w w w . r b o . o r g . b r
Original
Article
Densitometric
study
of
the
clavicle:
bone
mineral
density
explains
the
laterality
of
the
fractures
夽
,
夽夽
Marcelo
Teodoro
Ezequiel
Guerra
a,
Maria
Isabel
Pozzi
b,
Gabriela
Busin
c,∗,
Lucas
Crestana
Zanetti
c,
José
Antônio
Lazzarotto
Terra
Lopes
c,
Vinícius
Orso
c aServic¸odeOrtopedia,HospitalUniversitário,UniversidadeLuteranadoBrasil(ULBRA),Canoas,RS,BrazilbGrupodoOmbroeCotovelo,HospitalUniversitário,UniversidadeLuteranadoBrasil(ULBRA),Canoas,RS,Brazil cHospitalUniversitário,UniversidadeLuteranadoBrasil(ULBRA),Canoas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received13June2013 Accepted19July2013 Availableonline16July2014
Keywords: Densitometry Bonefracture Physiopathology Clavicle
a
b
s
t
r
a
c
t
Introduction:Epidemiologicalstudieshaveshownlateralityinclaviclefractures,suchthatthe leftsideismorefrequentlyfractured.Thepresentstudyhadtheaimofevaluatingwhether theclavicleonthedominantsideisdenserandthusexplainingthegreaterincidenceof fracturesonthenon-dominantside.
Materialsandmethods:Thiswasadescriptivestudyon52healthypatients,whowere clas-sifiedaccordingtoage,sexandwhetherthedominantornon-dominantsidewasaffected. Results:Theparticipantscomprised28women(53.8%)and24men(46.2%).Regardingthe dominantside,30wereright-handed(57.7%)and22wereleft-handed(42.3%).Themeanage was25years.Inthisstudy,itcouldbeseenthatthenon-dominantsidehadgreaterbone massthanthedominantside.Itwasalsoobservedthatthebonedensitywasgreaterinthe middleanddistalthirdsonthenon-dominantside,withastatisticallysignificant differ-ence.Inthewomen,thedensitywasalsogreateronthenon-dominantside;thisdifference wasnotsignificantinrelationtothedominantside,butthereweresignificantdifferences betweenthemiddlethirds(p<0.001)andthedistalthirds(p<0.006).
Conclusion:Variationsinbonedensity,towardhigherandlowerbonemass,mayhavebeen responsibleforthefractures.Accordingtothefindingsfromthisstudy,fracturesoccurmore inthemiddlethirdofthenon-dominantclavicle,asaresultofgreaterbonemineralmass, whichgivesrisetolowerflexibilityandfracturesintheregion.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:TeodoroEzequielGuerraM,IsabelPozziM,BusinG,CrestanaZanettiL,AntônioLazzarottoTerraLopesJ,Orso Vetal.Estudodensitométricodaclavícula:adensidademineralósseaexplicaalateralidadedasfraturas.RevBrasOrtop.2014;49(5):468–72. 夽夽
StudydevelopedattheUniversidadeLuteranadoBrasil,Canoas,RS,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](G.Busin).
http://dx.doi.org/10.1016/j.rboe.2014.07.002
Estudo
densitométrico
da
clavícula:
a
densidade
mineral
óssea
explica
a
lateralidade
das
fraturas
Palavras-chave: Densitometria Fraturaóssea Fisiopatologia Clavícula
r
e
s
u
m
o
Introduc¸ão: Estudosepidemiológicosmostramumalateralidadenasfraturasdaclavícula, comoladoesquerdomaisfrequentementefraturado.Opresenteestudotemcomo finali-dadeavaliarseaclavículadoladodominanteémaisdensaeexplicar,dessaforma,amaior incidênciadefraturasnoladonãodominante.
Materialemétodos: Estudodescritivode52pacienteshígidos,classificadosquantoaidade, sexoeladodominanteounão.
Resultados: Fizerampartedesteestudo28mulheres(53,8%)e24homens(46,2%);emrelac¸ão aoladodominante,30eramdestros(57,7%)e22,canhotos(42,3%);aidademédiafoide 25anos.Nesteestudo,foipossívelconstatarqueoladonãodominantetevemaiormassa ósseaquandocomparadoaoladodominante.Tambémobservamosqueadensidadeóssea foimaiornosterc¸osmédiosedistaisnoladonãodominante,comdiferenc¸a estatistica-mentesignificativa.Nasmulheres,adensidadetambémfoimaiornoladonãodominante; essadiferenc¸anãofoisignificativaquandocomparadocomoladodominante,porémfoi significativamentediferenteentreosterc¸osmédio(p<0,001)edistal(p<0,006).
Conclusão:Asvariac¸õesdadensidadeóssea,tantocommaiorcomocommenormassaóssea, podemserresponsáveispelasfraturas.Deacordocomosachadosdesteestudo,asfraturas ocorremmaisnoterc¸omédiodaclavículanãodominante,emdecorrênciadeumamaior massamineralóssea,oqueacarretariaumamenorflexibilidadedaregiãoeasfraturas.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Changesintherapeuticmethodsforclaviclefractures have ledtoepidemiologicalstudiesconductedmorefrequently.1–3 Classically,conservativetreatmentwasusedwithexcellent results.However,somefracturepatternshavebeenshownto beproblematicwithconservativetreatment,independentof themanagementused.Thus,newstudieshaveemerged, out-liningtheepidemiologicalprofileandmanagementofclavicle fractures.4
Clavicularfractures accountforapproximately 5%ofall patientswithfracturesadmittedtoemergencyservices.5Male childrenandadolescentsuptotheageof20yearsarethegroup mostlikelytosuffer thistypeoffracture,andits incidence decreaseswith increasingage.Amongfemalepatients, the incidenceisgreatestduringtheadolescentyearsand dimin-ishesinsubsequentdecades,butthenincreasesagaininold age.6,7
InanepidemiologicalstudyconductedinSweden,on535 fracturesoftheclaviclealone,greaterfrequencywasobserved ontheleftside(60.7%)thanontherightside(49.3%)andthis differencewasstatisticallysignificant.Itisknownthat differ-entbonedensitiesmaycausefractures.8–11 Pycnodysostosis isasyndromecharacterizedbybonefragilityandfracturing duetodiffuselyincreasedbonedensity.Osteoporosis,onthe otherhand,isadisorder characterizedbydiminishedbone massandincreasedriskoffractures.12,13
Thisstudyhastheaimsofevaluatingclavicularbone min-eraldensitybetweenthedominantandnon-dominantsides andevaluatingbonemineralmassinthemiddleandlateral thirdsoftheclavicle,soastoascertainwhetherdifferentbone
mineraldensitiescouldexplaincertainepidemiological char-acteristicsoffracturesoftheclavicles.
Materials
and
methods
Thiswas across-sectionalstudy conductedintheimaging departmentofourhospitalbetweenMayandJune2007and betweenJanuaryandMay2012.Densitometricexaminations wereperformedonbothclaviclesinasampleof52patients, comprising24males(eightleft-handedand16right-handed) and 28 females (14 left-handed and 14 right-handed).The examinationswereperformedusingbonedensitometry appa-ratusandwereanalyzedbymeansoftheDualFemursoftware, adaptedfortheclavicle.
Alluniversitystudentsagedbetween20and30yearswho were in a healthy condition were eligible for inclusion in the study. Professional athletes, individuals with previous clavicularfractures(whether congenitalor not),individuals withosteometabolicdiseases,casesofbrachialplexusinjury, ambidextrousindividualsandcasesofanyorthopedic disor-derthataffectstheshoulderwereexcluded.
anotherwasstoredforsubsequentstudies.Thishadbeenlaid outintheconsentstatement.
Inthisstudy,thenonparametricWilcoxontestwasused, withasignificancelevelof5%.Toviewtheresultsobtained, boxplotgraphswereused.
This study was approved by our institution’s Research EthicsCommittee,underprotocolnumber2006-064H.
Results
Among the 52 patients who underwent the densitometry examination on the clavicle, 24 (46.2%) were male and 28 (53.8%)werefemale.Inrelationtothedominantside,30were right-handed(57.7%)and22wereleft-handed(42.3%)(Table1). Thepatientsanalyzedwerebetween20and30yearsofage (meanageof25years).
Amongthese52universitystudentswhounderwentthe examination,the bone mineral density ofthe claviclewas greater on the non-dominant side, i.e. among the right-handed individuals,the bone mineral density was greater in the left claviclethan in the right clavicle; whilein the left-handedindividuals,thedensitywasgreaterintheright claviclethanintheleftclavicle.Thisdifferencebetweenthe dominantand non-dominantsideswasstatistically signifi-cant(p<0.001),withgreaterdensityonthenon-dominantside (Table2).
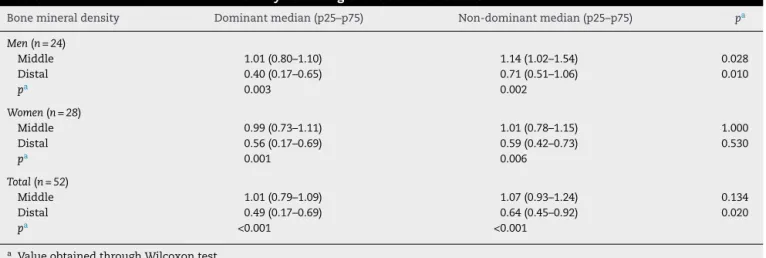
Amongthemen,therewasastatisticallysignificant differ-encebetweenthedominantandnon-dominantsidesbothin themiddlethird(p=0.028)andinthedistalthird(p=0.010)of theclavicle,withgreaterdensityonthenon-dominantside (Table2).Therewasalsoastatisticallysignificantdifference between the middle and distal thirds, both on the domi-nantside(p=0.003)andonthenon-dominantside(p=0.002). Themiddlethird presentedhighervaluesin bothclavicles (Figs.1and2).
Inthewomen,thedominantsidehadgreaterdensity,but therewasnostatisticallysignificantdifferencebetweenthe dominantandnon-dominantsides.Therewasonlya differ-encebetweenthemiddlethirds(p=0.001)andbetweenthe distalthirds(p=0.006). Themiddlethirdspresentedhigher values(Table2andFigs.1and2).
In general,we can affirm that the clavicleon the non-dominant side presented significantly greater values than shownbytheclavicleonthedominantside,inthedistalthird (p=0.020)and that themiddle thirdpresentedsignificantly greatervaluesthanthedistalthirdinbothclavicles(p<0.001).
Table1–Characterizationofthesample.
Characteristics n=52
Sex–n(%)
Male 24(46.2)
Female 28(53.8)
Dominance–n(%)
Right-handed 30(57.7)
Left-handed 22(42.3)
8
7
5
4
3
3 2
1
0
–1
Male
Dominant middle
14 19
21
Non-dominant middle Female
Sex
Bone mineral density (g/cm
2) 6
Fig.1–Evaluationofbonemineraldensityrelatingtothe middlethirdoftheclavicle,accordingtothepatient’ssex.
Discussion
It hasalready been well establishedthat there isa strong relationshipbetweenbonemineraldensityandthedominant side.Bonemassvariesaccordingtouse.Boneisdeposited pro-portionallytothecompressiveloadthatithastobear,andthis iswhyathleteshavegreaterbonemassthanpeoplewhodo notpracticeexercise.Thelattertendtolosebonemass.14–16
Thepresentstudyfoundsignificantdatafromasampleof 52individualswhounderwentexamination.Sincethestudy groupwashomogenous,theresultsfoundwouldnotchange withalargerorsmallersamplethaninthepresentstudy.This wasprovenwhenweaddednewcasestothestudy,giventhat thefirstsamplewasobtainedin2007andthesecond,in2012. Inaprospectivestudyinvolving213patients,densitometry wasperformedontheradiusandulnaofbothforearms.Itwas observedthatthedominantforearmhadgreaterbonemass andalsogreaterbonearea.Onepossibleexplanationforthe greaterbonemassinthedominantlimbwasitsgreateruse. Thedifferencesintheulnawerestatisticallysignificant.17
Table2–Evaluationofbonemineraldensityaccordingtothedominantside.
Bonemineraldensity Dominantmedian(p25–p75) Non-dominantmedian(p25–p75) pa
Men(n=24)
Middle 1.01(0.80–1.10) 1.14(1.02–1.54) 0.028
Distal 0.40(0.17–0.65) 0.71(0.51–1.06) 0.010
pa 0.003 0.002
Women(n=28)
Middle 0.99(0.73–1.11) 1.01(0.78–1.15) 1.000
Distal 0.56(0.17–0.69) 0.59(0.42–0.73) 0.530
pa 0.001 0.006
Total(n=52)
Middle 1.01(0.79–1.09) 1.07(0.93–1.24) 0.134
Distal 0.49(0.17–0.69) 0.64(0.45–0.92) 0.020
pa <0.001 <0.001
a ValueobtainedthroughWilcoxontest.
8
7
5
4
3
2
1
0
–1
Male
14 19
21
Female
Sex
Bone mineral density (g/cm
2) 6
Dominant distal Non-dominant distal
Fig.2–Evaluationofbonemineraldensityrelatingtothe distalthirdoftheclavicle,accordingtothepatient’ssex.
OurfindingsweresimilartothoseofGumustekinetal.,14 i.e.thebonemineraldensityoftheclaviclewasgreateron
thenon-dominantthanonthedominantside.Theclavicleon thedominantsidepresentedlowerbonemineralmassthan shownbytheclavicleonthenon-dominantside.This differ-encewasstatisticallysignificant.
Fracturesoftheclaviclearestatisticallymorefrequenton theleftsideandoccurmostofteninthemiddlethirdoftheleft clavicle(81%),followedbythelateralthird(17%)andmedial third(2%).12
It could be seen that greater bone density on the non-dominantsidecouldleadtogreaterbonefragilitythroughloss offlexibility,18–20sincefracturesoftheclavicleoccurmost fre-quentlyinthemiddlethird,preciselywherethebonedensity isgreatest,bothinthe dominantandinthenon-dominant clavicle.
Conclusion
Theclavicleonthenon-dominantsideisdenserthanthe clav-icleonthedominantside.Likewise,themiddlethirdofthe clavicles, bothon the dominantand onthe non-dominant side, isdenserthan thedistalthird.Thus, theoccurrences ofclavicularfracturesmoreontheleftside,asfoundinthe presentstudy,couldbeduetogreaterbonemineraldensityon thenon-dominantside,whichwoulddiminishboneflexibility and,hypothetically,increasethepropensitytofractures.
Conflicts
of
interest
Annex
1.
Questionnaire:
Densitometric
study
on
the
clavicle:
does
bone
density
explain
the
laterality
of
fractures?
Name: _______________________________________ Reg. no.: _______________
Date of birth: ____________________________ Age: _________________
Sex: ( ) F ( ) M Course: ( ) Medicine ( ) Other:_________________
Handedness: ( ) Right-handed ( ) Left-handed ( ) Ambidextrous
Do you have any chronic disease?
( ) Yes: ____________________________________ ( ) No
Are you a professional athlete?
( ) Yes ( ) No
Have you ever suffered a clavicular fracture? (Including fractures during childbirth)
( ) Yes ( ) No
Have you ever undergone any surgical intervention in the clavicle or shoulder?
( ) Yes ( ) No
Do you have any upper-limb deformity?
( ) Yes ( ) No
Do you have or have you had any injury to the brachial plexus?
( ) Yes ( ) No
Do you have any orthopedic disease of the shoulder?
( ) Yes ( ) No
Do you have any osteometabolic disease?
( ) Yes ( ) No
Do you have any type of restriction on upper-limb movement?
( ) Yes ( ) No
For the researcher to fill out
Was the volunteer selected for the study in accordance with the criteria?
( ) Yes ( ) No
I agree with all the information expressed in this form.
____________________________
Signature of the research subject
r
e
f
e
r
e
n
c
e
s
1. EskolaA,VainionpaaS,MyllynenP,PatialaH,RokkanenP. Outcomeofclavicularfracturein89patients.ArchOrthop TraumaSurg.1986;105(6):337–8.
2.AllmanFLJr.Fracturesandligamentousinjuriesofthe clavicleanditsarticulation.JBoneJointSurgAm. 1967;49(4):774–84.
3.CraigEV.Fracturesoftheclavicle.In:RockwoodCAJr,Green DP,BucholzRW,editors.Fracturesinadults.Philadelphia:JB LippincottCompany;1996.p.928–90.
4.NordqvistA,PeterssonC.Theincidenceoffracturesofthe clavicle.ClinOrthopRelatRes.1994;(300):127–32.
5.DelTortoU,BonaccorsiS.Considerazionisullaterapiadelle fratturedellaclavicola.OrizzOrtopOdieRiabil.1963;8:135–54.
6.RobinsonCM.Fracturesoftheclavicleintheadult. Epidemiologyandclassification.JBoneJointSurgBr. 1998;80(3):476–84.
7.NowakJ,MallminH,LarssonS.Theaetiologyand epidemiologyofclavicularfractures.Aprospectivestudy duringatwo-yearperiodinUppsala,Sweden.Injury. 2000;31(5):353–8.
8.MazessRB,NordR,HansonJA,BardenHS.Bilateral measurementoffemoralbonemineraldensity.JClin Densitom.2000;3(2):133–40.
9.PetleyGW,TaylorPA,MurrillsAJ,DennisonE,PearsonG, CooperC.Aninvestigationofthediagnosticvalueofbilateral femoralneckbonemineraldensitymeasurements.
OsteoporosInt.2000;11(8):675–9.
10.SeemanE,MeltonLJ3rd,O’FallonWM,RiggsBL.Riskfactors forspinalosteoporosisinmen.AmJMed.1983;75(6):977–83.
11.YangRS,ChiengPU,TsaiKS,LiuTK.Symmetryofbone mineraldensityinthehipsisnotaffectedbyage.NuclMed Commun.1996;17(8):711–6.
12.PostacchiniF,GuminaS,DeSantisP,AlboF.Epidemiologyof claviclefractures.JShoulderElbowSurg.2002;11(5):452–6.
13.FernandesCH,MatheusRC,FaloppaF,AlbertoniWM. Alterac¸õesesqueléticasdamãonapicnodisostose.RevBras Ortop.1996;31(5):441–2.
14.GumustekinK,AkarS,DaneS,YildirimM,SevenB,VarogluE. Handednessandbilateralfemoralbonedensitiesinmenand women.IntJNeurosci.2004;114(12):1533–47.
15.DaneS,AkarS,HacibeyogluI,VarogluE.Differencesbetween right-andleft-femoralbonemineraldensitiesinright-and left-handedmenandwomen.IntJNeurosci.
2001;111(3–4):187–92.
16.GuytonAC,HallJE.Tratadodefisiologiamédica.Riode Janeiro:GuanabaraKoogan;1997.
17.WaltersJ,KooWW,BushA,HammamiM.Effectsofhand dominanceonbonemassmeasurementinsedentary individuals.JClinDensitom.1998;1(4):359–67.
18.BrownerB,JupiterJ,LevineA,TraftonP.Skeletaltrauma. Philadelphia:Saunders;2003.
19.CanaleST.Campbell’soperativeorthopaedics.St.Louis: Mosby;2007.