jcoloproctol(rioj).2014;34(3):189–192
Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Review
Article
Management
of
acute
colorectal
diseases
in
febrile
neutropenic
patients
夽
Camila
Perazzoli
a,
Marley
Ribeiro
Feitosa
a,∗,
Lorena
Lobo
de
Figueiredo-Pontes
b,
José
Joaquim
Ribeiro
da
Rocha
a,
Belinda
Pinto
Simões
b,
Omar
Féres
aaDivisionofColoproctology,DepartmentofSurgeryandAnatomy,RibeirãoPretoMedicalSchool,UniversityofSãoPaulo(USP),
RibeirãoPreto,SP,Brazil
bDivisionofHematology,DepartmentofInternalMedicine,RibeirãoPretoMedicalSchool,UniversityofSãoPaulo(USP),RibeirãoPreto,
SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24April2014 Accepted17June2014 Availableonline8July2014
Keywords:
Febrileneutropenia Typhlitis
Analcanal
a
b
s
t
r
a
c
t
Patientswithhematologicmalignanciesare susceptibletoseriouscomplicationsdueto immunosuppression.Neutropenic-relatedinfectionisoneofthemajorcausesofmorbidity andmortalityinthisgroupofdiseases.Febrileneutropeniaisacommoncomplicationof thehematologicneoplasmitselforchemotherapy,andhasworseprognosisifprolonged (lastingmorethan7days)orsevere(neutrophilcountbelow500cellsperL).Amongthe
usualsitesofinfection,wehighlighttheneutropenicenterocolitisandperianalinfectionas gastrointestinalcomplicationsofgreaterinteresttothecolorectalsurgeon.Althoughmost casesrespondtoconservativetreatment,aportionofpatientswillneedsurgeryforcomplete recovery.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Tratamento
das
doenc¸as
colorretais
agudas
no
paciente
neutropênico
febril
Palavras-chave:
Neutropeniafebril Tiflite
Canalanal
r
e
s
u
m
o
Ospacientescomneoplasiashematológicasestãosujeitosaumasériadecomplicac¸ões devidoàimunossupressão.Infecc¸ãoéumasdasprincipaiscausasdemorbidadee mor-talidadenessegrupodedoenc¸as.Aneutropeniafebriléumacomplicac¸ãofrequenteda própriadoenc¸aonco-hematológicaoudaquimioterapia,eapresentapiorprognósticose prolongada(durac¸ãoacimade7dias)ousevera(contagemdeneutrófilosinferiora500 células pormicrolitro).Dentre osfocosde infecc¸ãomaiscomunsdestacamosa entero-coliteneutropênicae ainfecc¸ãoperianalcomocomplicac¸ões demaiorinteresseparao
夽
PerformedattheDepartmentofSurgeryandAnatomy,RibeirãoPretoMedicalSchool,UniversityofSãoPaulo(USP),SãoPaulo,SP, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.R.Feitosa).
http://dx.doi.org/10.1016/j.jcol.2014.06.002
190
jcoloproctol(rioj).2014;34(3):189–192cirurgiãocolorretal.Apesardegrandepartedoscasosapresentarboarespostaaotratamento conservador,umaparceladepacientesnecessitarádecirurgiaparacompletarecuperac¸ão. ©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Febrile
neutropenia
Neutropeniaisacommonfindinginpatientswith hematolog-icalmalignancies.Itoccursasamanifestationofthedisease oraconsequenceofimmunosuppressivetreatment.1Itis
usu-allydefinedasanabsoluteneutrophilcount(ANC)of1500or fewerneutrophilsperLofblood.Patientsaffectedbyacute
leukemia,leukemicphaselymphomas,myelodisplastic syn-dromesandthosereceivinghighintensitychemotherapyor bonemarrowtransplantationconditioningregimensare espe-ciallypronetodevelopsevereneutropeniadefinedbyanANC oflessthan500cells/L.2
Theriskofseriousinfectionissignificantlyhigherif neu-tropeniaissevereorprolonged(morethansevendays)and themostcommonsitesare:skin,venouscatheters,dental dis-eases,oropharynx,gums,paranasalsinuses,lungs,abdomen, genitalsandperianalarea.2 Inflammatoryresponseis
com-promisedinthosepatients,thusfewornosignsmaybefound. Sometimes fever may be the only complaint. In this con-text,theclinicalconditionofFebrileNeutropeniaisdefined asthedetectionofasingleoraltemperaturemeasurement of≥38.3◦Coratemperatureof≥38◦Csustainedoveraone
hour-periodinthe presenceofanANC≤500neutrophils/L
oranANCthatisexpectedtodecreaseto≤500neutrophils/L
duringthenext 48h.Inaddition,neutropenicpatientswho areafebrilebuthavesignsorsymptomsofinfectionshould beequallymanagedasfebrileneutropenicpatients.Prompt recognitionandtreatmentofanyinfectiousprocessiscrucial sincetheclinicalstatusmayrapidlydeterioratetosepsisand death.2
Correct evaluation of patients includes detailed anam-nesis, meticulous physical exams and laboratory tests to determine the severity of the complication and to locate the source of infection. Low-risk patients are those who haveestimatedneutropeniaforno longer than sevendays and no organ failures. In contrast, high-risk patients are thosewithanticipatedprolongedneutropenia,profound neu-tropenia(ANC≤100neutrophils/L)and/orclinicalconditions
suchashypotension,pneumonia,neurologicalsymptomsand abdominalpain. Theindex from the Multinational Associ-ation forSupportiveCareinCancer maybe usedasa risk assessmenttoolwithhighsensitivityandspecificity.3Ofnote,
all high risk patients should be admitted to the hospital andreceiveempiricalintravenouslargespectrumantibiotic therapy.2
Thephysicianmust carefully evaluatethe complaint of abdominalpaininaneutropenicpatientsinceitmayalertfor theoccurrenceofaseveregastrointestinalinfection.Indeed, signs of peritonitis during the evaluation may represent complicationssuchastyphlitis, pseudomembranouscolitis orothercausesofacuteabdomen.4,5Patientsmustalsohave
their perianal region checked for anorectal diseases and
flogosis.Rectalexam should notbeneglectedand invasive proceduresmustbetakenwiththeappropriateconsideration oftheriskofbacterialtranslocationanddiseaseworsening.6
Neutropenic
enterocolitis
Classically known astyphlitis or ileocecal syndrome, neu-tropenic enterocolitis is anecrotizing polymicrobialcolitis, diagnosedalmostexclusivelyinpatientswithneutropenia.7
Theword“typhlon”meanscecuminGreek,neverthelessthe terminal ileumand the whole colon may bealsoaffected. Although this condition is often described as necrotizing enterocolitis,theclinicalpicturemayvaryfromamild, non-necrotizingform,toaseveretransmuralprocesswithahigh riskofdeath.8
Neutropenicenterocolitishasbeenhistoricallyreportedas themostcommongastrointestinalcomplicationinpatients with fever, neutropenia and abdominal pain, affecting as muchas50%ofsuchpatients,whichmortalityratesthatvary from20to50%.9,10
The genesis of this complication waits for complete understanding, however some factors may be involved: chemotherapy cytotoxic effects, damage of gut mucosa, immunosuppression and translocationofvirulent microor-ganisms. The pathologic result is gangrenous necrosis, subserosalgasaccumulationandperforationoftheaffected segment,duetointestinalinfarction.4
Thediagnosisoftyphlitisshouldbepresumedinpatients withsevereneutropenia,abdominalpain(rightlower quad-rant) and fever. Physical exam may evidence abdominal distention and tenderness. Differential diagnosis includes acute appendicitis, psoas abscess and pseudomembranous colitis.5,11Computedtomographyusuallysealsthediagnosis
by revealing thick and dilated bowel walls with mesen-teric stranding.12 Plain films of the abdomen can be used
to detect pneumoperitoneum. Invasive procedures suchas colonoscopy and bariumenema may cause bowel perfora-tionandshouldnotbeattempted.Aflexiblesigmoidoscopy and C. difficile assays may be necessary to rule out pseu-domembranouscolitisinapatientwithimportantdiarrhea associated to abdominal distention and recent history of antibiotictherapy.13
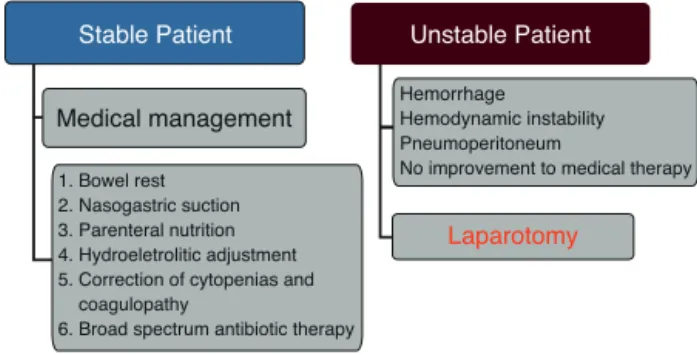
Medicaltreatmentofuncomplicatedtyphlitisconsistsof broad-spectrum antibiotics,bowelrest,nasogastricsuction, hydroeletroliticadjustmentandanemiacorrection(Fig.1).To choose the right empiric antibioticregimen, the physician must:(1)considerthepolymicrobialnatureoftheinfection; (2)evaluatethepatient’sriskfactorsforcomplicatedoutcome; and(3)knowthelocalresistanceofpathogens.2,14Cefepime,
jcoloproctol(rioj).2014;34(3):189–192
191
1. Bowel rest 2. Nasogastric suction 3. Parenteral nutrition 4. Hydroeletrolitic adjustment 5. Correction of cytopenias and coagulopathy
6. Broad spectrum antibiotic therapy
Medical management
Unstable Patient Stable Patient
Hemorrhage Hemodynamic instability Pneumoperitoneum
No improvement to medical therapy
Laparotomy
Fig.1–Neutropenicenterocolitismanagement.
suspectedeitherbybloodculturesorpreviouspatient’s colo-nization,theadditionofanaminoglycosideisrecommended. Theuseofacarbapenemorpiperacillin-tazobactamisalso acceptableasfirstlinetherapy.Metronidazoleorvancomycin shouldbeaddedforsuspectedC.difficileinfection.Theuseof antifungaltherapycanbealsoadvisedinindividualcaseswith persistentand long-termneutropenia andrefractoriness to theantibacterialagent.Finally,supportivecarewith transfu-sionstoimproveanemia,thrombocytopeniaandcoagulation defectsaswellastheuseofgranulocytestimulatingfactors or granulocyteinfusionsshould bealso beconsidered and individualizedtoeachpatient.
Thediseaseisconsideredascomplicatedinthepresence ofbowelperforationwithperitonitis,gastrointestinal hemor-rhageordeteriorationoftheclinicalstatus(suchassepsisor organperfusionimpairment).Forthosecases,surgeryisthe onlyoptionandpatient’slifedependsontheabilityofthe sur-geontoidentifyandremovealldevitalizedtissue.15Usually,a
righthemicolectomywithaterminalileostomyandmucous fistulaappearsto beareasonableoptiongiventhe serious natureofthediseaseatthispoint.16
Anorectal
diseases
Neutropenicpatientsaresusceptibletoanyanorectaldisease. Perianalinfection(representedbyanabscessorinfected fis-tula)isthe mostfeared complication, consideringthe lack ofnaturaldefenseagainstinfectiousmicroorganisms. Man-ifestationsmaydifferfromthosewithacompetentimmune systemandincludemildtosevereanorectalpain,feveranda poorlydefinedindurationoftheanalcanal.Perianalinfection isalife-threateningcomplicationthatrequiresready diagno-sisandinterventionasrecurrenceandmortalityratesmaybe expressive.17Inaseriesof92patientswithacuteorchronic
leukemia,themostcommonmanifestationswereperirectal abscess(27%),followedbyanalfissures(23%),external hem-orrhoids(19%)andperianalulcerations(13%).Only16%ofthe patientsrequiredsurgerymostcommonlytodrain perirec-talabscesses.18Anotherretrospectivestudyof1102patients
foundaperianalinfectionprevalenceof6.7%.Recurrencewas diagnosedin31%ofthecasesand34%ofthepatientsreceived surgicalintervention.19
Conservativemeasuresconsistofsystemicantibiotics,sitz baths,stoolsoftenersandproperanalhygiene.Spectrumof antibioticcoverageshouldbebroadgiventhepolymicrobial
nature of the Infection. In a review of 963 cases of bone marrowtransplantation,themostcommonmicroorganisms wereEscherichiacoli,Bacteroides,Enterococcus,andKlebsiella.20
Surgeryharborstherisksofuncontrolledbleedingandpoor healingbutmaybetheonlychoiceforabscessesandfistulas. Ifanyoperationistobeconsidered,commonsensedictates thedecisiononholdingthechemotherapy.
Conclusions
Patients with neutropenia are predisposed to a variety of infectiousdiseases.Promptrecognitionandearlytreatment ofsuchcomplicationsareessentialforsurvival.Much atten-tionshouldbepaidtotheabdomen,perineumandanorectal area,sincetheycanbethesitesofinfection.Thediagnosis ofneutropenicenterocolitis,anorectalabscesses,orfistulas requires immediateconsultationwithacolorectal surgeon, even though medicalmanagement may be sufficient fora significantportionofcases.Inthepresenceofuncontrolled sepsis, bowel wall perforation, continuous gastrointestinal hemorrhage,surgerybecomesthelastresourceandlifewill dependonthesurgeon’sknife.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KeidanRD,FanningJ,GatenbyRA,WeeseJL.Recurrent typhlitis.Adiseaseresultingfromaggressivechemotherapy. DisColonRectum.1989;32:206–9.
2.FreifeldAG,BowEJ,SepkowitzKA,BoeckhMJ,ItoJI,Mullen CA,etal.Clinicalpracticeguidelinefortheuseof
antimicrobialagentsinneutropenicpatientswithcancer: updatebytheInfectiousDiseasesSocietyofAmerica.Clin InfectDis.2010;52:427–31.
3.UysA,RapoportBL,AndersonR.Febrileneutropenia:a prospectivestudytovalidatetheMultinationalAssociationof SupportiveCareofCancer(MASCC)risk-indexscore.Support CareCancer.2004;12:555–60[Epub2004].
4.KatzJA,WagnerML,GresikMV,MahoneyJuniorDH,Fernbach DJ.Typhlitis.An18-yearexperienceandpostmortemreview. Cancer.1990;65:1041–7.
5.WadeDS,NavaHR,DouglassHO.Neutropenicenterocolitis clinicaldiagnosisandtreatment.Cancer.1992;69:17–23.
6.GrewalH,GuillemJG,QuanSH,EnkerWE,CohenAM. AnorectaldiseaseinneutropenicleukemicpatientsOperative vs.nonoperativemanagement.DisColonRectum.
1994;37:1095–9.
7.RolstonKV,BodeyGP,SafdarA.Polymicrobialinfectionin patientswithcancer:anunderappreciatedand
underreportedentity.ClinInfectDis.2007;45:228–33.
8.BremerCT,MonahanBP.Necrotizingenterocolitisin neutropeniaandchemotherapy:aclinicalupdateandold lessonsrelearned.CurrGastroenterolRep.2006;8:333–41.
192
jcoloproctol(rioj).2014;34(3):189–19210.CardonaAF,RamosPL,CasasbuenasA.Fromcasereportsto systematicreviewsinneutropenicenterocolitis.EurJ Haematol.2005;75:445–6.
11.deBritoD,BartonE,SpearsKL,CranmerHH,KarpSJ,Anglin D,etal.Acuterightlowerquadrantpaininapatientwith leukemia.AnnEmergMed.1998;32:98–101.
12.KirkpatrickID,GreenbergHM.Gastrointestinalcomplications intheneutropenicpatient:characterizationand
differentiationwithabdominalCT.Radiology.2003;226:668–74 [Epub2003].
13.KellyCP,PothoulakisC,LaMontJT.Clostridiumdifficilecolitis. NEnglJMed.1994;330:257–62.
14.AverbuchD,OraschC,CordonnierC,LivermoreDM,Mikulska M,ViscoliC,etal.ECIL4,ajointventureofEBMT,EORTC, ICHS,ESGICH/ESCMIDandELN.Europeanguidelinesfor empiricalantibacterialtherapyforfebrileneutropenic patientsintheeraofgrowingresistance:summaryofthe 20114thEuropeanConferenceonInfectionsinLeukemia. Haematologica.2013;98(December(12)):1826–35,
http://dx.doi.org/10.3324/haematol.2013.091025[Erratumin: Haematologica.2014;99:400].
15.ShambergerRC,WeinsteinHJ,DeloreyMJ,LeveyRH.The medicalandsurgicalmanagementoftyphlitisinchildren withacutenonlymphocytic(myelogenous)leukemia.Cancer. 1986;57:603.
16.MoirCR,ScudamoreCH,BennyWB.Typhlitis:selective surgicalmanagement.AmJSurg.1986;151:563–6.
17.BarnesSG,SattlerFR,BallardJO.Perirectalinfectionsinacute leukemiaImprovedsurvivalafterincisionanddebridement. AnnInternMed.1984;100:515–8.
18.NorthJH,WeberTK,Rodriguez-BigasMA,MeropolNJ,Petrelli NJ.Themanagementofinfectiousandnoninfectious anorectalcomplicationsinpatientswithleukemia.JAmColl Surg.1996;183:322–8.
19.ChenCY,ChengA,HuangSY,ShengWH,LiuJH,KoBS,etal. Clinicalandmicrobiologicalcharacteristicsofperianal infectionsinadultpatientswithacuteleukemia.PLOSONE. 2013;8:e60624,http://dx.doi.org/10.1371/journal.pone.0060624
[Epub2013].