BrazJOtorhinolaryngol.2017;83(3):299---312
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Airway
reconstruction:
review
of
an
approach
to
the
advanced-stage
laryngotracheal
stenosis
夽
Mohamad
Ahmad
Bitar
a,b,c,d,∗,
Randa
Al
Barazi
a,
Rana
Barakeh
aaAmericanUniversityofBeirut,FacultyofMedicineandMedicalCenter,DepartmentofOtolaryngologyandHead&NeckSurgery,
Beirut,Lebanon
bAmericanUniversityofBeirut,FacultyofMedicineandMedicalCenter,DepartmentofPediatricsandAdolescentMedicine,
Beirut,Lebanon
cUniversityofSydney,SydneyMedicalSchool,TheChildren’sHospitalatWestmead,DepartmentofENTSurgery,Sydney,Australia dAlJalilaChildren’sSpecialtyHospital,DepartmentofOtolaryngologyHead&NeckSurgery,Dubai,UAE
Received9December2015;accepted31March2016 Availableonline27April2016
KEYWORDS Laryngotracheal stenosis;
Subglotticstenosis; Laryngotracheal reconstruction; Cricotracheal resection; Staging; Mapping
Abstract
Introduction:The management oflaryngotracheal stenosis iscomplex andis influenced by
multiplefactorsthatcanaffecttheultimateoutcome.Advancedlesionsrepresentaspecial
challengetothetreatingsurgeontofindthebestremedyingtechnique.
Objective: Toreviewtheefficacyofoursurgicalreconstructiveapproachinmanaging
advanced-stagelaryngotrachealstenosistreatedatatertiarymedicalcenter.
Methods:A retrospective review of all patients that underwent open laryngotracheal
repair/reconstruction by the senior author between 2002 and 2014. Patients with
mild/moderate stenosis(e.g. stage 1 or2), or thosewho hadanopen reconstructive
pro-cedure prior toreferral, were excluded.Patientswho hadonlyendoscopic treatment(e.g.
laser,balloondilatation)andwerenotsubjectedtoanopenreconstructiveprocedureatour
institution,werenotincludedinthisstudy.Variablesstudiedincludedpatientdemographics,
clinicalpresentation,etiologyofthelaryngotrachealpathology,thelocationofstenosis,the
stageofstenosis,thetypeofcorrectiveorreconstructiveprocedureperformedwiththetype
ofgraftused(whereapplicable),thetypeanddurationofstentused,thepost-reconstruction
complications,andthedurationoffollow-up.Outcomemeasuresincludeddecannulationrate,
totalnumberofreconstructivesurgeriesneededtoachievedecannulation,andthenumberof
post-operativeendoscopiesneededtoreachasafepatentairway.
Results:Twentyfivepatientswereincluded,aged0.5months to45years(mean13.5years,
median15years)with16malesand9females.Seventeenpatients(68%)wereyoungerthan18
years.Mostpatients presentedwithstridor,failureofdecannulation,orrespiratorydistress.
Majorityhadacquiredetiologyfortheirstenosiswithonly24%havingacongenitalpathology.
夽
Please citethisarticle as:Bitar MA,AlBaraziR, BarakehR. Airwayreconstruction: reviewofanapproach to theadvanced-stage laryngotrachealstenosis.BrazJOtorhinolaryngol.2017;83:299---312.
∗Correspondingauthor.Currentaddress:PediatricOtolaryngologyProgram,Al-JalilaChildren’sSpecialtyHospital,Dubai,UAE.
E-mail:[email protected](M.A.Bitar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.03.012
300 BitarMAetal.
Thirty-tworeconstructiveprocedureswereperformedresultingindecannulating24 patients
(96%),with15/17(88%)pediatricpatientsand5/8(62.5%)adultpatientsrequiringonlya
sin-glereconstructiveprocedure.Cartilagegraftsweremostlyusedinchildren(84%vs.38%)and
stentsweremostlysiliconemade,followedbyendotrachealtubes.Thenumberofendoscopies
requiredrangedfrom1to7(mean3).Moreco-morbiditiesexistedinyoungchildren,resulting
infailuretodecannulateonepatient.Adultpatientshadmorecomplexpathologiesrequiring
multipleprocedurestoachievedecannulation,withgraftinglessefficaciousthaninyounger
patients.Thepediatricpatientshaddoubletheincidenceofgranulationtissuecomparedto
adults.Thedecannulatedpatientsremainedasymptomaticatameanfollow-upof50.5months.
Conclusion:Thereviewofourapproachtoopenairwayrepair/reconstructionshowedits
effi-cacyinadvanced-stagelaryngotrachealstenosis.Goodknowledgeofavarietyofreconstructive
techniquesisimportanttoachievegoodresultsinavarietyofagegroups.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published
by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Estenose
laringotraqueal; Estenosesubglótica; Reconstruc¸ão laringotraqueal; Ressecc¸ão cricotraqueal; Estadiamento; Mapeamento
Reconstruc¸ãodeviaaérea:revisãodeumaabordagemàestenoselaringotraqueal emestágioavanc¸ado
Resumo
Introduc¸ão:A conduta daestenose laringotraqueal é complexo eé influenciado por vários
fatoresquepodemafetaroresultadofinal.Lesõesemestágioavanc¸adorepresentamumdesafio
especialparaocirurgiãoencontraramelhortécnicadetratamento.
Objetivo:Avaliaraeficáciadenossaabordagemdereconstruc¸ãocirúrgicanotratamentode
estenoselaringotraquealemestágioavanc¸adoemumcentromédicoterciário.
Método: Revisão retrospectiva de todos os pacientes que foram submetidos a tratamento
cirúrgico/reconstruc¸ão laringotraqueal aberta pelo autor principal, entre 2002 e 2014. Os
pacientescomestenoseleve(porexemplo,estágio1ou2),ouaquelessubmetidosa
proced-imento de reconstruc¸ão aberta antes daindicac¸ão, foramexcluídos. Pacientes quetinham
sidosubmetidossomenteatratamentoendoscópico(porexemplo,laser,dilatac¸ãoporbalão)
enãohaviamsidosubmetidosaprocedimentodereconstruc¸ãoabertaem nossainstituic¸ão,
não foramincluídos nesteestudo.As variáveisestudadasincluíram dadosdemográficos dos
pacientes,apresentac¸ãoclínica,etiologiadadoenc¸alaringotraqueal,localdaestenose,estágio
daestenose,otipodeprocedimentocorretivooureconstrutorrealizadocomotipodeenxerto
utilizado(ondeaplicável),tipoedurac¸ãodostentutilizado,complicac¸õespós-reconstruc¸ão,
e durac¸ão do seguimento. Os resultados incluíram taxas de decanulac¸ão, número total de
cirurgiasreconstrutorasnecessáriasparapossibilitaradecanulac¸ão,eonúmerodeendoscopias
pós-operatóriasnecessáriasparaobterumaviaaéreapatenteesegura.
Resultados: Vinteecincopacientesforamincluídos,comidadede0,5mesesa45anos(média
de13,5anos,medianade15anos)com16homense9mulheres.Dezessetepacientes(68%)
erammenoresde18anos.Amaioriadospacientesapresentavaestridor,falhadedecanulac¸ão
ou desconforto respiratório. A maioria das estenoses era adquirida, enquanto apenas 24%
presentavamapresentavamcausacongênita.Trintaedoisprocedimentosreconstrutoresforam
realizados, resultando em decanulac¸ão de 24 pacientes(96%), com15/17 (88%) pacientes
pediátricose5/8pacientes(62,5%)adultosquenecessitaramdeapenasumúnicoprocedimento
reconstrutor.Enxertosdecartilagemforamutilizadosprincipalmenteemcrianc¸as(84%vs.38%)
eamaioriadosstentserafeitaprincipalmentedesilicone,seguidosportuboendotraqueal.
Onúmerodeendoscopiasnecessáriasvarioude1a7(médiade3).Maiscomorbidadesforam
observadas em crianc¸as pequenas, resultando em falha de decanulac¸ão em um paciente.
Pacientesadultosapresentavamdoenc¸asmaiscomplexasquerequereramváriosprocedimentos
paradecanulac¸ão,comenxertosmenoseficazesdoqueempacientesmaisjovens.Ospacientes
pediátricosapresentaramodobrodaincidênciadetecidodegranulac¸ãoemcomparac¸ãoaos
adultos. Ospacientesdecanulados permaneceramassintomáticos em um seguimento médio
de50,5meses.
Conclusão:Arevisãodanossaabordagemparatratamentocirúrgico/reconstruc¸ãoabertadas
viasaéreas demonstrarameficácianaestenoselaringotraquealem estágioavanc¸ado.O
con-hecimentodeumavariedadedetécnicasdereconstruc¸ãoéimportanteparaconseguirbons
resultadosemváriosgruposetários.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado
por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
Airwayreconstructioninadvanced-stagelaryngotrachealstenosis 301
Introduction
A significant increase in the incidence of laryngotracheal stenosis (LTS)occurred aftertheadvent of neonatal intu-bation in the 1960s as described first by McDonald and Stocks.1 However, over the past few decades, the inci-dencehasdecreasedgiventheeffortputintheeducation of thenursing and medicalstaffinvolved in endotracheal tube care and the development of new tube material.2 Laryngotrachealstenosiscanbecongenitaloracquiredand can affect the supraglottis, glottis, subglottis, the tra-chea, or a combination ofthese levelsat thesame time, although the most common location in children is the subglottis.2,3
On the other hand, LTS in the adult population has a differentspectrum ofpathologies. The main causeof air-waystenosisinadultshasbeenreportedbyPenaetal.,to beendotracheal intubation followedby laryngealtrauma, hamartoma andamyloidosis.4 As such,the trachea is the mostcommonsitetobeaffected(2rytotraumafromthe tube’scuff)followedbythelarynx.
The managementofLTScanbechallengingwith multi-plefactorsinvolvedthatcanaffecttheultimateprognosis. Treatmentshouldbepersonalizedasperthepatient’s char-acteristics. The most commonly used approach so far is laryngotrachealairwayreconstruction(LTR).Othermethods include laser ablation, and endoscopicballoon dilatation. The latter is usually used in patients with mild stenosis (stage1 or 2),in early immature lesionsor soon afteran airwayreconstructionproceduretopreventrestenosis. Bal-loondilatationhasrecentlybecomepopularandsometimes overused.WebelieveLTRisstillthetreatmentmodalityof choiceformatureandadvancedLTS.
OurapproachtoLTShasbeentoadapttoeachpatient’s typeofpathologybyrelyingonmappingthelesion preop-erativelytochoosethemostappropriatecorrectivesurgical techniqueforthatparticularpatient.Italsoreliesonusing a staging system specific to each type of pathology to ensureproperdocumentation,transmissionofinformation, andreportingofdata.Inthisstudywe revisitthesurgical treatmentofLTS,byreviewingourexperienceandassessing the efficacy of our approachin managing advanced-stage laryngotracheal stenosis treated at a tertiary medical center.
Methods
We performed a retrospective review of all patients who weremanagedbytheseniorauthor(MAB)forLTSbetween 2002 and 2014. The institutional review board approved thestudy(EthicalcommitteeapprovalnumberOTO.MB.11). Patients with mild stenosis (e.g. stage 1 or 2), or those whohadanopenreconstructiveprocedurepriortoreferral, were excluded. Patients, whohad only endoscopic treat-ment(e.g.laser,balloondilatation)andwerenotsubjected to an open reconstructive procedure at our institution, werenotincluded inthisstudy.Variablesstudiedincluded patientdemographics,clinicalpresentation,etiologyofthe laryngotrachealpathology,thelocationofthestenosis,the stageof thestenosis usingvariousgrading systems appro-priatetothetopographyoflesion,thetypeofcorrectiveor
reconstructiveprocedureperformedwiththetypeofgraft used (where applicable), the type and duration of stent used,thepost-reconstructioncomplications,andthe dura-tionoffollow-up.
Our adopted approach includes mapping the various encounteredairwaypathologiespreoperatively.On presen-tation, all patients had a flexible fiberoptic nasopharyn-golaryngoscopyperformed toevaluatethe patencyof the upperairways andassess the mobility of thevocal cords. Ifthepatienthadalreadyatracheostomyinplace,a flex-ible fiberoptic tracheoscopy was performed through the tracheostomytubetoassessthelowerairways.
Ifnotalreadyavailable fromthe referringphysician,a CTscanof theneck/chest wasthen orderedtostudy the extentofthelesionpriortofurtherevaluationinthe operat-ingtheater.Directlaryngoscopyandbronchoscopywasthen undertakenforafinal anddirectmappingofthelesion.If possibledistalendoscopythroughthestenoticareawas per-formedtomarkthedistalpartofthestenosis.Thelocation ofthe tracheostomytube (ifpresent) withrespecttothe stenotic segmentwas alsoassessed. The final topography of the lesion wasdelineated by combining the results of alltheaboveandrecordedinthechart;includinglocation, thickness,andlength.
To better documentthe findings andproperlytransmit theinformationtootherphysicians,weclassifiedthe stud-iedstenosesusinglesion-appropriatestagingsystems.These included;theCotton---Myerstagingsystem5forisolated Sub-glotticStenosis (SGS),theCohen’sclassification6for Ante-rior Glottic webs/stenosis (AGS), the Bogdasarian---Olson classification7forPosteriorGlotticwebs/stenosis(PGS)and theMcCaffreystagingsystem8forLTS.
TheCotton---Myerstagingsystem5describesthestenosis basedonthepercentrelativereductionin cross-sectional areaofthesubglottisanditconsistsoffourgrades:
GradeI---lessthan50%obstruction; GradeII---51---70%obstruction; GradeIII--- 71---99%obstruction;
GradeIV---nodetectablelumenorcompleteobstruction.
Cohen proposed the classification for anterior glottic web/stenosis6:
TypeI---involvementof35%orlessoftheglottiswithlittle ornosubglotticinvolvement;
TypeII---involvementof35---50%oftheglottiswithminimal subglotticinvolvement;
TypeIII---involvementof50---75%oftheglottisextending tothelowerborderofthecricoids;
TypeIV---athickwebcovering75---90%of theglottisand extendingtothelowerborderofthecricoids.
Ontheotherhand,BogdasarianandOlsonclassifiedthe extentofposteriorglotticweb/stenosisintofourtypes7:
TypeI---vocalprocessadhesion;
302 BitarMAetal.
Type III --- posterior commissure stenosis with unilateral cricoarytenoidjointankylosis;
Type IV --- posterior commissure stenosis with bilateral cricoarytenoidjointankylosis.
TheMcCaffrey stagingsystem8 wasdevelopedandused forLTSintheadultpatient.Thoughitwasnotvalidatedto measuretheoutcomeinthepediatricagegroup,weopted touseitjustfordocumentationbecauseoflackofasimilar systeminchildren.TheMcCaffreystagingsystemisdivided intofourstagesdescribingthesiteofstenosis:
StageI---lesionsconfinedtothesubglottisortracheathat arelessthan1cmlong;
Stage II --- subglottic lesionslonger than 1cm withinthe cricoidringandnotextendingtotheglottisortrachea; StageIII---subglotticlesionsextendingintotheupper tra-cheabutnotinvolvingtheglottis;
StageIV---lesionsinvolvingtheglottiswithfixationor paral-ysisofoneorbothvocalcords.
Theclassificationofanisolatedtrachealpathologywas hardasthereisnospecificallyadoptedstagingsystem for thatlocation.We have adopted the classificationusedby Anandetal.9tostratifythemanagedtrachealpathologies. The lesionis classified depending onitslocation(cervical vs. thoracic), length (1---3cm vs. > 3cm) and severity of obstruction(mild,moderateorsevere).
The outcomewasmeasured bythedecannulationrate, the total number of reconstructive procedures required to achieve decannulation, and the number of post-reconstructiveendoscopiesneededtoreachasafepatent airway.
Thetypeofsurgeryperformedoneachpatientwas tail-oredaccordingtothepreoperativemappingofthelesion, andthestabilityofthelaryngotrachealframework.
Supraglottic stenosis’ correction (what we like to call ‘‘supraglottic reconstruction’’) was the most challenging procedurewhichalwaysinvolvesstentingandrequiresclose follow-up.
Laryngotrachealreconstructionwasusedtoexpandthe glottic,subglotticorlaryngotrachealstenoticsegment.The framework should be stable enough to accommodate an insertedgraft.Theexpansionmaybeanterior,posterioror bothdependingonthetopographyofthestenosisata partic-ularsite.Thetrachealsegmentofacombinedstenosis(i.e. laryngotracheal)canbeshortenedbyexcisingitifneededto limitthenumberofusedgraftsorifitiscircumferentialas thegraftwillonlyexpandtheanteriorpartofthetracheal segment.
Cricotrachealresection(CTR)wasusedinadvancedstage LTS, in cases where the framework was unstable due to replacementofthecartilagewithfibrosis,inadultswhere theossificationof theribcartilageandthe airway frame-workwaspresent,andinrevisionLTR’swheregraftswere previouslytried.
Trachealresectionandanastomosiswasusedtoremove anisolatedsegmentof thetracheawhere circumferential stenosisexists.
The reconstructive procedure was sometimes a single stage where the patient did not need a tracheostomy present postoperatively. This was feasible in cases where
thestenoticlesionwasexcisedorexpandedandthe resul-tantreconstructionwasstableenoughtorequireshortorno stentinginthepostoperativeperiod.Atothertimes,a dou-blestagewasneeded,wheredecannulationwasperformed afterensuringthatthereconstructedareahealedproperly andtheairwaywassafe.
As the studied population included both pediatric and adult patients, we further analyzed the results as two separate series tocompare patients’ characteristics, pre-operative findings,thetypeof surgeriesneeded andtheir outcome.
Results
Wereviewed25patientsaged0.5monthsto45years(mean 13.5years,median15years)with16malesand9females. Seventeen patients (68%) were younger than 18 years. The clinical presentation was variableamong the studied patients; 36% presented with stridor, 28% were referred forfailureofdecannulation,20%presentedwithhistoryof respiratorydistress,8%wereseenforfailureofintubation, and8%complainedofinabilitytoswim.Mostpatientshadan acquiredcausewithonly24%havingacongenitalpathology (Table1).
Afterpreoperativemapping,wecouldclassifythelesions as:
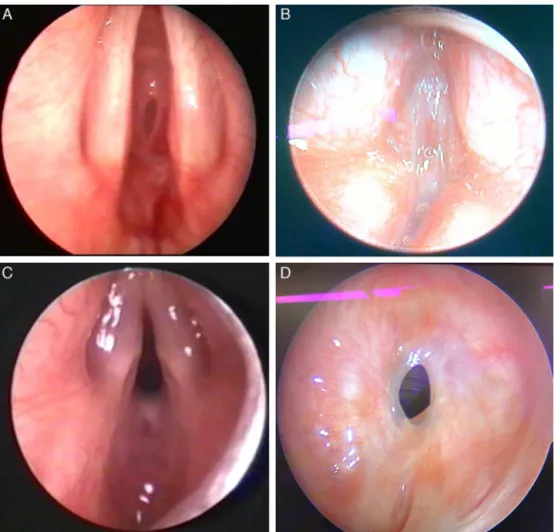
Subglottic(36%)---allhadMyer---CottongradeIII(Fig.1A); Anteriorglottic/subglottic(12%)---2patientshadCohen’s type4lesionwhileonehadtype3(Fig.1B);
Posteriorglottic/subglottic (12%)---all hadatype4 Bog-dassarian&Oslonlesion(Fig.1C);
Tracheal(16%)---5patientshadisolatedtracheallesions; four had a cervical tracheal pathology while one had a thoraciclocation.Onehadsevere,twomoderateandtwo mildnarrowing.Threeofthepatientshadalesionaffecting
Table1 Etiologyoftheairwaypathology.
Etiology Numberofpatients
Acquired 19
Prolongedintubation 13
Polytrauma 7
Neurologicaldisorder 3
Respiratoryfailurea 1
Suicidalattempt 1
Post-operativecomplicationb 1
Non-closureoftracheostomysite 3
Trachealtearc 1
Chemicalinjury 2
Congenitald 6
Total 25
a Patienthadcongenitalheartdisease.
b Patienthadsubglotticstenosisfollowingintubationfor rhino-plastyatanotherinstitution.
c Secondary to traumatic bronchoscopy while removing an aspiratedforeignbodyatanotherinstitution.
Airwayreconstructioninadvanced-stagelaryngotrachealstenosis 303
Figure1 Mappingofvariouspathologies.(A)Grade3isolatedsubglotticstenosis;(B)type4glotticweb;(C)type4posterior glotticstenosis;(D)cervical,moderate,1---3cmisolatedtrachealstenosis.
>3cmofthetracheallengthwhiletheother2hadalesion involving1---3cmofthetrachea(Fig.1D);
Laryngotracheal(20%)---4patientswithLTShadMcCaffrey stage3,whileonehadstage4;
Supraglottic(4%).
Thirty-two open reconstructive procedures were per-formed on25 patients (Tables 2 and 3). Sixteen patients had alreadyhad a procedure attempted prior toan open surgicalreconstructionwhetheritwasatracheotomy, bal-loondilatation, or lasertreatment. All theintraoperative findingscorrespondedtothetopographyresultantfromthe preoperativemapping.
Cartilage graftswere usedtoexpand the airway when needed;theseweremainlycartilageribgrafts(for cricoid expansion),conchalgraft(fortrachealexpansion)and thy-roidalargraft(ininfants)(Fig.2).Stentingwasneededto supportthereconstructedareain84%oftheperformed pro-cedures. The stents were different in types and included siliconestents (partof MontgomeryT-tube),endotracheal tubes, Aboulker stents, Montgomery T-tubes, and keels (Fig.3).Thedurationofstentingvariedfromoneto40days withameanof12.5andamedianof14.5days.
The outcome of the variouscorrective procedures was assessedbasedonthedecannulationrate,andthenumber of needed corrective procedures to achieve decannula-tion.Thenumberofneededendoscopywasalsocalculated andwasnotfound tocorrelate withthedegree of steno-sis or type of surgery performed. Twenty four out of 25 patientswereeventuallydecannulated(96%).Mostpatients requiredonlyonereconstructiveprocedure(80%)toachieve that.The numberofendoscopiesrequiredtofollow-upon the reconstructive procedures ranged from 1 to 7 with a mean of 2.8 and a median of 3. A general compari-sonbetweenpediatricandadultpatientsissummarizedin
Table4.
The most commoncomplication wasgranulation tissue formation,whichaffectedmainlypatientswithstents(75%). Postoperative complications are summarized in Table 5, along with the interventional steps taken to remedy them and their effect on the decannulation rate of the patients.
304
Bitar
MA
et
al.
Table2 Reviewedpediatricpatientswithadvancedlaryngealandortrachealstenosis.
N Age Co-morbidities Lesion Stage Tracheostomytiming Procedures Stenting
(type/duration/g.t.)
Numberof endoscopies neededaftereach surgery
Outcome
1 12d Cardiacanomalies SGS CottonMyerIII None LTR+AG(SS) ETTube-5days-No Three Decannulated
2 3m Sturge-Weber
syndrome
SGS CottonMyerIII Duringthe1st procedure
EndoscopicCO2laser ablation
Decannulated
Subglottic hemangioma
LTR+AG(SS) ETtube-5days-No Two
3 8m CongenitalTOF SGS CottonMyerIII Priortotheprocedure LTR+APG(DS) Siliconea5days---Yes Seven Decannulated
Esophagealatresia Duodenalatresia
4 1y None AGS CohenIV Priortothe1st
procedure
Anteriorcricoid split+AG(DS)
Keel-19
days-Yes-Mitomycin
Four Decannulated
LTR+AG(DS) Silicone-12
days-Yes-Mitomycin
Five
5 2y Seizures SGS CottonMyerIII Priorto1stthe
procedure
LTR+APG(DS) Silicone-7days-No Four Decannulated
LTR+AG(SS) ETtube-3days-No Two
6 3y Bilateralsevere
hearingloss
PGS BogdassarianOlsonIV Duringtheprocedure LTR+APG(DS) Silicone-21days-Yes Four Decannulated
7 5y None Tracheal Anand(tracheal,
moderate,>3cm)
Aftertheprocedureb Primaryrepairthrough
Thoracotomy(DS)
ETtube-11days-No Three Decannulated
8 6y Cerebralpalsy LTS Mc-CaffreyIII Priortotheprocedure LTR+AG(DS) None One Notdecannulated
9 9y None SGS CottonMyerIII Duringthe1st
procedure
Endoscopicdilatation Decannulated
LTR+APG(DS) Silicone-7days-Yes Two
10 9y None LTS Mc-CaffreyIII Priortothe1st
procedure
Endoscopicdilatation Decannulated
LTR+AG(DS) Abulkheir-5days-No Five
Endoscopicdilatation
11 12y None Tracheal Anand(cervical,
severe,>3cm)
Priortotheprocedure R+A(SS) ETTube-8days-No Two Decannulated
12 13y None PGS BogdassarianOlsonIV None LTR+PG(SS) ETtube-7days-No One Decannulated
13 15y None SGS CottonMyerIII Priortotheprocedure LTR+APG(DS) Silicone-21days-Yes Two Decannulated
14 15y Downsyndrome SGS CottonMyerIII Priortotheprocedure LTR+AG(DS) None-Yes Five Decannulated
15 15y Mildmental
retardationpost trauma(caraccident)
PGS BogdassarianOlsonIV Duringtheprocedure LTR+APG(DS) Silicone-25days-Yes Three Decannulated
16 16y None Tracheal Anand(cervical,mild,
1---3cm)
None Tracheoplasty+AG(SS) None One Decannulated
17 17y None AGS CohenIII Duringthe2nd
procedure
Endoscopicexcisionof web
Decannulated
LTR+AG(DS) Keel-27
days-Yes-Mitomycin
Three
Endoscopicexcisionof web
SGS,subglotticstenosis;LTR,laryngotrachealreconstruction;AG,anteriorgraft;APG,anteriorandposteriorgrafts;CTR,cricotrachealresection;R+A,resectionandanastomosis;PG, posteriorgraft;ET,endotrachealtube;SS,singlestage;DS,doublestage;g.t.,granulationtissue.
Airway
reconstruction
in
advanced-stage
laryngotracheal
stenosis
305
Table3 Reviewedadultpatientswithadvancedlaryngealandortrachealstenosis.
N Age Co-morbidities Lesion Stage Tracheostomy
timing
Procedures Stenting
(type/duration/g.t.)
Numberof
endoscopies
neededafter
eachsurgery
Outcome
1 18y None LTS Mc-CaffreyIII Duringthe3rd
procedure
R+A(SS) ETTube1day-No One Decannulated
Endoscopic Dilatation
LTR+APG(DS) Montgomery
T-tube21days-No
Five
Tracheoplasty+AG
(DS)
Siliconea40
days-Yes
One
2 18y Vocalcords
paralysis
LTS Mc-CaffreyIV Priortothe1st
procedure
CTR(DS) None Three Decannulated
RightPosterior cordotomy
3 18y None Supra-glottic NA Priortothe1st
procedure
Supraglottic reconstruction (DS)
Silicone21 days-No
One Decannulated
Releaseof adhesions Releaseof adhesions
4 22y None Tracheal Anand(cervical,
mild,1---3cm)
None Tracheoplasty+AG
(SS)
ETtube1day-No One Decannulated
5 23y None LTS Mc-CaffreyIII Priortothe1st
procedure
R+A(DS) Montgomery
T-tube7days-No
Two Decannulated
LTR+APG(DS) Silicone-17
days-No
Three
6 25y None SGS CottonMyerIII Priortothe
procedure
LTR+APG(SS) ETTube4days-No Three Decannulated
7 29y GERD AGS CohenIV Priortothe
procedure
CTR+AG(DS) None-Yes Three Decannulated
8 45y None SGS CottonMyerIII Duringthe3rd
procedure
Endoscopic Dilatation
Decannulated
LTR+APG(SS) ETtube5days-No Four
LTR+APG(DS) Silicone19
days-No
Two
Endoscopic dilatation
CTR(DS)
None-Yes-Mitomycin
One
SGS,subglotticstenosis;LTR,laryngotrachealreconstruction;AG,anteriorgraft;APG,anteriorandposteriorgrafts;CTR,cricotrachealresection;R+A,resectionandanastomosis;PG, posteriorgraft;ET,endotrachealtube;SS,singlestage;DS,doublestage;g.t.,granulationtissue.
306 BitarMAetal.
Figure2 Grafting.(A)LTRusingamodifiedboatforanteriorgraftingina15yoDownsyndromegirlwithanteriorSGS2rytoa highlong-standinghightracheostomy.(B)Graftbeingfixedtotheexpandedcricoidcartilage.(C)Anteriortrachealdefect2ryto lossofcartilageandformationoffibrosis(thatwasexcised)2rytoatraumaticandlong-standingtracheostomyina16yoboy.(D) Reconstructionusingauricularcartilagegraft.
Airwayreconstructioninadvanced-stagelaryngotrachealstenosis 307
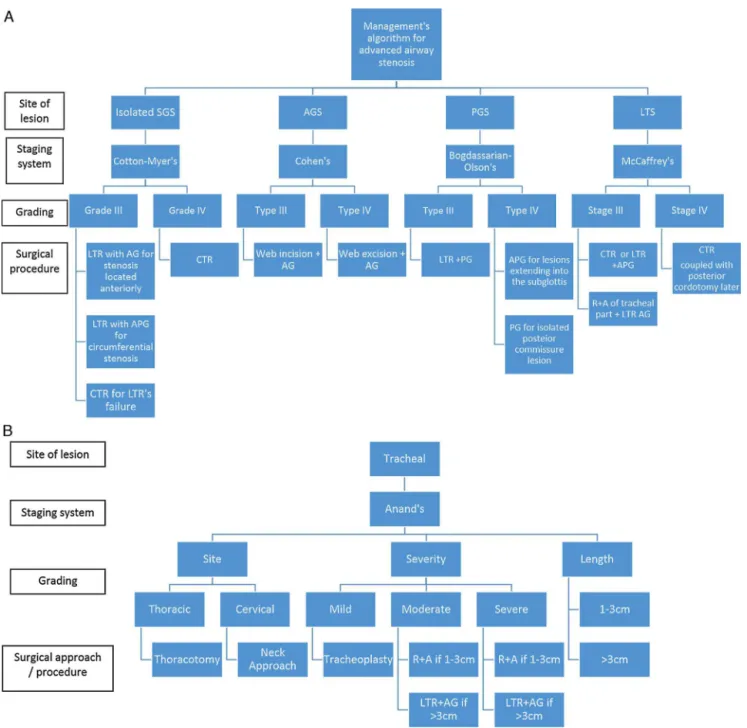
Figure4 (A)and(B)Suggestedalgorithmtofollowwhenmanagingadvancedairwaystenoticlesions.Thekeyistomapthelesion first,stageitproperlyandthentailorthesurgicalprocedureaccordingly.
functiontest)wasperformedonthesepatientsastheyhad noclinicalindicationforit.
Thevoicewasevaluatedpostoperativelyinourpatients by the speech pathologist.The assessment evaluated the needforspeechtherapyorothermeasuresincasethevoice wasnotadequateandornotacceptabletothepatientand orcorrespondingparents.AllpatientswithSGSorposterior glottic/subglottic stenosishad anormalvoice,eventhose patientswhoneededmorethanoneprocedure.
Wehavedevisedanalgorithmtomanageadvanced laryn-geal andor tracheal stenosis (Fig.4Aand B), focusingon accuratelymappingthelesionandstagingitbeforedeciding onchoosingaparticularsurgicalprocedure.
Pediatricpatients
Weoperated on17pediatric patients,aged12daysto17 years,mean8.2years,median 9years(Table 2).Eight of them(47%)hadassociatedco-morbiditiesthatcould poten-tially affect the postoperative course and eventually the outcome(exceptthehearingloss).
308 BitarMAetal.
Table4 Comparisonbetweenpediatricandadultgroups.
Pediatrics Adults
No.ofpatients 17 8
Meanage(y) 8.2 25
Comorbidity 8(47%) 2(25%)
Glottic/SGS 12(71%) 3(38%)
Noofprocedures 19 13
2proceduresneeded 2 1
3proceduresneeded 0 2
Graftingused 16(84%) 5(38%)
MeanNooffollow-upendoscopy 3 3
Incidenceofgranulationtissue 9(47%) 3(23%)
Meandurationofstenting(days) 12 14
Frequencyofstent’susing 16(84%) 10(77%)
Stentmadeofsilicone 9 6
performed asdouble-stage(11/16), mainly when anterior andposteriorgraftswereusedsimultaneously,whenthere wasaneed for relatively prolongedstenting, whena tra-cheostomytubewasneededtobekeptinthepostoperative periodforcontrollingairwaysecretionsinhighriskpatients (e.g.cerebralpalsy,seizures,Downsyndrome).
Stentingwasfrequentlyneededinthepediatricpatients (16/19 procedures), with silicone-made stents being the most commonly used. This resulted in a high incidence of granulation tissue formation that was dealt with appropriately (Table 5). Tracheomalacia wasencountered postoperatively only in pediatric patients, but was mild and did not require further intervention. Postopera-tive endoscopy was a crucial part of the care, ensuring close follow-up of the reconstructed area, removing any growing granulation tissue to prevent restenosis or for-mation of adhesions. Despite variability among patients, theremight bea trend to need more endoscopies in the youngestpatients(Fig.5).Allpatients weredecannulated
8
7
6
5
4
3
No of endoscop
y
2
0
0 2 4 6 8
Age (y)
10 12 14 16 18
1
Figure5 Numberoffollow-upendoscopiesneededaccording totheageofthepatient.
except one with cerebral palsy, who needed the tra-cheostomytubetostayinplacetoprovideairwaytoileting (Table2).
Thevoicewasadequateinmostpediatricpatients. How-ever, severe dysphonia was encountered in a one year old infantwith Cohen IVAGS (patient4, Table 2), where the vocal cords were found to be ill defined during the first surgery (Fig. 1B). She is currently receiving voice therapy and awaiting a trial of injection of hyalo-urinic acid to givebulk to her vocal folds and create adequate contact during phonation. A 17 year old girl also suf-fered frommoderatedysphonia(patient15,Table 2).She had a previous unsuccessful CO2 laser trial of excision of
the web prior to referral to our clinic. Her vocal cords lookedtraumatizedbythatinitial attemptandresulted in a persistent dysphonia. She is currently undergoing voice therapy.
Table5 Complicationsencounteredpostoperativelyandtheireffectondecannulation.
Typeofcomplication No.ofpatients Intervention Eventually
decannulated
Pediatric Adult Type No.ofpatients
Granulation tissue formation
9 3 Inhaledsteroids 2 2/2
Excision 11 11/11
MitomycinC 4 4/4
Tracheomalaciaa 4 0 Nointervention 4 4/4
Infectionandextrusionofgraftb 0 1 Removalofgraft 1 1/1
Re-stenosis 1 3 Surgicalcorrection 4 4/4
Persistenceofhoarsenessc 1 0 Nointervention 1 1/1
T-tubeobstruction 0 2 Tubecleaning 1 1/1
Tuberemoval 1 1/1
aMildinnature(patients2,3,5,14inTable2). b Posteriorgraftinpatient8---Table3.
Airwayreconstructioninadvanced-stagelaryngotrachealstenosis 309
Adultpatients
Eightadultpatientswerereviewed,aged18---45years,mean 25years,median22.5years(Table3).Onlytwopatientshad co-morbiditiesthatdidnotaffecttheoutcome,exceptfor thequalityofvoice.Incontrasttothepediatric patients, adult patients had morelesions affecting multiple levels, including supraglottic and tracheal. Multiple procedures wereneededin3patients,includingonepatientthatfailed LTRtwice andrequired asalvageCTR.The latter became theprocedureofchoiceforadultswithadvancedLTSafter encounteringdifficulties(e.g.infection,re-stenosis,delay in healing)using expansion proceduresusing ribcartilage grafts.Stents were usedasfrequently asin thepediatric patients for a comparable duration of time too, with surprisingly less granulation tissue formation. However, adultpatientshadothercomplicationsdetailedinTable5.
The postoperativevoiceoftheadultpatientswasgood in general. One patient (patient 7, Table 3) had gastro-esophageal reflux causing intermittent mild dysphonia; it wastreatedbyPPIwithgoodimprovement.Anotherpatient (patient2,Table3)hadmoderatedysphonia secondaryto pre-existingbilateralvocalcordparalysis(2rytohisinitial necktrauma).Heisreceivingvoicetherapytoimprovehis phonation.
Discussion
Congenitalairwaystenosisincludeslaryngealatresia, laryn-geal web, posterior glottic stenosis, subglottic stenosis and tracheal stenosis (complete tracheal rings). Most of these pathologies are believed to result from failure of recanalization of the airway during embryological devel-opment. Congenital subglottic stenosis is defined as a subglotticdiameteroflessthan4.5mminanewbornorless than4mminaprematureinfant,intheabsenceofacquired causes ofstenosis.10 It isthe mostcommon causeof con-genitalairwaynarrowingandthethirdmostcommoncause of congenital stridor after laryngomalacia and vocal cord paralysis.Itcanbeduetoacartilaginousmalformation,a fibrousnarrowingoraglandularhyperplasia.Ittendstobe milderthananacquiredstenosis,havingabetterprognosis andallowinginsomecasesawait-and-seepolicy.3
Acquired LTS is more common and results from pro-longed endotracheal intubation in 90% of the cases. It is estimatedthat1---5% ofintubatedchildrenmayeventually developLTS.11 Otherfactorsmayincludeexternaltrauma, inflammatory conditions or tumors. In children, the most susceptibleareaisthesubglottis,asitisthenarrowestpart of thelarynx, hasa delicatemucosa andsubmucosa, and is formedof acomplete cartilaginous ring.3The posterior glottic/subglotticareacanbeanothersiteofpathologyasit maybesubjectedtodirectpressuretraumafromthe endo-trachealtube. Other sites of trauma includethe trachea, duetoballoonortracheostomytubeinjury,andtheglottis secondarytointubationorexternaltrauma.
Inadults,LTSisusuallyacquiredandistheresultof intu-bation’straumainmorethan50%ofthecases.Autoimmune diseaseandidiopathicetiologycanaccountfor18% ofthe cases, each. The site of stenosis differs according to the etiological factor.The trachea,for example,is commonly
involved in autoimmune andiatrogenic causes, while less affectedinidiopathicetiology.12,13
Treatment may include balloon dilatation, which has recently gained popularity and has been tried even in patientswithadvancedstenosisorasaprimarytreatment modality.14,15Itwasusedinsomeofourpatientsbutwasnot successful,resultingintheneedofanopenreconstructive procedure.Nonetheless,theuseofballoondilatation post-operativelymightbebeneficialtotreatanearlyre-stenosis orstrictureandpreventitsprogressionintoamoresevere form.
Inasystematicreview ofdilatation asaprimary treat-mentmodalityforLTS,ChuengandChadha(2013)reporteda 50%successratewithballoondilatation,whichincreasedto 50---78%uponcouplingitwithadjuvanttherapy.16Recently, Günaydınetal.(2014)comparedballoondilatation toLTR asa primarytreatment modalityandnoticed thatballoon dilatationneedsmorerepetitiveinterventionsthanLTRwith ahigherre-stenosisrate(63.2%vs.31.3%).17Moreconcerns wereraisedinanotherrecentcomparativestudybyMaresh etal.(2014)whostatedthatthereisapoordefinitionofthe safetyprofileforballoondilatation.18Theybelievethatthe procedurecarriesrisksofworseningthestenosis,affects air-waytissueintegrity,andinparticularincreasesthechance ofneedingurgentairwayintervention.Balloondilatationhas definitelyits rolebut does notreplace the effective role ofLTRinprovidingalonglastingsafeairway,especiallyin advancedstenosis.
We have shown in our study that LTR is an impor-tanttoolintheairwaysurgeon’s handtorepairmoderate toseverelaryngotrachealstenosis.Laryngotrachealairway surgeryincludesa varietyoftechniques dependingonthe site and extent of the airway pathology. The aim is to increasetheairwaylumendiameterandallowthepatient tobedecannulatedasearlyaspossible.Attemptstorelieve suchan obstruction startedwaybackin 1956,whenRethi describedposteriorsplittingorcricoidotomywithlong-term stenting.2,19 Anterior cricoid split was then performed by Cotton and Seid in 1980, to enableextubation of infants sufferingfromSGS.These procedureswerelatermodified byintroducingcostalcartilagegraftswithorwithout sten-tingtheexpandedarea.20,21 Sincethen,variouscorrective andreconstructivetechniqueshavebeendescribed includ-ingcricotrachealresection.
Because laryngotracheal airway pathologies can affect differentareasofthelarynxandtrachea,itwouldbe impor-tant to use appropriate mapping of the lesion prior to decidingonthe bestreconstructive/corrective procedure. Wehave used acombination ofassessment techniques to correctly mapthe locationand extent of the lesionsand this combinedmethod proved tobe valid and beneficial, especiallythatintraoperative findingcorresponded toour preoperative topographic delineation of the lesion in all cases.
Thevariousavailablestagingsystemsarequiteusefulto correctlydocumentthepresentstenosis.Oneshouldavoid usingasinglestagingsystemtodescribeanytypeofstenosis, asthismayleadtoinaccuratedescriptionofthelesionand toinappropriatereportingofresults.
310 BitarMAetal.
beenusedinseveralreportstostageotherstenoticareas, like tracheal and laryngotracheal, something we do not agreeonoradvise.AsymptomaticisolatedSGSoftenneeds surgical intervention. It can be caused by a narrowing anteriorshelf,bilaterallateralshelvesoracircumferential narrowing.Themodeofexpansionwilldependonthetype ofnarrowing.Ananteriorshelfcanbeadequatelycorrected by an anteriorcricoid split and a modified boat cartilage grafttomaintain theexpansion. Itis often asinglestage procedurethatneedsashort-termornostenting,whichis usuallydoneusinganendotrachealtube.Asubglottiswith circumferentialstenosisorbilateralshelvesaremanagedby ananteriorandposteriorcricoidsplitwhicharesupported by a boat shaped posterior and modified boat shaped anterior grafts. The reconstructed area almost always needsstenting tostabilizethe areawhile healing occurs. Thedurationofstentingwilldependonthestabilityofthe reconstructedareaattheendoftheprocedure.
Stentsareoftenasourceofgranulationtissueformation andcareshouldbetakentomonitorsuchareactionto pre-ventrestenosisorformationofobstructiveadhesions.Inour series,noteverypatientofthe21whohadastent,got gran-ulationtissue,andgranulationtissueevenoccurredinsome patients whohad nostent (Tables 2 and 3). The ET tube wasusedin10patientsandwasnotassociatedwith granu-lationtissueformation,incontrasttothesiliconestentthat showedareaction in8 outof12 patients inwhomit was used.Theagerangewassimilarbetweenbothgroups,but themeandurationofstentingwasdifferent(5daysforET tubevs.21daysforthesiliconestent),reflectingthe neces-sitytolimitthestentingperiod.Lookingspecificallyatthe ageofthepatients,pediatricpatientsseemedtobemore vulnerabletoformgranulationtissuethanadultpatientsand thusshouldbemorecloselymonitoredwithfrequent endo-scopiesuntilresolutionofthegranulation tissueformation (Table4).
Performing a single-stage or a double-stage operation reliesontheabilitytoavoidatracheostomyattheendofthe procedurewhileachievingasafeairway.Italsoreliesonthe severityofthepresentpathology,andthestabilityofthe air-way.Includinggraftsduringreconstructionwoulddecrease the required stenting duration. Cartilage grafts are most commonlyharvestedfromtheribsbutalternativesinclude auricular,thyroidalarandseptalcartilage.2,22Ribgraftsare harvestedwithanintactperichondriumononesideto facil-itate mucosalization. Their success in reconstructing the subglotticareaexceedsthatincorrectingtrachealstenosis. Theyarealsonoticed tobetterintegratewiththeairway framework in the pediatrics than in adults. Adult’s carti-lagehas fociofossification which makesitscarving more difficult,suturingitintotheairwayframeworkharder,and healingslower,withapossibilityof acquiringaninfection andextruding.
When thesubglottic areaistotallyoccluded(grade4), theareacannotbeexpandedandisratherresected,hence the CTR. In addition, severe grade 3 stenosis, especially whenframeworkfibrosisexists,isbesttreatedwithCTR.23 Itisa morechallengingprocedure, butwithahigher suc-cessrate.24ThoughonlyfewcasesofCTRwerereviewedin thecurrentstudy,wehavefoundthisprocedureparticularly rewardingintheadultpatients,whereusingofcartilagerib graftsisavoided.
Whenthestenosisinvolves boththelarynxandthe tra-chea,themanagementmayincludetrachealresectionand anastomosisand or airwayexpansionusing cartilagegraft orCTR.Inthesecases,thereconstructionmethodis tailo-redspecificallytothepresentpathology, accordingtothe obtainedpreoperativetopographyofthelesion.Thesemay betoughcasesanddecannulationmaynothappenfollowing onereconstructiveprocedure(Table3).
Lookingat thosecasesthatfailedaninitial reconstruc-tiveproceduredespiteadequatepreoperativemapping,we couldrealizethefollowing:
Twopatients(patients1and5,Table3)weresubjected toinitial resectionandanastomosisof theinvolved upper trachea,whichresulted inaggravation oftheexistingSGS at the site of anastomosis (crico-tracheal junction). This necessitatedadditionalreconstructionofthesubglotticarea with an anterior and posterior graft. These 2 procedures could have been avoided by performing a CTR from the start.
Patients5(Table2)and1(Table3)hadanadditional pro-cedure (LTR withanterior graft) tocorrecta suprastomal collapse,whichisoftenassociatedwithalongstanding tra-cheostomytube.
Patient8(Table3)taughtustoavoidusingribcartilage graftsinsubsequentrepairofanadultairwaystenosis.ACTR fromthestartwouldhavesparedthepatienttwoadditional majorprocedures.
Patient4(Table2)wasachallengingcaseandtwo proce-durescouldnotbeavoided.Thepathologywasofwhatcould beclassifiedaspartiallaryngealatresia.Thesearedelicate andtoughcasesthatareexpectedtorequiremorethanone proceduretoreachasafeairway.
Isolatedtrachealpathologyarehardtostageasthereis nosinglecommonlyusedgradingsystemthatcanassessall trachealpathologies. When expansionisneeded, wehave foundtheauricularcartilagegraftofgreatusebothin pedi-atricandadultspatientsduetoitsappropriatecontourand elasticity thatconformswiththenormalshapeofthe tra-chealrings.25
Glotticstenosisislesscommonbutcanusuallybe man-aged successfullywith a singlesurgical procedure. Again, using appropriate classification for each type of stenosis (anteriorvs. posterior glottis)will ensure proper dissemi-nation ofinformationabout the existingpathologyamong treatingsurgeonsandinpublishedreports.
Airwayreconstructioninadvanced-stagelaryngotrachealstenosis 311
Thoughbothpediatricandadultpatientshadfavorable outcome, it is worth mentioning that pediatric patients (especiallytheinfantsandyoungchildren)needmore metic-ulous techniques during airwayreconstruction due to the smallerdimensionsoftheairwayandthetendencytoform granulationtissuewhenastentisused.Postoperativecarein theintensivecareunitaddsanotheraspecttothechallenges encountered in the pediatric patients regarding the need for sedation and tracheostomy/endotracheal tube care, and other medical treatment especially if co-morbidities exist.
To betransparent, it is veryimportant to specify how many reconstructive/corrective procedures were needed to achieve decannulation. Requiring multiple procedures mayreflecteither thecomplexity ofthecase (e.g. multi-levelsstenosis,co-morbidities)ortheinefficacyoftheused techniquefor theparticularlesion.Detailswillbeableto pinpointthereasonbehindaparticularfailure.
Conclusion
The review of our approach to open airway repair/ reconstruction showed its efficacy in advanced-stage laryngotracheal stenosis. Good knowledge of a variety of reconstructivetechniquesiscrucialtoachievegoodresults inavarietyofagegroups.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.McDonaldIH,StocksJG.Prolongednasotrachealintubation.A reviewofitsdevelopmentinapediatrichospital.BritJAnaesth. 1965;37:161---73.
2.Rizzi MD, Thorne MC, Zur KB, Jacobs IN. Laryngotracheal reconstruction with posterior costal cartilage grafts: out-comes at a single institution. Otolaryngol Head Neck Surg. 2009;140:348---53.
3.LesperanceMM,ZalzalGH.Laryngotrachealstenosisinchildren. EurArchOtorhinolaryngol.1998;255:12---7.
4.Pe˜na J, Cicero R, Marín J, Ramírez M, Cruz S, Navarro F. Laryngotracheal reconstruction in subglottic stenosis: an ancient problem still present. Otolaryngol Head Neck Surg. 2001;125:397---400.
5.MyerCM3rd,O’ConnorDM,CottonRT.Proposedgradingsystem forsubglotticstenosisbasedonendotrachealtubesizes.Ann OtolRhinolLaryngol.1994;103:319---23.
6.Cohen SR. Congenital glottic webs in children: a retrospec-tivereviewof51patients.AnnOtolRhinolLaryngol.1985;121: 2---16.
7.BogdasarianRS,OlsonNR.Posteriorglotticlaryngealstenosis. OtolaryngolHeadNeckSurg.1980;88:765---72.
8.McCaffreyTV.Classificationoflaryngotrachealstenosis. Laryn-goscope.1992;102:1335---40.
9.AnandVK,AlemarG,WarrenET.Surgicalconsiderationsin tra-chealstenosis.Laryngoscope.1992;102:237---43.
10.ZalzalGH,CottonRT.Glotticandsubglotticstenosis.In: Cum-mingsCW, Fredrickson JM, Krause CJ, Schuller DE, editors. Otolaryngology-head and neck surgery. 2nd edn St. Louis: Mosby-YearBook;1993.p.1981---2000.
11.CottonRT.Preventionandmanagementoflaryngealstenosisin infantsandchildren.JPediatrSurg.1985;20:845---51.
12.Lorenz R. Adult laryngotracheal stenosis: etiology and sur-gical management. Curr Opin Otolaryngol Head Neck Surg. 2003;11:467---72.
13.Gelbard A, FrancisD, SandulacheV,SimmonsJ, DonovanD, OngkasuwanJ.Causesandconsequencesofadult laryngotra-chealstenosis.Laryngoscope.2015;125:1137---43.
14.GuariscoJL,YangCJ.Balloondilationinthemanagementof severeairwaystenosis inchildrenand adolescents.JPediatr Surg.2013;48:1676---81.
15.Hautefort C,TeissierN,Viala P, VanDen Abbeele T. Balloon dilationlaryngoplastyfor subglotticstenosisinchildren.Arch OtolaryngolHeadNeckSurg.2012;138:235---40.
16.ChuengK,ChadhaN.Primarydilatationasatreatmentfor pedi-atriclaryngotrachealstenosis:asystematicreview.IntJPediatr Otorhinolaryngol.2013;77:623---8.
17.GünaydınRO,SüslüN,BajinMD,KuscuO,YılmazT,ÜnalÖF, et al. Endolaryngealdilatation versuslaryngotracheal recon-structionintheprimarymanagementofsubglotticstenosis.Int JPediatrOtorhinolaryngol.2014;78:1332---6.
18.MareshA, PreciadoDA,O’ConnellAP,ZalzalGH. A compara-tiveanalysisofopensurgeryvsendoscopicballoondilationfor pediatricsubglotticstenosis.JAMAOtolaryngolHeadNeckSurg. 2014;140:901---5.
19.AgrawalN,BlackM,MorrisonG.Ten-yearreviewof laryngotra-chealreconstructionforpaediatricairwaystenosis.IntJPediatr Otorhinolaryngol.2007;71:699---703.
20.FearonB,CottonR. Surgicalcorrectionofsubglotticstenosis ofthelarynx.Preliminaryreportofanexperimentalsurgical technique.AnnOtolRhinolLaryngol.1972;81:508---13. 21.Evans T. Laryngo-tracheoplasty. J Laryngol Otol. 1974;88:
589---97.
22.Fayoux P, Devisme L, Merrot O, Chevalier D. Thyroid alar cartilage graft in laryngoplasty anatomical study in prema-ture and newborn babies. Int J Pediatr Otorhinolaryngol. 2002;66:259---63.
23.HartleyBEJ,RutterMJ,CottonRT.Cricotrachealresectionasa primaryprocedureforlaryngotrachealstenosisinchildren.Int JPediatrOtorhinolaryngol.2000;54:133---6.
24.Monnier P, Lang F, SavaryM. Partial cricotracheal resection for pediatric subglottic stenosis: a single institution’s expe-rience in 60 cases. Eur Arch Otorhinolaryngol. 2003;260: 295---7.
25.Lusk RP, Kang DR, Muntz HR. Auricular cartilage grafts in laryngotracheal reconstruction. Ann Otol Rhinol Laryngol. 1993;102:247---54.
26.ReaF,CallegaroD,LoyM,ZuinA,NarneS,GobbiT,etal.Benign trachealandlaryngotrachealstenosis:surgicaltreatmentand results.EurJCardio-thoracicSurg.2002;22:352---6.
27.RutterMJ,CottonRT.Theuseofposteriorcricoidgraftingin managingisolated posteriorglotticstenosis inchildren.Arch OtolaryngolHeadNeckSurg.2004;130:737---9.
28.WyattME,HartleyBE.Laryngotrachealreconstructionin con-genital laryngeal webs and atresias. Otolaryngol Head Neck Surg.2005;132:232---8.
29.Rutter MJ, Hartley BEJ, Cotton RT. Cricotracheal resection in children. Arch Otolaryngol Head Neck Surg. 2001;127: 289---92.
30.YounisRT,LazarRH,AstorF.Posteriorcartilagegraftin single-stage laryngotrachealreconstruction. OtolaryngolHead Neck Surg.2003;129:168---75.
31.White DR,CottonRT,BeanJA, RutterMJ.Pediatric cricotra-chealresection:surgicaloutcomesandriskfactoranalysis.Arch OtolaryngolHeadNeckSurg.2005;131:896---9.
312 BitarMAetal.
33.WhiteDR,BravoM,VijayasekaranS,RutterMJ,CottonRT,Elluru RG.Laryngotracheoplastyasanalternativetotracheotomyin infantsyounger than6 months. Arch OtolaryngolHead Neck Surg.2009;135:445---7.
34.SaundersMW,ThirlwallA,JacobA,AlbertDM. Single-or-two-stagelaryngotrachealreconstruction;comparisonofoutcomes. IntJPediatrOtorhinolaryngol.1999;50:51---4.
35.GustafsonLM,HartleyBE,LiuJH,LinkDT,ChadwellJ,Koebbe C,et al. Single-stage laryngotracheal reconstructionin chil-dren: a review of 200 cases. Otolaryngol Head Neck Surg. 2000;123:430---4.