www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Time
to
left
ventricular
reverse
remodeling
after
cardiac
resynchronization
therapy:
Better
late
than
never
André
Viveiros
Monteiro
∗,
Mário
Martins
Oliveira,
Pedro
Silva
Cunha,
Manuel
Nogueira
da
Silva,
Joana
Feliciano,
Luísa
Branco,
Pedro
Rio,
Ricardo
Pimenta,
Ana
Sofia
Delgado,
Rui
Cruz
Ferreira
Servic¸odeCardiologiadoHospitaldeSantaMarta---CentroHospitalardeLisboaCentral,Lisboa,Portugal
Received3August2015;accepted22November2015 Availableonline2March2016
KEYWORDS Cardiac resynchronization therapy; Leftventricular reverseremodeling; Timecourse Abstract
Introduction:Leftventricularreverseremodeling(LVRR),definedasreductionofend-diastolic and end-systolic dimensions and improvement of ejection fraction, is associated with the prognosticimplicationsofcardiacresynchronizationtherapy(CRT).ThetimecourseofLVRR remainspoorlycharacterized.Nevertheless,ithasbeensuggestedthatitoccurs≤6months afterCRT.
Objective:Tocharacterizethelong-termechocardiographicandclinicalevolutionofpatients withLVRRoccurring>6monthsafterCRTandtoidentifypredictorsofadelayedLVRRresponse. Methods:Atotalof127consecutivepatientsaftersuccessfulCRTimplantationweredivided into three groups according toLVRR response: Group A, 19 patients (15%) with LVRRafter >6months (lateLVRR);Group B,58patients (46%)withLVRRbefore 6months (earlyLVRR); andGroupC,50patients(39%)withoutLVRRduringfollow-up(noLVRR).
Results:ThelateLVRRgroupwasolder,moreoftenhadischemicetiologyandfewerpatients wereinNYHAclass ≤II.Overall, group Apresented LVRRbetweengroup BandC. Thiswas alsothecasewiththepercentageofclinicalresponse(68.4%vs.94.8%vs.38.3%,respectively, p<0.001),andhospitalreadmissionsduetodecompensatedheartfailure(31.6%vs.12.1%vs. 57.1%,respectively,p<0.001).Ischemicetiology(OR0.044;p=0.013)andNYHAfunctionalclass <III(OR0.056;p=0.063)werethevariableswiththehighestpredictivevalueforlateLVRR. Conclusions:Late LVRR has better clinical and echocardiographic outcomes than no LVRR, althoughwithasuboptimalresponsecomparedtotheearlyLVRRpopulation.Ischemicetiology andNYHAfunctionalclass<IIIarepredictorsoflateLVRR.
©2016SociedadePortuguesa deCardiologia.Publishedby ElsevierEspaña,S.L.U.All rights reserved.
∗Correspondingauthor.
E-mailaddress:[email protected](A.ViveirosMonteiro).
http://dx.doi.org/10.1016/j.repc.2015.11.008
PALAVRAS-CHAVE Terapêutica deressincronizac¸ão cardíaca; Remodelageminversa doventrículo esquerdo;
Evoluc¸ãotemporal
Tempoparaaremodelageminversadoventrículoesquerdo:maisvaletarde doquenunca
Resumo
Introduc¸ão: Aremodelageminversadoventrículoesquerdo(RIVE),definidapelareduc¸ãodas dimensõestelediastólicasetelessistólicasepelamelhoriadafrac¸ãodeejec¸ão,temsido asso-ciadaàsimplicac¸ões prognósticasdaterapiaderessincronizac¸ãocardíaca(TRC).A evoluc¸ão temporaldaRIVEpermaneceumprocessopoucocaracterizado.Noentanto,temsidosugerido queocorreránumperíodo≤6mesesapósTRC.
Objetivos: Caracterizaralongoprazoaevoluc¸ãoecocardiográficaeclínicadospacientes(P) comevidênciadeRIVE,numperíodo>6mesesapósTRC,eidentificarpreditoresdeumaresposta deRIVEtardia.
Métodos: CentoevinteesetePconsecutivos,apósimplantac¸ãobem-sucedidadeTRC,foram divididosemtrêsgrupos,deacordocomarespostadeRIVE:grupoA,19P(15%)comRIVEapós seismeses(RIVEtardia);grupoB,58P(46%)comRIVEantesdosseismeses(RIVEprecoce)e grupoC,50P(39%)semRIVEduranteofollow-up(semRIVE).
Resultados: OgrupodaRIVEtardia eramais velho,tinha maisetiologiaisquémicaemenos PemclasseNYHA≥III.Globalmente,ogrupoAapresentouumgraudeRIVEentreosgruposB eC.Omesmoocorreuemrelac¸ãoaograudarespostaclínica(68,4versus94,8versus38,3%, respetivamente,p<0,001)eàsreadmissõeshospitalarespordescompensac¸ãodainsuficiência cardíaca(31,6versus12,1versus57,1%,respetivamente,p<0,001).Aetiologiaisquémica(OR 0,044;p=0,013)eaclassefuncional<III(OR0,056;p=0,063)foramasvariáveiscommaiorvalor preditorparaaocorrênciadeRIVEtardia.
Conclusões: ARIVEtardiatemumamelhorrespostaclínicaeecocardiográficadoqueaausência deRIVE,emboracomumarespostasubótima,quandocomparadacomapopulac¸ãocomRIVE precoce.AetiologiaisquémicaeumaclasseNYHA<IIIforampreditoresdeRIVEtardia. ©2016SociedadePortuguesadeCardiologia.PublicadoporElsevierEspaña,S.L.U.Todosos direitosreservados.
Introduction
Cardiac resynchronization therapy (CRT) has become an effectivenon-pharmacologicaltreatment forpatientswith impairedleftventricularejectionfraction(LVEF),prolonged QRSdurationandNewYorkHeartAssociation(NYHA) func-tional class ≥III symptoms of heart failure (HF) despite optimal medical therapy. Large multicenter clinical trials have shownthat CRTcan mitigateHFsymptoms, improve exercisecapacityandqualityoflife,reducetheincidence of hospitalizations due to HF and decrease mortality.1---4
Most of these benefits are thought to be related to left ventricular(LV)reverseremodeling(LVRR),aresponse char-acterized by a reduction in LV end-diastolic (LVEDD) and end-systolic(LVESD)dimensionsandvolumesand improve-ment of LV ejection fraction (LVEF).5---7 The time course
of this phenomenon remains poorly characterized. It has beensuggested thatthestructuralandfunctional changes associatedwithLVRRoccurearlyafterCRTandaremore pro-nouncedbeforethe six-monthlandmark, a timebywhich theextent of reverse remodeling hasbeen shown to pre-dictlong-termprognosisinthesepatients.6---9Nevertheless,
avariableproportionofeligiblepatientsfailtorespond ini-tiallybutappeartodevelopLVRRaftersixmonthsfollowing CRTimplantation.ThispopulationwithlateLVRR,whoare notincludedinthealreadyknownproportion(around30%) ofnon-responders toCRT, correspondtoadifferent spec-trumofindividualsthat,tothebestofourknowledge,has
neverbeendirectlyanalyzedinaprospectivestudy.To over-come this limitation,the present study characterizes the timingofLVRRoccurrenceandassessesthelong-term echo-cardiographic andclinical evolution of patientswith LVRR occurring>6monthsafterCRTimplantation.Wealsosought toidentify potentially relatedclinical characteristics that mightpredictalateresponsetoCRT.
Methods
This isa single-centeranalysisofpatients whounderwent successfulCRTdeviceimplantation.Atotalof127 consec-utive CRTrecipientswereincluded andpatientdatawere prospectivelycollectedintheinformationsystemofour car-diology department and analyzed. Patientswere selected for CRT if they met currently recommended criteria: (1) LVEF<35%; (2)symptomsof HF, definedasNYHAclass II---IVdespiteoptimalmedicaltherapy;and(3)QRSduration ≥120 ms.Patientswereclassifiedasischemicinthe pres-enceofsignificantcoronaryarterydisease(>50%stenosisof twoormoreepicardialvesselsor>50%leftmainorproximal left anteriordescendingcoronaryartery stenosis on coro-nary angiographyand/or a history of previous myocardial infarction or revascularization).Other patients were clas-sifiedasnon-ischemic.Allleadswereplacedtransvenously via the subclavian and cephalic route using fluoroscopy. The right ventricular lead was positioned in the apex or midseptum.TheLVleadwasplacedwithanover-the-wire
systemintheposterolateralorlateraltributaryveinofthe coronary sinus depending on the ability to cannulate theveins, pacingthreshold,or diaphragmaticstimulation. The standard settings included an atrioventricular (AV) delayof100ms(sensed)and130ms(paced),withDDDor DDDRmodeand standardlower(50 beats/min)andupper (120---130 beats/min)pacing rates. Extensivedemographic andclinicaldata,includingdeath,NYHAclassand hospital-izationforworseningHForCRTdysfunction,werecollected from medical records. Transthoracic two-dimensional echocardiographicinformationwasassessedatbaseline,six monthsafterCRTdeviceimplantationandthereafteronce a year untilthe endof follow-up. In thisstudy,LVRR was definedasanincrease>10%inLVEFoverbaseline,combined witha>10% reductioninLVEDDandLVESD. Echocardiogra-phic cardiacstructure andfunction wereassessed usinga commerciallyavailableultrasoundsystem(Vivid7andVivid E9;GEVingmedUltrasound,Horten,Norway)equippedwith a 3.5-MHztransducer.LVESD, LVEDDand LVEFwere deter-minedaccordingtostandardtechniquesanddigitallystored for offline analysis in cine-loop format. Interventricular mechanical delay wascalculatedbypulmonary and aortic pulsedDopplermeasurementofthedifferenceintimefrom QRSonsettoonsetofflowinthepulmonaryandaortic out-flow tracts, respectively. LV intraventriculardyssynchrony wasassessed offlineusinga previously validatedsoftware package (EchoPACPC-2Dstrain;GE Healthcare,USA).The cohort was divided according to the time course of LVRR responseintothreegroups:GroupA,presenceofLVRRafter >6months(lateLVRR);GroupB,withLVRRbefore6months (early LVRR); andGroup C,without LVRR during follow-up
(no LVRR). Follow-up data were obtained by review of medicalrecords, outpatient clinical visits, and telephone contact. Ethical and hospital permission were obtained fromtheappropriatelocalauthorities.
Statistical
analysis
SPSS version 21 software (SPSS Inc., Chicago, Illinois) was used for computation. Data are expressed as means ± standard deviation for continuous variables and as frequencies and percentages for categorical variables. Data distribution was tested for normality using the Kolmogorov---Smirnov or Shapiro---Wilk test as appropriate. Missingpatient-levelcovariateswereassumedtobemissing andnoimputationwasperformed.Baselinecharacteristics andoutcomeswerecomparedusingthechi-squaretest or Fisher’sexacttest,whenappropriate,forcategorical varia-blesandtheStudent’sttestortheMann---Whitneytestfor continuous variables. Univariate and multivariate logistic regressionanalysiswasusedtoexaminefor potential pre-dictorsofadelayedLVRR response.Avalueofp<0.05was consideredstatisticallysignificant.
Results
Patientbaselinecharacteristics
Overall,thestudypopulation consistedof127consecutive patientswhounderwentsuccessfulCRTimplantation(aged 63.9±10.7 years, 74.8% male). The mean follow-up was
Table1 Baselineclinicalandechocardiographiccharacteristics.
Baseline Allpatients
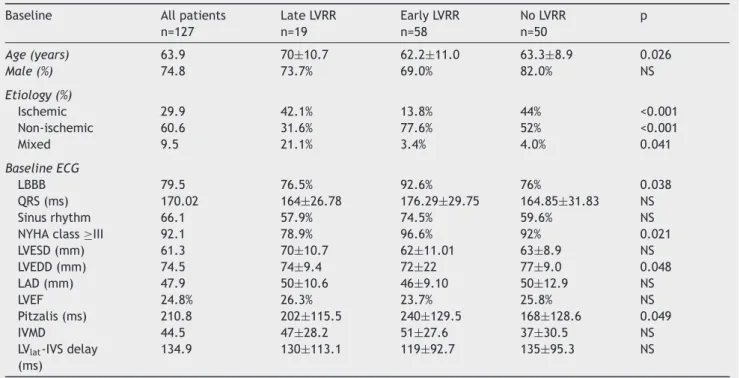
n=127 LateLVRR n=19 EarlyLVRR n=58 NoLVRR n=50 p Age(years) 63.9 70±10.7 62.2±11.0 63.3±8.9 0.026 Male(%) 74.8 73.7% 69.0% 82.0% NS Etiology(%) Ischemic 29.9 42.1% 13.8% 44% <0.001 Non-ischemic 60.6 31.6% 77.6% 52% <0.001 Mixed 9.5 21.1% 3.4% 4.0% 0.041 Baseline ECG LBBB 79.5 76.5% 92.6% 76% 0.038 QRS(ms) 170.02 164±26.78 176.29±29.75 164.85±31.83 NS Sinusrhythm 66.1 57.9% 74.5% 59.6% NS
NYHAclass≥III 92.1 78.9% 96.6% 92% 0.021
LVESD(mm) 61.3 70±10.7 62±11.01 63±8.9 NS LVEDD(mm) 74.5 74±9.4 72±22 77±9.0 0.048 LAD(mm) 47.9 50±10.6 46±9.10 50±12.9 NS LVEF 24.8% 26.3% 23.7% 25.8% NS Pitzalis(ms) 210.8 202±115.5 240±129.5 168±128.6 0.049 IVMD 44.5 47±28.2 51±27.6 37±30.5 NS
LVlat-IVSdelay (ms)
134.9 130±113.1 119±92.7 135±95.3 NS
IVMD:interventricularmechanicaldelay;LAD:leftatrialdiameter;LBBB:leftbundlebranchblock;LVEDD:leftventricularend-diastolic diameter;LVEF:leftventricularejectionfraction;LVESD:leftventricularend-systolicdiameter;LVlat-IVS:leftventricularlateralwallto
interventricularseptum;LVRR:leftventricularreverseremodeling;NYHA:NewYorkHeartAssociation;Pitzalis:LVdyssynchronybythe Pitzalismethod.Amixedetiologywasdefinedasthepresenceofbothischemicandnon-ischemiccauses.
Table2 Echocardiographiccharacteristicsatfollow-up. Follow-up Allpatients
n=127 LateLVRR n=19 EarlyLVRR n=58 NoLVRR n=50 p LVESD(mm) 53.53±13.56 53±11.80 49±12.93 63±11.04 <0.001 LVEDD(mm) 69.31±12.45 68±10.05 66±12.33 77±11.12 <0.001 LAD(mm) 47.38±10.76 54±10.04 44±9.26 50±11.22 <0.001 LVEF(%) 38.48±11.04 41±7.73 43±9.35 27±6.32 <0.001
LAD:leftatrialdiameter;LVEDD:leftventricularend-diastolicdiameter;LVEF:leftventricularejectionfraction;LVESD:leftventricular end-systolicdiameter;LVRR:leftventricularreverseremodeling.
48±36months(median37months).Baselinepatient char-acteristicsareshowninTable1.Themajorityofthecohort (60.6%)hadnon-ischemiccardiomyopathy.
Regarding differences between groups, late LVRR patientswereolderthanthoseinGroupsBandC(70years vs. 62.2 years vs. 63.3 years, respectively, p=0.026) and fewer were in NYHA class ≥III (78.9% vs. 96.6% vs. 92%, respectively, p<0.021). Group B, with an early favorable CRT response, were younger than those in Groups A and C (62.24 years vs. 70 years vs. 63 years, respec-tively, p=0.026), less often had ischemic etiology (13.8% vs. 42.1% vs. 44%, respectively, p<0.001), included more patients with left bundle branch block (LBBB) (92.6 vs. 76.5 vs. 76, respectively, p=0.038) and showed more LV dyssynchrony (240±129.5 vs. 202±115.5 vs. 168±128.6, respectively,p=0.049)asevaluatedbythePitzalismethod. Group C, the non-responders, had more patients with ischemicetiologythanGroupsAandB(44vs.13.8vs.42.1, respectively,p<0.001),andhadgreaterLVEDD(77±9.02vs. 74±9.38 vs. 72±22 mm, respectively, p=0.048) and less previous LV dyssynchrony (168±128.6 vs. 202±115.5 vs. 240±129.5ms, respectively, p=0.049),as assessed bythe Pitzalismethod.Nostatisticallysignificantdifferenceswere detectedinotherelectrocardiographicorechocardiographic parameters.
Echocardiographicandclinicalchanges aftercardiacresynchronizationtherapy
Comparison between groups of echocardiographic data from the last evaluation during follow-up is displayed in Table 2. After CRT implantation, LVRR occurred in 77 (60.6%) patients. The time course of LVRR was different within this population, with 19 patients having late LVRR (Group A), and 58 patients having evidence of earlyLVRR (GroupB). Asignificant differencewasnoticed betweengroupsintermsoftheextentofLVRRresponse.At thelastechocardiographicevaluation,comparedtoGroups A and C, Group B presented lower LVEDD (66±12.33 vs. 68±10.05vs.77±11.12mm,respectively, p<0.001),lower LVESD(49±12.9vs.53±11.8vs.63±11.0mm,respectively, p<0.001), higher LVEF (43±9.4 vs. 41±7.73 vs. 27±6.3%, respectively, p=<0.001) and smaller left atrial diameter (44±9.3vs.54±10.0vs.50±11.2,respectively,p<0.001).
Regardingclinicaloutcomes,duringthemeanfollow-up of 48±36 months, both groups A and B presented bet-ter clinical status than Group C (Figure 1). The clinical
Clinical responders (%) Hospital readmissions (%) Cardiac death (%) <0.001 <0.001 0.010 0 20 40 60 80 100
C-No LVRR B-Early LVRR A-Late LVRR
Figure1 Clinicaloutcomesduringfollow-up.LVRR:left
ven-tricularreverseremodeling.
response to CRT, defined as a sustained improvement in NYHA functional class,was more evident in group Bthan ingroups AandC(94.8%vs.68.4%vs.38.3%,respectively, p<0.001).GroupBsubjectswerealsolessoftenhospitalized for worseningofHFsymptoms(12.1%vs.31.6% vs.57.1%, respectively,p<0.001).GroupCshowedhighercardiac mor-talitycomparedtoGroupsAandB(28.6%vs.5.6%vs.7.3%, respectively,p=0.010).
Predictorsoflateleftventricularreverse remodeling
Inordertoidentifycharacteristicsthatmighthaveanimpact on the time course of LVRR after CRT, a logistic regres-sionanalysiswasperformedtopredictalateLVRRresponse (Table3).Ischemicetiology(oddsratio[OR]0.044;p=0.013) andNYHAfunctionalclass≤II(OR0.056;p=0.063)werethe baseline variables withthe highest predictive value for a lateLVRRresponsetoCRT.
Table 3 Multivariate baseline predictors of late reverse
remodelingresponse.
OR p
Etiology 0.044 0.013
NYHAclass<III 0.056 0.063
Discussion
The majorfindingsof thepresentstudy,whichfocusedon the impact of the time course of LVRR after CRT, are as follows:first,themajorityofpatients(60.6%)presented evi-dence of LVRR during long-term follow-up; second, 14.9% showed LVRR only six months after CRT; third, late LVRR patientswereolderandmoreoftenhadischemicetiology, and fewerwere inNYHA class≥III; fourth, lateLVRR was significantlyassociatedwithbetterclinicaland echocardi-ographicoutcomesthannoLVRR,althoughwithasuboptimal response compared with the early LVRR population; and finally,ischemicetiologyandNYHAfunctionalclass≤IIwere independentpredictorsoflateLVRR.
Severalstudieshaveaddressedthefavorableimpactof CRTinmid-andlong-termfollow-up,whichusuallyoccursin thefirstsixmonthsafterimplantation.10---15The underlying
mechanism responsible for this early improvement seems to be the LVRR response initiated soon after biventricu-lar pacing.5---7 Van de Veire et al., analyzing 49 patients
scheduled for CRT, documenteda decreaseof ≥15% in LV end-diastolicvolumein47%ofpatientsinthefirst48hours after device implantation.15 Nina et al., in a review of
222consecutivepatientswithHFimplantedwithaCRT sys-tem,reportedasignificantincreaseinLVEFandadecreasein LVend-diastolicvolume(LVESV)acutelyafterimplantation followed by an additional improvement in these parame-ters at six-month follow-up.16 Wang et al., in a study of
30patientsscheduledforCRT,revealedadecreaseof≥15% inLVESVbeforesixmonthsin60%ofthepopulation.17Also,
Sanderson etal.,in areport of30 patients scheduledfor CRT,revealedanincreaseof≥15%inLVESVatthreemonths after implantationin 56.7% of thepopulation.18 However,
tothebestofourknowledge, noreportshave focusedon LVRRdocumentedonlyaftersixmonths.Therearenostudies demonstratingdifferencesinthelong-termprognosisofthis groupcomparedwithearlyreverseremodeling.Piresetal., inarelatedstudyof313HFpatientsfromtheMIRACLE-ICD trial, compared early (1---3 months) and late(six months) clinicalresponseafterCRTandcorrelateditwiththe pres-enceorabsenceofLVRR,butnosignificantdifferencewas found.19
Despite being a recognized therapy with a favorable influence on NYHA functional class,quality-of-life scores, rehospitalizationsandcardiacdeath,thereareasignificant proportionofpatients, estimatedat 30%,whoare consid-eredclinicalnon-responderstoCRT.20---22Thispopulationhas
beenextensivelystudiedinpreviousreportsandmany fac-torshavebeenproposedaspotentialcontributorstoalack ofresponse.Inthisstudywefound thatadelayedreverse remodeling responseafter six months shares some of the variablesthatarepresentinnon-responders.
Patientswith an LVRR response, in fact, also had less conventionalelectricaldyssynchrony(i.e.shorterQRS inter-val),eventhoughnotstatisticallysignificant,andlesssevere mechanical dyssynchrony evaluated by echocardiography at baseline.Although the PROSPECT trial showed modest sensitivityandspecificityofechocardiographicparameters of dyssynchrony,23 subanalysis including286 patientsfrom
theoriginalPROSPECTcohortthatfocusedonthreesimple preproceduralmeasuresofdyssynchronyreportedastrong
associationoftheirparameterswithmoreextensivereverse remodeling at 6-month follow-up.24 LBBB is clearly more
evident inearly LVRR patients.25,26 In ourstudy,Groups B
andChadahigherincidenceofischemicetiology.Several previous studies have shown less clinical and LV function improvementinischemicpatients,probablyduetothe pres-enceofmyocardialscartissueinthevicinityofthepacing lead,limitingthe extent ofLVRR regardless of theextent ofbaselinedyssynchrony.20---22Pressureandvolumeoverload
associatedwithLVinvolvementtypicalofHFpatientsleads togradualfibrosis,leftatrial(LA)enlargementand subse-quentlymitralregurgitation.Inthisreport,asstatedinother studies,anincreasedinLAsizewasalsocorrelatedwithlate ornoremodeling.27,28
Thosewhorespondedearlywithreverseremodelingwere moresymptomaticandalsohadhigherLVsystolicand dia-stolicdimensionsatbaseline,suggestingthatsickerpatients have more to benefit from CRT. There are other factors that could help to explain the difference in LVRR. Iden-tification and treatment of reversible causes in the first six months after CRT,such as AV andVV delays and sub-optimal HF therapy, could transform a late into an early response.Furthermore,factorssuchasthepositionofthe LVlead,optimizationofdeviceprogrammingandthe pres-enceofrhythmabnormalitiescouldberelatedtoadelayed response,butwerenotanalyzedinthisreport.
Regarding clinical outcomes during follow-up, the achievement of LVRR, regardless of duration of CRT, was followed by symptomatic and prognostic improvement as demonstratedbya sustaineddecreasein NYHAfunctional class, fewer hospitalizations due to HF worsening and less cardiac deaths compared to non-responders. Poten-tial underlying factors could be the restoration of inter-and intraventricular synchrony and improvements in con-tractilityandhemodynamics.Theseresultsareinlinewith previouslydescribedlong-termpositiveoutcomesofreverse remodelingobtainedbyCRT.5---7However,analyzingearlyand
lateLVRRresponses,itisclearthatclinicalbenefitsaremore pronounced in the early group. This could be explained, in part, by the less intense LVRR response achieved in GroupA,withasmallerimpactonLVdimensions andLVEF comparedwithGroupB.Nevertheless,long-termoutcomes of late LVRR patients are significantly better than non-responders.
ThemechanismofadelayedresponsetoCRTiscomplex andprobablymultifactorial,withnoconclusiveexplanation currently available. Proper selection of a suitable subset of patients is mandatory, since it appears that sicker HF patientsmayrespondbettertoCRT.Accordingtoour find-ings,ischemicetiologyandNYHAfunctionalclass<IIIwere the only baseline features with predictive value for the occurrenceofadelayedLVRRresponsetoCRT.
Limitations
The present study had some limitations. First, it was a single-center retrospective cohort, albeit representative of real-world clinical practice. Second, the definition of LVRR,alsousedinpreviousstudies,30 requiredacut-offof
10% reduction in LV dimensions and an increase of 10% in LVEF. Other studies were stricter and used a 15%
threshold.29,30 Third, clinical response was based only on
improvementinNYHAclassanddidnotincludeassessment offunctionalcapacityorqualityoflifescores.Fourth, echo-cardiographicparametersdependontheoperatorandthere will always be a degree of intra- and interobserver vari-ability.Fifth,otherparameterssuchaspositionofLVlead, deviceprogramming,presenceofrhythmabnormalitiesand levelsof brainnatriureticpeptide (BNP)were incomplete andthuswerenotconsideredforthepresentstudy.Finally, because of the modest number of patients studied, the currentfindingsregardinglateLVRRpredictorsneed confir-mationinlarge-scaleprospectivestudies.
Conclusions
Ourdataconfirm,likeotherreports,thatCRTisassociated withfavorableclinicalandechocardiographicresponses dur-inglong-termfollow-up.This studyisthefirstofthiskind to analyze the time course of LVRR and to characterize the impact of a delayed reverse remodeling response in long-term follow-up. Late LVRR is significantly associated withbetter clinical andechocardiographic outcomesthan no LVRR, although with a suboptimal response compared to the early LVRR population. Improvement in HF symp-tomsandsurvivalafterCRTareproportionaltothetiming andextent of LVRR response.Among allbaseline parame-ters studied, ischemic etiology and NYHA functional class ≤IIwereidentifiedaspredictorsoflateLVRR.Better selec-tionofsuitablepatientsmaypotentiallyimprovetherateof earlyCRTresponders.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Right to privacy and informed consent.The authors declarethatnopatientdataappearinthisarticle.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.PiresLA,GhioS,ChungES,etal.Relationshipbetweenacute improvementinleftventricularfunctionto6-monthoutcomes aftercardiacresynchronizationtherapyinpatientswithchronic heartfailure.CongestHeartFail.2011;17:65---70.
2.Cazeau S,LeclercqC,Lavergne T,et al.Effects ofmultisite biventricularpacinginpatientswithheartfailureand intraven-tricularconductiondelay.NEnglJMed.2001;344:873---80. 3.ClelandJG,DaubertJC,ErdmannE,etal.Theeffectofcardiac
resynchronizationonmorbidityandmortalityinheartfailure. NEnglJMed.2005;352:1539---49.
4.Young JB, Abraham WT, Smith AL, et al. Combined cardiac resynchronizationandimplantablecardioversiondefibrillation inadvancedchronicheartfailure:theMIRACLEICDtrial.JAMA. 2003;289:2685---94.
5.Sutton MS, Keane MG. Reverse remodelling in heart fail-ure with cardiac resynchronisation therapy. Heart. 2007;93: 167---71.
6.St John Sutton MG, Plappert T, Abraham WT, et al. Effect ofcardiac resynchronizationtherapy onleft ventricu-lar size and function in chronic heart failure. Circulation. 2003;107:1985---90.
7.SuttonMG, PlappertT, Hilpisch KE,et al. Sustainedreverse leftventricularstructuralremodelingwithcardiac resynchro-nization at one year is a function of etiology: quantitative Doppler echocardiographic evidence from the Multicenter InSyncRandomizedClinicalEvaluation(MIRACLE).Circulation. 2006;113:266---72.
8.YpenburgC,vanBommelRJ,BorleffsCJ,etal.Long-term prog-nosisaftercardiacresynchronizationtherapyisrelatedtothe extentofleftventricularreverseremodelingatmidterm follow-up.JAmCollCardiol.2009;53:483---90.
9.Yu CM,BleekerGB, Fung JW, etal. Leftventricularreverse remodeling but not clinicalimprovement predicts long-term survival aftercardiac resynchronizationtherapy. Circulation. 2005;112:1580---6.
10.BreithardtOA,StellbrinkC,KramerAP,etal.Echocardiographic quantificationofleftventricularasynchronypredictsanacute hemodynamic benefit of cardiac resynchronization therapy. JAmCollCardiol.2002;40:536---45.
11.DohiK,Suffoletto MS,SchwartzmanD,etal.Utility of echo-cardiographicradialstrainimagingtoquantifyleftventricular dyssynchronyandpredictacuteresponsetocardiac resynchro-nizationtherapy.AmJCardiol.2005;96:112---6.
12.GorcsanJ3rd,KanzakiH,BazazR,etal.Usefulnessof echo-cardiographictissuesynchronizationimagingtopredictacute responsetocardiacresynchronizationtherapy. AmJCardiol. 2004;93:1178---81.
13.Kass DA, Chen CH, Curry C, et al. Improved left ventricu-larmechanicsfromacuteVDDpacinginpatientswithdilated cardiomyopathyandventricularconductiondelay.Circulation. 1999;99:1567---73.
14.Marsan NA, Bleeker GB, Ypenburg C, et al. Real-time three-dimensionalechocardiographypermitsquantificationof left ventricularmechanical dyssynchrony and predicts acute response to cardiac resynchronization therapy. J Cardiovasc Electrophysiol.2008;19:392---9.
15.Veire van de N, BleekerGB, Ypenburg C, et al. Usefulness oftriplane tissueDopplerimagingto predictacuteresponse tocardiacresynchronizationtherapy.AmJCardiol.2007;100: 476---82.
16.Marsan NA, Bleeker GB, Bommel RJ, et al. Comparison of timecourseofresponsetocardiacresynchronizationtherapy inpatientswithischemicversusnonischemiccardiomyopathy. AmJCardiol.2009;103:690---4.
17.Wang CL, Wu CT, Yeh YH, et al. Recoordination rather than resynchronization predicts reverse remodeling after cardiac resynchronization therapy. J Am Soc Echocardiogr. 2010;23:611---20.
18.Sanderson JE, Yu CM.Can cardiacresynchronization therapy causeharm?EurHeartJ.2012;33:816---8.
19.PiresLA,AbrahamWT,YoungJB,etal.MIRACLEand MIRACLE-ICDInvestigators.Clinicalpredictors and timingofNewYork HeartAssociationclass improvementwithcardiac resynchro-nization therapy in patients with advanced chronic heart failure:resultsfromtheMulticenterInSyncRandomizedClinical Evaluation (MIRACLE) and Multicenter InSync ICD Random-ized Clinical Evaluation (MIRACLE-ICD) trials. Am Heart J. 2006;151:837---43.
20.Díaz-Infante E, Mont L, Leal J, et al. Predictors of lack of response to resynchronization therapy. Am J Cardiol. 2005;95:1436---40.
21.Brunet-BernardA, LeclercqC,Donal E.Definingpatients at-risk of non-response to cardiac resynchronization therapy. Value of rest and exercise echocardiography. Int J Cardiol. 2014;171:279---81.
22.Zaca V, Mondillo S, Gaddi R, et al. Profiling cardiac resyn-chronizationtherapypatients:responders,non-respondersand thosewhocannotrespond---thegood,thebadandtheugly?Int JCardiovascImaging.2011;27:51---7.
23.Chung ES, Leon AR, Tavazzi L, et al. Results of the Pre-dictors of Response to CRT (PROSPECT) trial. Circulation. 2008;117:2608---16.
24.VanBommelRJ,BaxJJ,AbrahamWT,etal.Characteristicsof heartfailurepatientsassociatedwithgoodandpoorresponse tocardiacresynchronizationtherapy:aPROSPECT(Predictors ofResponsetoCRT)sub-analysis.EurHeartJ.2009;30:2470---7. 25.Zareba W, Klein H, Cygankiewicz I, et al. Effectiveness of cardiac resynchronization therapy by QRS morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation. 2011;123:1061---72.
26.GoldMR,ThébaultC,LindeC,etal.EffectofQRSdurationand morphologyoncardiacresynchronizationtherapyoutcomesin mildheartfailure:resultsfromtheResynchronizationReverses RemodelinginSystolicLeftVentricularDysfunction(REVERSE) study.Circulation.2012;126:822---9.
27.Rossi A, Cicoira M, Zanolla L, et al. Determinants and prognosticvalueofleftatrialvolumeinpatientswithdilated cardiomyopathy.JAmCollCardiol.2002;40:1425.
28.Giannuzzi P, Temporelli PL, Bosimini E, et al. Independent and incremental prognostic value of Doppler-derived mitral deceleration time of early filling in both symptomatic and asymptomaticpatientswithleftventriculardysfunction.JAm CollCardiol.1996;28:383---90.
29.RafieR,NaqviTZ.Echocardiography-guidedbiventricular pace-maker optimization: role of echo Doppler in hemodynamic assessment and improvement. Expert Rev Cardiovasc Ther. 2012;10:859---74.
30.Gorcsan J, Marek JJ, Onishi T. The contemporary role of echocardiography in improving patient response to car-diac resynchronizationtherapy. CurrCardiovascImagingRep. 2012;5:462---72.