Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
article
Transanal
minimally
invasive
surgery
(TAMIS)
for
local
excision
of
selected
rectal
neoplasms:
efficacy
and
outcomes
in
the
first
11
patients
Gustavo
Sevá-Pereira
∗,
Luis
Gustavo
Capochin
Romagnolo,
Joaquim
José
de
Oliveira
Filho,
Ricardo
Bolzam-Nascimento,
Sandra
Pedroso
de
Moraes,
Gabriela
Domingues
Andrade
Ribeiro
MárioGattiCityHospital,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received9April2014 Accepted15May2014 Availableonline14June2014
Keywords: Rectalneoplasm Localexcision TAMIS
a
b
s
t
r
a
c
t
Disposablesingle-portsurgerydeviceshavebeenusedfortransanal minimallyinvasive surgery(TAMIS)withbenefits,whencomparedtolocalresectionandtransanalendoscopic microsurgery(TEM).
Objective:Toshowoutcomesanddetailsofthetechnique.
Method:Aseriesofpatientswithindicationforlocalresectionofrectaltumorswere sub-mittedtosurgeryusingtheTAMISplatform.
Results:ElevenpatientshavebeensubmittedtoTAMIS.Distancefromanalvergewasfrom 1.5to8cmandmaximum tumordiameterwas6cm. Initialdiagnosisofadenomawas themostfrequentindicationforresection.Onepartialdehiscencewastheonly compli-cationseen.Minimalsetuptime,lowcostandthepossibilityofusingregularlaparoscopic instrumentsmakeTAMISagoodoptionfortransanalresection.Theresultsofthis tech-niqueareencouraging,concerningthefeasibility,maneuverability,upfrontcost,setuptime, resectabilityandcomplicationrate.Becauseofitssimplicityandsimilaritywith conven-tionallaparoscopic surgery,it canbe learnedeasily.Although atthe presenttime the appropriateuseoflocalexcisionisstillunderdebate,TAMISisatechniquethatstillexpects alotofgrowingandmuchremainstobelearned.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](G.Sevá-Pereira).
http://dx.doi.org/10.1016/j.jcol.2014.05.002
Cirurgia
Trans-anal
Minimamente
Invasiva
(CTAMI)
para
excisão
local
de
neoplasias
retais
selecionadas:
eficácia
e
desfechos
nos
primeiros
11
pacientes
Palavras-chave: Neoplasiaretal Excisãolocal CTAMI
r
e
s
u
m
o
DispositivoscirúrgicosdeportaúnicadescartáveistêmsidoutilizadosparaaCirurgia Trans-analMinimamenteInvasiva(CTAMI)combenefícios,quandocomparadoscomressecc¸ão localemicrocirurgiaendoscópicatrans-anal(MET).
Objetivo: Apresentarosdesfechosedetalhesdatécnica.
Método: Umasériedepacientescomindicac¸ãopararessecc¸ãolocaldetumoresretaisfoi tratadacirurgicamentepelaplataformaCTAMI.
Resultados: Onzepacientesforamtratados porCTAMI.Adistânciaacontardamargem analvarioude1,5até8cm,eodiâmetromáximodotumorfoi6cm.Umdiagnóstico ini-cialde adenomafoia indicac¸ãomaisfrequenteparaaressecc¸ão.A únicacomplicac¸ão ocorridafoiumadeiscênciaparcial.Mínimotempoparapreparac¸ão,baixocustoea pos-sibilidadedousodeinstrumentoslaparoscópicosconvencionaisfazemdeCTAMIumaboa opc¸ãoparaaressecc¸ãotrans-anal.Osresultadosdessatécnicasãoanimadores, noque dizrespeitoàexeqüibilidade,manobrabilidade,custosiniciais,tempodepreparac¸ão, res-sectabilidadeepercentualdecomplicac¸ões.Grac¸asàsuasimplicidadeesemelhanc¸acom acirurgialaparoscópicaconvencional,CTAMItemumafácilcurvadeaprendizado.Embora atualmenteaindasejamotivodediscussãoousoapropriadodaexcisãolocal,CTAMIéuma técnicaqueaindaprovavelmenteaindacrescerámuito–ehámuitoaseraprendido.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Asscreeninghassubstantiallyincreasedtheearlydiagnosisof tumors,thereisaneedforlocaltreatmentsthatare oncolog-icallyequivalenttoradicalsurgery,butsaferandfunctionally superior.1Localexcisionofrectaltumorshasbeenperformed
sinceearly1800,whenLisfrancdescribedalocalresectionfor rectalcarcinoma.2
Transanalendoscopicmicrosurgery(TEM) wasdescribed initially by GerhardBuess in 1983 to provide a means for removingbenignlesionsofmidandupperrectumnoteasily accessiblebyconventionalmethods.3
Comparedtolocalexcision,TEMprovidessuperior qual-ity of resection, decreased localrecurrence, and improved survival, particularly amongpatients with adenomas4 and
histologicallyfavorablestageIrectalcancer.3,5 Inlong-term
follow-up,TEMexcisionofrectaltumorshasproventobesafe andeffective,withmorbidityandmortalitysimilartothatof conventionaltransanalexcision.6,7
However,although TEMhas been in use formore than 20years,ithasbeenslowtobecomeuniversallyadoptedby colorectalsurgeons,partlyduetoalonglearningcurve,but alsobecauseofthesignificantcostofthehighlyspecialized equipment.2–4
Astechnologycontinuestoundergorapidevolution,the minimallyinvasivesurgeons’skillsdevelopquickly.Recently theNaturalOrificeTransluminalEndoscopicSurgery(NOTES) hasprovidedtechnologyfordevelopingpermanentand dis-posableequipmentandinstrumentsthatcanbeusedforboth abdominaland pelvicoperations throughasingle incision. These devices have facilitated a wide range of operations,
includingbariatricandallsortsofcolorectalsurgeriesusinga single-incisionmutiportdevice.
Theworkinganglesinsingle-accesslaparoscopyare essen-tially identical to those used inTEM. Therefore, crossover existsbetweentheskillsetnecessarytoperformsingle-port laparoscopyandTEM.TheconsiderableupfrontcostofTEM instrumentation,however,remainsasignificantbarriertoits widespreaduse.
Transanal minimally invasive surgery(TAMIS) has been describedfirstbyDr.Attalah,Dr.LarachandDr.Albert,from Orlando,FL,3whoreportedthistechniquetobeeffectiveand
safeforearlyrectalcancerandadenomas,withexcellent oper-ativefieldvisibilityandnottechnicallydifficult.Astheauthors say,theTAMISisa“giantleapforward”whencomparedto TEM.Mountingiseasieranddemandslesstimepriorto begin-ningsurgery;asitisadisposabledevice,thecostismuchlower andmanipulationismuchmorecomfortablethanTEM.
Recently,EthiconTM(Cincinnati,OH)presentedtheirSingle
SiteTM(SSL)deviceforNOTES.Ithasbeendesignedfor
single-incisionlaparoscopicabdominalsurgeries,buthasbeenalso usedsuccessfullyforTAMISresection.8Alittlelater,GelPoint
PathTMhasbeenlaunchedbyAppliedMedical(RanchoSanta
Margarita,CA),specificallyforTAMIS.
Methods
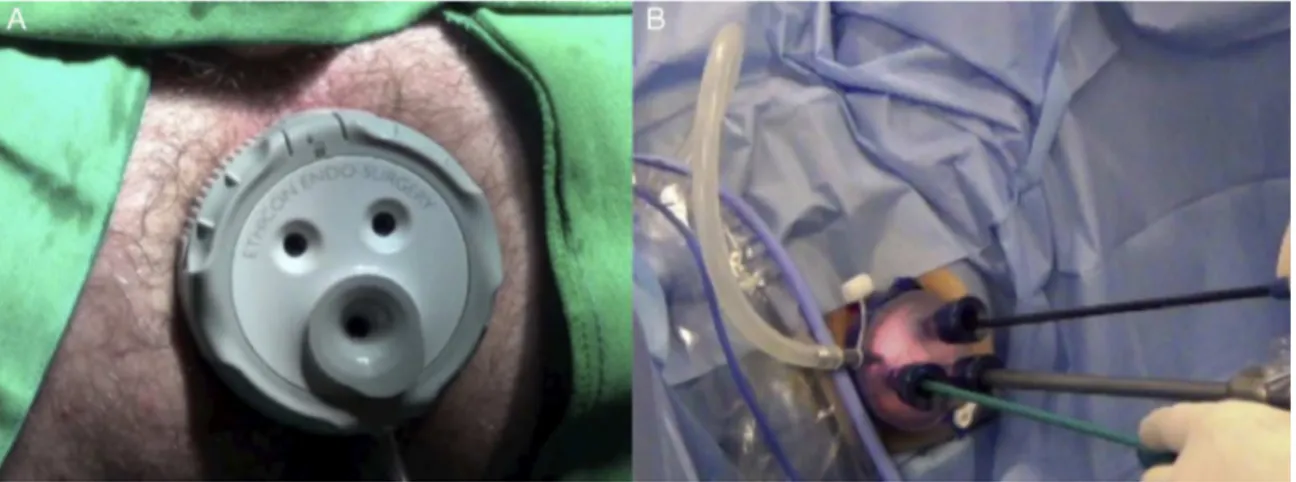
Fig.1–Portsplaced.A,SSLTM;B,GelPointPathTM.
were given the option to undergo conventional surgery. Patientswithknownmalignantlesionswereexcluded.
FromAugust2010toAugust2013alldataofpatients under-goingthissurgicaltechnique,usingbothSSLTMandGelPoint
PathTM, was collected prospectively. Follow-up was for up
to24months.Allpatientshaddigitalrectalexaminationor colonoscopypostoperativelly.Patients undergoingthe tech-niqueofTAMISpatientshadadenomaswithdysplasiaoflow and high grade,onlyoneofthem had a scarafter incom-plete endoscopicresection, and one asadenocarcinoma in situ.Patients havingpreviousdiagnosis ofadenocarcinoma underwenttransrectalultrasoundtoevaluatedepthandnodal invasion.
Surgicalprocedureswereperformedatatertiary-care Hos-pital.Allpatientswereadministeredgeneralanesthesia.To performtheprocedurethepatient’spreferablepositionisone inwhichthelesionisintherectumwallthatisclosertothe operatingtable.Whenthelesionisintheposteriorrectalwall, thepatientisinlithotomyposition,withlegsup;whenthe tumorisintherightlateralwall,thepatientcanbeturnedwith therightsidedown.Althoughnotmandatory,thisisthemost comfortablewaytoperformthisprocedure.Mechanicalbowel preparationwasadministeredpreoperativelyandreceiveda single3g-doseofintravenousUnasyn®(Pfizer,Brazil),at
anes-theticinduction.
Afterinsertionofthetransanalport(eithertheSSLTMor
GelPointPathTM,Fig.1),thepneumorectumwasgainedusing
CO2insufflationwithaninitialpressureseta12mmHgand
flowset at40mmHg per minute.Standard straight laparo-scopicinstruments were used. Full-thickness excision was performed on all lesions aiming a 1cm minimum nega-tivemargin(Fig.2).Alldefectswereclosedcompletelywith absorbablesuturematerial(Fig.3).
Patients had a planned discharge for the next day of surgery.
Results
Eleven patients aged 50–86 years (average 67.4 y) under-wentTAMISresectionofrectallesions(Table1).Theaverage distancefrom anal vergewas47.7mm(15–80mm)and the
mean tumor diameter measured by pathology was 35mm (10–60mm). Eightpatients had an initialdiagnosis of ade-noma. Onepatient had a previousendoscopic resectionof a T1 adenocarcinoma (case C), made with mucosectomy
Fig.2–AdenomawithcentralfocalpT1aftermonopolar marking.
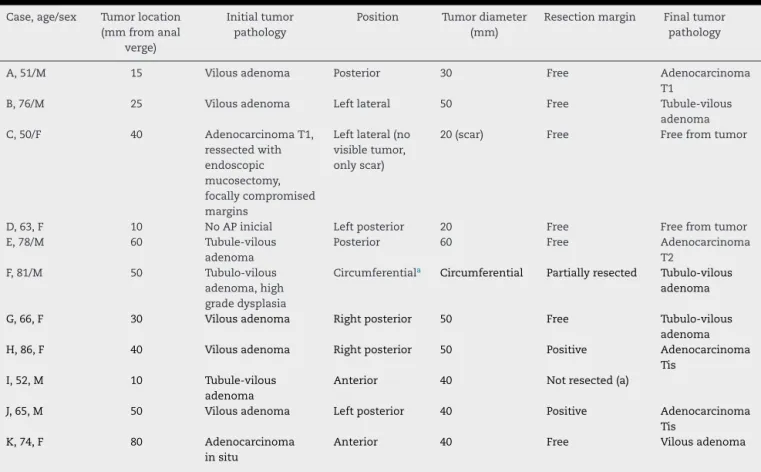
Table1–Tumorcharacteristics.
Case,age/sex Tumorlocation (mmfromanal
verge)
Initialtumor pathology
Position Tumordiameter (mm)
Resectionmargin Finaltumor pathology
A,51/M 15 Vilousadenoma Posterior 30 Free Adenocarcinoma T1
B,76/M 25 Vilousadenoma Leftlateral 50 Free Tubule-vilous adenoma C,50/F 40 AdenocarcinomaT1,
ressectedwith endoscopic mucosectomy, focallycompromised margins
Leftlateral(no visibletumor, onlyscar)
20(scar) Free Freefromtumor
D,63,F 10 NoAPinicial Leftposterior 20 Free Freefromtumor E,78/M 60 Tubule-vilous
adenoma
Posterior 60 Free Adenocarcinoma T2
F,81/M 50 Tubulo-vilous adenoma,high gradedysplasia
Circumferentiala Circumferential Partiallyresected Tubulo-vilous adenoma
G,66,F 30 Vilousadenoma Rightposterior 50 Free Tubulo-vilous adenoma H,86,F 40 Vilousadenoma Rightposterior 50 Positive Adenocarcinoma
Tis I,52,M 10 Tubule-vilous
adenoma
Anterior 40 Notresected(a)
J,65,M 50 Vilousadenoma Leftposterior 40 Positive Adenocarcinoma Tis
K,74,F 80 Adenocarcinoma insitu
Anterior 40 Free Vilousadenoma
a Afterpositioningthepatientthedevicecouldnotbepositionedandthetechniquewaschangedtostandardlocalresection.
techniqueandhadpositivemargins.Thispatientwaseligible forscarresectionwithlargermargins.Notumorwasfoundby thepathologistinthispatient.
Onepatient(caseD)couldnotbeoperatedbythedescribed technique.ExpansionoftheSSLTMretractorintorectallumen
wasnotpossible.Thesizeoftheprostateoccupyingtherectal lumenwasprobablyresponsiblefornotallowingthedeviceto opentowardtheanteriorrectalwallandthusaconventional localexcisionwasusedinstead.
Anotherpatient(caseF)wasunderevaluatedduring pre-operativecolonoscopy,asthetumorwasdescribedaslateral, andduringsurgeryitshowedascircumferential.Inthiscase itwas resectedpartially,onlyforensuringpathologic diag-nosis, and furthertaken to laparoscopicanterior resection withcolonic pouch-analanastomosis.Pathologic specimen showedtubulo-vilousadenoma.
Setuptimevariedfrom1to45min(average9.8min),and totalsurgerytimewasfrom38to80min(average51min).Two ofthetenresectedspecimenscontainedearlystage adenocar-cinomas.Allmarginswerefree(Table2).
Oncetheresectionwascompleted,thedefectwas approx-imatedwithintraluminalsuture.Inninepatientstheoption wastoplacemetallicclipsonbothedgesofthesuture,instead oftying.Onepatienthadtiesdoneonthesuture’sedges.
Allpatientsstayedovernightandweredischargedthenext morning.
Asthe onlyknowncomplication,onepatienthada par-tialdehiscenceofthesuturelineindistalrectumdiagnosed onninthpost-operativeday,andwastreatedwithoutsurgical
Table2–Clinicalandoperativeresults.
Case Operativetime (min)
Hospitalstay (days)
Morbidity/ mortality
A 55 1 None
B 50 1 None
C 45 1 None
D 45 1 None
E 80 1 None
F 40 1 None
G 47 1 None
H 60 1 None
I Notperformed Notoperated None
J 50 1 None
K 38 1 None
re-intervention.Inthispatient,scarcompletiontookabout45 days.
Discussion
forTEM.WhenTAMISwasfirstdescribed,theworldbecame awareofacompletelynewtechniqueusinganaffordable, sim-ple,easy-to-useandeffectivedevice.
Care must be taken in patient selection, as local exci-sion must be considered onlyfor early rectal cancer with noevidenceofnodalmetastasis,5,10 parametersthatcanbe
predicted by clinical and radiological evaluation.11,12 Even
afteradequate pre-operativeevaluation, up to44.3% of T1 tumorscanbemisevaluatedpre-operatively.1,13Althoughall
patientsweresubmittedtosurgerywithatumorthoughtto bebenign,onehadaT1andtheotheraT2tumor.As onco-logical safety for localresection for T2tumors isnot well stablished,1,14–17 this lastone was furthertaken to
laparo-scopic anterior resection with colo-anal anastomosis and pathologyshowednoresidualcarcinomaorpositive lymphn-odes(pT0N0)inthesurgicalspecimen.
Atiptobelearnedisthattheprostatevolumeshouldbe evaluatedpre-operatively,asitcanbelimitingforthe tech-nique.
Consideringtheminimalsetuptime,lowcostandspecially the adaptationof regularlyused laparoscopic instruments, TAMISprovidesanidealplatformfortransrectalortransanal resection.18 Ithas alsobeen usedfor other diseases, such
as high fistulas and distal rectal mobilization for coloanal anastomosis19 and carcinoid tumors resection.20,21 Other
indications that lack consensus are re-excision following endoscopic removalof malignant polyps22 and excision of
downstagedtumororscaraftercompleteresponseto neoad-juvantchemo/radiotherapy.13,23–25Recently,totalmesorectal
excision performed by TAMIS showed to be feasible and promisesgoodfutureresults.
Inthisseries,maximumdistancefromtumortoanalverge was8cm.Thispatienthada5cmdiametertumor,soresection wasupto14cmfromanalverge,consideringmargins,without difficulties,showingthatitsusemustnotberestrictedtolow tumors,assuggestedbefore.26
TheadvantagesofTAMISoverTEMarewelldescribed:3,27
• Devicesused forTAMIS are pliable and allowwell-fitted
positioningattheanalcanal,possiblyleadingtoless impair-mentofsphincterfunctionthanthe40mmrigidscopeused forTEM.
• SetuptimeissignificantlylowerforTAMIS.
• Possibilitytouseregularstraightlaparoscopicinstruments
andastandard30◦laparoscope,asopposedtothefixed eye-pieceoftheTEMrectoscope,whichenablesadvancement ofthescopeintotheproximalrectumandsigmoid,thereby allowingthesurgeontolookbeyondthetumor.
• It can be easily learned by surgeons not used to TEM
techniqueduetoitspotentialinstrumentalsimplicityand similarity withconventional laparoscopic surgery. Larger ports, up to15mm port are available only for TAMIS devices,and it can bevery helpful when a 12-mm sta-plerisneeded(e.g.forsaferesectionofabigpedunculated polyp).
• Cost makes SSLTM and GelPoint PathTM very
comfort-able,safeandcost-effectivealternativesforTEM.28When
abdominal resection is considered for adenomas or T1 tumorsthatarefromdentatelineuptohigherrectum,or eveniffuturestudiesshowthatselectedT2andT3tumors
can belocallycontrolled,1,14,16,29 TAMISdevices canbea
remarkablecost-effectivealternative.
• The cap can be removed and re-located quickly, when
needed.Itcanberemovedforspecimenretrievaland repo-sitionedinlessthan1minforsuturing.
• Positioningthedevicetakesusuallylessthan1min.
• Duetoitsdesign,thereisnoneedforinvestmentinspecial
curvedinstruments.Allregular laparoscopicinstruments canbeused.
• Therepositionablecapallowschangingofinstrument
posi-tionwithouthavingtoreinsertthedevice.
• Asthedevicesarebasicallyahollowsleevewithacapin
whichthe portsare located,thereisnoresistancewhen movingaroundtheinstruments.Thismakestheuseof reg-ularstraightlaparoscopicinstrumentseasierthanTEMor SILSTM(Covidien,Mansfield,MA).
Conclusions
Althoughatpresenttimetheappropriateuseoflocalexcision isstillunderdebate,TAMISisatechniquethathasapotential ofincreasedapplicationandmuchremainstobelearned.Like others,3,27ourgroupisoptimisticthatTAMIScameasagood
alternativetoTEMandalsoasoneofthemostimportant con-tributionsfortransanalsurgeryinthelastdecadesyears.Its reducedcostandsimplicityshallallowsurgeonstolearnthe techniquequiteeasily.Despitesimplicity,caremustbetaken inpatientselection,aspre-operativestagingisfrequentlyan understagingoftumors.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BachSP,HillJ,MonsonJRT,SimsonJNL,LaneL,MerrieA,etal. Apredictivemodelforlocalrecurrenceaftertransanal endoscopicmicrosurgeryforrectalcancer.BrJSurg. 2009;96:280–90.
2.InoueY,KusunokiM.Resectionofrectalcancer:ahistorical review.SurgToday.2010;40:501–6.
3.AtallahS,AlbertM,LarachS.Transanalminimallyinvasive surgery:agiantleapforward.SurgEndosc.2010;24:2200–5.
4.RamirezJM,AguilellaV,GraciaJA,OrtegoJ,EscuderoP, ValenciaJ,etal.Localfull-thicknessexcisionasfirstline treatmentforsessilerectaladenomas.AnnSurg. 2009;249:225–8.
5.ChristoforidisD,ChoH-M,DixonMR,MellgrenAF,MadoffRD, FinneCO.Transanalendoscopicmicrosurgeryversus conventionaltransanalexcisionforpatientswithearlyrectal cancer.AnnSurg.2009;249:776–82.
6.ZacharakisE,FreilichS,RekhrajS,AthanasiouT,ParaskevaP, ZiprinP,etal.Transanalendoscopicmicrosurgeryforrectal tumors:theSt.Mary’sexperience.AmJSurg.2007;194:694–8.
7.NashGM,WeiserMR,GuillemJG,TempleLK,ShiaJ,GonenM, etal.Long-termsurvivalaftertransanalexcisionofT1rectal cancer.DisColonRectum.2009;52:577–82.
disposabledevice:ourinitialexperience.TechColoproctol. 2013;18:393–7.
9. RochaJJRD,FéresO.Transanalendoscopicoperation:anew proposal.ActaCirBras.2008;23:93–104.
10.PalmaP,HorisbergerK,JoosA,RothenhoeferS,WillekeF,Post S.Localexcisionofearlyrectalcancer:istransanal
endoscopicmicrosurgeryanalternativetoradicalsurgery? RevEspEnfermDig.2009;101:172–8.
11.KimSH,ParkIJ,JohYG,HahnKY.Laparoscopicresectionof rectalcancer:acomparisonofsurgicalandoncologic outcomesbetweenextraperitonealandintraperitoneal diseaselocations.DisColonRectum.2008;51:844–51.
12.DoorneboschPG,TollenaarRAEM,DeGraafEJR.Isthe increasingroleoftransanalendoscopicmicrosurgeryin curationforT1rectalcancerjustified?Asystematicreview. ActaOncol.2009;48:343–53.
13.MortensenN.Commentary.ColorectDis.2008;10:327–9.
14.PerezRO,Habr-GamaA,ProscurshimI,CamposFG,KissD, Gama-RodriguesJ,etal.LocalexcisionforypT2rectalcancer –muchadoaboutsomething.JGastrointestSurg.
2007;11:1431–40.
15.NairRM,SiegelEM,ChenDT,FulpWJ.Long-termresultsof transanalexcisionafterneoadjuvantchemoradiationforT2 andT3adenocarcinomasoftherectum.JGatrointestSurg. 2008;12.
16.BorschitzT,KneistW,GockelI,JungingerT.Localexcisionfor moreadvancedrectaltumors.ActaOncol.2008;47:1140–7.
17.WhitehousePA,ArmitageJN,TilneyHS,SimsonJNL. Transanalendoscopicmicrosurgery:localrecurrencerate followingresectionofrectalcancer.ColorectalDis. 2008;10:187–93.
18.BarendseRM,VerlaanT,BemelmanWA,FockensP,DekkerE, NonnerJ,etal.Transanalsingleportsurgery:selectinga suitableaccessportinaporcinemodel.SurgInnov. 2012;19:323–6.
19.WolthuisAM,CiniC,PenninckxF,D’HooreA.Transanalsingle portaccesstofacilitatedistalrectalmobilizationin
laparoscopicrectalsleeveresectionwithhand-sewncoloanal anastomosis.TechColoproctol.2011;16:161–5.
20.TsaiBM,FinneCO,NordenstamJF,ChristoforidisD,Madoff RD,MellgrenA.Transanalendoscopicmicrosurgeryresection ofrectaltumors:outcomesandrecommendations.DisColon Rectum.2010;53:16–23.
21.SemanM,BretagnolF,GuedjN,MaggioriL,FerronM,PanisY. Transanalendoscopicmicrosurgery(TEM)forrectaltumor: thefirstFrenchsingle-centerexperience.GastroenterolClin Biol.2010;34:488–93.
22.MelisM,GruelR,DarwinP,DrachenbergC,ShibataD.Full thicknesstransanalre-excisionfollowingendoscopicremoval ofmalignantrectalpolyps.IntJColorectalDis.2009;24: 531–6.
23.PerezRO,Habr-GamaA,LynnPB,SãoJuliãoGP,BianchiR, ProscurshimI,etal.Transanalendoscopicmicrosurgeryfor residualrectalcancer(ypT0-2)followingneoadjuvant chemoradiationtherapy:anotherwordofcaution.DisColon Rectum.2013;56:6–13.
24.ParkC,LeeW,HanS,YunS,ChunH-K.Transanallocal excisionforpreoperativeconcurrentchemoradiationtherapy fordistalrectalcancerinselectedpatients.SurgToday. 2007;37:1068–72.
25.Habr-GamaA,PerezRO,SãoJuliãoGP,ProscurshimI,Nahas SC,Gama-RodriguesJ.Factorsaffectingmanagement decisionsinrectalcancerinclinicalpractice:resultsfroma nationalsurvey.TechColoproctol.2010;15:45–51.
26.CasadesusD.Surgicalresectionofrectaladenoma:arapid review.WorldJGastroenterol.2009;15:3851–4.
27.BarendseRM,DoorneboschPG,BemelmanWA,FockensP, DekkerE,DeGraafEJR.Transanalemploymentofsingle accessportsisfeasibleforrectalsurgery.AnnSurg. 2012;256:1030–3.
28.CandaAE,TerziC,SagolO,SariogluS,ObuzF,FuzunM. Transanalsingle-portaccessmicrosurgery(TSPAM).Surg LaparoscEndoscPercutanTech.2012;22:349–53.