jcoloproctol(rioj).2014;34(3):181–184
Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Case
Report
Successful
endoscopic
treatment
of
fecalith
blocking
sinus
in
a
patient
with
ileal
pouch-anal
anastomosis
Jessica
Ma
a,1,
Brook
Zhang
a,1,
Xian-rui
Wu
b,
Bo
Shen
a,∗ aDepartmentofGastroenterology/Hepatology,TheClevelandClinicFoundation,Cleveland,USA bDepartmentofColorectalSurgery,TheClevelandClinicFoundation,Cleveland,USAa
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13February2014
Accepted27February2014
Availableonline2July2014
Keywords:
Fecalith
Needleknife
Pouchsinus
Ulcerativecolitis
a
b
s
t
r
a
c
t
Background:Ulcerative colitispatients whounderwent restorativeproctocolectomywith
ilealpouch-analanastomosiscandevelopvariousmechanicalcomplications.Amongthem
ispresacralsinusresultingfromchronicanastomoticleak.
Methods:Wepresentasymptomaticpatientwithalargefecalithblockingthesinuswhich
wassuccessfullytreatedwithDopplerultrasoundguidedendoscopicneedleknife
sinuso-tomyalongwithfecalithextraction.
Results:A67-year-oldfemalepresentedwitha4-monthhistoryofperianalpainandurgency.
Pouchocopyshoweda3-cmdeepwide-mouthedanastomoticsinus,theorificeofwhichwas
blockedbyalargehardfecalith.RemovalofthefecalithusingRothNet,Tripod,orBasketwere
madebutfailed.Thenneedleknifewasappliedtocuttheorificetoenlargetheopeningofthe
sinus.Onemonthlater,thepatientreturnedandthefecalithwassuccessfullyremovedwith
twoBasketsandtwoRothnets.Sixmonthsafterfecalithextraction,pouchoscopyshowed
acompartalizeddistalpouchsinuswithtwocavities,whichwastreatedbytwosessions
ofDopplerultrasoundguidedendoscopicneedleknifesinusotomy.Sixmonthsfollowing
thetreatment,thesinuswascompletedhealed.Thepatienttoleratedallprocedureswell
withoutanycomplication.
Conclusion: Fecalithblockingpouchanastomoticsinusisararecomplicationinpatientswith
restorativeproctocolectomy.Inourcase,thissurgicalcomplicationwassuccessfullytreated
withacarefullyplanned,stepwiseendoscopyapproach.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All
rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](B.Shen).
1 SummerinternfromCaseWesternReserveUniversity,Cleveland,OH,USA.
http://dx.doi.org/10.1016/j.jcol.2014.06.005
182
jcoloproctol(rioj).2014;34(3):181–184Tratamento
endoscópico
bem-sucedido
de
fecálito
bloqueando
seio
em
paciente
com
anastomose
bolsa
ileal-anal
Palavras-chave:
Fecálito Bisturi-agulha
Seiobursal
Coliteulcerativa
r
e
s
u
m
o
Experiência:Pacientescomcoliteulcerativatratadosporproctocolectomiarestauradoracom
anastomosebolsaileal-analpodemseracometidospordiversascomplicac¸õesmecânicas.
Entreelas,cita-seoseiopré-sacralresultantedevazamentocrônicopelaanastomose.
Métodos: Apresentamosumapacientesintomáticacomumgrandefecálitobloqueandoo
seio,comtratamentobem-sucedidocomsinusotomiaporbisturi-agulhaguiadopor
ultras-som,juntamentecomaextrac¸ãodofecálito.
Resultados:Mulher,67anos,apresentou-secomhistóriade4mesesdedorperianale
urgên-cia. A avaliac¸ãoendoscópica da bolsa ilealrevelouum seio anastomótico comgrande
aberturasituadaa3cmdeprofundidade,cujoorifícioestavabloqueadopor umgrande
fecálitoendurecido.Foitentadasemsucessoaremoc¸ãodofecálitocomaajudade
Roth-Net,Tripod,oucestosrecuperadores.Depoisdessastentativas,aplicamosumbisturi-agulha
comoobjetivodeseccionaroorifíciocomvistasàampliac¸ãodaaberturadoseio.Ummês
depois,apacienteretornou,eofecálitofoiremovidocomsucessocomdoiscestos
recupe-radoresedoisRothNets.Transcorridosseismesesapósaremoc¸ãodofecálito,umaavaliac¸ão
endoscópicadabolsailealrevelouumseiodistalcompartimentadocomduascavidades,
tratadoporduassessõesdesinusotomiaendoscópicaporbisturi-agulhaguiadopor
ultras-som.Seismesesdepoisdotratamento,oseioestavacompletamentecurado.Apaciente
tolerousatisfatoriamentetodososprocedimentos,semqualquercomplicac¸ão.
Conclusão: A presenc¸a de um fecálitobloqueandooseio anastomótico de bolsaileal é
complicac¸ãoraraempacientessubmetidosaumaproctocolectomiarestauradora.Emnosso
caso,essacomplicac¸ãocirúrgicafoitratadacomsucessocomumaabordagemendoscópica
emetapas,cuidadosamenteplanejada.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.
Todososdireitosreservados.
Background
Restorative proctocolectomy with ileal pouch-anal
anas-tomosis (IPAA) has been widely accepted as the surgical
procedureofchoiceforthemajorityofpatientswith
ulcerat-ivecolitis(UC)orfamilialadenomatouspolyposis(FAP)who
requirecolectomy.However,thisprocedurecancausevarious
postoperative complications. Anastomotic leak resulting in
theformationofsinusisoneofthemostcommonsurgical
technique-associated complications.1,2 On the other hand,
fecalbezoarcanoccurinpatientswithilealpouches,being
oftenlocated atthe pouch body.2,3 Herewe reported on a
patientwith alarge fecalith locatedatthe orifice of
anas-tomotic sinus causing severe symptoms. The fecalith and
sinusweresuccessfully treatedwithastepwiseendoscopic
approach.
The
patient
A67-year-oldfemalepresentedtoourPouch Centerwitha
4-monthhistoryofperianalpainandurgencyinApril2012.
Her past medical and surgical history was significant for
havingatwo-stageJpouch surgeryformedicallyrefractory
ulcerativecolitis(UC)in1999.Bothsurgeryandhospitalization
wereuneventful.
At presentation, the patient was taken to the
out-patientendoscopysuite.Informedconsentwasobtained.On
conscious sedation, a pouchoscopy was performed with a
GIF-H180 gastroscope (Olympus, Tokyo, Japan). An
anasto-moticsinuswithadepthof3cmwasfoundandtheorifice
wasblockedbyalargehardfecalith.Initiallyweplannedto
retrievethefecalithfirstfollowedbytreatingthepouchsinus
with ultrasound (Vascular Technology Inc. [VTI], Nashua,
New Hampshire, USA) guided endoscopic needle knife
(OlympusMedicalSystems,Tokyo,Japan)sinusotomyatthe
settingofERCPendocut(USAIncorporatedSurgicalSystems,
Marietta,Georgia,USA).MultipleattemptsusingRothNet(US
Endoscopy,Mentor,OH), Tripod(EndoscopySupportService
America, Brewster, NY), or endoscopic Basket (Olympus
America, Melville, NY) were made to remove the fecalith,
howevernoneofthemsucceeded. Thenwedecidedtouse
theneedleknifetocutthecommonwallbetweenthesinus
andthepouchbodytolayopenthesinustractandtrytotake
outthefecalithinthenextpouchoscopy.Atthepouchoscopy,
there was also a tight anastomotic stricture, which was
successfully dilated using the guide wire-controlled radial
expansion (CRE) balloons (Boston Scientific, Boston, MA).
Multiplebiopsiesweretaken,whichwerenotremarkable.
Onemonthlater,thepatientreturnedtoourPouchCenter.
Pouchoscopywasperformedfollowingthesameprotocolas
thepreviousone.Thefecalithatthesinuscavitywas
success-fullyremovedwithtwoendoscopicBasketsandtwoRothnets
jcoloproctol(rioj).2014;34(3):181–184
183
(A)
(B)
(C)
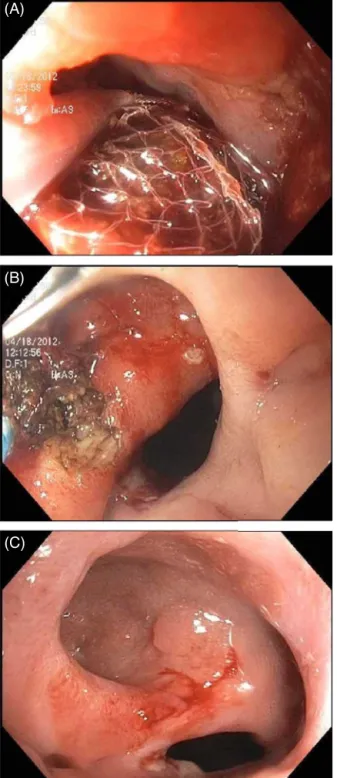
Fig.1–Successfulendoscopictreatmentoffecalith blockingsinusinapatientwithanilealpouch.A,fecalith
removedusingtwobasketsandtwoRoth-Nets;B,
compartmentalizedsinustreatedwithneedle-knife
sinustomy;C,ahealedandepithelializedpouchsinus.
between the sinus and pouch body resulted from the last
sessionofneedle-knifetherapy,pouchsinuswasnottreated.
Sixmonthsafterremovingthefecalith,thepatientcameback
toourPouchCenterforthefurthermanagementofthepouch
sinus.Then,the pouchoscopyshowedacompartalized
dis-talpouchsinuswithtwocavities.AnothersessionofDoppler
ultrasoundguidedendoscopicneedleknifesinusotomywas
offeredtotreatthesinus(Fig.1B).Atthemostrecent
follow-up6monthsaftertreatingthepouchsinus,thepouchoscopy
showedahealedsinus(Fig.1C).Thepatienttoleratedall
proce-dureswellinanoutpatientsettingwithoutanycomplication.
Thepatient continued todowell afterthe procedures and
reportedtheresolutionofhersymptoms.
Discussion
Pouch sinus,a less known disease entityin patients with
IPAA,isaspecialformofanastomoticleakdefinedbya
blind-endedtrack.Thereportedfrequencyofpouchsinusinpatient
undergoingIPAArangedfrom2.8%to8%.1,4,5 Thecommon
symptomsofpouchsinusincludedpelvicdiscomfortorpain,
dyschezia,andurgency.Pouchsinusdeservesaclose
surveil-lanceandtimelytreatment,asitmayhaveasignificantimpact
on pouch outcomes and patients’ QOL. Bezoarin the ileal
pouchesisanevenmorerarecomplicationfollowingIPAA,
withonlycasereportspublishedintheliterature.2,3,6Tothe
bestofourknowledge,ourstudyreportedthefirstcasewith
asymptomaticsinusatthedistalpouchwhichwasblocked
by alarge fecalith.Furthermore,we showedthe feasibility
oftreating fecalithblocking sinus byremovingthe fecalith
andapplyingtheultrasoundguidedneedleknifesinusotomy
accomplishedusingtheendoscopicapproach.
Themanagementforbezoarintheilealpouchesis
straight-forward.Withadvancedequipmentandtechniques,retrieval
of the bezoar using the endoscopic approach has become
the preferred treatment modality. The challenging part of
endoscopic extractioninthis patient isthe location ofthe
fecalith.Inourcase,wefailedtoremovethefecalithinthefirst
pouchoscopy althoughmultipleattemptswere made using
differenttools.
Pouchsinusmaybemanagedbyobservation,endoscopy,
orsurgery.Patientswithpouchsinuseshavebeenhistorically
managedwithanoperativeapproach,includingdrainageor
surgical closingofthe sinus,mucosaladvanced flaps, redo
pouch surgery orpouch excision.4 Although surgical
treat-mentforpouchsinusmightbeeffectiveinexperiencedhands,
theproceduresthemselvesareoftentechnicallychallenging
withthepotentialriskforprocedure-relatedadverseevents.In
ourstudyof65patientswithpouchsinusesfromourgroup,1
weshowedthatendoscopicneedle-knifetherapywasan
effi-caciousandsafeprocedureforpouchsinuses.Withprevious
vastexperienceofthistreatmentmodality,weapplied
ultra-soundguidedneedleknifesinusotomytotreatthepouchsinus
inthispatient,aftertwosessionsofwhichthepouchsinuswas
foundtobecompletedhealedinthefollow-uppouchoscopy.
As shownin ourprevious study,1 theneedle-knife therapy
hasits prosand cons.Endoscopicneedle-knifesinusotomy
holds the benefitsof beingless invasive, relatively easy to
perform.Nohospitalizationisrequired,andpatientshavea
quickrecovery.However,someofpatientsneedtobetreated
inmultiplesessions.Furthermore,thisprocedureshouldbe
performedinexperiencedhands.
Inconclusion,wesuccessfullyappliedendoscopictherapy
inasymptomaticpatientwithalargefecalithtrappedatthe
orifice ofpresacral sinus.Wedemonstrated that this
com-plexsurgicalcomplicationmightbesuccessfullytreatedwith
184
jcoloproctol(rioj).2014;34(3):181–184Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Prof.BoShenholdtheEdandJoeyStoryEndowedChair.
r
e
f
e
r
e
n
c
e
s
1.WuXR,WongRC,ShenB.Endoscopicneedle-knifetherapyfor ilealpouchsinus:anovelapproachforthesurgicaladverse event(withvideo).GastrointestEndosc.2013;78:875–85.
2.LianL,FazioV,ShenB.Endoscopictreatmentforpillbezoars aftercontinentileostomy.DigLiverDis.2009;41:e26–8.
3.MmejeC,BouchardA,HeppellJ.Imageofthemonth. Pharmacobezoar:ararecomplicationafterilealpouch-anal anastomosisforulcerativecolitis.ClinGastroenterolHepatol. 2010;8:A28.
4.AhmedAliU,ShenB,RemziFH,KiranRP.Themanagementof anastomoticpouchsinusafterIPAA.DisColonRectum. 2012;55:541–8.
5.AkbariRP,MadoffRD,ParkerSC,HagermanG,MinamiS, BullardDunnKM,etal.Anastomoticsinusesafterileoanal pouchconstruction:incidence,management,andoutcome. DisColonRectum.2009;52:452–5.