]bloodpressure)orboth(SBP/DBP).
Table3 Adjustedoddsratio(OR)andrespectiveconfidenceintervals(CI)oftheanalysisofvariablesassociatedwithblood pressureinpreschoolers.Diamantina,MG-2010.
Variables SBPa SBP/DBPb
OR 95%CI p-Value OR 95%CI p-Value
Birthweight(kg)
≥2.5 1 1
<2.5 6.0 1.5---23.3 0.009 2.6 0.6---10.5 0.171
Totalbreastfeeding(months)
≥6 1 1
<6 4.9 1.6---14.9 0.005 3.5 1.3---9.1 0.011
Significancelevelused:5%ofprobability.
aSystolicbloodpressure(SBP)---analysisadjustedfortimeofbreastfeedingandbirthweight.
b Systolic(SBP)anddiastolic(DBP)bloodpressure---analysisadjustedfortimeofbreastfeedingandbirthweight.
ofbreastfeedingandincreasedBPinchildhood.9,11,14,28,29In
thepresentstudy,thechildrenwhowerebreastfedforless
thansix monthsshowed afour-fold increasedrisk of high
SBP,andthree-foldhigher riskof elevatedSBP/DBP ratio,
whencomparedwiththosewhowerebreastfedforlonger
periods.
Itisworthmentioningthatthiswascross-sectionalstudy
nested in acohort and, thus, this factgives greater
con-sistencytothefindings,consideringthatthebreastfeeding
data collection was performed prospectively, i.e., it was
assessed monthly in the first year of life of the children,
reducinganimportantbias,whichisthemothers’recallof
theirchildren’seatinghabits.
As in the present study, Amorin et al.11 and
Naghet-tini et al.28 observed a higher mean SBPin children with
shorter breastfeeding duration when compared to those
with longer periods. Martin et al.14 also observed similar
Theseresearchersobservedthat at7.5yearsof age,
chil-dren whowerebreastfedshowed1.2mmHg-lowersystolic
and0.9mmHg-lowerdiastolicBPwhencomparedwiththose
whowereneverbreastfed.
In the study by Lawlor et al.29 with students aged
9---15years,researchersidentifiedasignificantassociation
betweentimeofbreastfeedingandBP,withadose-response
effect,i.e.,greaterreductionsinBPoccurredamongthose
withlongerexclusivebreastfeedingtime.
Inthepresentstudy,theprevalenceofelevatedDBPwas
lowerthanelevatedSBP,whichexplainsthelackof
associ-ationwiththestudiedvariables.Thisresultwasexpected,
asthestudiedgroupconsistsofpreschoolchildren,without
anydiagnosis of diseasesthat couldaffectthecirculatory
system. And considering that BP measurement evaluates
cardiac contraction (SBP) and subsequent blood flow to
extra-cardiacbody parts(DBP),which is indicative of the
strengthofbloodflowinthearteries,itisnotcommonto
findthistypeofalterationinchildrenconsideredotherwise
healthy,asinthisresearch.
Fromtheperspectiveoftheaforementionedmechanisms
proposed in this study about the effect of breastfeeding
onBP,16Forsythetal.30 developedastudyinwhichbabies
werefedintheneonatalperiodwithmilkformula
supple-mentedwithlong-chainpolyunsaturatedfattyacids.These
researchersobserved that at theend of childhood, these
childrenhada3mmHgdecreaseinBPwhencomparedwith
children who received formula without fatty-acid
supple-mentation.
Although the study developed by Yi et al.,8 with
Chi-nese children, identified that a family history of high BP,
waist circumference values, and body mass index were
associated withBP of theassessed children, in thisstudy
these variables were not associated withBP of the
stud-iedpreschoolchildren.Inthepresentstudy,thesevariables
were control variables for the main investigated
associa-tion.
Onelimitationofthisstudyisitscross-sectionaldesign,
makingitdifficulttoidentifyacausalassociation.
Random-izedclinicaltrialsandcohortstudiesaremoreappropriate
forcausalidentification.Additionally,other variablessuch
asdietandpaternalhypertensionwerenotstudied;these
can have a confounding effect on the observed
associa-tion.
Theresultsofthisresearchshowthatpreschoolchildren
whowere breastfed for less than six months, when
com-pared tothose breastfed for a longer period, were more
likelytohavewithhigh BP,suggesting aprotective effect
of breastfeeding against high BP in the studied
popula-tion.
Funding
Fundac¸ãodeAmparoàPesquisadoEstadodeMinasGerais ---Fapemig(Processn.:APQ-00428-08).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.InstitutoBrasileirodeGeografiaeEstatística(IBGE).Pesquisa deorc¸amentos familiares2008-2009:antropometriaeestado nutricionaldecrianc¸as,adolescenteseadultosnoBrasil.Rio deJaneiro:IBGE;2010.
2.FriedemannC,HeneghanC,MahtaniK,ThompsonM,PereraR, WardAM.Cardiovascular diseaseriskinhealthychildrenand its associationwithbodymass index: systematicreview and meta-analysis.BMJ.2012;345:e4759.
3.Sociedade Brasileira de Cardiologia/Sociedade Brasileira de Hipertensão/SociedadeBrasileira de Nefrologia.VI diretrizes brasileirasdehipertensão.ArqBrasCardiol.2010;95:1---51. 4.Brady TM, Solomon BS, Neu AM, Siberry GK, Parekh RS.
Patient-, provider-, and clinic-level predictors of unrecog-nizedelevatedbloodpressureinchildren.Pediatrics.2010;125: e1286---93.
5.Rosaneli CF,Baena CP,Auler F,NakashimaAT, Netto-Oliveira ER.Aumentodapressãoarterialeobesidadenainfância:uma avaliac¸ão transversal de 4.609 escolares. Arq Bras Cardiol. 2014;103:238---44.
6.SilvaAO,SilvaMV,PereiraLK,FeitosaWM,Ritti-DiasRM,Diniz PR,etal.Associationbetweengeneralandabdominalobesity withhighbloodpressure:differencebetweengenders.JPediatr (RioJ).2016;92:174---80.
7.KarS,KhandelwalB.Fastfoodsandphysicalinactivityarerisk factorsforobesityandhypertensionamongadolescentschool childrenineast districtofSikkim,India.JNatSciBiolMed. 2015;6:356---9.
8.YiZ,RongLW,ChongS,QianF,MingSX.Prevalenceand corre-latesofelevatedbloodpressureinChinesechildrenaged6---13 years:a nationwideschool-basedsurvey.BiomedEnvironSci. 2015;28:401---9.
9.CrispimPA,PeixotoMR,JardimPC.Fatoresderiscoassociados aosníveispressóricoselevadosemcrianc¸asdedoisacincoanos. ArqBrasCardiol.2014;102:39---46.
10.XiB,ZhangT,ZhanM,LiuF,ZongX,ZhaoM,etal.Trendsin elevatedbloodpressureamong USchildrenand adolescents: 1999---2012.AmJHypertens.2016;29:217---25.
11.AmorimRJ,CoelhoAF,LiraPI,LimaMC.Isbreastfeeding pro-tectiveforbloodpressureinschoolchildren?Acohortstudyin northeastBrazil.BreastfeedMed.2014;9:149---56.
12.JuholaJ,OikonenM,MagnussenVM,MikkiläV,SiitonenN, Joki-nenE,et al.Childhoodphysical,environmental,and genetic predictors of adult hypertension:the Cardiovascular Risk in YoungFinnsstudy.Circulation.2012;126:402---9.
13.KelishadiR,FarajianS.Theprotectiveeffectsofbreastfeeding onchronicnon-communicablediseasesinadulthood:areview ofevidence.AdvBiomedRes.2014;3:3.
14.MartinRM,NessAR, GunnellD,EmmettP,DaveySG,ALSPAC StudyTeam.Doesbreast-feedingininfancylowerblood pres-sureinchildhood?TheAvonLongitudinalStudyofParentsand Children(ALSPAC).Circulation.2004;109:1259---66.
15.Djalalinia S, Qorbani M, Heshmat R, Motlagh ME, Ardalan G. Association of breast feeding and birth weight with anthropometric measures and blood pressure in children and adolescents: the CASPIAN-IV study. Pediatr Neonatol. 2015;56:324---33.
16.BalabanG,SilvaGA.Efeitoprotetordoaleitamentomaterno contraaobesidadeinfantil.JPediatr(RioJ).2004;80:7---16. 17.HortaB,BahlR,MartinesJ,VictoraC.Evidenceofthelong-term
effectsofbreastfeeding:systematicreviewsandmeta-analysis. Geneva, Switzerland:WorldHealth Organization Publication; 2007.
19.Nobre LN, Lamounier JA, Franceschini SC. Padrão alimen-tar de pré-escolaresefatores associados. J Pediatr (Rio J). 2012;88:129---36.
20.Prefeitura de Diamantina. Dados Gerais; 2015. Avail-able from: http://www.diamantina.mg.gov.br/portal1/ dadogeral/mumain.asp?iIdMun=100131242[cited28.08.15]. 21.LohmanTG,RocheAF,MartorellR.Anthropometric
Standardiza-tionReferenceManual.AbridgedEditionChampaign,IL:Human KineticsBooks;1991.p.39---54.
22.JelliffeDB.Evaluacióndelestadodenutricióndelacomunidad. Ginebra:OrganizaciónMundialdelaSalud;1968[OMS---Série demonografias,53].
23.World Health Organization. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: World Health Organization, Department of Nutrition for Health and Development; 2006.
24.OrganizaciónMundialdelaSalud.Indicadoresparaevaluarlas prácticas de alimentación del lactantey del ni˜no peque˜no: conclusiones de la reunión de consenso llevada a cabo Del 6 al8 noviembre de 2007. Washington, DC,EE.UU. Geneva: Unicef/OMS;2009.
25.NobreLN[thesis]Fatoresassociadosaoexcessodepesoe dis-lipidemiaempré-escolaresdacidadedeDiamantina/MG.Belo Horizonte:UniversidadeFederaldeMinasGerais,Programade Pós-Graduac¸ãoemSaúdedaCrianc¸aedoAdolescente;2011.
26.PortneyLG,WatkinsMP.Foundationsofclinicalresearch: appli-cationstopractice.3ed.PrenticeHall;2008.
27.NationalHighBloodPressureEducationProgramWorkingGroup on High Blood Pressure in Children and Adolescents. The fourthreportonthediagnosis,evaluation, andtreatmentof high blood pressure in children and adolescents. Pediatrics. 2004;114:555---76.
28.NaghettiniAV,BelemJM,SalgadoCM,VasconcelosJúniorHM, SeronniEM,JunqueiraAL,etal.Avaliac¸ãodosfatoresderiscoe protec¸ãoassociadosàelevac¸ãodapressãoarterialemcrianc¸as. ArqBrasCardiol.2010;94:486---91.
29.LawlorDA,RiddochCJ,PageAS,AndersenLB,WedderkoppN, HarroM,etal.Infantfeedingandcomponentsofthemetabolic syndrome:findingsfromtheEuropeanYouthHeartstudy.Arch DisChild.2005;90:582---8.