Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
Article
Association
of
sociodemographic
and
clinical
factors
with
the
self-image
and
self-esteem
of
individuals
with
intestinal
stoma
Geraldo
Magela
Salomé
a,∗,
Sergio
Aguinaldo
de
Almeida
baUniversidadedoValedoSapucaí(UNIVÁS),SãoPaulo,SP,Brazil bPrivatePractice,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25February2014 Accepted15May2014 Availableonline17June2014
Keywords:
Ostomy Qualityoflife Bodyimage Self-image Self-esteem
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicalandsociodemographicfactorsandcorrelatethemtothe self-imageandself-esteem.
Methods:AstudyconductedatOstomyPoleofPousoAlegre.Thedatawerecollectedbetween December2012andMay2013.Thiswasanon-probabilistic,byconvenience,sample.Fordata collection,theRosenbergSelf-EsteemScale/UNIFESP-EPMandBodyInvestmentScalewere used.Forstatisticalanalysis,chi-squaredtest,Kruskal–WallistestandSpearmancorrelation wereused.Levelsofsignificanceof5%(p≤0.05)wereconsidered.
Results:Participantshadameanscoreof10.81intheRosenbergSelf-EsteemScale/UNIFESP. RegardingBodyInvestmentScaleresults,themeantotalscorewas38.79;themeaninthe domainofbodyimagewas7.74,andforpersonaltouch,21.31.Whencomparingdatarelated tothestomaandsociodemographicprofileswiththeRosenbergSelf-EsteemScale/UNIFESP andBodyInvestmentScale,werealizethatallpatientsdemonstratedadecreasein self-esteemandself-image.Individualswereover60yearsold,male,retired,marriedandwere not participants insupportgroup/association.With regardtothecharacteristics ofthe stoma,thosepermanentcolostomizedhadascausesofstomaimplementation inflamma-torydiseaseandneoplasia;stomatameasuredbetween20and40mm;thesepeopleused two-piecedevices.Peoplewhohavenotbeennotifiedthatwouldbesubjectedtothestoma andinwhomnodemarcationwasdoneshowedworseninginself-esteemandself-image inrelationtootherfeaturesrelatedtoinjuryandsociodemographicdata.
Conclusion: Patientswhoparticipatedinthisstudyhadlowself-imageandself-esteeminall characteristicsofthestomaandinsociodemographicdata,meaningthattheseindividuals hadnegativefeelingsabouttheirownbodies.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](G.M.Salomé).
http://dx.doi.org/10.1016/j.jcol.2014.05.005
Associac¸ão
dos
fatores
sociodemográficos
e
clínicos
à
autoimagem
e
autoestima
dos
indivíduos
com
estoma
intestinal
Palavras-chave:
Estomia
Qualidadedevida Imagemcorporal Autoimagem Autoestima
r
e
s
u
m
o
Objetivo: Avaliarosfatoressociodemográficoseclínicosecorrelacioná-losàautoimageme autoestima.
Métodos: Estudo realizado no Polo dos Estomizados de Pouso Alegre. Os dados foram coletados entre dezembro de 2012 e maiode 2013. A amostra foi por não probabilís-tica, por conveniência.Paracoleta de dados, foram utilizadasa Escala de Autoestima Rosenberg/UNIFESP–EPMea escalaBodyInvestmentScale.Paraanáliseestatística,foram utilizadosostestesdoQui-quadradoedeKruskal-Walliseacorrelac¸ãodeSpearman.Foram consideradososníveisdesignificância5%(p≤0,05).
Resultados: Os participantes apresentaram a média de 10,81 na Escala de Autoestima Rosenberg/UNIFESP–EPM.Comrelac¸ãoàescalaBodyInvestmentScale,amédiadoescore totalfoi38,79;amédianosdomíniosimagemcorporalfoide7,74enotoquepessoal,21,31. AocomparamososdadosrelacionadosaoestomaesociodemográficoscomaEscalade AutoestimaRosenberg/UNIFESP–EPMecomescalaBodyInvestmentScale,percebemosque todosospacientesapresentaramquedanaautoestimaenaautoimagem.Osindivíduos estavam nafaixa etáriaacima de 60 anos,sexo masculino, eramaposentadose casa-dosenãoparticipavamdegrupodeapoio/associac¸ão.Comrelac¸ãoàscaracterísticasdo estoma,osindivíduoscomcolostomiapermanentetinhamcomocausasdarealizac¸ãodo estomadoenc¸ainflamatóriaeneoplasia;osestomasmensuravamentre20a40mm;eles utilizavamdispositivocomduaspec¸as.Pessoasquenãoforamcomunicadasdequeiriam sersubmetidasaoestoma,eemquenãofoirealizadaademarcac¸ãoapresentarampiorana autoestimaenaautoimagemcomrelac¸ãoàsoutrascaracterísticasrelacionadasàlesãoe àssociodemográficas.
Conclusão: Pacientesqueparticiparamdesteestudoapresentarambaixanaautoimageme autoestimaemtodasascaracterísticasdoestomaenosdadossociodemográficos, signifi-candoqueessesindivíduostinhamsentimentosnegativosemrelac¸ãoaoprópriocorpo.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Undoubtedly the technological and scientific advances in health,aswellastheprocessofdemographicand epidemi-ological transition, enabled an increase in life expectancy ofthe population inrecent years.In this twenty-first cen-tury,therearestillhugeandrelevantproblemsthatcontinue toaffectthehealthofpeople worldwideand alsoinBrazil. These implications ofscientific and technological develop-ment in people’s living conditions have been worrying to researchers,1 primarilythose relatedto the ostomytheme.
These concerns are about the effectiveness of therapeutic interventions,complications,devicesused,self-care,butalso withtheimprovementsmadeinqualityoflife,self-esteem, self-imageandsexualityoftheseindividuals,especiallythose whohavedegenerativeandnotdegenerativediseases.1,2
Stomaand ostomy are Greek terms meaning mouth or opening.Itisachangeinbowel habits,anatomically mod-ified,inwhichthereisanexternalizationofhollowviscera throughthebody;inthecaseoftheintestine,thedeviceis inserted into the outerabdominal wall,3 and may be
tem-poraryor permanent.Temporarystomasaimtoprotectan intestinalanastomosisandcanbereversed.Thepermanent stomas usuallyare indicated in cases of intestinal cancer
withoutthepossibilityofreestablishmentofnormalintestinal transit.4
Usually, these individuals who underwent intestinal stoma,breakingwiththisusualeliminationpattern,arefaced withemotionalandpsychologicaldifficultiesandfeelasense ofdisgustinrelationtothemselves.5
Besides the emotional and psychological changes, the ostomy generatesa series ofphysicalchanges that impair social life of stoma users, especially those related to the lackoftheanusandthepresenceofaholeintheabdomen throughwhichthefecesareeliminated.Asaresult,not infre-quentlythepersonfeelsverydifferentfromtheothers,and evenexcluded.Thisisbecauseeveryhumanbeingconstructs, throughouthislife,animageofhisownbody,whichfitstothe customsandtheenvironmentwherehelives–inshortthat meethisneedstofeelnestledinhisownworld.6
Inourmodernsociety,thebodyimagecanberelatedto youth,beauty,strength,integrityandhealth;andthosethat donotcorrespondtotheconceptofbodybeautycan experi-encesignificantsenseofrejection.7,8Bodyimageisthemental
The individual, in coming to terms with an intestinal stoma, suffer changes in his body image, self-esteem and sexuality,as heiseliminatingfecesandgases throughthe abdomen.Thus,hestartsanewlifeindifferentliving con-ditionsassociatedwithdisabilityandloss,feelingworthless, ashamedofotherpeopleandendinginisolationwithrespect tofamily,friendsandleisureactivities,andchanginghis qual-ityoflife.Whenapersonhashealthyself-esteemandbody image,hedealseasilywithits presentlivingsituation and carryonleavinganexistencewithouttrauma.
This study aimed to evaluate the clinical and sociode-mographicfactorsandcorrelatethemtotheself-imageand self-esteem.
Methods
Thisisaprimary,descriptive,analytical,prospectiveclinical study.
ThisstudywasconductedattheOstomyPoleof PousoAle-gre.ThedatawerecollectedintheperiodbetweenDecember 2012andMay2013,afterapprovalbytheEthicsCommittee, UniversidadedoValedoSapucaí,OpinionNo.23,277.The sam-plewasselectedinanon-probabilistic,forconvenience,way. Thedatacollectionwasconductedbyresearchersthemselves, afterallpatientshavesignedtheinformedconsentform.In thisstudy,theinclusioncriteriawere:≥18yearsoldandcarry anintestinalstoma.Exclusioncriteriawere:patientswith syn-dromesofdementiaandotherconditionsthatwouldprevent themtounderstandandanswerthequestionnaires.
Three instruments to collect data for the survey were used. First,a questionnaireon sociodemographicdata and characteristicsofthestomawasused; then,the Rosenberg Self-EsteemScale/UNIFESP-EPM(RSES)wasused;andthird, theBodyInvestmentScale(BIS)wasapplied.
TheRosenbergscaleisascaleusedinseveralstudieson self-esteem.10,11 Thisisaone-dimensional scale translated
andadaptedinBrazilbyDinietal.12tobeusedintheirwork,
andwhichwasappliedinapopulationofpatientswhowould undergoplasticsurgery.12–14RosenbergScaleisaLikert-type
4-pointscale(1=Istronglyagree,2=Iagree,3=Idisagree,4=I stronglydisagree),containing10items.Ofthistotalofitems, fiveassesstheindividual’spositivefeelingsabouthimself(in general:Iamsatisfiedwithmyself;IfeelIhaveabitofgood qualities;Iamabletodothingsaswellasmostother peo-ple,providedthatI’mtaughttodothem;IfeelIamaworthy person,atleastonaplanelikeother people;Ihavea posi-tiveattitudetowardmyself)andfiveassessnegativefeelings (SometimesIthinkI’mnogood;Idonotfeelsatisfactionin thethingsthatIaccomplish;Ifeel thatIhavenotmuchto beproud of; Sometimes Ireally feel useless, unable to do things;Iwouldliketohavemorerespectformyself,I’malmost alwaysinclinedtothinkI’maloser).Toscoretheresponses, thefiveitemsexpressingpositivefeelingshaveinverted val-ues,which,addedtotheotherfive,totalasinglevalueforthe scale.Thisscaleconsistsoftenstatementswithfourresponse options. Eachalternative has avalueranging from zero to three.Thus,thescalepresentsafinalscoreof0to30,where 0isthebestvalueforself-esteemand30theworst.
TheBrazilianversionofthe BodyInvestmentScale(BIS) consistsof20itemsdividedintothreedomains(bodyimage, bodycareandbodytouch).Theanswersarearrangedina five-pointLikertscale,rangingfrom“Istronglydisagree”(1point) to“Istronglyagree”(5points).Toobtainthefinalscoreofthe scale,onemustreversethescoresofitems2,5,9,11,13and 17andaddupalltheitems.Thehigherthescore,thegreater thepositivefeelingtowardthebody.13
Whenassessingtheresults,thedatawereenteredand ana-lyzedusingtheSPSS–8.0statisticalprogram.Forthestatistical analysis, the following tests were also used: Chi- squared test for socio-demographic variables and characteristics of thestoma;andinordertocomparebetweentheRosenberg Self-EsteemScale/UNIFESP and BodyInvestmentScale and sociodemographicand clinicaldata,theKruskal–Wallistest andSpearmancorrelationwereused.Forallstatisticaltests, weconsidereda5%levelassignificant(p≤0.05).
Results
The results will be presented initially based on sociode-mographiccharacterizationandthenbycharacterizationof patientswithintestinalstomaandfinallybyassessmentof self-esteemandself-image.
InTable1,mostparticipantshadover60years,weremale,
retired, and attendingtosupportgroups. Twenty-one(30%) ofrespondentswereilliterateand19(25.10%)couldreadand write.
ItisobservedinTable2thatmostofthecausesthatled patientstoacquireostomywerecasesofneoplasia;thetype ofostomywasapermanentcolostomy.Mostindividualswere nottoldtheywouldbesubmittedtothestoma.Inaddition, individualswerenotsubjecttothedemarcationofthestoma and didnotundergoirrigation.Regarding thetypeof com-plication,34(48.60%)haddermatitis;14(20%)hadretraction; and13(18.60%)sufferedprolapse.Withrespecttothe diam-eterofthestoma,34(48.60%)had20–40mm;and23(32.90%) 40–60mm.
In Table 3, we can see in face of the responses of
our participants that the mean of Rosenberg Self-Esteem Scale/UNIFESP-EPMwas10.81,implyingthattheseindividuals hadlowself-esteem.AsregardstotheBodyInvestmentScale, in the domains body image and personal touch the mean waslow,meaningthattheseindividualshadnegativefeelings abouttheirownbodies.
InTable4,wefindacomparisonamongdataofthestoma
and the scales used in this study, where it is possible to observethatallpatientsshowedchangesinself-esteemand self-imagewithrespecttocharacteristicsofthestoma; how-ever, individuals withpermanent colostomy had neoplasia andinflammatorydiseaseascausestoperformthestoma;in addition,theirstomatahaddiametersbetween20and40mm. Theseparticipantsusedtwo-piecedevices.Thosewhowere nottoldtheywouldbesubjectedtothestomaandinwhom thedemarcationwasnotperformedexhibitedworseningin self-esteemandself-image.
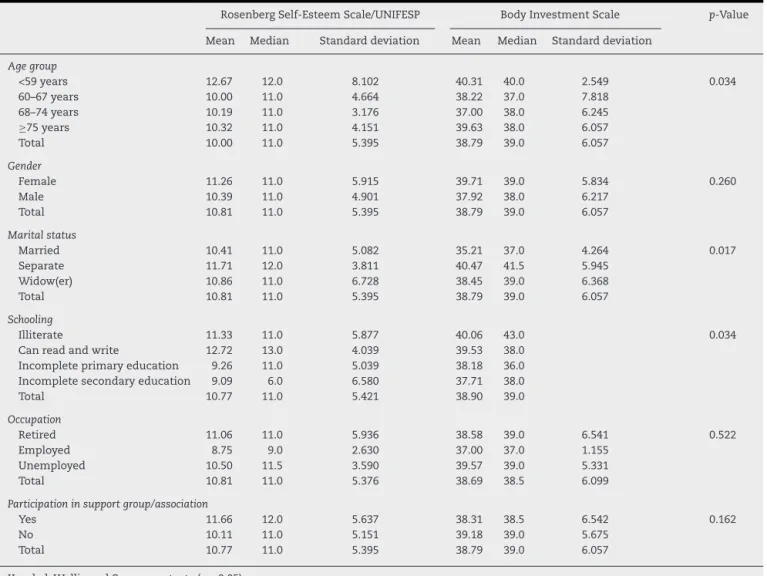
From Table 5, it can be inferred that all the patients
Table1–Socio-demographiccharacteristicsofindividualswithintestinalstoma.
Variable p N %Overall %Valid %Cumulative
Gender
Male 0.003 52 74.3 74.3 100.0
Female 18 25.7 25.7 25.7
Total 70 100.0 100.0
Agegroups
44–59years 17 24.3 24.3 24.3
60–67years 18 25.7 25.7 50.0
68–74years 0.057 16 22.9 22.9 72.9
75to85years 19 27.1 27.1 100.0
Total 70 100.0 100.0
Maritalstatus
Married 34 48.6 48.6 48.6
Separated 14 20.0 20.0 68.6
Widow(er) 0.035 22 31.4 31.4 100.0
Total 70 100.0 100.0
Occupation
Retired 50 71.4 73.5 73.5
Unemployed 4 5.7 5.9 79.4
Atwork 14 20.0 20.6 100.0
Total 0.003 68 97.1 100.0
Noanswer 2 2.9
Total 70 100.0
Participationinsupportgroup/association
Yes 38 54.3 54.3 54.3
No 0.075 32 45.7 45.7 100.0
Total 70 100.0 100.0
Total 70 100.0 100.0
Chi-squaredtest(p≤0.05).
primary education, employed and married. Patients who
werenotparticipatinginsupportgroup/associationpresented worseself-esteemandself-imageinrelationtootherpatients.
Discussion
Intermsofsociodemographiccharacteristicsofthestudy par-ticipants,mostparticipantshadover60years,ofmalegender andretirees,andparticipatinginsupportgroups.Only21(30%) ofrespondents were illiterate and nineteen (25.10%) could read and write; these findings corroborate several studies. Regardingstomafeatures,mostofthecausesthatledpatients
tohaveanostomyperformed wereneoplasms; thetypeof
ostomywaspermanentcolostomy.Mostindividualsdidnot
knowthatwouldbesubmittedtothestoma.Inaddition,the individualswerenotsubjecttothedemarcationofthestoma. Regardingthetypeofcomplication,34(48.60%)had dermati-tis;14(20%),retractionand13(18.60%),prolapse.Withrespect tothediameterofthestoma,34(48.60%)had20–40mm,and 23(32.90%),40–60mm.Thesefindingscoincidewithresultsof severalstudies.2,4,5,7,14–17
Theincreaseintheelderlypopulation,whichiscurrently taking placein Brazil,tendsto cause socialand economic changesandanincreaseinchronicdiseases,forexample dia-betesmellitus,hypertension,traumaand cancer;the latter twocancausethepatienttoundergoasurgicalprocedurefor removingfecalcontentsbytheabdominalwall.Inmy expe-rienceasastomatherapistnurse,Ihaverealizedthatwhen
theindividualissubjectedtothepreparationofthestoma,a breakuphappensautomaticallyfromhiseliminationpattern, andoftenthepatienthaspsychologicalandsocialchanges, experiencingfeelingsofdisgust,resultinginsocialandfamily isolation and inleisure loss. Such feelingshave as a con-sequence changes ofself-image,self-esteem,sexuality and qualityoflife.
In psychic alterations, the change in self-image is one aspectthatstandsout,sincethepatientwillneedtoresethis bodyimage,mannerofdressandofinteractingwithhisown body.Asregardstothesocialaspect,thepresenceofthestoma affectsbothatthefamilylevel,asinthepatient’sleisureand workactivities.Changesinleisureactivitiesrelatemostlyto theshameortotheapparentpresenceofgasinthebag.
Ibelieveitispertinenttotranscribeherethespeechofa patientduringaninterview,thatmovedme:“FirstIwasvery sadtolookatmybellyandseefecesandgasescomingout,I wasverytraumatized,Ifeltfilthy,uglyandinmybody some-thingthatwasnotminewasthere.IntheearlyyearsIwas ashamedandIisolatedmyselfanddidnotletanypersonsee mybellyandtouchme,onlymywifecouldtouchmebecause shehelpedtochangethebagandcleanmyskinandstoma”.
Table2–Characteristicsoftheintestinalstoma.
Variable p N %Overall %Valid %Cumulative
Causeofostomy
Diverticulitis 3 4.3 4.3 4.3
Inflammatoryboweldisease 5 7.1 7.1 11.4
Neoplasia 0.003 52 74.3 74.3 85.7
Crohn’sdisease 10 14.3 14.3 100.0
Total 70 100.0 100.0
Typeofstoma
Colostomy 54 77.1 77.1 77.1
Ileostomy 0.007 16 22.9 22.9 100.0
Total 70 100.0 100.0
Diameterofthestoma
0to20mm 10 14.3 14.3 14.3
20to40mm 34 48.6 48.6 62.9
40to60mm 0.056 23 32.9 32.9 95.7
60to80mm 3 4.3 4.3 100.0
Total 70 100.0 100.0
Complicationtype
Dermatitis 34 48.6 48.6 48.6 34
Fistula 1 1.4 1.4 50.0 1
Peristomalhernia 5 7.1 7.1 57.1 5
Pseudo-verrucous 0.0023 1 1.4 1.4 58.6
Allergicreactiontodevice 1 1.4 1.4 60.0
Pseudo-verrucousinjuries/dermatitis 1 1.4 1.4 61.4
Retraction 14 20.0 20.0 81.4
Prolapse 13 18.6 18.6 100.0
Total 70 100.0 100.0
Demarcationwascarriedout
Yes 17 24.3 24.3 24.3
No 0.002 53 75.7 75.7 100.0
Total 70 100.0 100.0
Devicetype
SingleSystem 22 31.4 31.4 31.4
TwoParts 0.043 48 68.6 68.6 100.0
Total 70 100.0 100.0
Makesirrigation
Yes 26 37.1 37.1 37.1
No 0.047 44 62.9 62.9 100.0
Total 70 100.0 100.0
Itwasreportedthatyouhaveastoma
Yes 48 68.6 68.6 68.6
No 0.049 22 31.4 31.4 100.0
Total 70 100.0 100.0
Stomacharacteristic
Temporary 18 25.7 25.7 25.7
Definitive 0.003 52 74.3 74.3 100.0
Total 70 100.0 100.0
Chi-squaredtest(p≤0.05).
By having the anatomical structure modified, the
ostomised individual also is faced with his conflicts and
fantasiesaccordingtotheimagehemakesofhisownbody, aswellasaccordingtotheimagethatpeoplewhosurround himmakeofhim.18Thisfactfavorsthelossofself-esteem,
sincewhendealingwithcolostomy,people’sattentionstays focusedonthevaluesrelatedtointestinalelimination,and a thing that before was considered as something natural becomestheobjectofreflectionandmustbereacessed.19
Socialisolationissomethingvisible;however,itis impor-tanttonotethatgiventhisreality,itisimperativetheneedof socialinteraction,asthisprocesswillhelptorestorethe per-ceptionrelatedtotheostomisedbodyanditsownself-image and,mainly,willcontributetoovercomingtheloneliness.20
Table3–ResultsobtainedintheBodyInvestmentScalemeanscoreandtheRosenbergSelf-EsteemScale/UNIFESP-EPM inindividualswithintestinalstoma.
RosenbergSelf-EsteemScale/UNIFESP BodyInvestmentScale p-Value
Dominium Dominium
Totalscore Bodyimage Personalcare Personaltouch
Mean 10.81 38.79 7.74 21.31 10.19
Median 11.00 39.00 8.00 21.00 10.00 0.002
Mode 11 36 9 19 10
StandardDeviation 5.395 6.057 3.077 6.342 3.965
Kruskal–WallisandSpearmantests(p≤0.05).
When comparing data related to the stoma and to the
demographicprofilewiththeRosenbergSelf-Esteem/UNIFESP scaleandtheBodyInvestmentScale,werealizethatallthe patientsshowedchanges(decrease)inself-esteemand self-image.Theparticipantshadover60years,male,marriedand retiredandwerenotattendingthesupportgroup/association.
Withregard tothe characteristicsofthestoma,individuals
with permanent colostomy had as their cause for stoma
application neoplasia and inflammatory disease; the
sto-matameasured20–40mm.Thoseusersoftwo-piecedevices
were not communicated that they would be subjected to
the stoma and the demarcation was not performed. They
Table4–ComparisonbetweengroupsaccordingtocharacteristicsofthestomaandtheBodyInvestmentScaleand RosenbergSelf-EsteemScale/UNIFESP-EPMinindividualswithintestinalstoma.
RosenbergSelf-EsteemScale/UNIFESP BodyInvestmentScale p-Value
Mean Median Standarddeviation Mean Median Standarddeviation
Causeofstoma
Diverticulitis 15.00 15.0 10.000 40.40 40.0 2.881 0.016
Inflammatorydisease 10.00 11.0 3.808 32.67 29.0 6.351
Neoplasia 10.40 11.0 4.770 37.77 38.0 5.501
Other 12.10 10.0 7.520 45.10 45.0 5.744
Total 10.81 11.0 5.395 38.79 39.0 6.057
Stomatype
Colostomy 10.70 11.0 5.279 38.33 38.0 6.100 0.306
Ileostomy 11.19 11.0 5.935 40.31 40.0 5.839
Total 10.81 11.0 5.395 38.79 39.0 6.057
Diameterofstoma
0–20mm 13.70 13.5 6.783 37.40 37.0 7.891 0.187
20–40mm 9.76 11.0 4.881 37.67 39.0 6.110
40–60mm 11.09 11.0 5.169 38.70 38.0 6.574
60–80mm 11.00 14.0 7.000 39.35 39.0 5.256
Total 10.81 11.0 5.395 38.79 39.0 6.057
Demarcationofthestomawascarriedout
Yes 11.59 14.0 4.757 38.88 38.0 7.339 0.110
No 10.57 11.0 5.604 38.75 39.0 5.667
Total 10.81 11.0 5.395 38.79 39.0 6.057
Devicetype
Systematic 11.02 11.0 5.537 39.09 38.5 5.639 0.546
Two-piece 10.36 11.0 5.169 38.65 39.0 6.292
Total 10.81 11.0 5.395 38.79 39.0 6.057
Itwasreportedthatyouhaveastoma
Yes 10.92 11.0 5.386 39.82 39.0 5.877 0.634
No 10.59 11.0 5.535 38.31 38.0 6.141
Total 10.81 11.0 5.395 38.79 39.0 6.057
Stomacharacter
Temporary 12.00 11.5 6.589 39.15 39.0 6.182 0.332
Definitive 10.40 11.0 4.5924 37.72 37.5 5.717
Total 10.81 11.0 5.39 38.79 39.0 6.057
Table5–ComparisonbetweengroupsaccordingtodemographicdataandRosenbergSelf-EsteemScale/UNIFESP-EPM andHerthHopeScaleinindividualswithintestinalstoma.
RosenbergSelf-EsteemScale/UNIFESP BodyInvestmentScale p-Value
Mean Median Standarddeviation Mean Median Standarddeviation
Agegroup
<59years 12.67 12.0 8.102 40.31 40.0 2.549 0.034
60–67years 10.00 11.0 4.664 38.22 37.0 7.818
68–74years 10.19 11.0 3.176 37.00 38.0 6.245
≥75years 10.32 11.0 4.151 39.63 38.0 6.057
Total 10.00 11.0 5.395 38.79 39.0 6.057
Gender
Female 11.26 11.0 5.915 39.71 39.0 5.834 0.260
Male 10.39 11.0 4.901 37.92 38.0 6.217
Total 10.81 11.0 5.395 38.79 39.0 6.057
Maritalstatus
Married 10.41 11.0 5.082 35.21 37.0 4.264 0.017
Separate 11.71 12.0 3.811 40.47 41.5 5.945
Widow(er) 10.86 11.0 6.728 38.45 39.0 6.368
Total 10.81 11.0 5.395 38.79 39.0 6.057
Schooling
Illiterate 11.33 11.0 5.877 40.06 43.0 0.034
Canreadandwrite 12.72 13.0 4.039 39.53 38.0
Incompleteprimaryeducation 9.26 11.0 5.039 38.18 36.0
Incompletesecondaryeducation 9.09 6.0 6.580 37.71 38.0
Total 10.77 11.0 5.421 38.90 39.0
Occupation
Retired 11.06 11.0 5.936 38.58 39.0 6.541 0.522
Employed 8.75 9.0 2.630 37.00 37.0 1.155
Unemployed 10.50 11.5 3.590 39.57 39.0 5.331
Total 10.81 11.0 5.376 38.69 38.5 6.099
Participationinsupportgroup/association
Yes 11.66 12.0 5.637 38.31 38.5 6.542 0.162
No 10.11 11.0 5.151 39.18 39.0 5.675
Total 10.77 11.0 5.395 38.79 39.0 6.057
Kruskal–WallisandSpearmantests(p≤0.05).
had low self-esteem and self-image change in relation to
otherpatients.Thesefindingscorroborateresultsofseveral studies.2,4,5,7,14,16,19
Inreality,theostomyandthecollectorequipmentcausea realchangeinthelivesofostomizedpeople,andthischange requirestimeforacceptanceandforself-carelearning.The personhastheobligationofadailycareofthestomaandits accessories.Thistaskisnoteasy;theyareexposedtocontact withaphysicaldeformitycausedbysurgeryandalsowiththe needtodirectlymanipulatetheirownfeces,whichleadsthem totheexperienceoffeelingsoflowself-esteem.Itisalsothe timewhenpeoplestarttobecomeawareofthelimitations causedbythestomaintheiractivitiesofdailyliving.14
Thecoexistencewiththe collectorequipmentgenerates theonsetofconflictingfeelings,concernsanddifficultiesto dealwiththisnewsituation.Thereare emotionalstagesof negation co-responsible for the declineof self-esteem and of self-image, thus causing sensation of mutilation, self-rejection and of peer people, as well as changes in other dimensions,such as moodand anger.15 I rememberagain
anotherpatient,thatconfidedme,“WhenIlookedinthe mir-rorandsawthecollectionbagwithfecesandthatIwaswith averylargevolumeintheabdomen,Ifeltverysad,verycross,
veryangry.SoIputaskirt,lookedagaininthemirroragain Inoticedthatthebagwasappearing.ThenIrealizedwhatI woulddo–Ihadtowearlooseclothing.”
Duetotheuseofthecollectorequipment,stomized peo-plemodifythemodeofdressing,usingmainlybaggyclothes thatareintendedtohidetheuseofcollectorequipment. How-ever,thisstrategycontributestoalossinbodyaestheticsand, consequently,ofself-esteemandself-image.14
Inastudywhichtheperceptionofpatientswithcolostomy was analyzed regarding the use of the collection bag, the authorsfoundthattherelationshipbetweenthepersonwith acolostomyandhisbagcollectorisfullofnegativefeelings, significantchangesofthephysical,psychologicalandsexual nature,aswellasinhiswebofsocialrelationships.15,20
andexercisesinordertopreventcomplicationsandpromote comfortandsafety.
Thecareandcleaningoftheostomyandbagexchangein ostomizedpeopleareveryimportanttoensuretheintegrityof theskinandpreventinfection.Inordertocarryoutsuch meas-uresproperly,itisnecessarythatostomypatientsbeguided bynursingprofessionals,sotheycandevelopself-care.21,22
Thesocialreintegrationofostomizedpeopleisachallenge forthemultidisciplinaryteaminvolved,soitisimportantto encouragethesepeopletobelievethattheyareabletolive withthenewrealitythatwasimposedtothem.Therefore,the nurse’actionmustbebasedontheacceptanceofacoexistence withthe ostomy,besidestocontributetomaintainingtheir physicalandmentalhealth.7,23,24
Conclusion
Inthisstudy,wecouldconcludethatpatientswhoparticipated inthesurveyshowedadeclineinself-imageandself-esteem, meaningthattheseindividuals hadnegativefeelingsabout theirownbodies.
When comparing data related to the stoma and sociodemographic profiles with the Rosenberg Self-Esteem Scale/UNIFESP-EPM and Body Investment Scale, werealize thatallthepatientsshowedabnormalities(decrease)in self-esteemandself-image,beingmaleindividualsover60years, married and not attending support groups/associations. Withregardtothe characteristicsofthestoma,those with permanent colostomy had ascause ofstoma implantation neoplasms and inflammatory diseases, and their stomata measuredbetween 20and 40mm.Theirstomata were two-piecedevices,andthesepeoplewerenotcommunicatedsuch thattheywouldbesubjectedtothestomaandthe demarca-tionwasnotperformed.Theparticipantsexhibitedsignificant worseningofself-esteemandself-imageinrelationtoother features.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. NunesJP,VieiraD,NóbregaWG,FariasTYA,TorresGV.
Venousulcersinpatientstreatedatfamilyhealthunitsin
Natal,Brazil:prevalenceandsociodemographicandhealth
characterization.FIEPBull.2008;78:338–41.
2. DanielsenAK,SoerensenEE,BurcharthK,RosenbergJ.
Learningtolivewithapermanentintestinalostomy:impact
oneverydaylifeandeducationalneeds.JWoundOstomy
ContinenceNurs.2013;40:407–12.
3. SantosVLCG.Estomaterapiaatravésdostempos.In:Santos
VLCG,CessarettiIUR,editors.Assistênciaemestomaterapia
cuidadodosostomizados.SãoPaulo,SP:Atheneu;2005.
4. SampaioFAA,AquinoOS,AraujoTL,GalvãoMTG.Nursing
caretoanostomypatient:applicationoftheOrem’theory.
ActaPaulEnferm.2008;21:94–100.
5.NascimentoCMS,TrindadeGLB,LuzMHBA,SantiagoRF.
Vivênciadopacienteestomizado:umacontribuic¸ãoparaa
assistênciadeenfermagem.TextoContexto–Enferm.
2011;20:557–64.
6.SalterM.‘Ifyoucanhelpsomebody...’:nursinginterventions
tofacilitateadaptationtoanalteredbodyimage.World
CouncEnterostomTherJ.1999:28–32.
7.SouzaJB,OliveiraPG,GinaniFF.Implicac¸õessexuaisna
cirurgiadoestomaintestinal.In:CremaE,SilvaR,editors.
Estomas:umaabordageminterdisciplinar.Uberaba,MG:Pinti;
1997.p.177–91.
8.AlbuquerqueAS,TróccoliBT.DesenvolvimentodeumaEscala
deBem-estarsubjetivo.RevPsicol:TeoriaPesqui.
2004;20:153–64.
9.CashTF,PruzinskyT.Bodyimage:ahandbookoftheory,
research,andclinicalpractice.NewYork:Guilford;2002.
10.RosenbergM,SchoolerC,SchoenbachC,RosenbergF.Global
esteemandspecificself-esteem:differentconcepts,different
outcomes.AmSociolRev.1995;60:141–56.
11.SouzaDBL,FerreiraMC.Autoestimapessoalecoletivaem
mãesenãomães.PsicolEstud.2005;10:19–25.Maringá.
12.DiniGM,QuaresmaMR,FerreiraLM.Adaptac¸ãoculturale
validac¸ãodaversãoBrasileiradaEscaladeAutoestima
Rosenberg.SocBrasCirPlas.2004;19:41–52.
13.GouveiaVV,SantosCA,GouveiaRSV,SantosWS,PronkSL.
Escaladeinvestimentocorporal(BIS):Evidênciasdesua
validadefatorialeconsistênciainterna.AvalPsicol.
2008;7:57–66.
14.SilvaAL,ShimizuHE.Elsignificadodelcambioenelmodode
vivirdelapersonaconostomíaintestinaldifinitiva.Rev
Lat-AmEnferm.2006;14:483–90.
15.BatistaMRFF,RochaFCV,SilvaDMG,JúniorFJGS.Self-image
ofclientswithcolostomyrelatedtothecollectingbag.Bras
Enferm.2011;64:1043–7.
16.GaldinoYLS,CastroME,PereiraMLD,LimaSSO,SilvaFAA,
GuedesMVC.Ocotidianodapessoaestomizadafrenteàs
necessidadeshumanasbásicasalteradas.Estima.
2012;10:22–30.
17.DanielsenAK,SoerensenEE,BurcharthKM.Learningtolive
withapermanentintestinalostomy:impactoneverydaylife
andeducationalneeds.JWoundOstomyContinenceNurs.
2013;40:407–12.
18.GemelliLMG,ZagoMMF.Ainterpretac¸ãodocuidadocomo
ostomizadonavisãodoenfermeiro:umestudodecaso.
Lat-AmEnferm.2002;10:34–40.
19.WongSK,YoungPY,WidderS,KhadarooRG.Adescriptive
surveystudyontheeffectofageonqualityoflifefollowing
stomasurgery.OstomyWoundManage.2013;59:16–23.
20.SouzaPCM,CostaVRM,MaruyamaSAT,CostaALRC,
RodriguesAEC,NavarroJP.Asrepercussõesdevivercomuma
colostomiatemporárianoscorpos:individual,sociale
político.EletrEnf.2011;13:50–9.
21.ZimnickiKM.Preoperativestomasitemarkinginthegeneral
surgerypopulation.JWoundOstomyContinenceNurs.
2013;40:501–5.
22.KimuraCA,KamadaI,GuilhemD,MonteiroPS.Qualityoflife
analysisinostomizedcolorectalcancerpatients.JColoproctol
(RioJ).2013;33:216–21.
23.MelottiLF,BuenoIM,SilveiraGV,SilvaMEN,FedosseE.
Characterizationofpatientswithostomytreatedatapublic
municipalandregionalreferencecenter.JColoproctol(RioJ).
2013;33:70–4.
24.CostaVF,AlvesSG,EufrásioC,SaloméGM,FerreiraLF.
Assessingthebodyimageandsubjectivewellbeingof