REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effects
of
dexmedetomidine
in
conjunction
with
remote
ischemic
preconditioning
on
renal
ischemia---reperfusion
injury
in
rats
Emine
Bagcik
a,
Sevda
Ozkardesler
b,
Nilay
Boztas
b,∗,
Bekir
Ugur
Ergur
c,
Mert
Akan
b,
Mehmet
Guneli
d,
Sule
Ozbilgin
baGordesStateHospital,AnesthesiologyandReanimation,Manisa,Turkey
bMedicalFacultyof9EylulUniversity,AnesthesiologyandReanimation, ˙Izmir,Turkey
cMedicalFacultyof9EylulUniversity,HistologyandEmbryology, ˙Izmir,Turkey
dMedicalFacultyof9EylulUniversity,LaboratoryAnimalScience, ˙Izmir,Turkey
Received4July2013;accepted2January2014 Availableonline18February2014
KEYWORDS
Kidney;
Ischemia---reperfusion injury;
Dexmedetomidine; Caspase-3; Ischemic preconditioning; Apoptosis
Abstract
Backgroundandobjectives: The aim of this study was to evaluate the effects of remote ischemic preconditioning by brief ischemia of unilateral hind limb when combined with dexmedetomidineonrenalischemia---reperfusioninjurybyhistopathologyandactivecaspase-3 immunoreactivityinrats.
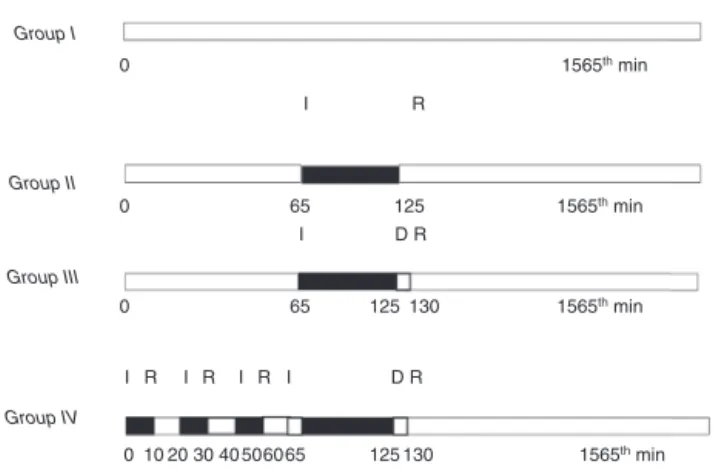
Methods:28Wistaralbinomaleratsweredividedinto4groups.GroupI(Sham,n=7): Laparo-tomyandrenalpedicledissectionwereperformedat65thminuteofanesthesiaandtherats wereobserved underanesthesiafor130min.Group II(ischemia---reperfusion,n=7):At65th minuteofanesthesiabilateralrenalpedicleswereclamped.After60minischemia24hof reper-fusionwasperformed.GroupIII(ischemia---reperfusion+dexmedetomidine,n=7):Atthefifth minuteofreperfusion(100g/kg intra-peritoneal)dexmedetomidine wasadministered with ischemia---reperfusiongroup.Reperfusionlasted24h.GroupIV(ischemia---reperfusion+remote ischemicpreconditioning+dexmedetomidine,n=7):Afterlaparotomy,threecyclesofischemic preconditioning(10minischemiaand10minreperfusion)wereappliedtothelefthindlimband after5minwithgroupIII.
Results:Histopathologicalinjury scoresand activecaspase-3immunoreactivity were signifi-cantlylowerintheShamgroupcomparedtotheothergroups.Histopathologicalinjuryscores ingroupsIIIandIVweresignificantlylowerthangroupII(p=0.03andp=0.05).Activecaspase-3 immunoreactivitywassignificantlylowerinthegroupIVthangroupII(p=0.01)andtherewas nosignificantdifferencebetweengroupIIandgroupIII(p=0.06).
∗Correspondingauthor.
E-mail:[email protected](N.Boztas).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Conclusions: Pharmacologic conditioning with dexmedetomidine and remote ischemic pre-conditioning when combined withdexmedetomidine significantly decreasesrenal ischemia---reperfusioninjuryhistomorphologically.Combineduseoftwomethodspreventsapoptosisvia activecaspase-3.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Rim; Lesãode
isquemia-reperfusão; Dexmedetomidine; Caspase-3;
Pré-condicionamento isquêmico;
Apoptose
Efeitosdedexmedetomidinaemconjuntocomopré-condicionamentoisquêmico
remotoemlesãodeisquemia-reperfusãorenalemratos
Resumo
Justificativaeobjetivos: Avaliarosefeitosdopré-condicionamentoisquêmicoremoto, medi-antebreveisquemiademembroposteriorunilateral,emcombinac¸ãocomdexmedetomidinaem lesãodeisquemia-reperfusãorenalpormeiodehistopatologiaeimunorreatividadedacaspase-3 ativaemratos.
Métodos: Foramdivididos em quatro grupos 28 ratosmachos albinosWistar. GrupoI(Sham [cirurgia controle], n=7): laparotomia e dissecc¸ão do pedículo renal foram feitas em 65 minutos de anestesia e os ratos foram observados sob anestesia por 130minutos. Grupo II (isquemia-reperfusão, n=7): no 65◦ minuto de anestesia, os pedículos renais bilaterais
foram pinc¸ados; após 60minutos de isquemia, foi feita reperfusão de 24horas. Grupo III (isquemia-reperfusão+dexmedetomidina,n=7):noquintominutodereperfusão, dexmedeto-midina (100mg/kg intraperitoneal) foi administrada ao grupo com isquemia-reperfusão. A reperfusão durou 24horas. Grupo IV (isquemia-reperfusão+pré-condicionamento isquêmico remoto+dexmedetomidina, n=7): após a laparotomia, três ciclos de pré-condicionamento isquêmico(10minutosdeisquemiae10minutosde reperfusão)foramaplicados nomembro posterioresquerdoedepoisdecincominutosaogrupoIII.
Resultados: Osescoresdelesãohistopatológicaeimunorreatividadedacaspase-3ativaforam significativamentemenoresnogrupoShamemcomparac¸ãocomosoutros.Osescoresdelesão histopatológicadosgruposIIIeIVforamsignificativamentemenoresdoqueosdoII(p=0,03e p=0,05).Aimunorreatividadedacaspase-3foisignificativamentemenornogrupoIVdoqueno II(p=0,01)enãohouvediferenc¸asignificanteentreosgruposIIeIII(p=0,06).
Conclusões: Ocondicionamentofarmacológicocomdexmedetomidinaeopré-condicionamento isquêmico remoto em combinac¸ãocomdexmedetomidina diminuem demodo significante a lesãodeisquemia-reperfusãorenalhistomorfologicamente.Ousocombinadodosdoismétodos previneaapoptoseviacaspase-3ativa.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Ischemicacuterenalinjuryisaclinicalsyndromewithhigh mortalityandmorbidity.Duetoitshighenergyrequirements and the complex network of the renal microvasculature, thekidney is highlysensitive toischemia---reperfusion(IR) injury.1---4ThemechanismsofrenalIRinjuryare multifacto-rial,includinghypoxia,free-radicaldamage,andlocaland systemicinflammatoryresponses.5Reperfusionofischemic renal tissue induces complex cellular conditions and the deathofrenalcells,duetoapoptosis.6
Apoptosisisaformofgeneticallyprogrammedcelldeath. Twomainpathwaysplayaroleinepithelialapoptosis.The first, known as the extrinsic or death receptor pathway, is stimulated by TNF-␣-family molecules bound to CD95 ligand(Fasligand=CD95)throughextracellularsignals.This pathway combines withthe second pathway, the intrinsic or mitochondrialpathway,via caspase-3 activation,which includescytochromecandtheBcl-2familyofproteins,and together,theyenhanceapoptosis.7
Renal tubular cell apoptosis is a resultof renal injury and a primary and major contributor to IR pathophysio-logy. Bothinflammation and apoptosiscoexist in renal IR injury.Duringhypoxia,caspaseactivityincreasesasaresult ofintracellular Ca2+ accumulation.Caspasebecomes
acti-vatedinischemictissuesandisanindicatorofcelldeath.8 Thesechanges,whichcanbeobservedintubularcells,may causethelossofbrushbordersofproximaltubularcells,and spilloutfromthebasementmembraneofthecellsintothe tubularlumen,witheventualtubuleobstruction.9,10
Among the methods used to reduce the effects of IR injury, remote ischemic preconditioning (RIPC) and phar-macological conditioning are the most commonly used.11 Inreviewingthe English-languageliterature,nostudy was found regarding an experimental IR model to investigate the effects of using pharmacological conditioning with dexmedetomidineadministeredincombinationwithRIPC.
I R Group I
Group II
Group III
Group IV
I D R
D R
1565th min
1565th min
1565th min
1565th min
125
125
125130 130 65
0 0
0
0 10 20 30 40 506065 I R I R I R I
65
Figure1 Schematicrepresentationoftheexperimental pro-tocol.I,ischemia;R,reperfusion;D,deksmedetomidine.
histopathologically and to evaluate active caspase-3 immunoreactivityinaratrenalIRmodel.
Materials
and
methods
In total, 28 adult male Wistar albino rats, weighing 250---300g,wereused.Untilthebeginningoftheresearch, ratswerekeptatroomtemperature(21---22◦C)and40---60% relativehumidity ona 12/12-hlight/dark cycle andwere fedwithstandard pellet diet andwater adlibitum.After approvalbytheLocalEthicsCommitteefor Animal Exper-iments at our faculty, the study was carried out in the MultidisciplinaryLaboratory of Animal Experiments. Anes-thesiawasprovidedwith50mg/kgketamineand10mg/kg xylazinehydrochlorideadministeredintraperitoneally(ip). Afteranesthesia,theanimalsweredividedintofourgroups.
Group I (Sham, n=7): After laparotomy, the left and
right renal pedicles were exposed at the 65th minute of anesthesia,andratswerekeptunderanesthesiafor130min withnootherintervention.
GroupII(IR,n=7):After60minofischemia,theclamp wasremovedandreperfusionofthekidneyswasallowedfor 24h.
Group III (IR+dexmedetomidine, n=7): After 60min
of ischemia, the clamp was removed and 100g/kg dexmedetomidine(Precedex100g/2mL,Abbott Laborato-ries,IL,USA) wasadministeredip,and reperfusionofthe kidneyswasallowedfor24h.
GroupIV(IR+RIPC+dexmedetomidine,n=7):
Follow-ing a laparotomy, after 5min of RIPC, and a subsequent 60min of renal ischemia, the clamp was removed and 100g/kgdexmedetomidine(Precedex100g/2mL,Abbott Laboratories)wasgivenandfinally24hofreperfusionwas performed(Fig.1).
ExposingrenalpediclesingroupI,andinitiatingischemia at the65th minute of anesthesiain groups II and III, was intended to synchronize all the groups to the precondi-tioning time of group IV and to standardize the start of theprocedures.Tissuesampleswereobtainedafter24hof reperfusion.
To protect the rats from hypothermia, the operating tablewasheatedwithalampheaterthroughoutthestudy andrectal body temperature wasmeasured with aprobe and maintained at 3737.5◦C. Hourly subcutaneous saline
solution,at 3mL/kgdosage, wasadministeredtoprevent dehydration. During the waiting time, the abdomen was closedwithamoiststerilepadandsurgicalforceps. Inall groups, the left kidneys were removed under anesthesia for histomorphological analyses and the rats were sacri-ficedbyacardiacpunctureexsanguinationattheendofthe study.Thekidneyswerefixedin10%bufferedformalinand embeddedinparaffinwax,cutat4---5m,andstainedwith hematoxylin and eosin for histological studies using light microscopy.
RenalIRmodel
Therightandleftrenalpedicleswereexposedafter laparo-tomy. Total renal ischemia in the left and right renal pedicles was maintained with atraumatic microvascular clampcompression.Adequateocclusionwasconfirmedbya lackofpulsationintherenalpediclesandpresenceofpallor inthekidneys.Aftertheischemicperiod,themicrovascular clampswereremovedandreperfusionoccurred.
RIPCmodel
ForthetourniqueteffectofRIPC,amethodthathasbeen showntobeeffectivebyperfusionscintigraphyandalaser meter wasused.12,13 Forthispurpose, thelefthindleg of theratwasboundwithanelasticbandage(1cmwideand 30cmlong)atthegroin,applyingpressureallaround.Three cycles of 10min of ischemia wereperformed followed by 10minofreperfusion(65mintotal).Thecessationofblood flow wasconfirmedusinga lasercurrent meter(Laser Flo BPM2,Vasamedic,USA).
Histomorphologicalevaluationofrenaltissue
Renal tissue sections after IR were evaluated by light microscopybytwohistologistsblindedtotheanimalgroups intermsofstructuralchangesinproximaltubules(tubular atrophy,loss oftubularbrush border,vacuolization, tubu-lar dilatation, cast formation), mononuclear cells (MNCs) infiltration,interstitialstructuralchanges,renalcorpuscle morphology,andnecroticandapoptoticcells.
The cross-sectional images were scored semi-quantitatively in terms of tubulointerstitial damage. Scoringwasconductedasfollows:0=notatall,1=0---25%, 2=26---45%,3=46---75%,and4=76---100%.14
Immunohistochemicalmethods
Kidneytissueswerefixedin10%bufferedformaldehyde,and after routine histological follow-up procedures, paraffin-embeddedkidneytissueswerecutinto3-mthicksections with a microtome and collected on poly-l-lysine-coated slides.
Samples were stored in the oven at 60◦C for 12h. Then, a rat-specific anti-caspase-3 monoclonal antibody (RB-10287-R7 Labvision)wasusedtoassess anti-caspase-3 immunoreactivity.
sectionsweretreatedwithanti-caspase-3antibody at4◦C overnightandthenincubatedwithabiotinylatedsecondary antibody for 30min. Afterapplication of the Vector Elite ABC kit (Vector Laboratories Inc., Burlingame, USA), the antibody---biotin---avidin---peroxidasecomplexwasvisualized using 0.02% 3,3′-diaminobenzidine solution. Following counterstaining with Mayer’s hematoxylin, image analysis wasperformed.
Thepositivestainingratewasevaluatedusingan indica-torofsemi-quantitativescoring (1---4),interms ofdensity anddistribution.
Exclusioncriteria
Ratsinneedofresuscitationwereexcludedfromthestudy.
Statisticalanalysis
The SPSS software (ver. 15.0; SPSS, Chicago, IL, USA) was used for statistical analyses. A Kruskal---Wallis analy-sis of variance was performed to analyze the data. The Mann---WhitneyU-testwasusedforpair-wisecomparisonsof thegroups.Alldataarepresentedasmeans±standard devi-ations.pvalues<0.05wereconsideredtoindicatestatistical significance.
Results
In total, 28 rats were included in the study group. One rat in the IR group died during the reperfusion period, andwasexcluded fromthe study.Histomorphologicaland immunohistochemicalinjuryscoresofthestudygroupsare presentedinTables1and2.
Renalhistomorphologicalinjuryscores
MNC infiltration. Histomorphological injury scores of the Sham group were significantly lowerthan those of the IR group(p=0.01).Injuryscores intheIRgroupwere signifi-cantlyhigherthanintheIR+DexandIR+RIPC+Dexgroups (p=0.04andp=0.04,respectively;Fig.2).
Structural changes in the proximaltubules. Histomor-phologicalinjuryscoresoftheShamgroupweresignificantly lower than those of the IR, IR+Dex, and IR+RIPC+Dex groups(p<0.01,p=0.02,andp=0.02,respectively).TheIR
Table2 Immunohistochemicalinjuryscoresofthegroups.
GroupI(n=7) Sham
0.85±0.37
GroupII(n=6) IR
2.50±0.54
GroupIII(n=7) IR+Dex
1.71±0.75
GroupIV(n=7) IR+RIPC+Dex
1.42±0.53
Dataarepresentedasmean±SS.
Sham
Monon
uclear cell infiltr
ation
1.8
1.6
1.4
1.2
0.8
0.6
0.4
0.2
0 1
IR IR+Dex IR+RIPC+Dex
Figure 2 Mononuclear cell infiltration scores detected by renalhistomorphological examination. *Comparisonof theIR group with the Sham group (p=0.01). =/Comparison of the
IR+DexandIR+RIPC+DexgroupswiththeIRgroup(p<0.05).
groupdisplayedsignificantlyhigherscoresthantheIR+Dex and IR+RIPC+Dex groups (p=0.05 and p=0.05, respec-tively),while nosignificant differencewasfoundbetween theIR+DexandIR+RIPC+Dexgroups(p=1.00;Fig.3).
Glomerularchanges.Histomorphologicalinjuryscoresof theShamgroupweresignificantlylowerthanthoseoftheIR group(p=0.04).TheIRgroupdisplayedsignificantlyhigher scoresthantheIR+DexandIR+RIPC+Dexgroups(p=0.04 andp=0.04,respectively), while nosignificant difference wasfoundbetween the IR+Dex andIR+RIPC+Dex groups (p=1.00;Fig.4).
Totalhistopathologicalinjuryscore.Thetotal histomor-phologicalinjuryscoresoftheShamgroupweresignificantly lower than those of the IR group (p=0.003). Comparison
Table1 Histomorphologicallyinjuryscoresofthegroups.
MCI SCPD CG TSHD
GroupI(n=7) Sham 0.14±0.38 0.0±0.0 0.0±0.0 0.28±0.48
GroupII(n=6) IR 1.0±0.63 1.67±0.82 0.50±0.55 3.83±2.22
GroupIII(n=7) IR+Dex 0.28±0.49 0.71±0.75 0.0±0.0 1.42±1.27
GroupIV(n=7)IR+RIPC+Dex 0.28±0.49 0.71±0.75 0.0±0.0 1.42±1.61
pa 0.04b 0.00b 0.01b 0.008b
Dataarepresentedasmean±SS.
MCI,mononuclearcellinfiltration;SCPD,structuralchangesintheproximaltubules;CG,changesinglomerular;TSHD,totalscoreof histologicaldamage.
a Kruskal---Wallistest.
Sham
T
ub
ular changes
3
2.5
1.5
0.5
0 1 2
IR IR+Dex IR+RIPC+Dex
Figure 3 Tubular change injury scores detected by renal histomorphological examination. *Comparison of the IR, IR+Dex and IR+RIPC+Dex groups with the Sham group (p<0.01). =/ComparisonoftheIRgroupwiththeIR+Dexand IR+RIPC+Dexgroups(p=0.05).
Sham
Glomer
ular changes
1.2
1
0.8
0.6
0.2
0 0.4
IR IR+Dex IR+RIPC+Dex
Figure4 Glomerularchangeinjuryscoresdetectedbyrenal histomorphology.*ComparisonoftheIR groupwith theSham group(p<0.01). =/ComparisonoftheIRgroupwiththeIR+Dex andIR+RIPC+Dexgroups(p<0.05).
of the IR group with the IR+Dex and IR+RIPC+Dex groupsshowedsignificantlyhigherscoresthantheIRgroup (p=0.03 and p=0.05, respectively), while the IR+Dex andIR+RIPC+Dex groupsshowednosignificant difference (p=0.79;Fig.5).
Sham
T
otal histopathological injur
y scores
7
6
5
4
3
2
1
0
IR IR+Dex IR+RIPC+Dex
Figure 5 Total histopathological injury scores detected by renalhistomorphology. *Comparisonofthe IRgroup withthe Shamgroup(p<0.01). =/ComparisonoftheIRgroupwiththe IR+DexandIR+RIPC+Dexgroups(p<0.05).
Sham
Glomer
ular changes
3.5
3
2.5
2
1
0 1.5
0.5
IR IR+Dex IR+RIPC+Dex
Figure6 Renalimmunohistochemicalscoring.*Comparisonof theIRgroupwiththeShamgroup(p<0.01).=/Comparisonofthe IRgroupwiththeIR+DexandIR+RIPC+Dexgroups(p=0.01).
Immunohistochemicalinjury score. Immunohistochemi-calstainingscoresoftheIRgroupweresignificantlyhigher than in theSham group(p=0.001). Nostatistically signif-icant difference was found between the IR and IR+Dex groups(p=0.06).
In the comparison of injury scores between the IR+RIPC+Dex and IR groups, those of the IR+RIPC+Dex groupweresignificantlylower(p=0.01).Theinjuryscores of the IR+Dex and IR+RIPC+Dex groups did not differ (p=0.47;Fig.6).
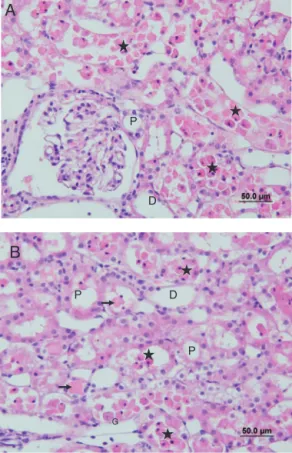
Nocellinfiltrationorlossofbrushborderwasobservedin thesectionsoftheShamgroup(Fig.7AandB).However,in
B
D G
P
P
Group I
P G
G P
A
A
D P
B
D
G
P P
Figure8 (AandB)SectionsoftheIRgroup.G,glomerular;P, theproximaltubule;D,thedistaltubule,( )accumulation ofproteinaceousmaterialintubules,(⋆)pouredintothelumen oftubularepithelialcells.
theIRgroup,peritubularMNCinfiltration,moreprominent inthecorticalarea,andlossofbrushborderoftheproximal tubulecells,tubularatrophy,tubulardilation,and vacuola-tionwereobserved.Insomeofthetubules,proteinaceous materialaccumulation,togetherwithcasteformation and celldebrisinthetubulelumen,wereobserved(Fig.8Aand B).
In the IR+Dex group, loss of the brush border of the tubulecells,tubularatrophy,tubulardilatation, vacuoliza-tion, and proteinaceous material accumulation and cell debrisinthetubulelumenwereobserved,albeittoalesser extentthanintheIRgroup(Fig.9AandB).
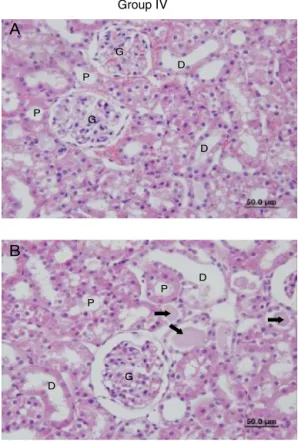
Compared withthe IR group, the IR+RIPC+Dex group displayedtubularatrophy,tubulardilatation,vacuolization, proteinaceousmaterialaccumulationandcelldebrisinthe lumenof thetubules, andloss ofthebrush borderof the tubulecells,albeittoalesserextent. However,compared withtheIR+Dexgroup,tubularchangeswerelessmarked (Fig.10AandB).
Immunohistochemicalstainingintensitywasincreasedin theactivecaspase-3-positivecellsoftheIRgroupcompared withthe Sham group,while it was decreased in thecells oftheIR+DexandIR+RIPC+Dexgroupscomparedwiththe IRgroup.Stainingintensityintheactivecaspase-3-positive cells ofthe IR+RIPC+Dex groupwasdecreased compared withtheIR+Dexgroup(Fig.11).
Group III
A
G P
P
D
B
Figure 9 (A and B) Sections of the IR+Dex group. G, glomerular; P, the proximal tubule; D, the distal tubule, ( )accumulation ofproteinaceous material to be reduced comparedtoothergroups.
Discussion
Acuterenal failure occurring asa result of ischemiamay be due to hypotension, hypovolemia, and hypoperfusion secondarytodehydrationaswellasIRdamageinmajor car-diothoracic,vascular,andtransplantsurgeries.15---18IRinjury isone ofthe mostcommoncauses of perioperativeacute renalfailure.18
MethodssuchasRIPCandpharmacologicalconditioning withdexmedetomidine,whichareusedtopreventortreat renalIRinjury,havebeenshowntohavepositiveeffectsin termsofIRinjuryinmanypreviousstudies.11
Inaliteraturesearch,wefoundnostudythathad eval-uatedthe effects of combiningthese twomethods for IR injury.Thisexperimentalstudy,usingaratmodelofrenal IR,comparedtheeffectsof usingdexmedetomidinealone orRIPCincombinationwithdexmedetomidineagainstrenal apoptosis,assessing usingcaspase-3 immunoreactivityand histopathologicalinjuryscores.
Group IV
A
B
D G
P
P
G
D
D
P P
D G
Figure 10 (A and B) Sections of the IR+RIPC+Dex group. G, glomerular; P, proximal tubule; D, distal tubule, and ( )accumulationofproteinaceoustobereducedcompared toother.
combined with RIPC group, suggesting that apoptosis, a majorpathwayofIRinjury,couldbereducedorprevented bythiscombination.
Variousperiods of ischemiaand reperfusion wereused inrenal IRinjury modelsinmanystudies.19---22 Thecritical ischemic period is dependent onthe organ,and ischemia lastingmorethan5minforthebrain,and15---20minforthe liverandkidneymaycauseneuronaldeathandinfarction.23 Williams et al.20 investigated the effects of IR injury in bloodandtissuesamplesobtainedafterreperfusion follow-ing 45min of renal ischemia, and reported that renal IR injuryoccurred earliest,atthefourth hourandpeakedat 24h.
Organ-protectiveeffectsofdexmedetomidineagainstIR damagehavebeenshowninmanytissues,suchasthebrain, heart, and kidneys.24---27 The effects of dexmedetomidine inratrenalIRinjurywereinvestigatedbyKoco˘gluetal.19 Theseresearchersreportedasignificantdecreaseinscores for histopathological injury, detected at the 45th minute after ip administration of 100g/kg dexmedetomidine at the beginningof reperfusion. Inour study,withthe same dose of dexmedetomidine administered at the beginning of reperfusion, a renoprotective effect was achieved, as evidencedbysignificantreductionsinthehistologicalinjury scores.Thisrenoprotectiveeffectwasfoundnotonlyduring theearly periodafterreperfusioninjurybut itcontinued, evenat24h,whichwasconsideredthepeakofIRinjury.20
Althoughthemechanismunderlyingtheprotectiveeffect ofdexmedetomidineinrenalIRisunclear,itisconsidered to increase renal blood flow and glomerular filtration by reducingthereleaseofnoradrenaline.28
Villelaetal.29reportedthatlow-dosedexmedetomidine administration in anesthetized dogs reduced the urinary osmolality and plasma vasopressin level and caused free-water diuresis. In patients who had no renal disease but
A
B
C
D
experiencedthoracicsurgery, byadministeringaninfusion ofdexmedetomidine,Frumentoetal.30showedan improve-mentinrenalfunction,includingurineflowandglomerular filtrationinthepostoperativeperiod.
One of the most likely mechanisms of the action of dexmedetomidineisprotectingthekidneybyinhibitingthe surgicalstressresponseandpreventingadrenergic system-mediated vasoconstriction.31---34 It may also increase renal arterialvasodilationthroughdirectvasculareffects.19 PKC has been reported to play an important role in ischemic preconditioning and to open sarcolemmal and mitochon-drialATP-dependentK+channelsbystimulatingintracellular
transductionpathwaysandinducingsynthesisofprotective cellularproteins.Inastudyofalternative signal transduc-tionpathways, alpha 2B receptoragonists were shown to stimulatePKCactivityandtheproductionofinositol triphos-phateinthedistalrenalcollectingtubulecells,suggesting thatalpha2agonists mimiccellprotectionbyIPC.35,36 Gu etal.18investigatedthemechanismofactionof dexmedeto-midine in vitro with a stabilized human renal proximal tubule cell culture deprived of both oxygen and glucose. They reported both a significant increase in phospho-Akt expression in cultured tubular cells after treatment with dexmedetomidine, dependent on the dose, and an alpha-2 adrenoreceptor effect. The phosphoAkt path-wayensures cellviability by inhibitingcaspase-controlled intrinsic apoptotic pathways through phosphorylation of proapoptoticBcl-2,whichtriggerscelldeath,and upregula-tionofanti-apoptoticBcl-2andBcl-XLexpression.
The neuroprotective effect of dexmedetomidine has beenreportedtobearesultoftheincreaseinanti-apoptotic Bcl-2andMdm-2expression;thisincreasehasbeen associ-atedwithadecreaseinthelevelsofproapoptoticcaspase-3 and Bax.37 The Akt pathway is criticalin recoveringfrom renalIR.Inthisstudy,asan indicatorofapoptosis, active caspase-3 immunoreactivity was evaluated. Activation of caspase-3isthefinalstepofapoptosis,whichiscommonto thetwomajorpathwaysofapoptosisandadefinitive indi-cator of cell death. Dexmedetomidine administrationwas showntodecreaseactivecaspase-3immunoreactivity,but notsignificantlyso(p=0.06),comparedwithIRinjury.
This statistically non-significant difference could be explainedbythesmallnumberofstudysubjects.Ischemic preconditioningisamethodappliedmechanicallyor phar-macologically prior to target organ ischemia to reduce the level of subsequent IR injury. The aim in ischemic preconditioningistoapplyischemiaandreperfusionto tar-get organs in short intervals, to ensure that the target organ(s)cantolerateischemiawell. Highenergydemands andtheintensemicrovascularnetworkofthekidneysmake them vulnerabletoIRinjury,which is considered amajor causeofkidney damagein renalarterystenosis andrenal microvascular surgery. Renal IR injury is the major cause ofcardiovascularmorbidityandmortality,andisassociated withpost-transplantationdelayingraftfunction,andrenal injuryoccurringincardiacandaorticsurgeryandpost-shock renalinjury.1---4,38,39
Bothexperimentalandclinical studiesinthe literature show that distant organ IPC may be protective for the kidney.40,41Similartoourstudy,Weveretal.40investigated theeffectof hindleg DIPConrenalIRinjury.Differently, these authors compared the effect of administering DIPC
eithercontinuouslyorperiodically,andalsotooneor two extremities.AlthoughtheyperformedthreecyclesofDIPC, theyusedI/Rperiodsof4/4minandinvestigatedthe even-tual effects of 25min of ischemia. They reported that molecule-1 expression, indicating renal tubular and renal injury,decreasedsignificantlyinthegroupwiththreecycles ofI/R;moreover,thisprotectionwasnotrelatedto adeno-sine,oneofthekeyelementsinI/Rinjury.Theunderlying mechanismof DIPCanditstransductionpathways arenot yetcompletelyunderstood.Bothneurogenicpathwaysand biochemicaltransmittersmayplayrolesinthemechanism ofDIPC.42 These mechanismsmayvary, depending onthe targetorgan and appliedpreconditioning protocol. In the myocardialischemiamethodsusingrenalDIPC, expression ofNF-BproteinfollowedbytheopeningofK+ATPchannels
havebeenreportedtobeimportant.43
AlthoughrenalIRinjuryisacommonandimportant clin-icalproblem,strategiestoreduceIRinjuryareinsufficient andnewtreatmentsareneeded.Intheliterature,noreport ofbothpharmacologicalandmechanicalprotectioninrenal IRinjuryinratscouldbefound.
Thus,twodifferentmethodsusedinratrenalIRinjury, dexmedetomidine, widely reported to be effective, and DIPC,thathasbeenshowntobeeffectiveinfewstudies,11 werecombinedandcompared.Similartodexmedetomidine, usingdexmedetomidineandDIPCincombinationprevented histopathological injury and improved IR injury scores, excepttubularchangescores, tolevelsclosetotheSham group. At the same time, significant decreases in active caspase-3 immunoreactivity compared with the IR group suggested that using dexmedetomidine and DIPC in com-binationmight preventapoptosis.Using dexmedetomidine alonedecreased activecaspase-3immunoreactivity,albeit non-significantlyso,whichsuggeststhatthesetwomethods operateviasimilarpathways.Thesetwoprotectivemethods arelikelytoincreasetheeffectofeachother.
Inourstudy,xylazine,ananestheticagenthavingalpha 2-agonistactivity,andketamine42suggestedtohavenegative effectsonIRinjury,wereused.Histopathologicalscoresand activecaspase-3immunoreactivitywerenormalintheSham group,whichsuggeststhatketaminehadnonegativeeffect onourresults.
WedidnotshowtheeffectofDIPCaloneonapoptosis, whichplaysakeyroleinthemechanismofIRinjury;thisis alimitationofthepresentstudy.Otherlimitingfactorsare thatoxidativestressandinflammatorymediators,whichare alsoresponsibleforIRinjury,andtheneurogenicpathway, werenotexamined.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OjoAO,WolfeRA,HeldPJ,etal.Delayedgraftfunction:risk factorsandimplicationsforrenalallograftsurvival. Transplan-tation.1997;63:968---74.
3.OjoAO,HeldPJ,PortFK,etal.Chronicrenalfailureafter trans-plantationofanonrenalorgan.NEnglJMed.2003;349:931---40.
4.Nigwekar SU, Kandula P, Hix JK, et al. Off-pump coronary arterybypasssurgeryandacutekidneyinjury:ameta-analysis of randomized and observational studies. Am J Kidney Dis. 2009;54:413---23.
5.CollardCD,GelmanS.Pathophysiology,clinicalmanifestations, andpreventionofischemia---reperfusioninjury.Anesthesiology. 2001;94:1133---8.
6.Tsutsui H, Sugiura T, Hayashi K, et al. Moxonidine pre-ventsischemia/reperfusion-inducedrenalinjuryinrats.EurJ Pharmacol.2009;603:73---8.
7.Yazıcı P, Alizadehshargh S,Akdogan G. Apoptosis: regulatory molecules,relationshipswithdiseasesandapoptosisdetection methods.TurkiyeKlinikleriJMedSci.2009;29:1677---86.
8.Faubel S, Edelstein CL. Caspases as drug targets in ischemicorganinjury.ImmuneEndocrMetabolDisord.2005;5: 269---87.
9.NoiriE,GailitJ,ShethD,etal.CyclicRGDpeptidesameliorate ischemicacuterenalfailureinrats.KidneyInt.1994;46:1050---8.
10.Friedewald JJ,RabbH. Inflammatorycells inischemicacute renalfailure.KidneyInt.2004;66:486---91.
11.TapuriaN,KumarY,HabibMM,etal.Remoteischemic precon-ditioning:anovelprotectivemethodfromischemiareperfusion injury---areview.JSurgRes.2008;150:304---30.
12.Kanoria S,Jalan R,Davies NA,et al.Remoteischaemic pre-conditioningofthehindlimbreducesexperimentalliverwarm ischaemia---reperfusioninjury.BrJSurg.2006;93:762---8.
13.Duru S, Koca U, Oztekin S, et al. AntithrombinIII pretreat-ment reduces neutrophil recruitment into lung and skeletal muscle tissues in the rat model of bilateral lower limb ischaemia and reperfusion: a pilot study. Acta Anaesthesiol Scand.2005;49:1142---8.
14.Feng L, Xiong Y, Cheng F, et al. Effect of ligustrazine on ischemia---reperfusioninjuryinmurinekidney.TransplantProc. 2004;36:1949---51.
15.ThadhaniR,PascualM,BonventreJV.Acuterenalfailure.NEngl JMed.1996;334:1448---60.
16.BrezisM,RosenS,SilvaP,etal.Renalischemia:anew perspec-tive.KidneyInt.1984;26:375---83.
17.Caron A, Desrosiers RR, Beliveau R. Kidney ischemia reper-fusionregulatesexpressionanddistributionoftubulinsubunits, beta-actinandrhoGTPasesinproximaltubules.ArchBiochem Biophys.2004;431:31---46.
18.GuJ,PamelaS,HailinZ,etal.Dexmedetomidineprovides reno-protection against ischemia---reperfusion injury in mice. Crit Care.2011;15:R153.
19.Koco˘glu H, OzturkH,Ozturk H,et al. Effect of dexmedeto-midine on ischemia-reperfusion injury in rat kidney: a histopathologicstudy.RenFail.2009;31:70---4.
20.WilliamsP,LopezH, BrittD,etal. Characterizationofrenal ischemia---reperfusioninjuryinrats.JPharmacolToxicol Meth-ods.1997;37:1---7.
21.Fujii T,Takaoka M,MuraokaT, et al.Preventiveeffectof l -carnosineonischemia/reperfusion-inducedacuterenalfailure inrats.EurJPharmacol.2003;474:261---7.
22.Hussein Ael-A, ShkeirAA, SarhanME, et al. Effects of com-bined erythropoietin and epidermal growth factor on renal ischaemia/reperfusioninjury:arandomizedexperimental con-trolledstudy.BJUInt.2011;107:323---8.
23.Jaeschke H,Farhood A. Kupffercell activationafterno-flow ischemia versus hemorrhagic shock. Free Radic Biol Med. 2002;33:210---9.
24.SandersRD,MazeM.Alpha2-adrenoceptoragonists.CurrOpin InvestigDrugs.2007;8:25---33.
25.BillingsFT,ChenSW,KimM,etal.Alpha2-adrenergicagonists protectagainstradiocantrast-inducednephropathyinmice.Am JPhysiolRenalPhysiol.2008;295:741---8.
26.Ma D, Hossain M, Rajakumaraswamy N, et al. Dexmedeto-midine produces its neuroprotective effect via the alpha 2A-adrenoceptorsubtype.EurJPharmacol.2004;502:87---97.
27.Kuhmonen J,Pokorny J, MiettinenR, et al. Neuroprotective effectsof dexmedetomidinein thegerbilhippocampusafter transientglobalischemia.Anesthesiology.1997;87:371---7.
28.TaodaM,AdachiYU,UchihashiY,etal.Effectof dexmedeto-midine onthereleaseof [3H]-noradrenaline from ratkidney cortex slices: characterization of alpha2-adrenoceptor. Neu-rochemInt.2001;38:317---22.
29.VillelaNR,NascimentoPVN,CarvalhoLR.Effectsof dexmedeto-midineonrenalsystemandonvasopressinplasmalevels. Exper-imentalstudyindogs.RevBrasAnestesiol.2005;55:429---40.
30.FrumentoRJ,LogginidouHG,WahlanderS,etal. Dexmedeto-midineinfusionisassociatedwithenhancedrenalfunctionafter thoracicsurgery.JClinAnesth.2006;18:422---6.
31.KulkaPJ, Tryba M,Zenz M. Preoperative alpha 2-adrenergic receptoragonistspreventthedeteriorationofrenalfunction aftercardiacsurgery:resultsofarandomized,controlledtrial. CritCareMed.1996;24:947---52.
32.Helbo-HansenS,FletcherR,LundbergD,etal.Clonidineandthe sympatico-adrenalresponsetocoronaryarteryby-passsurgery. ActaAnaesthesiolScand.1986;30:235---42.
33.KulkaPJ,TrybaM,ZenzM.Dose---responseeffectsofintravenous clonidine on stress response during induction of anesthe-sia in coronary artery bypass graft patients. Anesth Analg. 1995;80:263---8.
34.FlackeJW,BloorBC,FlackeWE,etal.Reducednarcotic require-mentbyclonidinewithimprovedhemodynamicandadrenergic stabilityinpatientsundergoingcoronarybypasssurgery. Anes-thesiology.1987;67:11---9.
35.GesekFA.Alpha2-adrenergicreceptorsactivatephospholipase Cinrenalepithelialcells.MolPharmacol.1996;50:407---14.
36.O’RourkeB.EvidenceformitochondrialK+channelsandtheir roleincardioprotection.CircRes.2004;94:420---32.
37.Engelhard K, Werner C, Eberspacher E, et al. The effect of the alpha 2-agonist dexmedetomidine and the N-methyl-d-aspartate antagonist S(+)-ketamine on the expression of apoptosis-regulating proteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg. 2003;96: 524---31.
38.Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344:431---42.
39.SchrierRW,WangW.Acuterenalfailureand sepsis.NEnglJ Med.2004;351:159---69.
40.WeverKE,MentingTP,RoversM,etal.Ischemicpreconditioning intheanimalkidney,asystematicreviewandmeta-analysis. PLoSONE.2012;7:e32296.
41.Venugopal V, Laing CM, Ludman A, et al. Effect of remote ischemicpreconditioningonacutekidneyinjuryinnondiabetic patientsundergoingcoronaryarterybypassgraftsurgery:a sec-ondaryanalysisof2smallrandomizedtrials.AmJKidneyDis. 2010;56:1043---9.
42.Curtis FG,Vianna PT, VieroRM. Dexmedetomidineand S(+)-ketamineinischemiaandreperfusioninjuryintheratkidney. ActaCirBras.2011;26:202---6.