w w w . r b o . o r g . b r
Original
Article
Use
of
adrenalin
with
lidocaine
in
hand
surgery
夽
,
夽夽
Ronaldo
Antonio
de
Freitas
Novais
Junior
∗,
Jorge
Ribamar
Bacelar
Costa,
Jose
Mauricio
de
Morais
Carmo
PedroErnestoUniversityHospital(HUPE),UniversidadedoEstadodoRiodeJaneiro(UERJ),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12July2013 Accepted2September2013 Availableonline18September2014
Keywords:
Localanesthesia Adrenalin Surgery Hand Fingers
a
b
s
t
r
a
c
t
Objective:Becauseofthereceivedwisdomwithinoursettingthatclaimsthatlocal anesthe-siashouldnotbeusedwithadrenalininhandsurgery;weconductedastudyusinglidocaine withadrenalin,todemonstrateitssafety,utilityandefficacy.
Methods:We conducteda prospectivestudyinwhich,inwrist,handandfingersurgery performedfromJuly2012onwards,weusedlocalanesthesiacomprisinga1%lidocaine solutionwithadrenalinat1:100,000.Weevaluatedthequantityofbleeding,systemic alter-ations,signsofarterialdeficitandcomplications,amongotherparameters.Wedescribed theinfiltrationtechniquesforspecificproceduresindividually.
Results:Weoperatedon41patientsandchosetodescribeseparatelytheraisingofalateral microsurgicalflaponthearm,whichwasdonewithoutexcessivebleedingandwithinthe usuallengthoftime.Inonlythreecaseswasthereexcessivebleedingoruseofbipolar twee-zers.Nosystemicalterationswereobservedbytheanesthesiologistsoranycomplications relatingtoischemiaandnecrosisinthewoundsorinthefingers,anduseoftourniquets wasnotnecessaryinanycase.
Conclusions:Useoflidocainewithadrenalininhandsurgerywasshowntobeasafelocal anesthetictechnique,withoutcomplicationsrelatingtonecrosis.Itprovidedefficient exsan-guinationofthe surgicalfieldandmadeitpossibleto performthesurgicalprocedures withoutusingapneumatictourniquet,therebyavoidingitsrisksandbenefitingthepatient throughlowersedation.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Uso
da
adrenalina
com
lidocaína
em
cirurgia
da
mão
Palavras-chave:
Anestesialocal Adrenalina
r
e
s
u
m
o
Objetivo:Porcausadodogmaexistenteemnossomeiodequenãodeveserusadaanestesia localcomadrenalinanacirurgiadamão,fizemosumestudocomousodelidocaínacom adrenalinaparademonstrarsuaseguranc¸a,utilidadeeeficácia.
夽
Pleasecitethisarticleas:deFreitasNovaisJuniorRA,BacelarCostaJR,deMoraisCarmoJM.Usodaadrenalinacomlidocaínaem cirurgiadamão.RevBrasOrtop.2014;49(5):452–60.
夽夽
WorkdevelopedatthePedroErnestoUniversityHospitalandthePiquetCarneiroPolyclinic,UniversidadedoEstadodoRiodeJaneiro, RiodeJaneiro,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected],[email protected](R.A.deFreitasNovaisJunior).
http://dx.doi.org/10.1016/j.rboe.2014.09.006
Cirurgia Mão Dedos
Métodos: Fizemosumtrabalhoprospectivonoqual,apartirdejulhode2012,usamoscomo anestesialocalumasoluc¸ãodelidocaína1%comadrenalina1:100.000nascirurgiasem punho,mãoededoseavaliamosaquantidadedesangramento,asalterac¸õessistêmicas, ossinaisdedéficitarterialeascomplicac¸ões,entreoutrosparâmetros.Descrevemosas técnicasdeinfiltrac¸ãodeprocedimentosespecíficosindividualmente.
Resultados: Operamos41pacienteseoptamospordescreverseparadamenteum levanta-mentoderetalhomicrocirúrgicolateraldobrac¸o,queocorreusemsangramentoexcessivoe notempohabitual.Emapenastrêscasoshouvesangramentoeusodepinc¸abipolar exces-sivos.Nãohouvealterac¸õessistêmicasverificadaspelosanestesiologistasoucomplicac¸ões relacionadasàisquemiaenecrosenasferidasounosdedoseemnenhumcasofoinecessário ousodotorniquete.
Conclusões: Ousode lidocaínacomadrenalina nacirurgiada mãomostrou-setécnica anestésicalocalsegura,semcomplicac¸õesrelacionadasànecrose,forneceucampo cirúr-gico exsangue eficiente, permitiu os procedimentos cirúrgicos sem uso do torniquete pneumático,evitouseusriscosebeneficiouospacientescommenorsedac¸ão.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
“Adrenalineshouldneverbeinjectedintothefinger,because of the gangrene that frequently results.” This affirmation, whichappearsinBunnel’stextbookSurgeryofthehand(1956), servestodemonstratetheextenttowhichadrenalinein asso-ciation witha local anesthetic has been rejected forhand surgery.1Despitestudiesshowingthatthetruecauseof
digi-talgangreneisnotadrenaline,suchastheworkbyThomson,2
themythrevolvingaroundthecausal relationshipbetween adrenalineandnecrosispersistsuntiltoday.
Itis importantto break downthis dogma, because the methodmostused formaintaining theoperative field free from blood (pneumatic tourniquets)may cause difficulties, giventhatpatientscanonlytoleratethisforshortperiods,of lessthan30minonaverage.3Thus,greatersedationisneeded
andthepneumatictourniquethastobedeflated,withawait beforeinflatingitagainsoastoavoidcomplicationssuchas ischemiaandmuscledysfunction,alongwithotherpossible complications.4
Useofadrenalineprovidestheadvantagesofafasterstart andlonger duration ofanesthesia,alonger-lastingsurgical fieldwithoutblood,withoutinterruptions,andalower con-centration of anesthesia for achieving pain control.5 This
makesitpossibletoperformthesurgerywithalowerdosage ofsedativesandalsofacilitatescertainsurgicalprocedures, suchastenolysisandtenorrhaphy,thusdemonstratingthe intraoperativeefficacyofadrenaline.6
Withtheaimofdemonstratingthevariousadvantagesof usinglidocainewithadrenalineinhandsurgery,giventhelack ofevidenceofoccurrencesofdigitalnecrosisintheliterature, andalsobecause oftheimpressivestrength ofthisdogma inoursetting andthescarcity ofthissubjectinthe Brazil-ianliterature,wedecidedtoconductthis studyinorder to demonstratethesafetyandefficacyofthismethodinhand surgery.
Wechoseto alwayshave ananesthetist present during oursurgicalprocedures,whichwereallperformedina sur-gicalcenter.Thus,ourstudydifferedfromthoseconductedin
othercountries,withoutananesthetistandwithprocedures doneinanoutpatientenvironment,whichwejudgednotto beapplicabletoourcountry,becauseofthelegislationandthe behaviorofourpatientsinthelightofthesituationoftension thattheproceduresinvolve.
Methods
StartingonJuly6,2012,patientsatourinstitutionandin pri-vatehospitalsunderwentthemethod.
Patientsundergoingsurgeryasaresultofcomplications (forexample,recurrenceofcarpaltunnelsyndromeor syno-vialcysts),orwhopresentedpoorperipheralperfusionbefore thesurgery,historiesofvasculardiseasesorcontraindications toanesthetics,wereexcluded.
The solution used was 1% lidocaine with adrenaline at 1:100,000. Thestandard was the solutions described by Lalonde,6whousedthemincasesinwhichlessthan50mL
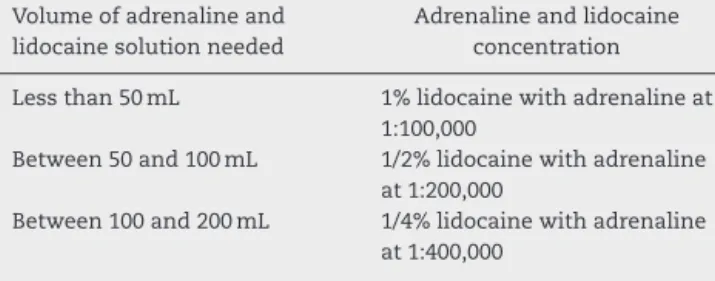
wasnecessary.Weusedflasksof20mLof1%lidocaineand added0.2mLofadrenalinetoobtainthesolution.Ifagreater volumeisnecessary,Lalonderecommendsthatthe concentra-tionsshouldbemorediluted(Table1),withaviewtomaintain asafetylimitforlidocainewithadrenalineoflessthan7mg/kg ofweight.
Table1–Dosageandconcentrationoflidocainewith adrenalinetobeinjectedintotheforearm,handand fingers.
Volumeofadrenalineand lidocainesolutionneeded
Adrenalineandlidocaine concentration
Lessthan50mL 1%lidocainewithadrenalineat 1:100,000
Between50and100mL 1/2%lidocainewithadrenaline at1:200,000
Between100and200mL 1/4%lidocainewithadrenaline at1:400,000
Initially,weinfiltratedthe desiredareaafterputtingthe fieldsintoplace,althoughinafewcaseswedidthe infiltra-tionbeforeplacingthefields,inordertomaketheprocess moredynamic.Weobservedthattheidealtimeforstarting tomaketheincisionwasatleast15minlater,whentheskin hadalreadyundergoneachangeincolorationintheareaof theincision,becominglighterintone(morewhitish),thereby leavingthefieldexsanguinatedandanesthetizedinorderto performtheplannedsurgicalprocedure.Atthetimeof infil-tration,allthepatientswereundersedationandwerebeing monitoredbythe anesthetist.Wehad thesubstance phen-tolamineavailable,incaseit was necessarytoreverse any situationofsevereischemiathatmightdevelop.Thedoseto beusedwouldbe1mgin1mLof0.9%physiologicalserum.
Wedevelopedastandardizedevaluationformtocoverall thecasesandbroachavarietyofparameters,asdescribedin
Annex1.
Theformbeganwiththedateandtypeofsurgeryandthe patient’sidentification.Followingthis,preoperativedatawere evaluated.
Bleedingduringtheoperationwasaddressedinaccordance withascalecreatedbyourgroup,gradedthus:3–excessive bleeding(haltingprogressintheoperationunlessatourniquet wasused);2–moderate(makingitdifficultbutnotimpossible
to continue without using a tourniquet); and 1 – minimal (bleedingsimilartothatofsurgerywithatourniquet).
Use ofbipolar tweezers: yes or no; if positive, this was gradedas1–minimal,2–normalor3–excessive.
Useofatourniquetwasassessedintermsofsituationsin whichthetourniquethadtobeinflatedduringthesurgery.
Intraoperativepainwasassessedaccordingtothepatient, theanesthetist(intermsofalterationsofvitalsigns,for exam-ple)andthesurgeon(intermsofthepatient’sreactions),and gradedasintense,moderate,minimalorabsent.
Systemicalterationswereevaluatedbytheanesthetistby describingalterationstovitalsigns,neurologicalsignsorany clinicalintercurrences.
Theotherparameters,whichwereself-explanatory,canbe seeninAnnex1.
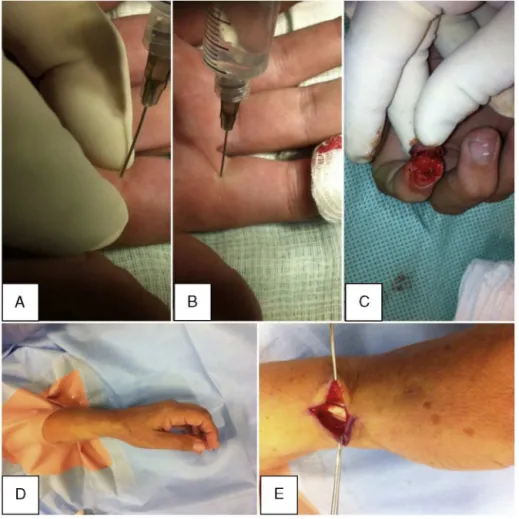
Regardingtheinfiltrationtechniqueincasesofcarpal tun-nelsyndrome,wefirstinfiltratedabout10mL,ataround4cm proximaltothewristflexioncrease,inparallelwiththeulnar borderofthelong palmartendon,whenpresent,underthe fascia oftheforearm, inordertobathe the spacebetween themedianandulnarnerves(Fig.1A).Aroundanother10mL ofthesolutionwasinjectedintotheincisionsite,advancing slowly withoutlettingthe needlegobeyond3–4mmofthe whitetumescentsubcutaneoustissue(Fig.1BandC).
Incasesoftriggerfinger,around4mLofthesolutionwas injectedintothefatunderthecenteroftheincision.TheA1 pulleywasreleasedandthepatientwasabletoviewactive fingermovementsthatweremadeintraoperatively(Fig.1D).
Intheoperationsonfingers,anesthesiawasappliedatthe base,onthemidlineandinthedigitalpalmarcrease,which couldbecomplementeddistally(Fig.2A–C).
In casesof Quervain’s tendinopathy, 10mLof the solu-tionwasinjectedproximallyandalsointothetendonsheath (Fig.2DandE).
In cases of Dupuytren’s contracture, a greater volume (10mL)was injectedinto the mostproximallocalityofthe incisionthatwastobemade,andthen theremainderwas injectedintotheincisionsiteinthehandandfingers.
Intheothercases,thelocalityoftheincisionwasinfiltrated proximallytodistally.AccordingtoLalonde,6ifthelocalityof
theincisiondoesnotundergoinfiltration,itwillbleedmore thantheareainfiltratedwithadrenaline.
Results
Weoperatedon41patients(18menand23women).Ofthese, 18underwentsurgicaltreatmentforcarpaltunnelsyndrome. In two of these cases, this was done in association with
surgicaltreatmentfortriggerfinger.Sixpatientsunderwent surgicaltreatmentfortriggerfinger(sevenfingers).Theother casescanbeseeninTable2.
There was onecase that we have described separately, in which we performed an additional application of the technique. Thisconsisted ofraisinga lateral microsurgical fasciocutaneousflapfromthearm,withaccompanyingskin ofdimensions9cm×6cm,whichwastransferredtocoveran
areaoftumorresectiononthecontralateralhemiface, with-out usingapneumaticcuff.Thepatientwasundergeneral anestheticanditwaspossibletoraisetheflapanddissectthe 6cmlengthoftheposteriorcollateralradialvascularpedicle withoutadditionaldifficultyand withintheusuallengthof timeforobtainingaflap.Wehavenotplacedthedataonthis patientwiththedataontheotherpatientsbecausethiswould distortthedata,giventhattheothersurgicalprocedureswere ofmuchsmallerproportions.
Thepatients’mean agewas 52years(range: 15–81);the meanwaitingtimebetweentheinfiltrationandtheincision was15min(range: 2–30);themean durationofthesurgery was 40min(range: 10–150); and the mean volumeof solu-tioninfiltratedwas14.6mL(range:4–20)fortheconventional proceduresand80mLintothelateralflapofthearm. Bipo-lar tweezerswere not usedin12 patients, minimally used in 16, normally used in 10 and excessively used in three.
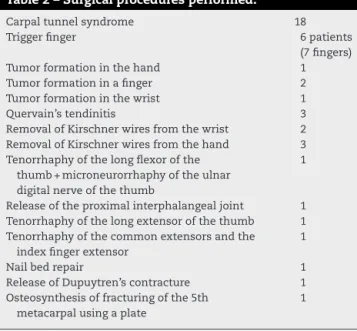
Table2–Surgicalproceduresperformed.
Carpaltunnelsyndrome 18
Triggerfinger 6patients
(7fingers)
Tumorformationinthehand 1
Tumorformationinafinger 2
Tumorformationinthewrist 1
Quervain’stendinitis 3
RemovalofKirschnerwiresfromthewrist 2 RemovalofKirschnerwiresfromthehand 3 Tenorrhaphyofthelongflexorofthe
thumb+microneurorrhaphyoftheulnar digitalnerveofthethumb
1
Releaseoftheproximalinterphalangealjoint 1 Tenorrhaphyofthelongextensorofthethumb 1 Tenorrhaphyofthecommonextensorsandthe
indexfingerextensor
1
Nailbedrepair 1
ReleaseofDupuytren’scontracture 1 Osteosynthesisoffracturingofthe5th
metacarpalusingaplate
1
Thebleedingwasminimalin32cases,moderateinsixand excessiveinthree.Twoofthesecasesofexcessive bleeding comprisedpatients withchronic kidney failure, in surgical treatmentsforcarpaltunnelsyndromeipsilateraltothe fis-tula.
Innoneofthecaseswastheprocedureinterrupteddueto bleeding.
Inallofthecases,theskincolorhadalteredatthetimeof injectingthesolution.
Innoneofthecaseswerethereanysignsofarterialdeficit, intraoperative pain or significant systemic alterations. Nor was it necessaryto introduceischemia using apneumatic tourniquet.
Intwocases,therewasaneedforinfiltrationduringthe surgicalprocedure,atadeeplevelorinacutaneousareathat hadnotbeenenvisagedintheinitialinfiltration.
As a complication, there was one case of injury to a digital nerve during fasciectomy,in surgical treatment for Dupuytren’s contracture. This was treated by means of microneurorrhaphyduringthesamesurgicalprocedure.
Therewerenocasesofnecrosis,hematomaoranyother postoperativecomplication.
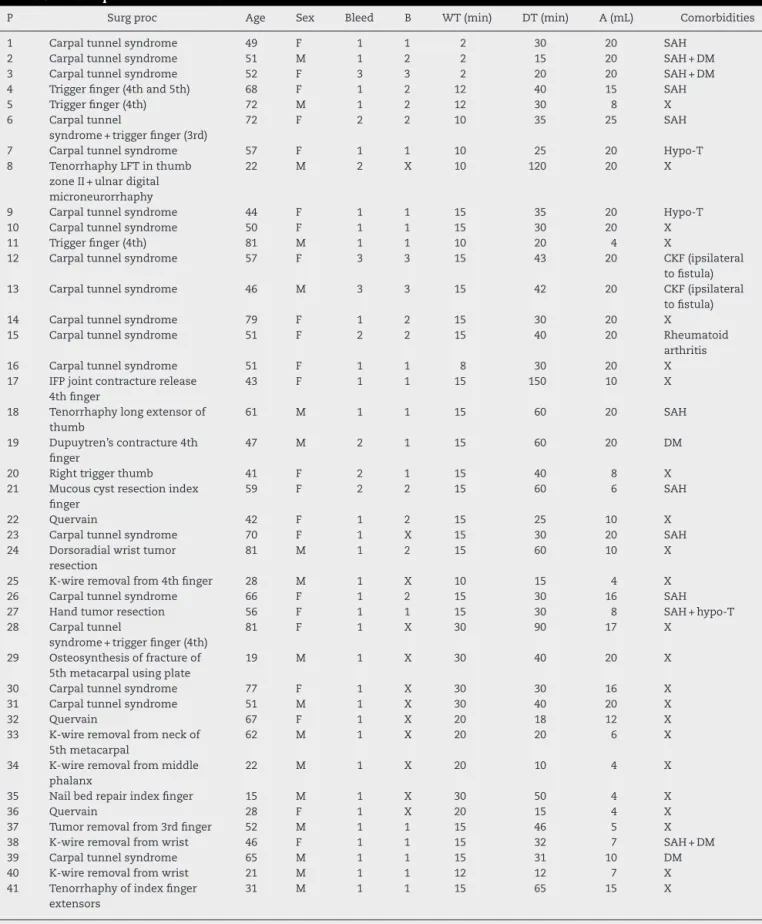
ThedataaredescribedindividuallyinTable3.
Discussion
Prohibition of use of local anesthetics together with adrenalinefordigitalblocksisasurgicaltradition.7Most
text-booksrefertothetheorythatthevasoconstrictioninducedby adrenalineleadstoischemiaandnecrosis.8InthebookGreen’s
OperativeHand Surgery – 5th edition,9 in relation to use of
adrenalinefordigitalblocks,theauthorswrite:“toavoid com-promisingthebloodsupplytothefingers,adrenalineshould notbeusedfordigitalblocks”.However,inthe6thedition,10
theauthorsofthechapter“AnesthesiaforHandSurgery”cite theprospectiverandomizedcontrolledtrialbyWilhelmi,on60 patients,inwhichtherewerenocomplicationsinanypatient ineitherofthegroups,prolongedpaincontrolwasachieved andtherewaslowerbleedingandlowerneedfortourniquet
useduringtheprocedureinthegroupwithadrenaline(with lidocaineat1:200,000).
Fitzcharles-Boweetetal.11reportedthat59casesof
acci-dental injection of adrenaline at 1:1000 into fingers in autoinjectorshadbeendescribedintheworldwideliterature and that therehad notbeen asingle caseoffinger necro-sis.Theauthorsalsoinjectedsolutionsof1:1000,1:10,000and 1:100,000intotheirownfingersandtherewereno complica-tions.Onecaseofaccidentalinjectionofadrenalineat1:1000 wasreversedefficientlyusingphentolamine.12
There are descriptions in the literature of 48 cases of digital gangrene associatedwith adrenalineuse withlocal anesthetic, anda study analyzingeach ofthese caseswas conducted.2Amongthe21patientsinwhomadrenalinewas
used,procainewasusedin18,cocaineintwoandanunknown druginone.Inthecaseswithoutadrenaline,procainewasalso usedmostfrequently(13outof27),whileanunknowndrug wasusedineightcases(probablyprocaine,becauseofthedate ofpublication),cocainewasusedinfourcases,screeninone caseandwaterinonecase.
Denkler7 alsoanalyzedallthese casesandshowed that
muchoftheinformationwasincomplete,regardingtheuse andconcentrationsofadrenaline,useofhotimmersionbaths (which causedburns in14 cases),tourniquets, tight dress-ings,infections(11cases)orpreexistingmedicalconditions. Inonlyfourofthe21casesthatinvolvedadrenalinewasthe concentrationofthesolutiondescribed.
Lalondeetal.13conductedaprospectivemulticenterstudy
in which nine hand surgeons in six cities prospectively reportedtheirconsecutivecasesofinjectionoflidocaineand adrenalineatconcentrationsof1:100,000orlower,intohands andfingers.Thisresultedin3110patientswithoutanytype of finger tissue loss. In none of these cases was phento-lamine necessary for reversing the vasoconstriction of the fingers.
Thestudy byNodwell andLalonde14 demonstrated that
phentolaminereliablyreversedthevasoconstrictioninthe fin-gerscausedbyadrenaline,inanaveragetimeofonehourand 25min.
Chowdhryet al.8 reportedaretrospective study
consist-ing of1111casesofhandandfingersurgery,amongwhich 611 casesreceived blocks of1% lidocaine with adrenaline (1:100,000),withoutanycomplicationsofnecrosis.
Sönmezetal.15publishedarandomizedcontrolledstudyin
whichbloodgasparametersatthefingertipswerecompared withandwithoutuseofadrenaline,andfoundthattherewas nostatisticallysignificantdifference.
ManneandHammert16reportedthattheyroutinelyused
lidocaine with adrenaline because of its safety, given that it decreasedthe needtousetourniquetsand sedation and reducedthecosts,aswellasmakingitpossibletoevaluatethe rangeofmotionintenorrhaphyandtenolysisprocedures.It alsoincreasedthedurationoftheanalgesiceffectand dimin-ishedtheneedforopioidsaftertheoperation.
Table3–Descriptionoftheresults.
P Surgproc Age Sex Bleed B WT(min) DT(min) A(mL) Comorbidities
1 Carpaltunnelsyndrome 49 F 1 1 2 30 20 SAH
2 Carpaltunnelsyndrome 51 M 1 2 2 15 20 SAH+DM
3 Carpaltunnelsyndrome 52 F 3 3 2 20 20 SAH+DM
4 Triggerfinger(4thand5th) 68 F 1 2 12 40 15 SAH
5 Triggerfinger(4th) 72 M 1 2 12 30 8 X
6 Carpaltunnel
syndrome+triggerfinger(3rd)
72 F 2 2 10 35 25 SAH
7 Carpaltunnelsyndrome 57 F 1 1 10 25 20 Hypo-T
8 TenorrhaphyLFTinthumb zoneII+ulnardigital microneurorrhaphy
22 M 2 X 10 120 20 X
9 Carpaltunnelsyndrome 44 F 1 1 15 35 20 Hypo-T
10 Carpaltunnelsyndrome 50 F 1 1 15 30 20 X
11 Triggerfinger(4th) 81 M 1 1 10 20 4 X
12 Carpaltunnelsyndrome 57 F 3 3 15 43 20 CKF(ipsilateral
tofistula)
13 Carpaltunnelsyndrome 46 M 3 3 15 42 20 CKF(ipsilateral
tofistula)
14 Carpaltunnelsyndrome 79 F 1 2 15 30 20 X
15 Carpaltunnelsyndrome 51 F 2 2 15 40 20 Rheumatoid
arthritis
16 Carpaltunnelsyndrome 51 F 1 1 8 30 20 X
17 IFPjointcontracturerelease 4thfinger
43 F 1 1 15 150 10 X
18 Tenorrhaphylongextensorof thumb
61 M 1 1 15 60 20 SAH
19 Dupuytren’scontracture4th finger
47 M 2 1 15 60 20 DM
20 Righttriggerthumb 41 F 2 1 15 40 8 X
21 Mucouscystresectionindex finger
59 F 2 2 15 60 6 SAH
22 Quervain 42 F 1 2 15 25 10 X
23 Carpaltunnelsyndrome 70 F 1 X 15 30 20 SAH
24 Dorsoradialwristtumor resection
81 M 1 2 15 60 10 X
25 K-wireremovalfrom4thfinger 28 M 1 X 10 15 4 X
26 Carpaltunnelsyndrome 66 F 1 2 15 30 16 SAH
27 Handtumorresection 56 F 1 1 15 30 8 SAH+hypo-T
28 Carpaltunnel
syndrome+triggerfinger(4th)
81 F 1 X 30 90 17 X
29 Osteosynthesisoffractureof 5thmetacarpalusingplate
19 M 1 X 30 40 20 X
30 Carpaltunnelsyndrome 77 F 1 X 30 30 16 X
31 Carpaltunnelsyndrome 51 M 1 X 30 40 20 X
32 Quervain 67 F 1 X 20 18 12 X
33 K-wireremovalfromneckof 5thmetacarpal
62 M 1 X 20 20 6 X
34 K-wireremovalfrommiddle phalanx
22 M 1 X 20 10 4 X
35 Nailbedrepairindexfinger 15 M 1 X 30 50 4 X
36 Quervain 28 F 1 X 20 15 4 X
37 Tumorremovalfrom3rdfinger 52 M 1 1 15 46 5 X
38 K-wireremovalfromwrist 46 F 1 1 15 32 7 SAH+DM
39 Carpaltunnelsyndrome 65 M 1 1 15 31 10 DM
40 K-wireremovalfromwrist 21 M 1 1 12 12 7 X
41 Tenorrhaphyofindexfinger extensors
31 M 1 1 15 65 15 X
Inourstudy,therewerenocasesofpostoperativenecrosis orhematomaamongthe41procedures.Innocasedidwehave tousephentolaminetoreversetheeffectsoftheischemia.
In the first three cases, we waited only two minutes betweentheanesthesiaandtheincision.Althoughexcellent ischemiawasobtainedinthefirsttwoofthesecases, abun-dantbleedingoccurred inthethirdcase,which stoppedat theendoftheprocedure.Followingthiscase,wethen estab-lishedaminimumof10minandsubsequently15min.Asa wayofmaintainingaminimumwaitingtimesoastoallowthe effectoftheadrenalinetobegin,westartedtoapplythe anes-theticbeforeplacingthesurgicalfields.Throughthisaction, westartedtoachieveabetterischemiceffect.Theintervalof 15minwassufficientinthemajorityofthesituations.Inmost cases(28),bipolartweezerswereeithernotusedorminimally used.
One possible complication resulting from this bleed-ing,evenif diminished,hasbeen inadvertentsectioningof the finger nerve when performing fasciectomy incases of Dupuytren’scontracture.AccordingtoLalonde,this surgery isoneofthemostdifficultprocedurestoperformusingthis method,becauseofthecloseproximityofthefinger’svessels.6
Inthetwocasesofpatientswithchronickidneyfailurewho underwent surgical treatment for carpal tunnel syndrome ipsilateraltothefistula,therewasexcessivebleeding,which madetheproceduredifficulttoperform.
Our study had some limitations.There was no control group; we still only have a small number of cases avail-able;andnostatisticalanalysiswasperformedonthedata. Nonetheless,weconductedaninitialprospectivestudyand obtainedgoodresults fromthis series, withgood ischemia and anesthesia, without any complications relating to necrosis.
Anothernoteworthypointwasthatthesolutionwas suc-cessfully used to raise a lateral flap on one patient’s arm intheabsenceofblood,withoutusingapneumaticcuff.In
theoriginaltechnique,asterilecuffisinstalledhighonthe arm,butthiswasnotpossibleherebecausethehospitalhad technicaldifficultyinsterilizingthetourniquet.Thepatient underwent general anesthesia so that a malignant tumor on theopposite hemifacecould beresectedbyahead and necksurgeon.Themicrosurgicalanastomosesofthe poste-riorcollateralpediclewereperformedonbranchesofthefacial vessels,withalumenof2.5mm,using10.0mononylonthread. Thesurgerywasperformedtakingthenormaltimeandusing normalmethods,withoutharmtothevascularpedicleafter injectionofthesolution,whichwasdistributedatdeeplevels aroundthehumerusandinthesubcutaneoustissue,inthe areaofthecutaneousandsubfascialincision.
A bibliographic survey was conducted through the CAPESperiodicalswebsite(www.periodicoscapes.gov.br)and PubMed (www.pubmed.com), and we didnot find any sci-entific studies that made specific use of adrenaline or lidocaine–adrenaline solution for replacing the pneumatic cuffinsurgeryoftheextremitiesthatwouldenablediscussion.
Conclusions
Useoflidocainewithadrenalineinhandsurgery,ata concen-trationof1:100,000orless,wasshowntobeasafetechnique forlocalanesthesia,withoutcomplicationsrelatingto necro-sisor systemicabsorption. Moreover,itprovidedasurgical field that was efficiently exsanguinated,thereby making it possibletoperformthesurgicalprocedureswithoutusinga pneumatic tourniquet,whichavoidedthepotential risksof tourniquetsandprovidedthebenefittopatientsofless seda-tion.
Conflicts
of
interest
Annex
1.
Evaluation
form
used
for
all
patients
Questionnaire for surgery without a cuff and with lidocaine + adrenaline 1:100.000
Date of surgery: _____________
Surgical procedure: _________________
Name: ____________________________________________________
Hospital reg. no.:________________ Polyclinic reg. no.:________________
Age: _____ Sex: ______ Weight: _______ kg
Address: ______________________________________________________________
Telephone: __________________________________
Comorbidities: _____________________________
Perioperative bleeding: excessive ( ) moderate ( ) minimal ( )
• Excessive: halts progression of the surgery unless a tourniquet is used
• Moderate: makes progression difficult without a tourniquet, but not impossible
• Minimal: bleeding similar to that of surgery with a tourniquet
Use of bipolar tweezers: no ( ) yes ( ) ____ (1- minimal; 2 – normal; 3 - excessive)
Use of tourniquet: no ( ) yes ( )
Intraoperative pain: intense ( ) moderate ( ) minimal ( ) none ( )
Systemic alterations (anesthetist): vascular system ( ) neurological alterations ( ) others ______________________
Length of time between anesthesia and incision: _________
Duration of surgery: ________
Any skin color alteration around the injection of anesthetic? (yes) (no)
Any signs of arterial deficit? (yes) (no)
Notes: _____________________________________________
Quantity of anesthetic (mL): ________ Any need for intraoperative repetition? (yes) (no)
Sedation: no ( ) yes ( )
Drugs and dosage: ________________________________________
Presence of postoperative hematoma: D3________D10_______D17_________
Presence of postoperative necrosis: D3________D10________D17___________
Other alterations: ____________________________________________________
r
e
f
e
r
e
n
c
e
s
1. SylaidisP,LoganA.Digitalblockswithadrenaline.Anold dogmarefuted.JHandSurgBr.1998;23(1):17–9.
2. ThomsonCJ,LalondeDH,DenklerKA,FeichtAJ.Acritical lookattheevidenceforandagainstelectiveepinephrineuse inthefinger.PlastReconstrSurg.2007;119(1):260–6.
3. TzarnasCD,DarbyPA.Carpaltunnelreleasewithouta tourniquet.JHandSurgAm.1993;18(6):1041–3.
4. OraguiE,ParsonsA,WhiteT,LongoUG,KhanWS.Tourniquet useinupperlimbsurgery.Hand(NY).2011;6(2):
165–73.
5. KrunicAL,WangLC,SoltaniK,WeitzulS,TaylorRS.Digital anesthesiawithepinephrine:anoldmythrevisited.JAm AcadDermatol.2004;51(5):755–9.
6. LalondeDH.Reconstructionofthehandwithwideawake surgery.ClinPlastSurg.2011;38(4):761–9.
7.DenklerK.Acomprehensivereviewofepinephrineinthe finger:todoornottodo.PlastReconstSurg.
2001;108(1):114–24.
8.ChowdhryS,SeidenstrickerL,CooneyDS,HazaniR,Wilhelmi BJ.Donotuseepinephrineindigitalblocks:mythortruth? PartII.Retrospectivereviewof1,111cases.PlastReconstSurg. 2010;126(6):2031–4.
9.RamamurthyS,AndersonD,Anesthesia,GreenDP.Green’s operativehandsurgery.5aed.Philadelphia:Elsevier;2005.p. 25–52.
10.FisherL,GordonM.Anesthesiaforhandsurgery.In:Wolfe SW,HotchkissRN,PedersonWC,KozinSH,editors.Green’s operativehandsurgery.6aed.Philadelphia:Churchill Livingstone/Elsevier;2010.p.25–38.
12.MarkovchickV,BurkhartKK.Thereversaloftheischemic effectsofepinephrineonafingerwithlocalinjectionsof phentolamine.JEmergMed.1991;9(5):323–4.
13.LalondeDH,BellM,BenoitP,SparkesG,DenklerK,ChangP.A multicenterprospectivestudyof3110consecutivecasesof electiveepinephrineuseinthefingersandhand:the DalhousieProjectclinicalphase.JHandSurgAm. 2005;30(5):1061–7.
14.NodwellT,LalondeD.Howlongdoesittakephentolamineto reverseadrenaline-inducedvasoconstrictioninthefingerand
hand?Aprospective,randomized,blindedstudy:the Dalhousieprojectexperimentalphase.CanJPlastSurg. 2003;11(4):187–90.
15.SönmezA,YamanM,ErsoyB,NumanodluA.Digitalblocks withandwithoutadrenalin:arandomised-controlledstudy ofcapillarybloodparameters.JHandSurgEurVol. 2008;33(4):515–8.