SEVERE OPTOCHIASMATIC ARACHNOIDITIS A F T E R RUPTURE
OF A N INTERNAL CAROTID ARTERY ANEURYSM
RICARDO RAMINA * — WALTER O. ARRUDA ** — ANTÔNIO C. F. PRESTES * MÔNICA K. F. PAROLIM ***
S U M M A R Y — T h e c a s e o f a 2 4 y e a r o l d m a n w i t h p r o g r e s s i v e v i s u a l l o s s d u e t o o p t o c h i -a s m -a t i c -a r -a c h n o i d i t i s i s p r e s e n t e d . T h e c -a u s e o f t h e -a r -a c h n o i d i t i s w -a s s u b -a r -a c h n o i d -a l b l e e d i n g d u e t o r u p t u r e o f a n i n t e r n a l c a r o t i d a r t e r y a n e u r y s m . T h e a n e u r y s m w a s c l i p p e d 5 y e a r s a f t e r t h e f i r s t e p i s o d e o f b l e e d i n g . T h e d i a g n o s i s o f o p t o c h i a s m a t i c a r a c h n o i d i t i s w a s c o n f i r m e d d u r i n g t h e o p e r a t i o n . T h i s case, i s p r e s e n t e d i n o r d e r t o d i s c u s s t h e c a u s e s , the s y m p t o m s a n d t h e t h e r a p e u t i c a l p o s s i b i l i t i e s o f t h i s r a r e c o n d i t i o n .
Aracnoidite optoquiasmática grave após ruptura de aneurisma da artéria carótida interna.
R E S U M O — R e l a t o d o c a s o d e p a c i e n t e m a s c u l i n o c o m 24 a n o s d e i d a d e , c o m p e r d a p r o g r e s s i v a d a v i s ã o d e v i d a a a r a c n o i d i t e o p t o q u i a s m á t i c a . A c a u s a d a a r a c n o i d i t e f o i r u p t u r a d e a n e u r i s m a d a p a r e d e d o r s a l d a a r t é r i a c a r ó t i d a i n t e r n a d i r e i t a , c o m h e m o r r a g i a s u b a r a c n ó i d e a . O a n e u r i s m a f o i c l i p a d o 5 a n o s a p ó s o p r i m e i r o e p i s ó d i o d e s a n g r a m e n t o . O d i a g n ó s t i c o d e a r a c n o i d i t e o p t o q u i a s m á t i c a f o i c o n f i r m a d o d u r a n t e c i r u r g i a . A f i n a l i d a d e d o r e l a t o é r e v e r e d i s c u t i r a s c a u s a s , o q u a d r o c l í n i c o o a s p o s s i b i l i d a d e s t e r a p ê u t i c a s d e s s a c o n d i ç ã o rara.
Optochiasmatic arachnoiditis is an unusual inflammatory disease at the base of
the skull 4,18. The diagnosis is difficult in the majority of the cases and it is based
on the history of the patient and the surgical findings. If a correct diagnosis is not
made soon the patient may become blind.
W e describe the case of a man with progressive bilateral visual loss due to an
optochiasmatic arachnoiditis caused by the rupture of an internal carotid aneurysm.
C A S E R E P O R T
J R M , a 24-year-old man presented severe headaches and epileptic fits 5 years prior
to admission to our clinic. H e remained unconscious during some hours. This w a s his first
epileptic episode and he started to complain of headaches and progressive visual loss since
then. Seven months later he was admitted to another hospital for investigation of the
headaches and the visual disturbances. A t that admission a severe bilateral visual loss
with papiledema was observed. Angiographic studies of both carot d arteries were performed
and disclosed bilateral subdural hematoma over both fronto-parietal hemispheres. The
hema-tomas were evacuated through frontal burr holes. After this operation the headaches
improved, but the visual acuity showed progressive impairment. The patient became blind
U n i d a d e d e C i ê n c i a s N e u r o l ó g i c a s , H o s p i t a l S ã o V i c e n t e : * N e u r o c i r u r g i ã o ; ** N e u r o -l o g i s t a , b o -l s i s t a d o C N P q ; *** N e u r o -l o g i s t a .
Oplochiaxmutic arachnoiditis 19.'!
two months after the operation. On M a y 22, 1986 the patient was admitted to our Department
complaining of headaches. H i s parents reported that he presented since some months ago
behavioural disturbances, with confusion and hypersexuality. At examination we found a
demented patient, blind, with no cranial nerve palsies nor extremities palsies. T h e cptic
nerve discs were pale and atrophic. A C T scan (Fig. 1) showed a hypodense zone in the
right temporal pole as well as in the suprasellar region. Angiographic studies revealed
an aneurysm of the dorsal wall of the right internal carotid artery, after the origin of the
Fig. 1 — Case JRM. CT-scan examination showing hypo-density (h) in the supra-sellar and anterior tempo-ral region.
ophtalmic artery (Fig. 2 ) . This aneurysm was not observed at the first angiography
performed 5 years before. Considering the age of the patient and the natural history of
ruptured intracranial aneurysms, the surgical treatment was indicated. The aneurysm was
exposed through a right fronto-temporal craniotomy. T h e right temporal pole showed a
cystic formation, and a severe arachnoiditis of the whole skull base was noted. A n
aneurysm of the dorsal wall of the I C A distal to the origin of the ophthalmic artery was
found. T h e dome of the aneurysm w a s very adherent to the right optic nerve, which
probably occluded it after its rupture (Fig. 3 ) . T h e aneurysm was succesfully clipped with
an Yasargil clip. T h e optic nerve and the chiasm were very thin discolored, embebed in
a fibrosis with cystic formation. The cause of the bilateral amaurosis of the patient was
1F,4 Arq Ncuro-Psiquiat. (Sao Paulo) Jf7(2j 1989
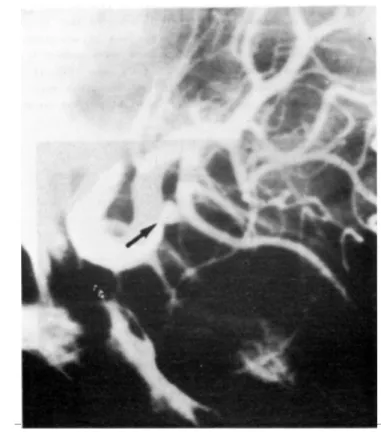
Fig. 2 — Case JRM. Angio-graphic study of the right internal carotid artery showing the aneurysm in the dorsal wall of this artery, be-tween the ophthalmic and the posterior com-municating arteries (ar-row).
adhesions was not carried out because the patient was already blind, and it could produce additional damage to other structures at the skull base. T h e postoperative course was
uneventfull. The patient could be discharged ten days after the operation without new neurological deficits.
C O M M E N T S
Optochiasmatic arachnoiditis caused by subarachnoidal haemorrhage due to rupture of intracranial aneurysms has been very seldom reported in the literature 8. It is an inflammatory process leading to fibrosis and adhesions envolving the structures at the base of the skull. Males under 4 0 years of age are more frequently affected 1?. Pathological features are thickening of the arachnoid with adhesions and cystic for-mation filled with cerebrospinal fluid 2. The chiasm and the optic nerve may be affected with consequent atrophy of the visual fibers. This condition has multiple c a u s e s4
including infections such as tuberculous meningitis 2,10,13,14^ syphilis, acute and chronic meningitidis, cysticercosis I 5 , i 6j infections of the neighbouring structures (para-nasal sinuses, teeth) 3, t r a u m a1
, polyarteritis n o d o s a1 2
, intracranial bleeding 8, foreign body reaction 7, after neurosurgical procedures (e.g. exeresis of pituitary tumors). Bleeding from intrachiasmal arteriovenous malformations usually produces sudden chiasmal visual field loss 8. This haemorrhage could eventually lead to a local arachnoidi-tis. The symptoms are produced by inflammation, direct compression (constriction), or impairment of vascular supply to the optic fibers 3 and other neighbouring structures.
uni-Optochiasmatic arachnoiditis 195
Fig. 3 — Case JRM. Opera-tive picture: the relation-ship of the aneurysm (A) to the optic nerve (ON) can be seen. F, forceps.
lateral or bilateral anosmia, facial paralysis, and auditory and visual disturbances 18. The correct diagnosis is usually difficult and it is based upon the anammesis and the findings at the time of sugery. Computed tomography examination, cerebral angiography, RIHSA (radioactive human serum albubin) cisternography, pneumocisternoencephalography may be helpful, but they often fail to indicate the d i a g n o s i s1 1
. The majority of intracranial saccular aneurysms are located at arterial divisions. Ohara et a l .1 1
described a 1% incidence for those aneurysms unrelated to arterial junctions. Aneurysms arising from the dorsal wal of the internal carotid artery are uncommon 9
>2
° . The proximity of this kind of aneurysm to the optic nerve and chiasm may produce direct compression of these structures or, as in our case, delayed effects from the bleeding. The cause of the arachnoiditis in our case was the subarachnoidal bleeding due to rupture of this aneurysm. This could be clearly demonstrated at the operation. It is surprising that so few cases of optochiasmatic arachnoiditis caused by rupture of intracranial aneurysms have been reported in the English literature 6,8. A reason for this is not presently known. The localization of the aneurysm could be an additional factor in the etiology of this inflammatory process. The operation of anerysms in the acute stage, with removal of clots and blood around the optic structures could eventually avoid this condition.
The treatment of optochiasmatic arachnoiditis remains controversial. Surgical lysis of the adhesions and removal of cysts in the cystic form of the disease is related to improve the symptoms only in minority of cases 8. Dexamethasone has been used in the majority of the cases but a complete relief of the symptoms can not always be obtained. Recently, cyclophosphamide was successfully used after failure of surgical lysis of the adhesions and dexamethasone therapy 6
R E F E R E N C E S
1. B o d e c h t e l G — D i a g n ó s t i c o D i f e r e n c i a l d e las E n f e r m e d a d e s N e u r o l ó g i c a s . P a z M o n t a l v o , M a d r i d , 1967, p g 646.
2. C o y l e J T — C h i a s m a t i c a r a c h n o i d i t i s . A m J O p h t h a l m o l 68:345, 1969.
3 G u p t a S R , B i l l e r J, F r e n k e l M , Y a r z a g a r a y L — F o r s t e r - K e n n e d y s y n d r o m e d u e t o o p t o c h i a s m a t i c a r a c h n o i d i t i s . S u r g N e u r o l 20 : 216, 1983.
4. H a r t m a n n E — O p t o c h i a s m a t i c a r a c h n o i d i t i s . A r c h O p h t h a l m o l 33:68, 1945.
5. I r a c i G, G a l l i y i o n i F , G e n o r a M , S e c c h i A G , F i o r e D , Z a r s p i e r i P, R i g o b e l l o L . T o m a z z o l i L , P a r d a t s c h e s K , M a r i n G, S c a t t o l i n R — O p t o c h i a s m a t i c a r a c h n o i d i t i s : a r e v i e w o f t r a d i t i o n a l n e u r o r a d i o l o g i c a l d i a g n o s i s (82 c a s e s 1951-1976). A c t a N e u r o c h i r ( W i e n ) 48 : 151, 1979.
6. L a v i n P J M , M c C r a r y J A I I I , R o e s s m a n n TJ, E l l e n b e r g e r C J r — C h i a s m a l a p o p l e x y : h e m o r r h a g e f r o m a c r y p t i c v a s c u l a r m a l f o r m a t i o n in t h e o p t i c c h i a s m . N e u r o l o g y 34 : 1007, 1984.
7. M a r c u s A O , D e m a k a s J J , R o s s A , D u i c k D S , C r o w e l l R M — O p t o c h i a s m a t i c a r a c h n o i d i t i s w i t h t r e a t m e n t b y s u r g i c a l l y s i s o f a d h e s i o n s , c o r t i c o s t e r o i d s a n d c y c l o p h o s p h a m i d e . N e u r o s u r g e r y 19 : 101, 1986.
8. M c F a d z e a n R M , G o w a n M E — O p t o c h i a s m a l a r a c h n o i d i t i s a f t e r r u p t u r e o f a n a n t e r i o r c o m m u n i c a t i n g a r t e r y a n e u r y s m . T r a n s O p h t h a l m o l Soc UK 98 : 490, 1978.
9. N a r a g a w a F , S h i g e a k i K , T s h i t i T , S u g i t a K — A n e u r y s m s p r o t u d i n g f r o m t h e d o r s a l w a l l o f t h e i n t e r n a l c a r o t i d a r t e r y . J N e u r o s u r g 65 : 303, 1986.
10 N a v a r r o I M , P e r a l t a V H R , L e o n J A M , V a r e l a E A S , C a b r e r a J M S — T u b e r c u l o u s o p t o c h i a s m a t i c a r a c h n o i d i t i s . N e u r o s u r g e r y 9 : 654, 1981.
11. O h a r a H , S a k a m o t o T , S u z u k i J — S c l e r o t i c c e r e b r a l a n e u r y s m s . I n : S u z u k i J ( e d ) : C e r e b r a l A n e u r y s m s . N e u r o n , T o k y o , 1979, p g 673.
12. O l i v e r M , B e l l e r A J , B e h a r A — C h i a s m a l a r a c h n o i d i t i s as a m a n i f e s t a t i o n o f g e n e r a l i z e d a r a c h n o i d i t i s in s y s t e m i c v a s c u l a r d i s e a s e . B r J O p h t h a l m o l 52 : 227, 1968.
13. S c h l e r n i t z a n e r D , H o d g e s F J I I I , B a g a n M — T u b e r c u l o m a o f t h e left o p t i c n e r v e a n d c h i a s m . A r c h O p h t h a l m o l 85 : 75, 1971.
14. S c o t t R M , S o n n t a g V K H , W i l c o x L M , A d e l m a n L S , R o c k e l T H — V i s u a l l o s s f r o m o p t o c h i a s m a t i c a r a c h n o i d i t i s a f t e r t u b e r c u l o u s m e n i n g i t i s . J N e u r o s u r g 46 : 524, 1977. 15. S o t e l o J, C u e r r e r o V , R u b i o F — N e u r o c y s t i c e r c o s i s : a n e w c l a s s i f i c a t i o n b a s e d o n a c t i v e
a n d i n a c t i v e f o r m s . A r c h I n t e r n M e d 145:442, 1985.
16 T o r r e a l b a G, D e l V i l l a r S, T a g l e . P, A r r i a g a d a P , K a s e C S — C y s t i c e r c o s i s o f t h e c e n t r a l n e r v o u s s y s t e m : c l i n i c a l a n d t h e r a p e u t i c c o n s i d e r a t i o n s . J N e u r o l N e u r o s u r g P s y c h i a t 47 : 784, 1984.
17. V a i l D — O p t o c h i a s m a t i c a r a c h n o i d i t i s . A r c h O p h t h a l m o l 20 : 384, 1938.
IS. W a l s h F B , H o y t W F — C l i n i c a l N e u r o O p h t h a l m o l o g y . W i l l i a m s a n d W i l k i n s , B a l t i -m o r e , 1969.
19. Y a m u k i T , O d a k e G, H o r i k a w a Y — A c a s e o f b i n a s a l q u a d r a n t a n o p s i a d u e t o o p t o c h i a s -m a t i c a r a c h n o i d i t i s . N o S h i n k e i G e k a 6 : 393, 1978.