w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
TAMIS
with
partial
excision
of
mesorectum
and
primary
closure
of
rectal
wound
using
vloc
Eduardo
Fonseca
Alves
Filho
a,b,∗,
Paulo
Frederico
de
Oliveira
Costa
a,b,
Alexandre
Lopes
de
Carvalho
a,baBrazilianSocietyofColoproctology,RiodeJaneiro,RJ,Brazil
bHospitalPortuguêsdaBahia,Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11January2015 Accepted20February2015 Availableonline1April2015
Keywords:
TES TAMIS Rectalcancer Vloc
Partialexcisionofmesorectum
a
b
s
t
r
a
c
t
Background:TransanalMinimallyInvasiveSurgeryhasproventobeaviablealternativeinthe treatmentofrectaltumors;however,rectalwoundclosurecanbechallenging.Wedescribe ourexperiencewiththisprocedureusingthevlocsuturedevice.
Resume:EightsuccessfulTransanalMinimallyInvasiveSurgerywithprimarywoundclosure usingvlocwereperformedin5men,62yearsmeanage;allcaseshadpre-operativediagnosis ofadenomawithhigh-gradedysplasia.Thesurgicalanatomic–pathologicresultsshowed6 adenomaswithhigh-gradedysplasiaand2welldifferentiatedadenocarcinomas,limited totheupperthirdofthesubmucosa(pT1SM1)withoutlymphaticorvascularinvasion.All lesionswereresectedwithnegativemargins.Nopatientreportedduringfollow-uprectal pain,fecalincontinenceorbleeding.
Conclusion:TheuseofvlocinrectalwoundclosureduringTransanalMinimallyInvasive Surgeryissecureandfacilitatestheprocedure.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
TAMIS
com
excisão
parcial
do
mesorreto
e
fechamento
primário
da
ferida
retal
usando
vloc
Palavras-chave:
TES TAMIS Câncerretal Vloc
Excisãoparcialdomesorreto
r
e
s
u
m
o
Tema:CirurgiaMinimamenteInvasivaTransanal(TAMIS)temprovadoserumaalternativa viávelparaotratamentodetumoresdoreto,porémofechamentodaferidarectalpode serdesafiadante.Nósdescrevemosnossaexperiênciacomesteprocedimentoutilizandoo dispositivodesuturavloc.
Resumo:OitoTAMISforamrealizadoscomsucessocomofechamentoprimáriodaferida usandovloc,cincohomens,comidademédiade62anos,todososcasostiveramdiagnóstico pré-operatóriodeadenomacomdisplasiadealtograu.Osresultadosanátomo-patológicos
∗ Correspondingauthor.
E-mail:[email protected](E.F.AlvesFilho).
http://dx.doi.org/10.1016/j.jcol.2015.02.001
pós-operatóriodemonstraram:6adenomascomdisplasiadealtograue2adenocarcinomas bemdiferenciados,limitadoaoterc¸osuperiordasubmucosa(pT1SM1),seminvasãolinfática ouvascular.Todasaslesõesforamressecadoscommargensnegativas.Nenhumpaciente relatouduranteoseguimentodorrectal,incontinênciafecalousangramento.
Conclusão: OusodevlocnofechamentodaferidaretalduranteTAMISéseguroefacilitao procedimento.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
TransanalEndoscopicSurgery(TES)hasbeenperformedwith traditional platforms such as TEM (Transanal Endoscopic Microsurgery)andTEO(TransanalEndoscopicOperation)and newertechniqueslike TAMIS(TransanalMinimallyInvasive Surgery).1,2
TAMISprocedureisthetransanaluseofdisposable mul-tiplechannelslaparoscopicports,associatedwiththeuseof ordinarylaparoscopicequipmentandCO2insufflation
(pneu-morectum). It can be performed with various devices like SILSTMport (Covidien), SSLTM(Ethicon), Gelpoint (Applied Medical)oradaptationsofanaldilatorwithsurgicalgloves.2
Theriskoflymphnodeinvolvementinadenocarcinomas limitedtosubmucosa(pT1)is10–34%.3Despiterecentstudies
haveshownthatinthetreatmentofrectaladenocarcinoma, TESis associatedwithhigher recurrence rates when com-paredtoradicalsurgery(2.9–12%ofthe casessubmittedto TESand0.5%submittedtoradicalsurgery),4overallsurvival
ratesdidnotdifferbetweenthetwogroups.Thisisprobably becausepatientsundergoingTESfollowrigoroussurveillance protocolsandwhenrelapseoccurs,theyarereferredtoradical surgeryoradjuvanttreatment.Multicenterstudyconcluded thatTEM can bebeneficial invery selected casesofrectal cancer,taking into account the degree ofpenetration into thesubmucosa(pT1SM1),tumordiameter(less3cm),absence of lymphatic or vascular invasion and well differentiated tumor,3,4 inthissituation localrecurrencerateoflessthan
5%wasreportedwhentreatedbyTES,whichissimilartothe resultsofradicalsurgery,butwithasignificantreductionin morbidityandmortality.
VariableratesofcomplicationsarereportedwithTES, espe-ciallyrelatedtosuturedehiscence.Thisismoreprevalentin patientsundergoingneoadjuvanttherapytherpy.5
TEShasthreesteps.Firststep:initialtransanalinstallation ofthedevice,whenperformingTEMandTEOtheintroduction ofa rigidsurgicalproctoscopyand holdit totheoperating table;thepatientwillbepositionedaccordingtothelocation ofthelesion;inTAMISnoattachmenttotheoperatingtable isnecessaryand thedevice canbesuturedtothe perianal skin; usually it is possible to perform most procedures in thelithotomyposition.Secondstep:excision,whereincases ofpartialthickness resectionisnot necessaryto closethe wound;wecaneasilyidentifythesubmucosaplanedissection withvisualization ofthe circular orientationofthemuscle fibers.IncasesofPartialMesorectalExcision(PME)withfull thicknessresection ofrectal wall, the perirectal fatis also easilyidentified.1
Thirdstep:incasesofPME,usuallyprimarywound clo-sure isindicated, although the possibility to leave it open without major complications is described. The realization ofsutureinanarrow operatingfield,wheretheconflictof toolsfrequentlyoccurs,istoughanditisnotalwayspossible. Severaltechniqueshavebeendescribed:continuoussutures anchoredwithconventionallaparoscopicorsilverclips; auto-maticcontinuoussutures(endostich),separatedstitcheswith extracorporealknot,anchoredstitchesandclosureusing tra-ditional anal retractors. The difficulty or impossibility of woundclosureandtheinadvertentopeningoftheabdominal cavityhavebeen describedforcasesofconversionto tradi-tionaltransanalsurgeryorlaparotomyorlaparoscopy.6
Theobjectiveofthisstudyistoreporttheuseofvlocdevice (Fig.1)toclosetherectalwoundinTAMISprocedure.
Methods
SurgicaltechniqueinstallationofTAMIS
Thepatientunderwentpreviousmechanicalbowel prepara-tion,andtheprocedureisperformedundergeneralanesthesia in the lithotomyposition. Thepatient’s position usuallyis
Fig.2–SILSTMportdevice.
Fig.3–SSLTMportdevice.
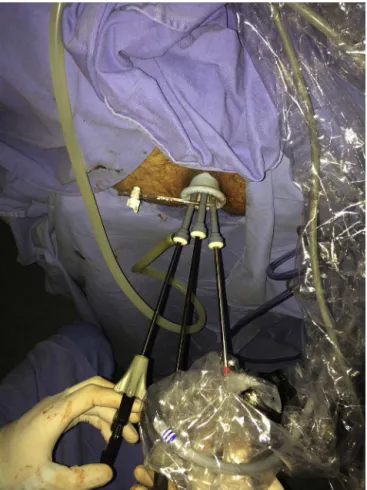
independentofthelocationofthelesions(butinour previ-ousexperience,inoneanteriorbulkylesionwehaveopted totheproneposition).1NextisintroductionofSILSTMport
(Covidien,USA)(Fig.2)orSSLTM(Ethicon,USA)(Fig.3)andone 5mmor12mmopticand2clampsthroughdeviceholesand fixationtotheperianalskin,ifnecessaryandCO2insufflation
tomaintainasatisfactorylevelofrectaldistension(usually 12–15mmHg).
Fig.4–Finalaspectoftherectalwoundclosure.
Dissectionofthelesion
Radial demarcation of the tumor; excision of the lesion, including thefullthickness ofthe rectalwalland adjacent perirectalfat;thisstepcanbeperformedeitherwith conven-tionalelectricscalpelorotherenergysourceslikebipolaror ultrasonicscalpel.IncasesthatusedSILS,wetookthe speci-menouttogetherwiththedevice.ReintroductionofSILSwith newinsufflation.
Closureofwound
Inthesecaseswheretheperirectalfatwasexposed,closureof rectalwallwasperformedusingvlocdevice;afterthe transfix-ationoftheedgesofthewound,theneedleispassedthrough thelooplocatedatitsendstartingacontinuoussuture, tak-ingintoaccountthatthesutureautomaticallyanchorsinthe wound;thankstomicro-spicules,itisnotpossibletoloosen thesutureorreturnthelastpassage.Whenthedefectistoo largeweusedmorethanonesuture.Whenthesutureis fin-isheditisnotnecessarytoperformknotoranchorwithclip, justcutit(Fig.4).Afterreviewinghemostasisandthesuture, withdrawthedevice.
EightPMEprocedureswithprimarywoundclosureusing vlocwereperformedandcomparedbygender,age,indication andsurgicalcomplications,operativetime,numberofsutures, positivemarginsandmortality.a
Results
Eightprocedures were performedin5men,62years mean age, and all caseshad pre-operativediagnosis ofadenoma with high-grade dysplasia. Four had undergone previous colonoscopicpolypectomy(piecemealresection)withpositive margins.
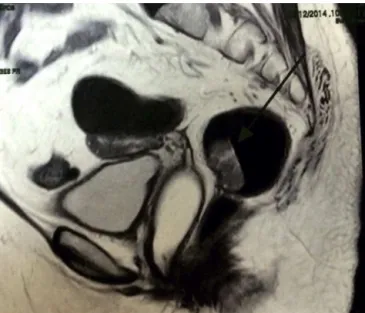
Colonoscopywithbiopsywasperformedinallpatientsand Magnetic Resonance Imaging(MRI) of abdomenand pelvis
aTo watch the video of this procedure access:https://www.
Fig.5–MRIofpelvisshowingrectaltumor.
withaspecificprotocolforstagingofrectaltumors(Fig.5); therewere nosuspicion ofinvasionofmusclelayerofthe rectumorsuspectlymphnodes.
In7casesSILSTMportdevice(Covidien,USA)wasused,and inonecaseSSLTM(Ethicon,USA).Theaveragelesionsizewas 2.5cm.Theaveragedistancefromtheanalvergewas6.2cm.
Themeandurationoftheprocedureswas95min;itwas possibletoperformtheprimaryclosureoftherectaldefectin allcasesusingthevlocsuturedevice(Covidien,USA).An aver-ageof1.5sutureperprocedurewasused;theaveragehospital staywas2.3days.
Theanatomic–pathologicresultsshowed6adenomaswith high-gradedysplasiaand2welldifferentiated adenocarcino-mas,limitedtotheupperthirdofthesubmucosa(pT1SM1) withoutlymphaticorvascularinvasionandnegativelymph nodes; in these 2 casesthe option of radical surgery was offered, but they refused this alternative. All lesions were resectedwithnegativemargins(Fig.6).
No patient reported during follow-up rectal pain, fecal incontinenceor bleeding. One patient had a hemorrhoidal thrombosistreatedwithmedications.Allpatientsunderwent flexiblesigmoidoscopy30daysaftertheprocedure(Fig.7);no dehiscencewoundwasdiagnosed.Therewerenodeaths.The meanfollow-upis11months,withoutrecurrence.No adju-vanttreatmentwasnecessary.
Discussion
When wecompare these resultswithour previous experi-ence(firstseriesinSouthAmerica),performingatotalof12 TAMISprocedures,thewoundclosureusingvlocdeviceseems todecreasesurgicaltimeandavoidtheuseofanalretractors tofacilitatetheclosureoftherectalwalldefect.Thewound closureinTESisgenerallythemostlaboriouspartofthe proce-dureandresponsibleforconversion.Vlocavoidsthenecessity ofintracorporealknotand facilitatesfurtherclosureofthe woundbythecontinuousanchoringasthesuturecontinues.
Fig.6–Surgicalspecimen.
Fig.7–Surgicalpostoperativeviewofscaronrectalwall.
Theuse of morethan onesuturefacilitates theclosure of largerwoundsbecauseitpreventsthenarrowingoftherectal lumenasthesutureisperformed.
Complications occurin about4% ofcasesofTES6,7 and
includebleeding,perforation,wounddehiscence,abscesses, incontinence, stenosis and subcutaneous emphysema. Among all the complications, bleeding and wound dehis-cence are the mostcommon surgicalcomplications (27.4% and 13.7%,respectively), and urinary tract infection is the most common overall complication (21.1%). Most surgical complicationsaretreatedconservativelyandonly2%require additionalprocedures.7–9
25.6% vs 5.3 vs 0%, respectively)5; small dehiscence are
moreprevalent(21%),largedehiscenceareuncommon(4.7%). Marks10alsoreportedthat91%ofdehiscencewastreated
con-servatively,withadiagnosismeantimeof3.8weeks. Thelearningcurveinfluencesonconversionrates, postop-erativecomplicationsandtheheightandsizeoftheresected lesions.9
Highcomplicationratesafterradiotherapy10(57%)have beenreportedwithTES;rectalpainisthemostfrequent man-ifestation(34%)andwasclassifiedasgradeIIandIIIinover70% ofpatients.9 Perezetal.11 showedhighindexofdehiscence
andrectalpainafterradiotherapycomparedtonon-irradiated group (61% vs 23%); the median time from diagnosis was oneweekandaeightweekshealingtime,8%developedlate complications,allafterdiagnosisofsuturedehiscence. Rec-tal stenosishasbeen described in 5%inbothgroups after woundcomplications.Themajority(93%)ofthepatientswere managedconservatively.
Saclarides12drawsattentiontothecareofthewound
clo-sureafterfullexcisionoftherectalwallinTES,astransverse woundclosurewithabsorbablesutures.Multiplesuturesare preferableforclosureoflargewounds;inthesecasesthe revi-sionofthepermeabilityoftherectallumemaftertheendof thesutureisalwaysmandatory,inordertoavoidstenosis.
AquestionthatremainsuncleariswhethertheTES tech-niques are comparable. Prospective studies have not been performedyet,comparingtheformerplatformsandTAMIS. Oneauthor13inanexperimentalstudyreportedthatTAMIS
isrelatedtohighfailurerates(30%)whencomparedtoTEM, incontrastwithreportsbyother authors whohaveshown highsuccessrateswithTAMIS.2 Strangely,itwasdescribed
toothatthetimefortheinstallationofTAMISdeviceisgreater thanTEMorTEO.Inrelationtocosts,contrastingresultshave alsobeendescribed inrelationtothe differentmethodsof TES,withthesereports:TEOD1920,TEMD2310and TAMIS D2220.14
A recent review2 found that 390 procedures had been
described usingTAMIS, the averagelesion sizewas3.1cm, theaveragedistancefromtheanalmarginwas7.6cm, pos-itivemarginsoccurredin4.3%,andfragmentationofsurgical specimensin4.1%.Conversionwasreportedin2.3%ofcases. Complications occurred in 7.4%, the most common being bleeding,pneumo-scrotum,subcutaneousemphysema,fever, suturedehiscenceandperitonealperforation.
TAMIShavebeenmostcommonlyperformedunder gen-eralanesthesia,althoughtheuseofspinalanesthesia15with
goodresultswasdescribed.Wright16reportssafetyreleaseof
thepatientafter48handmightbepossibletoconductTESin dayhospitalsystem.
NewTAMISapplicationsastransanallyproctectomywith TotalMesorectumExcision(TME)2,17seemtobepromisingand
mayindicatethatthemethodissuitableforthetreatmentof advancedrectaltumorsandperhapssuperiortoother tech-niquesofTESinspecificsituations.Improvementofdevices used in TAMIS may allow treatment of lesions located in upperrectum,18correctingthemostimportantlimitationof
themethodwhencomparedwithTEMandTEO.
LiketheothertechniquesofTES,thecarefulselectionof patientswithrectaltumortoundergoPMEbyTAMISiscritical toachievegoodresults.
Conclusion
Weconclude that theuse ofvlocinwoundclosure during TAMISissecureandfacilitatestheprocedure.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AlvesFilhoEF,deOliveiraCostaPF,GuerraJC.Transanal minimallyinvasivesurgerywithsingle-port(TAMIS)forthe managementofrectalneoplasms:apilotstudy.JColoproctol (RioJ).2012;32:402–6.
2.Martin-PerezB,Andrade-RibeiroGD,HunterL,AtallahS.A systematicreviewoftransanalminimallyinvasivesurgery (TAMIS)from2010to2013.TechColoproctol.2014;18:775–88.
3.LeonardD,ColinJ-F,RemueC,JamartJ,KartheuserA. Transanalendoscopicmicrosurgery:long-termexperience, indicationexpansion,andtechnicalimprovements.Surg Endosc.2012;26:312–22.
4.WuY,WuYY,LiS,ZhuBS,ZhaoK,YangXD,etal.TEMand conventionalrectalsurgeryforT1rectalcancer:a
meta-analysis.Hepatogastroenterology.2011;58:365.
5.MarksJH,ValsdottirEB,DeNittisA,YarandiSS,NewmanDA, NwezeI.Transanalendoscopicmicrosurgeryforthe treatmentofrectalcancer:comparisonofwound
complicationrateswithandwithoutneoadjuvantradiation therapy.SurgEndosc.2009;23:1081–7.
6.MorinoM,AllaixME,FamigliettiF,CaldartM,ArezzoA.Does peritonealperforationaffectshort-andlong-termoutcomes aftertransanalendoscopicmicrosurgery?SurgEndosc. 2013;27:181–8.
7.CocoC,RizzoG,MattanaC,GambacortaMA,VerboA,Barbaro B,etal.Transanalendoscopicmicrosurgeryafterneoadjuvant radiochemotherapyforlocallyadvancedextraperitoneal rectalcancer:short-termmorbidityandfunctionaloutcome. SurgEndosc.2013;27:2860–7.
8.DeGraafEJ,DoorneboschPG,TollenaarRA,Meershoek-Klein KranenbargE,deBoerAC,BekkeringFC,etal.Transanal endoscopicmicrosurgeryversustotalmesorectalexcisionof T1rectaladenocarcinomaswithcurativeintention.EurJSurg Oncol.2009;35:1280–5.
9.BarendseRM,DijkgraafMG,RolfUR,BijnenAB,ConstenECJ, HoffC,etal.Colorectalsurgeons’learningcurveoftransanal endoscopicmicrosurgery.SurgEndosc.2013;27:3591–602.
10.MarksJH,ValsdottirEB,DeNittisA,YarandiSS,NewmanDA, NwezeI,etal.Transanalendoscopicmicrosurgeryforthe treatmentofrectalcancer:comparisonofwound
complicationrateswithandwithoutneoadjuvantradiation therapy.SurgEndosc.2009;23:1081–7.
11.PerezRO,Habr-GamaA,LynnPB,SãoJuliãoGP,BianchiR, ProscurshimI,etal.TEMforrectalCAafterneoadjuvantCRT. DisColonRectum.2011;54:545–51.
12.SaclaridesTJ.TEM/localexcision:indications,techniques, outcomes,andthefuture.JSurgOncol.2007;96:644–50.
13.RimondaR,ArezzoA,ArolfoS,SalvaiA,MorinoM.Transanal MinimallyInvasiveSurgery(TAMIS)withSILSTMPortversus TransanalEndoscopicMicrosurgery(TEM):acomparative experimentalstudy.SurgEndosc.2013;27:3762–8.
endoscopicsurgeryinrectalcancer.WorldJGastroenterol. 2014;20(33):11538–45.
15.LeeT-G,LeeS-J.Transanalsingle-portmicrosurgeryforrectal tumors:minimalinvasivesurgeryunderspinalanesthesia. SurgEndosc.2014;28:271–80.
16.WrightCJ.Earlydischargefollowingtransanalendoscopic microsurgeryissafe.JLaparoendoscAdvSurgTech. 2014;24:399–402.
17.WexnerD,BerhoM.TransanalTAMIStotalmesorectal excision(TME)–aworkinprogress.TechColoproctol. 2014;18:423–5.
18.McLemoreEC,WestonLA,CokerAM,JacobsenGR,Talamini MA,HorganS,etal.Transanalminimallyinvasivesurgeryfor benignandmalignantrectalneoplasia.AmJSurg.