w w w . r b o . o r g . b r
Original
Article
Evaluation
of
the
quality
of
life
after
vertebroplasty
to
treat
compressive
osteoporotic
fractures
夽
,
夽夽
Renato
Faria
Santos,
Julio
César
Simas
Ribeiro,
Frederico
Barra
de
Moraes
∗,
André
Luiz
Passos
Cardoso,
Wilson
Eloy
Pimenta
Junior,
Murilo
Tavares
Daher
SchoolofMedicine,UniversidadeFederaldeGoiás(UFG),Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12July2013
Accepted29July2013
Availableonline29August2014
Keywords:
Vertebroplasty
Vertebralfractures
Qualityoflife
a
b
s
t
r
a
c
t
Objective:withincreasinglifeexpectancyaroundtheworld,fracturesduetoosteoporosis
havebecomemorecommonandtheexpenditurefortreatingthemhasalsoincreased.The
aimherewastoevaluatetheimprovementinpainandqualityoflifeamongpatientswith
compressiveosteoporoticvertebralfracturesundergoingvertebroplasty.
Methods:eighteenpatientswith27fracturedvertebraeunderwentvertebroplastyandwere
evaluatedusingtheOswestry2.0limitationsquestionnairebeforetheoperationand24h
andsixmonthsaftertheoperation.
Results:therewasa75%improvementinpainandqualityoflife,goingfromamean
preoper-ativeOswestryof40%to10%24haftertheoperationand9%sixmonthsaftertheoperation
(p≤0.05).
Conclusion: vertebroplastyiseffectiveinmanagingcompressiveosteoporoticvertebral
frac-tures,withimprovementinpainandqualityoflifeintheimmediatepostoperativeperiod
andoverthemediumterm.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
Avaliac¸ão
da
qualidade
de
vida
após
vertebroplastia
em
fraturas
osteoporóticas
compressivas
Palavras-chave:
Vertebroplastia
Fraturasdacolunavertebral
Qualidadedevida
r
e
s
u
m
o
Objetivo:comoaumentoda expectativadevidanomundo,asfraturaspor osteoporose
setornarammaisfrequenteseaumentaramtambémosgastosnotratamento.Avaliara
melhorianadorenaqualidadedevidadepacientescomfraturasvertebraisosteoporóticas
compressivassubmetidosavertebroplastia.
夽
Pleasecitethisarticleas:SantosRF,RibeiroJCS,deMoraesFB,CardosoALP,PimentaJuniorWEP,DaherMT.Avaliac¸ãodaqualidade
devidaapósvertebroplastiaemfraturasosteoporóticascompressivas.RevBrasOrtop.2014;49(5):477–81.
夽夽
WorkdevelopedintheDepartmentofOrthopedicsandTraumatology,HospitaldasClínicas,UniversidadeFederaldeGoiás,Goiânia,
GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
http://dx.doi.org/10.1016/j.rboe.2014.08.008
avaliadospeloquestionáriodelimitac¸õesdeOswestry2.0deformapré-operatória,24horas
eseismesesnopós-operatório.
Resultados: melhoriade75%da dorenaqualidadedevida,comOswestrymédio
pré-operatóriode40%,em24horasde10%eapósseismesesdacirurgia,de9%.(p≤0,05).
Conclusão: svertebroplastiaéefetivanomanejodasfraturasvertebraisosteoporóticaspor
compressãoemelhoraadoreaqualidadedevidadospacientesnopós-operatórioimediato
emédioprazo.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Osteoporosis is defined as a disease characterized by low
bonemassanddeteriorationofthebonetissue
microarchitec-ture,whichgivesrisetoincreasedfragilityandconsequently
greater riskof developingfractures.1 Dequeker et al.2
con-ducted radiological studies on Egyptian mummies from
approximately2000BCanddemonstratedoccurrencesof
ver-tebralfracturesrelatedtoosteoporosis.
Inthe UnitedStates,US$20 billion/yearisspenton 1.3
millionfracturesattributedtoosteoporosis,ofwhich500,000
are in the spine.3 The treatment for compressive
osteo-poroticvertebralfracturesisgenerallyclinical,withanalgesia,
early walking, vests and anti-reabsorptive medications for
osteoporosis, withthe aims ofavoiding newfractures and
diminishingpainandmorbidity–mortality.
Attheendofthe1990s,Jensenetal.4andDeramondetal.5
indicatedvertebroplastyfortreatingcompressiveosteoporotic
vertebral fractures that had not improved through clinical
treatment.ThismethodwasoriginallydescribedbyGalibert
etal.6in1987,fortreatingvertebraltumors.
Theobjectiveofourstudywastoevaluatetheimprovement
inpainandqualityoflifeamongpatientswithcompressive
osteoporoticvertebralfractureswhounderwentthetechnique
ofvertebroplastyfollowingfailureofconservativetreatment.
Materials
and
methods
Eighteen patients with 27 vertebrae affected by
compres-siveosteoporoticvertebralfractureswereevaluatedbetween
February2003andSeptember2004.
Thepatientsselectedforvertebroplastypresentedoneor
morecompressiveosteoporoticvertebralfractures,with
sig-nificantpainevenafter60daysofclinicaltreatmentconsisting
ofanalgesics,non-steroidanti-inflammatorydrugs(NSAIDs),
opioids,calcitonin,alendronate,calcium,vitaminDandvests
andbeltsforthespine.
Radiographyandmagneticresonanceimaging(MRI)(with
T1/T2/STIRweightedsignals)wereperformedbeforethe
oper-ationandradiographyandcomputedtomography(CT)were
performedaftertheoperation,onallthepatients.MRIshowed
hypersignalinSTIRimages,withboneedemainthefractured
andpainfulvertebralbody.
All the patients underwent general anesthesia. The
routes used for vertebroplasty were posterolateral and
transpedicular, using Jamshid needles and bone cement
(polymethylmethacrylate),with10%bariumsulfatefor
intra-operativeviewingbymeans offluoroscopy.All thepatients
werefollowedupforatleastsixmonthsaftertheprocedure.
Theexclusioncriteriawerethepresenceofacompromised
medullary canal,infection, coagulationdisorders,collapses
greaterthan90%,fracturesoftheposteriorwallofthevertebra
andoldfracturesthatwerenegativeonMRI.
Toevaluatetheimprovementinpainandqualityoflife,the
questionnaireoftheOswestryDisabilityIndex(ODI)(version
2.0)wasusedduringtheweekprecedingthevertebroplasty
and24handsixmonthsaftertheprocedure.
ThestatisticaltestusedforcomparingtheODIscoreswas
thenonparametricWilcoxontest,andresultsweretakento
besignificantwhenp≤0.05.
Results
Twomenand16womenwereevaluated,withanagerange
from 50 to 79 years (mean of64.5), who underwent
verte-broplastyduetocompressiveosteoporoticvertebralfractures
(Figs.1and2).
A total of 27 vertebrae were affected: 18 lumbar (L1 to
L4)and ninethoracic(T8toT12). Onepatientwas affected
at four levels, one at three levels, four at two levels and
12 at one level. We observed two complications among
the cases operated: one case of collapse of an adjacent
level, threeweeksafterthevertebroplasty;andonecaseof
extravasationofcementfromL3,withleft-sideradicular
com-pression.Decompressionviaaposteriorroutewasperformed,
witharthrodesisfromL2toL4using apedunculatedscrew
(Figs.3and4).
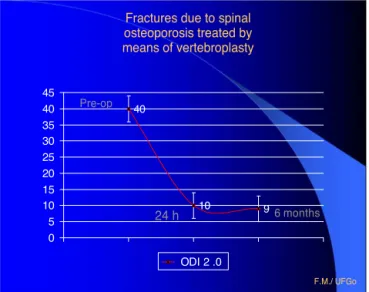
Inrelationtopainandqualityoflife,themeanpreoperative
ODIscorewas40%(±4)andthischangedto10%(±5)withinthe
first24h,thusshowinga75%improvementofpain(p≤0.05).
WhentheODIscorewasmeasuredsixmonthslater,itwas
observedthatthepain-freeconditionhadbeenmaintained
overthemediumterm,withameanvalueof9%(±5)(Fig.5).
Discussion
Osteoporosisisachronicosteometabolic diseasewith
mul-tifactorial causes. It usually has an asymptomatic course,
withprogressivelossofresistanceandbonequality,thereby
leading to greater propensity tofractures. Improvementof
Fig.1–Beforetheoperation:(A)lateralradiographofthespineshowingmildcompressivefracturesofthesuperiorplateau oftheL1andL4lumbarvertebrae;(B)sagittalMRIsliceshowinghypersignalinSTIRsequence,inL1andL4.
qualityoflifehaveprovidedincreasedlongevityand
conse-quentlyithasbeenobservedworldwidethatthepopulation
isaging.Osteoporosishasbeendescribed asthe“epidemic
ofthe21stcentury”7andistodayconsideredtobeapublic
health problem, although great advances in its
preven-tion,diagnosisandtreatmenthavebeenachievedsincethe
1960s.
Patientswithcompressiveosteoporoticvertebralfractures
oftenpresentcomplaintsofbackpain/lumbalgia,whichmay
beacuteorchronic.Suchcomplaintsareseenamong85%of
thepatientswitharadiologicaldiagnosisofthesefractures.8
Thedeformitiesduetothefractures arethe mostfrequent
cause of pain. The degree of kyphosis can be correlated
with the patients’ quality of life (motor, mental and
res-piratory function), the mortality rate and the risk of new
fractures.9,10
This situation leads to sleep disorders, anxiety,
depres-sion, diminished social life and increased dependency on
Fig.3–Complication:(A)lateralradiographofthelumbarspine;(B)axialCTboneslicethroughlumbarvertebra.Both(A) and(B)showextravasationofthevertebroplastycementtothemedullarycanal,withleft-sideradicularcompression.
otherpeople.10Theimprovementinpainissignificantwith
vertebroplasty.11,12Gaitanisetal.13observedanimprovement
inpainonavisualanalogscale,from8.5beforetheoperation
to2.5aftertheoperation,andadecreaseinthelimitationson
dailyactivitiesassessedthroughtheOswestryquestionnaire
from60%to28%.
Ourresultsconfirmthisimmediateimprovementinpain
throughvertebroplastyfortreatingcompressiveosteoporotic
vertebral fractures,with a decrease in the Oswestry index
from40%to10%.Moreover,thisisasafeprocedurewhen
per-formedusingthecorrecttechnique,withlowermorbiditythan
indecompressionsurgeryandarthrodesis.
Fractures due to spinal osteoporosis treated by means of vertebroplasty
40
10 9
0 5 10 15 20 25 30 35 40 45
ODI 2 .0
Pre-op
24 h 6 months
F.M./ UFGo
Fig.5–DecreaseoftheODIscorefrom40%to10%,24h aftervertebroplasty,anditsmaintenanceat9%,sixmonths aftertheprocedure.
Conclusion
Vertebroplasty iseffective inmanagingcompressive
osteo-porotic vertebral fractures. It improves patients’ pain and
quality of lifeimmediately after the operation and this is
maintainedoverthemediumterm.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WorldHealthOrganization.GuidelinesforPreclinal EvaluationandClinicalTriansinOsteoporosis.In:Technical ReportSeries,1998.
2.DequekerJ,OrtnerDJ,StixAI,ChengXG,BrysP,BoonenS.Hip fractureandosteoporosisinaXIIthDynastyfemaleskeleton fromLisht,upperEgypt.JBoneMinerRes.1997;12(6): 881–8.
3.JensenME,EvansAJ,MathisJM,KallmesDF,CloftHJ,DionJE. Percutaneouspolymethylmethacrylatevertebroplastyinthe treatmentofosteoporoticvertebralbodycompression fractures:technicalaspects.AmJNeuroradiol. 1997;18(10):1897–904.
4.OliveiraLG.Osteoporose:guiaparadiagnóstico,prevenc¸ãoe tratamento.RiodeJaneiro:Revinter;2002.
5.DeramondH,DepriesterC,GalibertP,LeGarsD.Percutaneous vertebroplastywithpolymethylmethacrylate.Technique, indications,andresults.RadiolClinNorthAm.
1998;36(3):533–46.
6.GalibertP,DeramondH,RosatP,LeGarsD.Preliminarynote onthetreatmentofvertebralangiomabypercutaneous acrylicvertebroplasty.Neurochirurgie.1987;33(2): 166–8.
7.NIHConsensusDevelopmentPanelonOsteoporosis
Prevention,Diagnosis,andTherapy.Osteoporosisprevention, diagnosis,andtherapy.JAmMedAssoc.2001;285(6): 785–95.
8.LyritisGP,MayasisB,TsakalakosN,LambropoulosA,GaziS, KarachaliosT,etal.Thenaturalhistoryoftheosteoporotic vertebralfracture.ClinRheumatol.1989;8Suppl2: 66–9.
9.KadoDM,BrownerWS,PalermoL,NevittMC,GenantHK, CummingsSR.Vertebralfracturesandmortalityinolder women:aprospectivestudy.StudyofOsteoporoticFractures ResearchGroup.ArchInternMed.1999;159(11):1215–20.
10.LylesKW,GoldDT,ShippKM,PieperCF,MartinezS, MulhausenPL.Associationofosteoporoticvertebral compressionfractureswithimpairedfunctionalstatus.AmJ Med.1993;94(6):595–601.
11.GangiA,KastlerBA,DietemannJL.Percutaneous vertebroplastyguidedbyacombinationofCTand fluoroscopy.AmJNeuroradiol.1994;15(1):83–6.
12.OliveiraFM,RodriguesAG,BastosJOCJr,YamazatoC, KusabaraR.Resultadosclínicosdavertebroplastiaem pacientescomfraturadacolunavertebralporosteoporose. Coluna.2007;6(1):28–33.