REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Postoperative
excessive
blood
loss
after
cardiac
surgery
can
be
predicted
with
International
Society
on
Thrombosis
and
Hemostasis
scoring
system
Yoon
Ji
Choi
a,
Seung
Zhoo
Yoon
b,∗,
Beom
Joon
Joo
b,
Jung
Man
Lee
c,
Yun-Seok
Jeon
d,
Young
Jin
Lim
d,
Jong
Hwan
Lee
e,
Hyuk
Ahn
faPusanNationalUniversityYangsanHospital,DepartmentofAnesthesiologyandPainMedicine,Yangsan,Gyeongsangnam-do,
SouthKorea
bKoreaUniversity,CollegeofMedicine,DepartmentofAnesthesiologyandPainMedicine,Seoul,SouthKorea
cSeoulNationalUniversity,BoramaeMedicalCenter,DepartmentofAnesthesiologyandPainMedicine,Seoul,SouthKorea dSeoulNationalUniversity,CollegeofMedicine,DepartmentofAnesthesiologyandPainMedicine,Seoul,SouthKorea
eSeongGyunKwanUniversity,CollegeofMedicine,DepartmentofAnesthesiologyandPainMedicine,Seoul,SouthKorea fSeoulNationalUniversity,CollegeofMedicine,DepartmentofThoracic&CardiovascularSurgery,Seoul,SouthKorea
Received16March2016;accepted30December2016 Availableonline24January2017
KEYWORDS
Cardiacsurgery; Coagulation; Disseminated intravascular coagulopathy; Morbidity; Transfusion
Abstract
Backgroundandobjective: Predictionofpostoperativeexcessivebloodlossisusefulfor man-agementofIntensiveCareUnitaftercardiacsurgery.Theaimofpresentstudywastoexamine the effectiveness of InternationalSociety on Thrombosis and Hemostasis scoring system in patientswithcardiacsurgery.
Method: After obtaining approvalfrom the institutional review board, themedical records ofpatientsundergoingelectivecardiacsurgeryusingCardio-PulmonaryBypassbetweenMarch 2010andFebruary2014wereretrospectivelyreviewed.InternationalSocietyonThrombosisand Hemostasisscorewascalculatedinintensivecareunitandpatients weredividedwithovert disseminatedintravascularcoagulationgroupandnon-overtdisseminatedintravascular coagu-lationgroup.Toevaluatecorrelationwithestimatedbloodloss,studentt-testandcorrelation analyseswereused.
Results:Among384patientswithcardiacsurgery,70patientswithovertdisseminated intravas-cular coagulation group (n=20) or non-overt disseminated intravascular coagulation group (n=50)wereenrolled.Meandisseminatedintravascularcoagulationscoresatintensivecareunit admissionwas5.35±0.59(overtdisseminatedintravascularcoagulationgroup)and2.66±1.29 (non-overtdisseminatedintravascularcoagulationgroup)andovertdisseminatedintravascular coagulationwasinducedin29%(20/70).Overtdisseminatedintravascularcoagulationgrouphad muchmoreEBLfor24h(p=0.006)andmaintainedlongertimeofintubationtime(p=0.005).
∗Correspondingauthor.
E-mail:[email protected](S.Z.Yoon).
http://dx.doi.org/10.1016/j.bjane.2016.12.001
Conclusion: Inspiteoflimitationofretrospectivedesign,managementusingInternational Soci-etyonThrombosisandHemostasisscoreinpatientsaftercardiacsurgeryseemstobehelpful forpredictionofthepost-cardio-pulmonarybypassexcessivebloodlossandprolongedtracheal intubationduration.
©2017SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Cirurgiacardíaca; Coagulac¸ão; Coagulac¸ão intravascular disseminada; Morbidade; Transfusão
Aperdasanguíneaexcessivanopós-operatóriodecirurgiacardíacapodeserprevista comosistemadeclassificac¸ãodaSociedadeInternacionaldeTromboseeHemostasia (ISTH)
Resumo
Justificativaeobjetivo: Aprevisãodeperdasanguíneaexcessivanopós-operatórioéútilpara omanejoemUnidadedeTerapiaIntensiva(UTI)apóscirurgiacardíaca.Oobjetivodopresente estudofoiexaminaraeficáciadosistemadeclassificac¸ãodaSociedadeInternacionalde Trom-boseeHemostasia(InternationalSocietyonThrombosisandHemostasis---ISTH)empacientes submetidosàcirurgiacardíaca.
Método: Após obter a aprovac¸ão do Comitê de Pesquisa Institucional, os prontuários de pacientessubmetidosàcirurgiacardíacaeletivausandocirculac¸ãoextracorpórea(CEC)entre marc¸ode2010efevereirode2014foramretrospectivamenterevisados.OescoreISTHfoi calcu-ladonaUTI,eospacientesforamalocadosemdoisgrupos:grupocomcoagulac¸ãointravascular disseminada (CID)manifesta egrupocomCIDnão-manifesta. Paraavaliaracorrelac¸ãocom a PerdaEstimadade Sangue(PES), oteste t de Studente asanálisesde correlac¸ão foram utilizados.
Resultados: Dentreos 384 pacientessubmetidos à cirurgia cardíaca, 70 pacientescomCID manifesta (n=20) ouCIDnão manifesta (n=50) foramincluídos.Asmédiasdos escoresCID na admissãona UTI foram5,35±0,59(Grupo CID manifesta)e 2,66±1,29(Grupo CID não manifesta)einduzidaCIDmanifestaem29%(20/70).OgrupoCIDmanifestaapresentouPES superiordurante24horas(p=0,006)eumtempomaiordeintubac¸ão(p=0,005).
Conclusão:Apesardalimitac¸ãododesenhoretrospectivo,ousodoescoreISTHparaomanejo depacientesapóscirurgiacardíaca pareceserútil parapreveraperdasanguíneaexcessiva pós-CECeoprolongamentodaintubac¸ãotraqueal.
©2017SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Excessive perioperative bleeding continues to complicate cardiacsurgerywithCardio-PulmonaryBypass(CPB)inspite of improvementsin extracorporeal oxygenationand surgi-caltechniques.PatientsaftercardiacsurgerywithCPBhas variouscauses of bleeding.1,2 Defective surgical
hemosta-sisandacquiredtransientplateletdysfunctionmainlycause bleedinginpatient withCPB. Afterstarting CPB, hemodi-lutioncausesplateletcountstodecreasetoapproximately 50%ofpreoperativelevelsrapidlyandevenisthe progres-sive loss of platelet function and prolonged PT and PTT and lowfibrinogen levels arealso attributabletodilution coagulopathy.Druginducedcausesalsoattributedthe peri-operativebleeding3andunknownmechanismscontributeto
decreaseinplateletcountsandplateletdysfunctionduring CPB.4Inaddition,thebalanceofpro-coagulationand
anti-coagulation is profoundly disturbed in Cardio-Pulmonary Bypass (CPB) patients. Both extensive contact between blood and non-endothelial surfaces of the bypass circuit and the release and reinfusion of tissue factor lead to
increasedthrombingenerationduringCPB.5---7Theseresults
cause fibrin formation, fibrinolysis, and platelet activa-tion, despite full heparinization.5,8 Thus, during CPB, it
thoughtthathyper-fibrinolysisis asecondaryphenomenon induced by the activation of coagulation factors. Activa-tionoffactorXIIandthrombinhavebeendemonstratedto inducethereleaseoftissue-typeplasminogenactivatorfrom endothelium.Therefore,itattenuatesthe effectsof both thrombinandplasmintomaintaincoagulationhomeostasis duringCPB, as unrestricted thrombin andplasmin activa-tionultimatelyleadtoconsumptionof coagulationfactors andplatelets(i.e.adisseminatedintravascularcoagulation state duringCPB).7,8 Therefore, variablereasons are
con-tributedin thepatients undergoingunpredictedexcessive bloodloss.
Table1 ScoringsystemforovertdisseminatedintravascularcoagulationproposedbyInternationalSocietyonThrombosisand Hemostasis.
0 1 2
Platelets(×103.mL−1) >100 50---100 <50
d-Dimer(fibrin-relatedmarker)(g.mL−1) <0.5 0.5---5 >5
Prolongedprothrombintime(s) >3 3---6 >6
Fibrinogen(g.L−1) >1.0 ≤1.0
Ifscore≥5,compatiblewithovertDIC
DIC,disseminatedintravascularcoagulation.
In 2001, the International Society on Thrombosis and Hemostasis (ISTH) Sub-Committee of the Scientific and Standardization Committee on Disseminated Intravascular Coagulation proposed that the working definition of dis-seminated intravascular coagulation (DIC) be delineated intotwophase.Non-overtDICrepresentsubtlehemostatic dysfunctionwhile overtDICrecognizeditsdecompensated phase.10ForovertDIC,acumulativescoreof5ormorefrom
prolonged Prothrombin Time (PT), reduced platelets and fibrinogen, and elevated fibrin-related markers proposed (Table1).Evenbleedingaftercardiacsurgeryhasvariable causes,we thoughtthe applyingISTHscoring systemmay beable topredict the postoperativeexcessive blood loss inpatientsaftercardiacsurgerywithCPB.Theaimsofthis presentstudyweretoinvestigatetheeffectivenessofISTH scoringsysteminpatientsaftercardiacsurgerywithCPB.
Method
After obtaining approval from the institutional review board,themedicalrecordsofpatientsagedover20 years undergoing elective cardiac surgery using CPB between March 2010 and February 2014 were retrospectively
reviewed. These demographic and clinical characteris-tics, perioperative laboratory findings, and postoperative complicationswereassessedusingcomputerizeddatabases fromourinstitution.Ofthe384patientsidentified,weonly included those(n=70) whounderwentvalvesurgeryusing CPB in Fig. 1. They did not have an underlying disorder knowntobeassociatedwithovertDIC.Patientsunderwent cardiac surgery except valvesurgery underwent anesthe-siawithmidazolam,rocuronium,andsufentanilorprevious cardiacoperation,anunderlyingdisorderknowntobe asso-ciatedwithovertDIC,ormissingperi-operativerecordswere excluded(n=314).
AnestheticandCPBmanagement
All valvesurgery in this study underwent anesthesiawith midazolam, rocuronium, and sufentanil. Before initiation of CPB, tidal volume was adjusted to achieve normo-ventilationwithoxygeninair(FiO20.5)andwascontrolled bymeansofbloodgasanalysistomaintainnormalarterial carbondioxidetension.
The operation was generally performed with standard non-pulsatile CPB technique (2.4L.min−1.m−2) with
Screening Assessed for screening (n=384)
Excluded (n=314)
♦ Patients underwent other cardiac surgery (n=174) ♦ Missing records (n=81)
♦ Patients underwent previous cardiovascular
related surgery (n=59)
Enrollment Eligibility (n=70)
Allocated to overt DIC group (n=20) Allocated to no overt DIC group (n=50)
Analysed (n=20) Analysed (n=50)
Allocation
Analysis
Figure1 CONSORTflowdiagraminthisretrospectivestudy.OvertDICgroup:DICscore≥5,non-overtDICgroup:DICscore<5.
moderate hypothermia (nasopharyngeal temperature 32---34◦C)withtheadministrationofheparin(300IU.kg−1). SincethereportofManganoetal.,11 ourinstitutehasnot
usedaprotininincardiacsurgery.Therefore,theactivated clotting time was maintained at above 400s. The circuit wasprimed withRinger’s lactated solution, albumin, and mannitol. Cardioprotection was achieved with cold blood cardioplegia. After separation from CPB (rectal tempera-ture36.5---37◦C)anticoagulationactivitywasreversedwith protaminesulfate,givenaratioof1mg:100IUofheparin.
LaboratorytestsandDICscoring
Perioperativelaboratorytestswerecollectedaftersurgery. Platelet counts, PT, fibrinogen, and Fibrinogen Degrada-tionProducts(FDP)were measuredbyelectric impedance methods,scatteredlightdetectionmethod,andlatex quan-titativeimmunoassay,respectively.
BasedontheISTHscoringsystem(Table1),wecalculated theDICscore.TheauthorsconsideredtheovertDICoccurred whenacumulativescoreof5ormorefromthescoring sys-tem.AccordingtotheresultofDICscoreonarrivaltoICU, wedividedthepatientsintotwogroups;OvertDICgroup, DICscore≥5,non-overtDICgroup,DICscore<5.
Bloodtransfusionprotocolandcriteriaforsurgical re-explorationforbleeding
Blood product transfusion guidelines were used to stan-dardizetransfusionpractice.InthepostoperativeICU, the threshold for packed Red Blood Cell (pRBC) transfusion wasaHct/Hb lessthan 0.25/8.0.The indicationfor post-operative transfusion of random donor platelets or fresh frozen plasma was the presence of excessive bleeding (>200mL.h−1),andalaboratory demonstratedcoagulation defect[plateletcount<100×109L,PToractivatedpartial thromboplastintime(aPTT)>1.5×controlvalue,or fibrino-genlevel<1.0g.L−1].
Postoperatively, blood loss from the mediastinal chest tubeswasreportedat6h,12h,and24hfromthetimethe patientarrived in the ICU. The 24h blood loss was docu-mented.The definitionofEBLinICU wasgreaterthan 1L blood loss for 24h.12 Surgical re-exploration was
consid-ered when bleedingduring the first 2h was greater than 300mL.h−1orwasgreaterthan200mL.h−1for4h consecu-tively,withnormalcoagulationvariables.
Patientmanagementprotocol
The tracheal extubation criteria were full conscious-ness, hemodynamic stability, adequate muscle strength andadequaterespiration(requiredpositiveend-expiratory pressure, ≤ to 5cmH2O; breathing rate, <30.min−1) as well as adequate gas exchange value (PaO2, ≥ to 80mmHg/FiO2=0.4;PaCO2,35---50mmHg).
Astheparametersofpostoperativemorbidity,intubation time, oxygen index (OI), length of stay in the Intensive CareUnit(ICU),andserumcreatininelevelfor2dayswere retrospectively assessed. Arterial blood gas analysis was
performedandtheOIwascalculated(arterialPO2/inspired fractionofoxygen)onarrivalofICU.
In accordance with the Acute Kidney Injury Network (AKIN)criteria,13thedevelopmentofpostoperativeAKIwas
evaluatedbasedonchangesinserumCreatinine(Cr) concen-tration within48h of surgery. Serum creatinine level was examinedpreoperatively,within2nddayofICU.
Statisticalanalysis
Values areexpressed as mean±SD or median (25th---75th percentile). To compare the categorical data, chi-square test was used. Continuous variables were expressed as mean±SEM comparedby means ofa parametric (Student t-test) or were expressed as median (25th and 75th per-centiles)comparedbymeansofanonparametric(Wilcoxon signed-ranksum) test, on the basis of the distribution of variables.Toevaluatecorrelationwithestimatedbloodloss (EBL),studentt-testandcorrelationanalyseswasused.To identifyfactors significantly predictive of EBL, univariate andmultivariatelinearregressionanalyseswasperformed. Ap<0.05wasconsideredsignificant.
Results
Duringthe4yearsperiod,384patientswerecollectedinthis study(Fig.1).Amongthepatients,70patientswithovertDIC group(n=20)ornon-overtDICgroup(n=50)wereenrolled. OvertDICincidenceonarrivaltoICUwas29%(20/70)inour studypopulation.
Table 2 summarizes clinical characteristics of the 70 patients studied. There were no statistical differences between the groups in preoperative NYHA classification, age,sex,pre-existingco-morbidityandtypeofsurgery.The CPB time did not differ between groups and transfusion exceptRBC alsodid notdiffer between groups (Table 3). However,patientswithOvertDICgrouphadhigherd-Dimer score(p<0.001) and lactate level (p=0.02) after surgery (Table4).
AlthoughtransfusionbetweengroupsinICUhasno statis-ticaldifferences,totalamountoftransfusedRBCwashigher inOvertDICgroup.And,intubationtimeofovertDICgroup wasalsolongerthannon-overtDICgroup.However,length ofstayintheICU,oxygenationindex(arterialPO2/inspired fractionof oxygen), AcutePhysiology and ChronicHealth Evaluation II (APACHE II) score, and incidence of post-operativeAKIwerenostatisticaldifferencesbetweengroups (Table5).
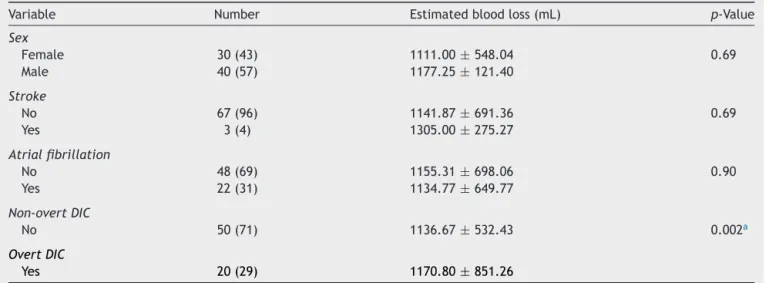
Inaddition,thesewerefoundedthatEBLwashigherin OvertDICgroupandcorrelatedwithoccurrenceofDIC,DIC scoreandCPBtime(Tables6and7).Inaddition,in univari-ateandmultivariateanalyses,DICscoreandCPBtimewas identifiedassignificantlypredictivefactorsofEBL(Table8).
Discussion
Table2 Preoperativepatients’characteristics.
OvertDICgroup(n=20) Non-overtDICgroup(n=50) p-Value
Age(years) 61.90±9.40 55.56±13.36 0.06
Gender(M/F) 12/8 28/22 0.97
Anti-thrombin(%) 129.45±44.30 124.34±42.79 0.67
NYHAclassification 2(2---3) 2(2---3) 0.70
Co-morbidity
Diabetesmellitus(%) 3(15) 5(10) 0.68
Hypertension(%) 6(30) 17(34) 0.97
Previousstroke(%) 2(10) 1(2) 0.19
Atrialfibrillation(%) 7(35) 15(30) 0.9
Renalfailure(%) 1(5) 0 1.00
COPD(%) 1(5) 0 1.00
Typeofsurgery 0.67
Singlevalve(%) 17(85) 38(76)
Doublevalve(%) 3(15) 12(24)
Triplevalve(%) 2(4)
Valuesareexpressedasaverage±SD,number(%),ormedian(25th---75thpercentile).OvertDICgroup:DICscore≥5;non-overtDIC group:DICscore<5.
DIC,disseminatedintravascularcoagulation;NYHA,NewYorkHeartAssociation;COPD,chronicobstructivepulmonarydisease.
Table3 Intraoperativepatients’characteristics.
OvertDICgroup(n=20) Non-overtDICgroup(n=50) p-Value
CPBtime(min) 193.25±60.35 187.46±56.75 0.71
Transfusionintheoperatingroom
PackedRBC(unit) 4(3---5) 2(1---3) 0.01a
FFP(unit) 1(0---3) 0(0---2) 0.80
PLT(unit) 3.5(0---10) 0(0---10) 0.91
Valuesareexpressedasaverage±SDormedian(25th---75thpercentile).OvertDICgroup:DICscore≥5,non-overtDICgroup:DICscore<5. DIC,disseminatedintravascularcoagulation;CPB,cardiopulmonarybypass;RBC,redbloodcell;FFP,freshfrozenplasma;PLT,platelet.
ap<0.05.
Table4 Postoperativepatients’characteristicsinICU.
OvertDICgroup (n=20) Non-overtDICgroup(n=50) p-Value
d-Dimer(g.mL−1) 2.79(2.01---3.37) 1.35(0.87---2.28) <0.001a
Lactate(mmoL.L−1) 3.25(2.80---3.90) 2.70(2.20---3.50) 0.02a
Fibrinogen(mg.dL−1) 308.19±77.25 324.76±90.14 0.51
PT(INR) 1.97±0.37 1.52±0.23 <0.001a
Platelet(×103.mL−1) 84.00(66.25---95.00) 113.00(92.00---141.00) <0.001a
EBL(mL) 1502.05(850.00---1825.00) 895.00(580.00---1290.00) 0.006a
TransfusionintheICU
PackedRBC(unit) 1(0---2) 0(0---2) 0.50
FFP(unit) 3(1.5---6) 3(0---6) 0.58
PLT(unit) 1(0---3.5) 0(0---6) 0.97
Totaltransfusion
PackedRBC(unit) 5(4---7) 3(2---5) 0.01a
FFP(unit) 5(2---7) 4(0---8) 0.53
PLT(unit) 7(0---10) 10(0---10) 0.97
Valuesareexpressedasaverage±SDormedian(25th---75thpercentile).OvertDICgroup,DICscore≥5;non-overtDICgroup,DICscore<5. DIC,disseminatedintravascularcoagulation;PT,prothrombintime;INR,internationalnormalizedratio;EBL,estimatedbloodloss;RBC, redbloodcell;FFP,freshfrozenplasma;PLT,platelet.
Table5 Postoperativepatients’outcomes.
OvertDICgroup (n=20) Non-overtDICgroup(n=50) p-Value
ICUstay(day) 2.50(2.00---5.00) 3.00(2.00---5.00) 0.90
Intubationtime(min) 2740.00(1796.50---4635.00) 1646.50(1310.00---2390.00) 0.005a
OxygenIndex 395.92±138.46 307.05±176.70 0.78 APACHEII 23.76±6.59 21.67±7.90 0.23 Acutekidneyinjury 5(25) 16(32) 0.56
Infection 2(10) 6(12) 0.81
CNSmanifestation 4(20) 6(12) 0.39
Valuesareaverage±SD,number(%),ormedian(25th---75thpercentile).OvertDICgroup:DICscore=5;non-overtDICgroup:DICscore<5. DIC,disseminatedintravascularcoagulation;ICU,IntensiveCareUnit;oxygenindex:arterialPO2/inspiredfractionofoxygen,APACHE
II,AcutePhysiologyandChronicHealthEvaluationII;CNS,centralnervoussystem.
a p<0.05.
Table6 Correlationwithestimatedbloodlossusingstudentt-test.
Variable Number Estimatedbloodloss(mL) p-Value
Sex
Female 30(43) 1111.00±548.04 0.69
Male 40(57) 1177.25±121.40
Stroke
No 67(96) 1141.87±691.36 0.69
Yes 3(4) 1305.00±275.27
Atrialfibrillation
No 48(69) 1155.31±698.06 0.90
Yes 22(31) 1134.77±649.77
Non-overtDIC
No 50(71) 1136.67±532.43 0.002a
OvertDIC
Yes 20(29) 1170.80±851.26
Valuesareexpressedasaverage±SDornumber(%).OvertDIC,DICscore≥5;non-overtDIC,DICscore<5. DIC,disseminatedintravascularcoagulation.
a p<0.05.
Table7 CorrelationwithEBLusingcorrelationanalysis.
EBL(mL) DICscore CPBtime(min) Age(year) Anti-thrombin(%) Lactate(mmoL.L−1)
EBL(mL) 1
DICscore 0.29a 1
CPBtime(min) 0.34a 0.12 1
Age(year) 0.20 0.24 0.03 1
Anti-thrombin(%) −0.17 −0.59a 0.04 −0.15 1
Lactate(mmoL.L−1) 0.13 0.03 0.14 0.11 −0.13 1
EBL,estimatedbloodloss;DIC,disseminatedintravascularcoagulation;CPB,cardiopulmonarybypass.
a p<0.05.
The working definition of DIC proposed by ISTH has been validated since2001. In the absenceof a reference gold standard for the ISTH overt DIC score, compari-son with the Japanese Ministry of Health and Welfare (JMHW)scorewereimportantasthebest-evidenced work-ingdiagnosistodate.14Theinitialreportedagreementrate
between ISTH and JMHW score was 67.4%.15 Discordance
was due to the JMHW sensitivity to DIC in hematologic
malignancieswithhighfibrinolyticactivity.Afurtherstudy, excludesuchcases,demonstrated93%concordance.16Using
a different approach with blinded expert assessment, Bakhtiari et al. found sensitivity of 91% and specificity of 97% withthe ISTH DIC score.17 Therefore, the authors
Table8 Univariateandmultivariatelinearregressionanalyses.
Variable Regressioncoefficient Upperlimitofthe95%CI Lowerlimitofthe95%CI p-Value
Univariate
DICscore 119.62 25.30 213.94 0.01a
CPBtime(min) 3.96 1.27 6.66 0.005a
Age(year) 10.64 −2.11 23.39 0.1
Anti-thrombin(%) −7.23 −17.38 2.92 0.16
d-Dimer(g.mL−1) 161.72 21.62 301.83 0.02a
pRBC(unit) 59.60 25.47 73.73 0.07
Lactate(mmoL.L−1) 68.97 −65.26 203.20 0.31
Multivariate
DICscore 105.27 14.53 196.00 0.02a
CPBtime(min) 3.61 0.98 6.24 0.008a
CI,confidenceinterval;DIC,disseminatedintravascularcoagulation;CPB,cardiopulmonarybypass;pRBC,intraoperativepackedred bloodcell.
ap<0.05.
Postoperative bleeding is one of the most common complications of cardiac surgery. Approximately 20% of patients bleed significantly after cardiac surgery, and 5% requirere-exploration.18,19 Asurgical cause of bleedingis
foundin50%ofpatientsundergoingreoperationfor bleed-ing.Intheremainderofpatients,thecauseismultifactorial andisprobablyrelatedtotheuniquecircumstancesofthe surgicalprocedure.20 Extensivesurgicaltrauma,prolonged
bloodcontactwiththeartificialsurfaceofCPB,highdosesof heparin,andhypothermiacontributetodysfunctionofthe coagulationandinflammatorysystemsthatleadtoa post-operativecoagulopathy.Thelinkbetweentheactivationof thecoagulationandinflammatorysystemsduringthecourse ofCPBiscomplexandisrelatedtothegenerationof acute-phasereactions similartothoseseen insepsis.Therefore, itis often difficult todemonstrate the specific contribut-ingfactorsofthecoagulopathyinanygivenpatientinthe operating room or in the Intensive Care Unit (ICU) since thecoagulopathyisrelatedtocoagulationandinflammatory systems.Inaddition,it is difficult todemonstratea clear associationbetweenfibrinolysisandEBLafterCPB.However, insomestudies,markersoffibrinolysishavebeenfoundto berelatedtopostoperativeEBL.Thesefindingshavebeen supported by theefficiency of theanti-fibrinolytic agents (e.g., aprotinin,tranexamic acid) during CPB in reducing bloodloss.21,22Ourresultsalsoshowedthattheoccurrence
ofDICinICUtriggeredbyCPBwasrelatedtopostoperative EBL.
Inconclusion,inthisstudy,tousetheISTHscoresystem for evaluatingthe occurrenceof DIC in patients undergo-ingcardiacvalvesurgerywasusefulandcouldbepredicted post-CPB excessive blood loss and prolonged mechanical ventilation. While this study had a limitation due to ret-rospective design, these data may help direct further studies and management of patients undergoing cardiac valvesurgery.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisworkwassupportedbyagrantfromtheKoreaHealth TechnologyR&DProjectthroughtheKoreaHealthIndustry DevelopmentInstitute,fundedbytheMinistryofHealth& Welfare,RepublicofKorea(grantnumber:HI13C2181).The authorsthanktheMedicalResearchCollaboratingCenterat Seoul National University Bundang Hospital for statistical analyses.
References
1.Jimenez Rivera JJ, Iribarren JL, Raya JM, et al. Factors associatedwithexcessivebleedingincardiopulmonarybypass patients: a nested case---control study. J Cardiothorac Surg. 2007;2:17.
2.BiancariF,Tauriainen T,Perrotti A, et al. Bleeding, transfu-sionandtheriskofstrokeaftercoronarysurgery:aprospective cohortstudyof2357patients.IntJSurg.2016;32:50---7.
3.LagaS,Bollen H,Arnout J,et al.Heparin influenceshuman plateletbehaviorincardiacsurgerywithorwithout cardiopul-monarybypass.ArtifOrgans.2005;29:541---6.
4.VargheseLCS,UnniCM,MukundanLCN,etal.Plateletfunctions incardiopulmonarybypasssurgery.MedJArmedForcesIndia. 2005;61:316---21.
5.Sniecinski RM, Chandler WL. Activation of the hemo-static system during cardiopulmonary bypass. Anesth Analg. 2011;113:1319---33.
6.KosterA,FischerT,PrausM,etal.Hemostaticactivationand inflammatoryresponseduringcardiopulmonarybypass:impact ofheparinmanagement.Anesthesiology.2002;97:837---41.
7.HertfelderHJ,BosM,WeberD,etal.Perioperativemonitoring ofprimaryandsecondaryhemostasisincoronaryarterybypass grafting.SeminThrombHemost.2005;31:426---40.
8.EissesMJ,VelanT,AldeaGS,etal.Strategiestoreduce hemo-staticactivationduringcardiopulmonarybypass.ThrombRes. 2006;117:689---703.
9.LeviM.Diagnosisandtreatmentofdisseminatedintravascular coagulation.IntJLabHematol.2014;36:228---36.
11.ManganoDT,TudorIC,DietzelC.Theriskassociatedwith apro-tininincardiacsurgery.NEnglJMed.2006;354:353---65.
12.WhitlockR,CrowtherMA,NgHJ.Bleedingincardiacsurgery: itspreventionandtreatment---anevidence-basedreview.Crit CareClin.2005;21:589---610.
13.MehtaRL,KellumJA,ShahSV,etal.AcuteKidneyInjury Net-work: report of an initiative to improve outcomes in acute kidneyinjury.CritCare.2007;11:R31.
14.Toh CH, Hoots WK. The scoring system of the Scientific and Standardisation Committee on Disseminated Intravascu-lar Coagulation of the International Society on Thrombosis and Haemostasis: a 5-year overview. J Thromb Haemost. 2007;5:604---6.
15.Wada H, Gabazza EC, Asakura H, et al. Comparison of diagnostic criteria for disseminated intravascular coagula-tion(DIC): diagnosticcriteriaofthe International Societyof Thrombosisand Hemostasis and of the Japanese Ministry of Health and Welfare for overt DIC. Am J Hematol. 2003;74: 17---22.
16.MatsumotoT,WadaH,NishiokaY,etal.Frequencyofabnormal biphasicaPTTclotwaveformsinpatientswithunderlying dis-ordersassociatedwithdisseminatedintravascularcoagulation. ClinApplThrombHemost.2006;12:185---92.
17.BakhtiariK,MeijersJC,deJongeE,etal.Prospectivevalidation of the International Society of Thrombosis and Haemostasis scoringsystemfordisseminatedintravascularcoagulation.Crit CareMed.2004;32:2416---21.
18.KarthikS,GraysonAD,McCarronEE,etal. Reexplorationfor bleeding after coronary artery bypass surgery: risk factors, outcomes, and the effect of time delay. Ann Thorac Surg. 2004;78:527---34,discussion534.
19.Ferraris VA, Ferraris SP, Saha SP, et al. Perioperative blood transfusionandbloodconservationincardiacsurgery:the Soci-ety of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologistsclinicalpracticeguideline.AnnThoracSurg. 2007;83:S27---86.
20.Paparella D,Brister SJ,Buchanan MR.Coagulation disorders of cardiopulmonary bypass: a review. Intensive Care Med. 2004;30:1873---81.
21.KuepperF,DangasG,Mueller-ChorusA,etal.Fibrinolytic activ-ity and bleedingafter cardiacsurgery withcardiopulmonary bypassandlow-doseaprotinintherapy.BloodCoagul Fibrinoly-sis.2003;14:147---53.