w w w . r b o . o r g . b r
Original
Article
Evaluation
of
the
results
from
arthroscopic
tenodesis
of
the
long
head
of
the
biceps
brachii
on
the
tendon
of
the
subscapularis
muscle
夽
Marcelo
Baggio
a,∗,
Fabrício
Martinelli
a,
Martins
Back
Netto
b,
Rafael
Olívio
Martins
b,
Romilton
Crozetta
da
Cunha
b,
Willian
Nandi
Stipp
baUniversidadedoSuldeSantaCatarina,Tubarão,SC,Brazil
bOrtoimagemCentrodeOrtopediaeImagem,Tubarão,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received7March2015 Accepted5May2015
Availableonline3February2016
Keywords: Tenodesis Arthroscopy Rotatorcuff
a
b
s
t
r
a
c
t
Objectives: Theaimofthisstudywastoevaluatetheresultsfromarthroscopictenodesisof thelongheadofthebicepsbrachii(LHBB)onthetendonofthesubscapularismuscle,with regardtothepresenceofpain,subscapularislesion,presenceofPopeye’ssignandpatient satisfaction.
Methods:A prospective cohortstudy wasconductedon 32 patients withLHBB lesions, through preoperative interviews and physical examinations,which were repeated six monthsaftertheoperation.Themainvariablesstudiedwerethebellypress,bearhugand lift-offtests,Popeye’ssign,anteriorpainandsatisfaction.ThedatawereenteredintoEpi Info3.5.4andSPSS18.0.Inordertoinvestigatethevariablesofinterest,thechi-square, Stu-denttandKruskal–Wallistestswereused.Theconfidenceintervalwas95%andpvalues lessthan0.05weretakentobestatisticallysignificant.
Results:32patientsofmedianage57.5yearswereevaluated.Anteriorpainwasreportedby oneintervieweeaftertheoperation.Thetestsforevaluatingsubscapularislesionsdidnot showanydamagetothismusculatureafterthesurgery.Popeye’ssignwasnegativeinall thepatients.Thepatientsatisfactionratereached90.6%oftheinterviewees.
Conclusion: Thisstudyshowedthatthenewsurgicaltechniquedescribedherepresented excellentperformance,withoutanysubscapularislesionandwithoutidentifyingPopeye’s sign.Only3.1%ofthepatientshadcomplaintsofresidualpain.Thehighlevelofsatisfaction amongthepatientsafterthesurgeryconfirmstheresultspresented.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedattheHospitalandMaternidadeSocimedandatHospitalNossaSenhoradaConceic¸ão,Tubarão,SC,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](M.Baggio).
http://dx.doi.org/10.1016/j.rboe.2016.01.006
Avaliac¸ão
dos
resultados
da
tenodese
artroscópica
do
cabo
longo
do
bíceps
braquial
no
tendão
do
músculo
subescapular
Palavras-chave: Tenodese Artroscopia Manguitorotador
r
e
s
u
m
o
Objetivos: Avaliarosresultadosdatenodeseartroscópicadocabolongodobícepsbraquial (CLB)notendãodomúsculosubescapularquantoàpresenc¸adedor,lesãodosubescapular, presenc¸adosinaldePopeyeesatisfac¸ãodopaciente.
Métodos: Foifeitaumacoorteprospectivacom32pacientescomlesãodoCLB,pormeio deentrevistaeexamefísicopré-operatórioetambémapósseismesesdoprocedimento cirúrgico.AsprincipaisvariáveisestudadasforamtestesBellyPress,BearHugeLift-Off, sinaldePopeye,doranterioresatisfac¸ão.OsdadosforaminseridosnoEpiInfoTM3.5.4e SPSS18.0.Paraverificarasvariáveisdeinteresseostestesqui-quadrado,tdeStudente deKruskal-Wallisforamusados.Ointervalodeconfianc¸afoide95%eforamconsiderados estatisticamentesignificativosvaloresdep<0,05.
Resultados: Foramavaliados32pacientescommedianade57,5anos.Adoranterior pós-operatóriafoireferidaporumentrevistado.Ostestesavaliadoresdelesãodosubescapular nãomostraramcomprometimentodessamusculaturaapósacirurgia.OsinaldePopeyefoi negativoem100%dospacientes.Aporcentagemdesatisfac¸ãodospacientesalcanc¸ou90,6% dosentrevistados.
Conclusão:Esteestudoapresentouumótimodesempenhodanovatécnicacirúrgicadescrita, semlesãodosubescapularesemidentificac¸ãodesinaldePopeye.Adorresidualfoiqueixada porapenas3,1%dospacientes.Aelevadasatisfac¸ãodospacientesapósacirurgiaconfirma osresultadosapresentados.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
The tendon ofthe long head of the biceps brachii (LHBB) isafrequentlocationforpaininpathologicalconditionsof theshoulder.Itsfunctioninvolvesdepressionoftheheadof thehumerusontheglenoidandsupinationtheforearmand, whenthisissupinated,elbowflexionisenabled.1
MostinjuriestotheLHBBoccursecondarilytodegeneration andtofrictionbetweentheanterosuperiorregionofthe rota-torcuffandthecoracoacromialarch.2Theseinjuriesresultin tendinopathy/tendinitis,whichmayevolvetopartialortotal tearingandinstabilityofthebiceps.3
Wheninsituationsoffailureofconservativetreatmentfor LHBBinjuries(suchasanalgesia,restandphysiotherapy), sur-gicalmeasuresareproposed.Amongtheoptionsforsurgical treatmenttenotomyand varioustechniquesforbiceps ten-odesiscanbehighlighted.4
Thedataintheliteraturearedivergent regardinguseof tenotomyortenodesisfortheLHBB.Althoughbothofthese techniques present positive results, there is still no con-sensusregardingthebestmethodforsurgicalcorrectionof theseinjuries.Therefore,itbecomesimportanttoevaluatethe resultsfromnewtechniquesforsurgicalcorrectionthatmight addanothertherapeuticavenue.
The objective of this study was to evaluatethe results fromarthroscopictenodesisoftheLHBBinthetendonofthe subscapularismuscleregardingthepresenceofpostoperative anteriorpain, presenceoftheestheticdeformityknown as Popeye’ssignaftertheoperationandpatientsatisfactionafter sixmonthsofpostoperativerecovery.
Material
and
methods
Aprospectivecohortstudywasconductedon32patientswho were followedup betweenJanuaryandAugust 2014.These patientsunderwentarthroscopictenodesisoftheLHBBonthe subscapularisbymeansofthetechniquedescribedbelow.
Thisstudywasauthorizedbytheethicscommitteesofthe institutions involved.Data were gathereddirectly from the patientswhounderwentthisoperation,bymeansofa ques-tionnaireandaphysicalexamination,aftertheyhadsigneda freeandinformedconsentstatement.
The patients underwent surgery without the examiner knowingwhichsurgicalprocedurewouldbeperformed.This wasdecidedbytheorthopedistduringtheoperation.
Individualsofbothsexesandanyagegroupwhopresented LHBBinjurieswereincludedinthestudy.Theseanatomical criteriawereevaluatedbymeansofmagneticresonance imag-ing(MRI).Patientswhopresentedinjuriestothesubscapularis tendon and those who didnot return for reevaluation six monthsaftertheoperationwereexcluded.
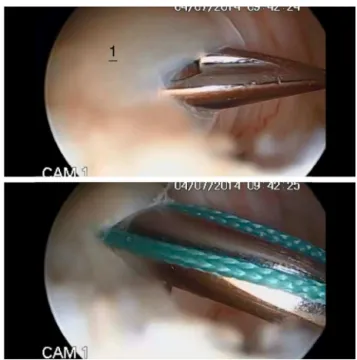
Fig.1–Arthroscopicimageshowinginflammationofthe longheadofthebicepsbrachii.1,Tenosynovitisofthelong headofthebicepsbrachii.
upper-limb position that the patient attained during the examinationwasused,describedasdifferentlevels.
Thedatathus gatheredwere inserted inthe Epi InfoTM version3.5.4and SPSS18.0 software.Toinvestigate associ-ationsbetweenthevariablesofinterest,thechi-squaretest or Student’st testwas appliedto evaluatemeans and the Kruskal–Wallis test to compare medians. Prevalence ratios with95%confidenceintervalswerecalculated.pvalues<0.05 wereconsideredtobestatisticallysignificant.
Surgical
technique
The patients underwent videoarthroscopy of the shoulder positioned inlateral decubitus. Theprocedure was started throughaposteriorportal,intowhichtheopticaldevicewas introduced.ThejointwasinspectedandtheinjurytotheLHBB andpossibleassociatedinjurieswereviewed(Fig.1). Follow-ingthis,ananteriorportalwasconstructedinordertoemplace acannulaforuseinthework.Usingbird-beaktweezersand Ethibond®orOrthocord®thread,thetendonoftheLHBBwas transfixed1.5cmfromitsorigin(Fig.2)andaloopedstitchwas made(Fig.3).TenotomyoftheLHBBwasperformedcloseto itsorigin(Fig.4).Followingthis,oneoftheendsofthethread wasalsousedtotransfixtheupperportionofthetendonof thesubscapularis,usingbird-beaktweezers(Fig.5).Suturing wasperformedwithaknotpusherusingalternatingsimple stitchesand,lastly,theknotendswerecut(Fig.6).
Note:ForNationalHealthSystem(SUS)patients,Ethibond® thread was used, and for health insurance patients, Orthocord®threadwasused.
Results
Beforetheoperation,128patientswhowere candidatesfor shouldersurgerywereevaluated.Ofthese,67didnotundergo the surgical procedure described above. The remaining 61 underwent this procedure and 32 of them returned for the postoperative reevaluation. Among these reevaluated patients,18(56.3%)weremale,allwithright-limbdominance. Thepatients’agesrangedfrom43to75years,withamedianof
Fig.2–Arthroscopicimageinwhichthelongheadofthe bicepsbrachiiistransfixed1.5cmfromitsorigin.1, Bird-beaktweezersusedtotransfixthelongheadofthe bicepsbrachiiwithasuturingthread.
Fig.3–Arthroscopicimageshowingtheloopedstitch performedonthelongheadofthebicepsbrachii.1, Humerus;2,loopedstitchonthelongheadofthebiceps brachii.
57.5years.In16cases(50%),theinjurywastrauma-relatedand in93.8%(15)ofthese,thecausewasafall.Theother16(50%) presentednon-traumaticfactors asthecause ofthe injury. Therightlimbwasinjuredmorefrequently,in71.9%(23)of thecases.
Beforethe operation,71.9%ofthepatientswerecapable ofinternalrotationtotheL2level,followedby21.9%toT10 and 6.3%to S1. Afterthe operation,the largest proportion (56.3%) maintained their capacity asrotation to L2.It was observedthattheproportionwithrotationtoT10increased to34.4%ofthepatientsevaluated,whilethesame6.3%were capableofrotationtoS1and3.1%presentedrotationtothe greatertrochanter.Themeanpreoperativeexternalrotation was 37.9◦, withdeviationof16.6◦. Aftertheoperation, this meanincreasedto50.6◦,withdeviationof13.3◦ (p
Fig.4–Arthroscopicimageshowingthetenotomy performedonthelongheadofthebicepsbrachii.1, Humerus;2,radiofrequencyusedfortenotomyonthelong headofthebicepsbrachii.
Fig.5–Arthroscopicimageshowingtransfixationofthe tendonofthesubscapularismuscle.1,Humerus;2, tweezersusedfortransfixingthetendonofthe subscapularismuscle.
Fig.6–Arthroscopicimageshowingthealternatingsimple stitchesaftercutting,intenodesisonthelongheadofthe bicepsbrachiiinthesubscapularis.1,Tendonofthe subscapularismuscle;2,longheadofthebicepsbrachii.
Regardingelevation,thepreoperativemeanwas110.3◦,with deviationof38.8◦.Aftertheoperation,themeanincreasedto 138.2◦,withdeviationof25.4◦(p≤0.0001).
Among the operations, 29 (90.6%) were performed at Socimed(healthinsurancepatients),usingOrthocord®thread. Three(9.4%)were performedatHospitalNossaSenhorada Conceic¸ão(HNSC;SUSpatients),usingEthibond® thread.In
2
29
1 2
30
0 0
5 10 15 20 25 30
Negative Did not do test because of pain Positive
Test results
Number of patients
Belly Press
Before operation After operation
Fig.7–Evaluationofthebellypresstestinpatients undergoingarthroscopyofthelongheadofthebiceps brachiiinthetendonofthesubscapularismuscle,before andaftertheoperation.
4
27
1 0
31
1 0
5 10 15 20 25 30 35
Pain Negative
Positive
Number of patients
Test results
Bear Hug
Before operation After operation
Fig.8–Evaluationofthebearhugtestinpatients undergoingarthroscopyofthelongheadofthebiceps brachiiinthetendonofthesubscapularismuscle,before andaftertheoperation.
relation to range ofmotion, the results from the different threadsdidnotpresentanysignificantdifference.
Anteriorpainaftertheoperationwasreportedbyone inter-viewee(3.1%).
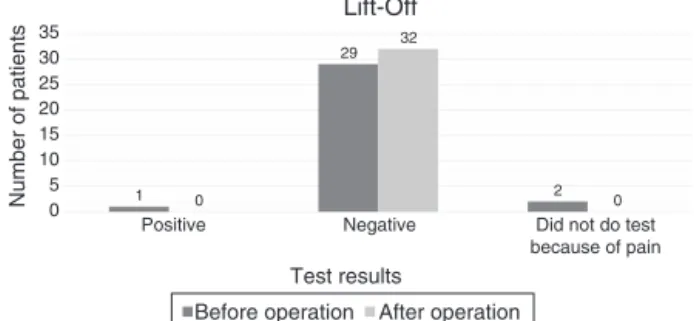
Theresultsfromtheteststoevaluatethefunctioningof thesubscapularistendonbeforeandaftertheoperationare presentedinFigs.7–9.Popeye’ssignwasnotseeninanyofthe patients,eitherbeforeoraftertheoperation,eitherthrough directobservationbytheexaminerorthroughthe interview-ees’responsestoquestions.
The satisfaction level reached 90.6% (29) among the patientsoperated.Outofthethreedissatisfiedpatients,two saidthattheywouldundergothesurgicalprocedurebecause ofthediminutionofpain.
Discussion
Therearedivergencesintheliteratureregardingthebest sur-gicaltechniquetousefortreatinginjuriestotheLHBB.5,6
1 29 2 0 32 0 0 5 10 15 20 25 30 35
Did not do test because of pain Negative
Positive
Number of patients
Test results
Lift-Off
Before operation After operation
Fig.9–Evaluationofthelift-offtestinpatientsundergoing arthroscopyofthelongheadofthebicepsbrachiiinthe tendonofthesubscapularismuscle,beforeandafterthe operation.
deformity.Hsuetal.4conductedareviewoftheliteratureand showedthatoutof376operationsinwhichtenotomywasused asthetechnique,156patients(41%)presentedPopeye’ssign. However,instudiesinwhichtenodesiswasapplied,the out-comewasfavorable.Sethietal.8reportedthattherewaslower riskofPopeye’ssignappearingwhentenodesiswaschosenas theprocedure. Inastudy inwhich63patients who under-wentarthroscopictenodesisonthetendonoftheLHBBwere evaluated,Godinhoetal.9reportedthatsevenpatients(11.1%) complainedaboutestheticdeformity.Whenexaminedbythe evaluator,41(65%)didnotpresentPopeye’ssign.Inastudy on84patientswhounderwentanotherarthroscopictenodesis technique,Leeetal.10foundthat11patients(12.9%)presented estheticdeformity.Onlytwoofthe11patientshadperceived thisdeformity.Areviewofthe literatureconductedbyHsu etal.4foundthat29patients(25%)outof117whounderwent arthroscopic tenodesispresentedestheticdeformity. Inthe presentstudy,estheticdeformitywasnotobservedeitherby theexaminerorbythepatient.Thisresultwasinconformity withtheliterature,i.e.tenodesispresentslowerriskof gen-eratingestheticdeformitythandoestenotomy,whichshows thegoodperformanceofthistechniqueregardingthismatter. Subscapularisinjurieswere testedbymeans ofthe bear hug,lift-offandbellypresstestsbeforeandaftertheoperation. Wedidnotfindanyscientificstudiesintheliterature corre-latinguseofthesetestswiththesurgicaltechniquedescribed inthepresentstudy,whichthereforemadeit impossibleto makecomparisonswiththeresultsfromotherstudies.
Therewerefourpatientswithpositiveresultsfromthebear hugtestbeforetheoperation(Fig.8).Aftertheoperation,the resultsfromthreeofthesepatientsbecamenegative,while theremainingpatientwasunabletodothetestbecauseof pain.The27patientswhosetestswere negativebeforethe operationcontinuedtopresentnegativeresults.Onepatient wasunabletodothetestbeforethesurgerybutpresenteda negativeresultaftertheoperation.
Thereweretwopatientswithpositiveresultsfromthebelly presstestbeforethe operation(Fig.7).These twopatients’ results became negative after the operation. Twenty-nine patientspresentednegativeresultsfromthistestbeforethe operationand27ofthesecontinuedtopresentnegativeresults aftertheoperation,whiletwopresentedpositivetestresults forsubscapularisinjuries.Onlyonepatientwasunabletodo
thetestbeforetheoperation,becauseofexacerbationofpain, andthispatientpresentedanegativeresultafterthe opera-tion.
Therewasonepatientwithapositiveresultfromthelift-off test(Fig.9)orGerbertestbeforetheoperation,andthisresult becamenegativeaftertheoperation.Therewere29patients withnegativeresultsfromthetestbeforetheoperationand these patientscontinued tohavenegativeresults afterthe operation.Onlytwopatientswereunabletodothetestbefore theoperation,andthesepatientshadnegativeresultsafter theoperation.
Throughthetestsapplied,itwasobservedthatoutofthe 32patients,onlytwo(6.25%)presentednegativetestresults before thesurgery and positiveresultsafterthe operation, whichmightindicatesomeinjurycausedbytheprocedure. Thebellypresstest,whichcheckedforsubscapularisinjury aftertheoperation,presentedspecificityof92%andaccuracy of59%.However,thelift-offtestpresentedthesamespecificity of92%andleftdoubtsregardingtherealexistenceofinjuries causedinthisprocedure.Inaddition,amongthetests evalu-ated,theonlyonethatcansuggestthepresenceofinjuryto theupperportionofthesubscapularis(thelocationwherethe proceduretakesplace)isthebearhugtest.However,according tothesample,thistestdidnotshowanyinjuries.11
Inevaluatingresidualpainaftertheoperation,thereview ofthe literatureconductedbyHsu et al.4 showed thatout of109patientswhounderwenttenotomy,19(17%)reported havinganteriorpain.Inastudyon42patients,ofwhom12 underwenttenotomy,AzevedoandVinga12observedthatpain wasreportedin18.1%ofthecases.However,whenwe eval-uated residual pain aftertenodesis,the resultswere more encouraging.OnlyHsuetal.,4amongtheanalysesfoundinthe literatureforcomparisonwiththeresultsfromthisstudy,did notshowbetterresultsincomparingtenotomyandtenodesis. They presented 18 cases of pain (24%) among 74 individ-ualswhounderwenttenodesis.InthestudybyAzevedoand Vinga,12 pain wasreported by9.1%ofthe22 patientswho underwent tenodesis.Boileau et al.13 subjected42 patients toa techniqueofarthroscopic tenodesis andreported that there wereonlyfour casesofpain (9.52%)afterthe opera-tionandthatthesecasesachievedremissionofthecomplaint afterphysiotherapy.Inaseriesof22patientswhounderwent another technique forarthroscopic tenodesis of the LHBB, Mazzocaetal.14didnotreportanycomplaintsofpainafterthe operation.Godinhoetal.9onlypresentedtwocasesofresidual pain(3.2%)among63patientswhowereevaluatedafter ten-odesis.Thepresentstudyshowedpostoperativeanteriorpain onlyinoneinterviewee(3.1%),observedexcellentresultsfrom thetechniquepresentedandwasinagreementwithmostof thestudies encounteredintheliterature.Thesestatedthat tenodesisproducesasmallerpercentageofresidualpainthan doestenotomy.
Thepositiveresultsregardingthelowrateofresidualpain, complete absence ofPopeye’s sign and lowrisk ofcausing subscapularisinjury afterthe surgerycorroborate the high percentageofpatientsatisfaction,whichreached90.6%(29) oftheindividualsoperated.
Conclusion
Thisstudyindicatedthatthenewsurgicaltechniquedescribed herehadgoodperformance.Thesurgeryuseddidnotgenerate subscapularisinjuriesaftertheoperation.Popeye’ssignwas notshowninanyofthepatients,eitherthroughthe exam-iner’sevaluationsorthroughthepatients’ownobservations. Complaintsofresidualpainwerereportedbyonlyonepatient (3.1%).Thepatientsatisfactionrateof90.6%afterthesurgery provestheresultspresented.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MurthiAM,VosburghCL,NeviaserTJ.Theincidenceof pathologicchangesofthelongheadofthebicepstendon.J ShoulderElbowSurg.2000;9(5):382–5.
2. AhmadSC,DiSipioC,LesterJ,GardnerRT,LevineNW,Bigliani L.Factorsaffectingdroppedbicepsdeformityaftertenotomy ofthelongheadohthebicepstendon.Arthroscopy. 2007;23(5):537–41.
3. SzabóI,BoileauP,WalchG.Theproximalbicepsasapain generatorandresultsoftenotomy.SportsMedArthroscRev. 2008;16(3):180–6.
4. HsuAR,GhodadraNS,ProvencherMT,LewisPB,BachBR. Bicepstenotomyversustenodesis:areviewofclinical
outcomesandbiomechanicalresults.JShoulderElbowSurg. 2011;20(2):326–32.
5.WolfRS,ZhengN,WeichelD.Longheadbicepstenotomy versustenodesis:acadavericbiomechanicalanalysis. Arthroscopy.2005;21(2):182–5.
6.JayamoorthyT,FieldJR,CostiJJ,MartinDK,StanleyRM,Hearn TC.Bicepstenodesis:abiomechanicalstudyoffixation methods.JShoulderElbowSurg.2004;13(2):160–4.
7.AlmeidaA,RovedaG,ScheiflerC.Avaliac¸ãodadeformidade estéticaapósatenotomiadacabec¸alongadobícepsna artroscopiadoombro.RevBrasOrtop.2008;43(7): 271–8.
8.SethiN,WrightR,YamaguchiK.Disordersofthelongheadof thebícepstendon.JShoulderElbowSurg.1999;8(6):
644–54.
9.GodinhoGG,MesquitaFAS,Franc¸aFO,FreitasJMT.Tenodese bicipitalarocambole:técnicaeresultados.RevBrasOrtop. 2011;46(6):691–6.
10.LeeHI,ShonMS,KohKH,LimTK,HeoJ,YooJC.Clinicaland radiologicresultsofarthroscopicbícepstenodesiswith sutureanchorinthesettingofrotadorcufftear.JShoulder ElbowSurg.2014;23(3):e53–60.
11.SchieferM,Ching-SanJúniorYA,SilvaSM,FontenelleC, CarvalhoMGD,FariaFG,etal.Diagnósticoclínicodaruptura dotendãosubescapularcomamanobrasemiológicabear hug.RevBrasOrtop.2012;47(5):588–92.
12.AzevedoC,VingaS.Reinserc¸ãoartroscópicado supraespinhoso.RevPortOrtopTraum.2012;20(1):45–56. 13.BoileauP,KrishnanSG,CosteJS,WalchG.Arthroscopicbíceps
tenodesis:anewtechniqueusingbioabsorbableinterference screwfixation.Arthroscopy.2002;18(9):1002–12.