REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Ultrasound-guided
versus
surgical
transversus
abdominis
plane
block
in
obese
patients
following
cesarean
section:
a
prospective
randomised
study
Aykut
Urfalıo˘
glu
a,∗,
Murat
Bakacak
b,
Ömer
Faruk
Boran
a,
Fatih
Mehmet
Yazar
c,
Mahmut
Arslan
a,
Hafize
Öksüz
aaKahramanmarasSutcuImamUniversity,SchoolofMedicine,DepartmentofAnesthesiaandReanimation,Kahramanmaras,
Turkey
bKahramanmarasSutcuImamUniversity,SchoolofMedicine,DepartmentofObstetricsandGynecology,Kahramanmaras,Turkey cKahramanmarasSutcuImamUniversity,SchoolofMedicine,DepartmentofGeneralSurgery,Kahramanmaras,Turkey
Received7February2016;accepted27July2016 Availableonline21August2016
KEYWORDS
Transversusabdominis
planeblock;
Cesareansection;
Pregnantwomen;
Visualanaloguescale;
Analgesia
Abstract
Backgroundandobjectives: Ultrasound-guided transversus abdominis plane block demon-stratedefficacyinprovidingpost-operativeanalgesiabyprolongingthetimetofirstanalgesic requirementandreducingthetotalanalgesicconsumption.Thesurgicaltransversusabdominis planeblock,anoveltechnique,canbeperformedsafelyinobesepatientsinwhommusclelayers cannotbesufficientlyexposed.Here,wecomparedapplicability,efficacyandcomplicationsof surgicaltransversusabdominisplaneandultrasound-guidedtransversusabdominisplaneblocks inobesepregnantwomenfollowingcesareansectionundergeneralanesthesia.
Methods:Seventy-fivepregnant women with pre-andpost-pregnancy body massindex>30 wererandomizedandallocatedintotwogroups:Ultrasound-guidedtransversusabdominisplane block(UTgroup;n=38)andsurgicalTAPblock(STgroup;n=37).Visualanaloguescalescoresat post-operative0,2,6,12and24hours(h),timetofirstanalgesicrequirement,totalanalgesic consumptionamountin24h,post-operativesideeffects,complicationsandpatientsatisfaction wererecorded.
Resultsandconclusions: Age,AmericanSocietyofAnesthesiologistscore,operativeduration, bodymassindex,meantimetofirstanalgesicrequirementandtotalanalgesicconsumptionin 24hweresimilarbetweengroups,whilesignificantdifferencesinpre-andpost-pregnancybody massindexwereobservedbetweengroups.Blockproceduredurationswere7and10minutes inST andUTgroups, respectively.Nosignificant differencesinvisualanalogue scalescores
∗Correspondingauthor.
E-mail:[email protected](A.Urfalıo˘glu). http://dx.doi.org/10.1016/j.bjane.2016.07.009
wereobservedbetweenthegroupsatalltimes;itchingandnauseawasobservedinone(UT group)andfour(UTandSTgroups)patients,respectively.Surgicaltransversusabdominisplane block was safe inobesepregnant patients andprovidedsimilar post-operativeanalgesia to ultrasound-guidedtransversusabdominisplaneblock.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Bloqueiodoplano
transverso abdominal; Cesariana; Grávidas;
Escalavisual
analógica; Analgesia
Bloqueiocirúrgicodoplanotransversoabdominalversusguiadoporultrassom empacientesobesasapóscesárea:estudoprospectivoerandomizado
Resumo
Justificativaeobjetivos: Obloqueiodoplanotransversoabdominal(TAP)guiadoporultrassom (US)demonstroueficácianofornecimentodeanalgesianopós-operatórioaoprolongarotempo atéaprimeiranecessidadedeanalgésicoereduziroconsumototaldeanalgésico.Obloqueio TAPcirúrgico(umanovatécnica)podeserrealizado comseguranc¸aempacientesobesasnas quais ascamadasmusculares não podemser suficientementeexpostas. Comparamosa apli-cabilidade, aeficáciaeascomplicac¸ões dobloqueioTAPcirúrgicoedobloqueioTAP-USem gestantesobesassubmetidasàcesáreasobanestesiageral.
Método: Setentae cincomulheres grávidas comíndice de massacorporal (IMC) pré e pós-gravidez>30foramrandomicamentealocadasemdoisgrupos:bloqueioTAP-US(GrupoTAP-US,
n=38)ebloqueioTAPcirúrgico(GrupoTAP-C,n=37).Osescoresdaescalavisualanalógica(VAS) nostempos0,2,6,12e24horasdepós-operatório,otempoatéaprimeiranecessidadede analgésico,oconsumototaldeanalgésicoem24horas,osefeitoscolateraisnopós-operatório, ascomplicac¸õeseasatisfac¸ãodopacienteforamregistrados.
Resultadoseconclusões: Idade,estadofísicoASA,tempocirúrgico,IMC,médiadetempoaté aprimeiranecessidadedeanalgésicoeconsumototaldeanalgésicoem24horasforam seme-lhantesentreosgrupos,enquantodiferenc¸assignificativasforamobservadasentreosgrupos em relac¸ãoaoIMCpré-epós-gravidez.Asdurac¸õesdosprocedimentosdebloqueioforam7 e10minutosnosgruposTAP-USeTAP-C,respectivamente.Nãohouvediferenc¸asignificativa nosescoresVASentreosgruposemtodososmomentos;prurido enáuseaforamobservados emumpaciente(GrupoTAP-US)eemquatro(GrupoTAP-C),respectivamente.ObloqueioTAP cirúrgicofoiseguronaspacientesgrávidasobesaseforneceuanalgesiasimilaràdobloqueio TAP-USnopós-operatório.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Adequatepaincontrolfollowingcesarean sectionprovides benefitstomothersandinfantsandfacilitatesearly rehabil-itationandmobilisationofthemother,therebypreventing thromboemboliceventsandallowingearlybreastfeeding.1,2
Although the use of opioids with neuraxial block is pre-ferredbecauseitprovidesefficientpost-operativeanalgesia followingcesareansection,multimodalanalgesiaprotocols includingPatient-Controlled Analgesia (PCA) withopioids, paracetamolorNon-SteroidalInflammatoryDrugs(NSAIDs) have also been used with a neuraxial block and, gener-ally, under anesthesia conditions in which the use of a neuraxialblockisrestricted.3,4Despitethesubstantial
effi-cacy of opioidsas analgesic agents, they cause maternal sideeffects,includingnausea,vomiting,sedation,pruritus and respiratorydepression. Becauseneonatal side effects occur via placental transmission, peripheral nerve blocks
andinfiltration,recently,methodsthatuselesseramounts of opioids have been developed as a part of multimodal analgesia protocols.5 The use of the classic Transversus
AbdominisPlane block (TAP), a block commonly used for post-operativeanalgesiafollowinglowerabdominalsurgery, was first described by Rafi in 2001 and involves block-ade of the T7---L1 intercostal, subcostal, ilioinguinal and iliohypogastricnerves that provide sensoryinnervation to theanteriorabdominalwall.The techniqueinvolves anal-gesic agent introduction into the lateral abdominal wall and between the internal oblique and transversus abdo-minismuscles(termed asTAP).6 The classic blindmethod
isassociatedwithseveralcomplications7;therefore,ithas
largelybeenreplacedbyUltrasound-Guided(USG)TAP,first describedbyHebbartetal.,8becausefewercomplications
are encountered with USG-TAP.9,10 USG-TAP blocks
timetofirstanalgesicrequirementandreducingtotal anal-gesicconsumptionfollowingvarioussurgicalprocedures.11,12
However, serious technical difficulties, similar to those reported for classic TAP block, have been reported with theuseofUSG-TAP,particularlyinobesepatientswhohave excesssubcutaneousadiposetissue.TheuseoftheTAPblock method,describedbyOwenetal.,iscurrentlyconsideredas themostappropriatemethodforachievingablockinobese patientsbecause complicationscan be prevented through theuseofanintra-abdominalapproach.13Subsequently,
sur-gicalTAPblocktechniquehasbeen usedfollowingseveral laparoscopicsurgicalprocedures.14---16
In obese pregnant women, maternal and foetal side effectsmaycontributetoarequirementforhigh-dose anal-gesia.TechnicalchallengeshavelimitedtheuseofUSG-TAP blockin thisgroupof patients inpost-operativeanalgesia protocols.Therefore,thesurgicalTAPblockhasbeen con-sideredasamoreappropriatetechniqueforpost-operative analgesiainobesepregnantwomenfollowingcesarean sec-tionundergeneralanalgesiacomparedwithUSG-TAPblock intermsofapplicability,efficacyandcomplications.Toour knowledge,inthisstudy,wearethefirsttocomparethe util-ityofUSGandsurgicalTAPblockinobesepregnantpatients.
Methods
The present study was conducted in Sütcü ˙Imam Univer-sity, Anesthesiology and Reanimation department, after receivingapprovalfromtheScientificResearchEthics Com-mittee (2014/16 Protocol n◦ 187) and written consent of
all patients. The study was prospectively performed in 75 pregnant women scheduled for elective cesarean sec-tionundergeneralanalgesiawithpre-andpost-pregnancy bodymassindex(BMI)of>30kg.m−2.Weincludedpregnant
women who received general analgesia and were at ≥37 weeksofgestation,hadfastedfor6h,wereaged>18years andhadASAscoresofI---II.PatientswithBMIof>30kg.m−2
withknownhypertensivediseases(pre-eclampsia, eclamp-siaandchronichypertension),placentalorfoetal abnormal-ities,abdominalorganomegaly or bleedingdiathesis were excluded from the study. Seventy-five pregnant women wererandomlydividedintotwogroups:UT(USG-TAPblock;
n=38)andSTgroups(SurgicalTAPblock;n=37)using web-basedrandomisationsoftware(www.randomizer.org).
After routine monitoring Noninvasive Blood Pressure (NIBP),HeartRate(HR),pulseoxymetryandthree-leadECG ofallpatientstakentotheoperatingroom,haemodynamic and demographic data (age, weight, height and BMI) of included pregnant women were recorded. General anal-gesia inductionwas performed with2mg.kg−1 IVpropofol
and 1mg.kg−1 IV succinylcholine. At 30s after
intuba-tion, patients were transferred to the care of surgeons. Sevoflurane(2%)andO2/air(50%/50%)wereusedfor
main-taininganesthesia. TAPblockprocedure wasperformed in patientsintheUTgroupfollowingsurgeryusingaMyLabTM five (Esaote, Genoa, Italy) ultrasound device and LA 435 (6---18MHz)linearprobessterilisedwithantisepticsolution. Theprobewasinsertedbetweenthecostalmarginandiliac crest;a20gauge150mmregionalanesthesianeedle (Stimu-plex, B.BraunMelsungen AG,Germany) wasadvanced at thesamelevelastheUSGprobeusinganin-planetechnique
EOM
IOM
TAM
IOF P
Figure 1 Ultrasoundimage ofthe following three abdomi-nalmusclelayers:EOM,externalobliquemuscle;IOM,internal obliquemuscle;TAM,transversusabdominismuscle;IOF, inter-nalobliquefacia;P,intraperitonealarea.
IOM
TAM
IOF LA
Figure2 Spreadoflocalanesthetic(LA)withinthe transver-sus abdominis plane between the IOM and TAM following injection and downward displacement of the IOF (USG-TAP block).
aftervisualconfirmationofthreemusclelayers(from exter-nal tointernal; inward external oblique, internal oblique and transversusabdominis)(Fig. 1).Following transversus abdominismusclefasciapunctureandneedletip visualisa-tionbetweentheinternalobliqueandtransversusabdominis musclesunderUSG,apre-prepareddoseof20mLof0.25% Bupivacaine(Marcaine0.5%;AstraZeneca,London,UK)was administeredfollowinga0.5---1mLtestdose.Thesame pro-cedurewasrepeatedontheoppositesideusinganidentical amountoflocalanesthetic.Fig.2showsTAPspreadoflocal anesthetic.
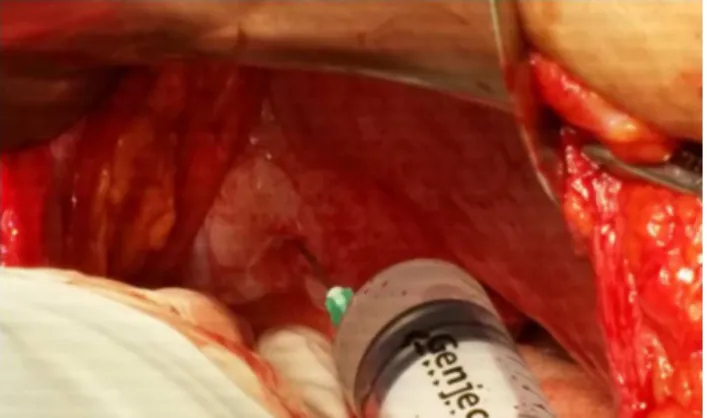
Figure3 Intra-abdominalaccessofablunt-endedneedleinto thetransversusabdominisplanethroughthetransversus abdo-minismuscle(surgicalTAPblock).
vesselsbythesurgeonusinganelevator,ablunt-ended 18 gaugeneedlewasadvancedthroughtheparietalperitoneum and transversus abdominis muscle. Following transversus abdominismusclefasciapuncture, 20mLof 0.25% bupiva-caine was intra-abdominally injected into the TAP at the midpointofthelineconnectingthecristailiacaandinferior costalmargin and at twolocations inthe lateral abdomi-nalwallat3---4cminferiortothepreviousmidlineinjection (Fig.3).Thesameprocedurewasrepeatedontheopposite sideusinganidenticalamountoflocalanesthetic.USG-TAP blockandsurgicalTAPblockprocedureswereperformedby the same anesthetic and surgeon. Block procedure dura-tion was defined as the time between probe placement ontheskinandlocalanesthetic injectionin theUTgroup and the timebetween the start and end of pre-prepared localanesthetic injectionintothe parietalperitoneumby thesurgeon.Allpatientswereadministeredwith1g para-cetamol IV and 50mg tramadol IV as standard at 20min prior tothe end of operation. The standard management ofpost-operativeanalgesiainvolvedtheuseoftramadolas a PCA according topatient preference depending on the degree of pain with routine 1g paracetamol IV (maximal dose, 4g.day−1)administered every6h. The PCAprotocol
wasappliedwithoutcontinuousinfusionasa12mgIVbolus dose of 300mg (6mL) tramadol in a 44mL isotonic solu-tionover 10min.Post-operative pain wasevaluatedusing VisualAnalogueScale(VAS),with0definedasnopainand 10definedastheworstpossiblepainandrecordedinboth groupsat0(immediatelypost-operation)andat2,6,12and 24h post-operatively. Timeto first analgesic requirement (min)andtotalanalgesicconsumption(mg)wererecorded. Post-operative adverse effectsand complications, suchas nausea/vomiting,pruritusandrespiratorydepression,were alsorecorded.Furthermore,patientswereaskedtoreport theirsatisfactiononascale between0and10points, sim-ilar toVAS scores, withscores recordedto assess patient satisfaction.
DatawereanalysedusingSPSS22.0(IBMCorp.,Armonk, NY, USA) and PAST3 (Hammer Ø, Harper DAT, Ryan PD. 2001; Paleontological statistics)software. The conformity of univariate and multivariate data to normal distribu-tions was analysed using the Shapiro---Wilk and Mardia tests, respectively, whereas Levene’s test was used to evaluate the homogeneity of variance. The independent
t-test was usedto compare the twoindependent groups, whereastheMann---WhitneyUtestwasusedwiththeMonte Carlosimulationtechnique.Wilcoxonsignedrankstestwas used for two repeat measurements of non-independent variables.Generallinearmodel-repeatedANOVAand Fried-man’s two-way test were used to study the interactions of repeated measurements of variables according to the groups, whereas non-parametric post hoc and LSD tests were used for the post hoc analyses. Fisher’s exact test wasused tocompare categorical data and odds ratios to quantifycategorical risk factors. Quantitative datain the tablesareexpressedasmeans±SD(StandardDeviation)and median±IQR(InterquartileRange)values.Categoricaldata aregiven as n (number) and percentages (%). Data were examined at a 95% confidenceinterval. p-Values of <0.05 wereconsideredtobestatisticallysignificant.
Results
Mean BMIin the ST group were32.2±1.56kg.m−2 before
pregnancy and 35.5±1.85kg.m−2 during delivery, with a
meanincrease of 3.3±0.77kg.m−2 observed during
preg-nancy.Mean BMI in theUT groupwere 32.5±1.86kg.m−2
beforepregnancyand 36.1±1.97kg.m−2 after pregnancy,
witha3.6±1.01kg.m−2changeobservedduringpregnancy.
StatisticallysignificantincreasesinBMIwereobserved dur-ingpregnancyinbothgroups,withnosignificantdifference observed between groups (p<0.01 and p=0.154, respec-tively)(Table1).
Themeanagewas30.2±5.17yearsintheSTgroupand 29.4±5.41 yearsin the UT group. Nostatistically signifi-cant differencewasobserved between groups (p=0.490). Nostatistically significant differences in median ASA val-ues or operative durationwere observed between groups (p=0.628 and p=0.716, respectively). The median block proceduredurationwaslowerintheUT(mean:7min;range: 4---10min) compared than in the ST group (mean: 10min; range: 8---12min; p<0.001). No significant differences in mean time to first analgesic requirement or total anal-gesicconsumptionover24hwereobservedbetweengroups (p=0.168 andp=0.539,respectively). Asignificant differ-enceinmedianpatientsatisfactionscoreswasnotobserved betweengroups(p=0.962)(Table2).
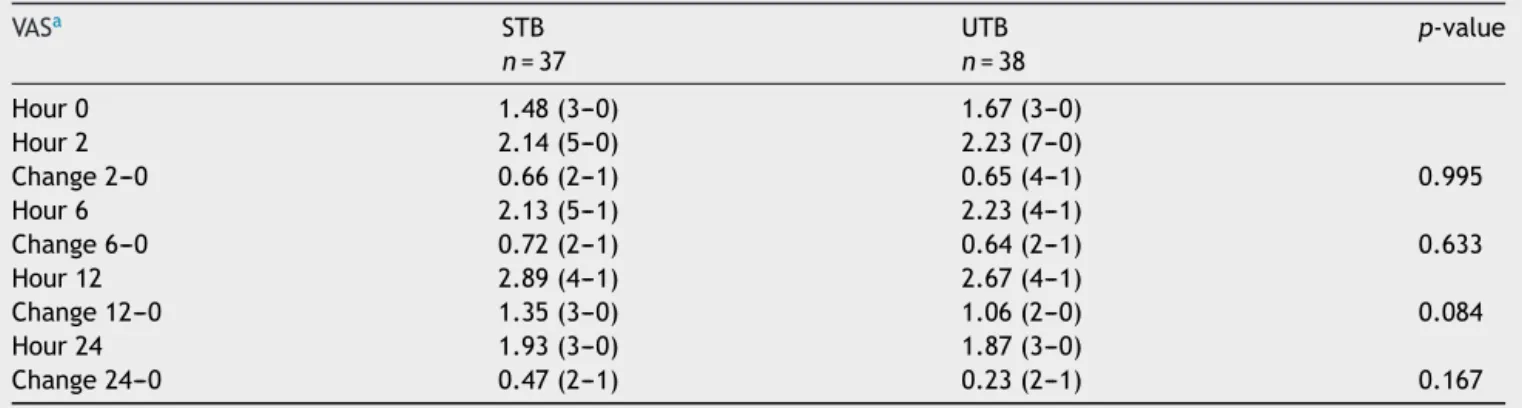
MedianVASscoresinboththegroupsat0,2,6,12and 24h post-operatively, and changes from baseline at each timepoint areprovidedinTable3. Accordingly,no statis-ticaldifferenceinVASscoreswasobservedbetweengroups atanytimepoint(p>0.05forall).
NauseawasobservedinfourpatientsineachoftheUT andSTgroups; itchingwasobservedin onepatientinthe UTgroupandwasattributabletodecreaseduseofopioids followingbothtechniques.p-Valuescouldnotbecalculated becausethesedatawerenotsuitableforstatisticalanalysis.
Discussion
Table1 BMIofpatientsbeforepregnancyandatthetimeofdeliveryaswellaschangesduringpregnancyaccordingtostudy group.
STB UTB p-value
BMI
Pre-pregnancy(1) 32.2±1.56 32.5±1.86
Atthetimeofdelivery(2) 35.5±1.85 36.1±1.97
Changeduringpregnancy 3.3±0.77 3.6±1.01 0.154
p-value <0.001 <0.001
GenerallinearmodelrepeatedANOVA,Wilks’Lambda;Fisherexacttest(MonteCarlo);Posthoctest,MonteCarlo;non-parametricpost hoctest.
UTB,USG-guidedtransversusabdominisplaneblock;STB,surgical-guidedtransversusabdominisplaneblock.
Table2 Age,ASA,operativeduration,blockproceduretime,timetofirstanalgesicrequirementandsatisfactionvaluesof patientsaccordingtostudygroup.
STB UTB p-value
n=37 n=38
Agea 30.2±5.17 29.4±5.41 0.490
ASAb 2(2---1) 2(2---1) 0.628
Operativedurationa 40.2±2.66 40.5±2.81 0.716
Blockproceduretime(min)b 7(10---4) 10(12---8) <0.001
Timetofirstanalgesicrequirement(min)a 513.2±102.78 476.6±125.59 0.168
Totalanalgesicconsumptionin24h(mg)a 91.1± 34.00 96.9± 46.38 0.539
Patientsatisfactionb 9(10---5) 9(10---4) 0.962
Independentt-test(Bootstrap);Mann---WhitneyUTest(MonteCarlo). aMean±SD(standarddeviation).
b Medianrange(maximum−minimum).
UTB,USG-guidedtransversusabdominisplaneblock;STB,surgical-guidedtransversusabdominisplaneblock.
Table3 MedianVASscoresat0,2,6,12and24handchangesfrombaseline.
VASa STB UTB p-value
n=37 n=38
Hour0 1.48(3---0) 1.67(3---0)
Hour2 2.14(5---0) 2.23(7---0)
Change2---0 0.66(2---1) 0.65(4---1) 0.995
Hour6 2.13(5---1) 2.23(4---1)
Change6---0 0.72(2---1) 0.64(2---1) 0.633
Hour12 2.89(4---1) 2.67(4---1)
Change12---0 1.35(3---0) 1.06(2---0) 0.084
Hour24 1.93(3---0) 1.87(3---0)
Change24---0 0.47(2---1) 0.23(2---1) 0.167
aMedian,range(maximum−minimum).
addition to neonatal side effects via opioid transmission throughbreastfeedingduringcesareansection.17,18Although
McKeen et al. reported the contrary, most studies have reportedTAP block utility asa component of multimodal analgesia protocols following cesarean sections in reduc-ing the use of opioids and associated opioid-related side effects.19,20Besidescesareansection,TAPblockageutilityin
providingsensorialblockadetotheabdominalwallhasbeen demonstratedasapartofpost-operativeanalgesia follow-ingmanylowerabdominalsurgicaltechniques.21,22Because
theTAPblockperformed usingtheclassicblindtechnique isassociatedwithsubstantialcomplications,USG,originally
usedforperipheralnerveblocks,hasrecentlybeenapplied toTAPblocks.8The USG-TAPblockincreasedsafety;
how-ever, becausetheabdominalmusclelayersandneedletip canbevisualised,liverdamagecouldbereported.Further, theTAPblock techniquemayremaintechnically challeng-ingdespitetheuseofUSGinobesepatientswithincreased subcutaneousadiposetissue.9Thus,thenewertechniqueof
surgicalTAPblockisconsideredtohavereducedmorbidity inthisgroupofpatients.13
section under general analgesia in terms of applicability, efficacy andsafety. On reviewing theliterature, we were unabletofindastudydirectlycomparingthesetwo meth-ods in obesewomen following cesarean section.Although demographicdata(age,ASAandoperativeduration)ofthe 75pregnantwomenwhowererandomlyassignedtotheST andUTgroups were foundtobe similar,herewe focused onobesepregnantwomenwithaBMIof>30kg.m−2because
weightgainwasanexpectedpregnancyoutcome.
Cesarean section is considered more appropriate in obesewomen;neuraxialblockshave greatersafetyduring cesareansectionthangeneralanesthesia.23Therefore,TAP
blocksaremoreoften performed withneuraxialblocksin previous studiesinvestigatingthepost-operativeanalgesic efficacy of TAP block following cesarean section. Belavy etal. reportedthatthe USG-TAPblock provideseffective analgesiawithouttheuseofopioidsfollowingcesarean sec-tionperformedwithspinalanesthesia,therebydecreasing opioid-relatedadverse effects.24 TAP block contributesto
spinal opioid analgesia by reducing post-operative opioid requirements andVAS scores.11 Despitetheadvantages of
spinalanesthesiadescribedin thisstudy,general anesthe-sia may be required in the patients who reject regional anesthesiaorhaveothercontraindications.Unlikeregional anesthesia, discontinuation of the analgesic effects of neuraxial block in the early post-operative period is a majordisadvantageofgeneralanesthesia.Therefore, post-operative analgesia is more important following general anesthesia.
Useofopioidsinthefirst24hpost-operativelyfollowing cesarean sectionundergeneral analgesiawassignificantly decreased bytheuse ofaTAPblock; however,VASscores werecomparablewiththecontrolgroup.1TAPblock
admin-istered during cesarean section under general analgesia increasedtimetofirstopioidsrequirement,decreasedtotal opioidconsumption,andsignificantlyreducedVASscoresup to12hpost-operatively.17Consistentwiththisresult,inour
study,timetofirstanalgesicrequirementincreasedinboth theSTandUTgroupsandthetotalanalgesicconsumption waslow at24h post-operatively.Beginningfromtheearly period,post-operativeVASscores werefound tobelowin boththegroupsinalltimeswithinthe24hfollow-upperiod. InthestudybyTanetal.,similarityinVASscoresofthestudy andcontrolgroupsmaybeattributabletotheuseofother analgesicagents,suchasparacetamol,withopioidsduring the post-operative period,which is similar toour study’s results.ATAPblockprovidessomaticsensoryblockadeonly in theabdominalwall,but it doesnot blockvisceral pain originatingfromtheuterus.25 Therefore,visceralpainmay
notbepreventedwiththeuseofadditionalagents,thereby leadingtoVASscoremisevaluation.
With decreased useof opioids, related adverse effects includingnausea,vomiting,pruritusandrespiratory depres-sion are expected to be less frequently observed. Here, nauseawasseeninfourpatientsineachUTandSTgroup; itchingwasobserved inonepatientin theUTgroup.This findingwasattributabletodecreaseduseofopioidsinboth groups.Additionally,highpatientsatisfactionscoresinboth groupswereanexpectedoutcomebecauseoffeweradverse effects and adequate post-operative analgesia. A meta-analysis of multiple TAP block studies found that opioid consumption and related side effects decreased and that
patientsatisfactionwashighwhenUSG-TAPblockwas per-formedduringlowerabdominalsurgeries.20
Although the use of USG in TAP block was apparently safe, as in the present study, technical difficulties may occasionallybeencounteredregardingprobeinsertionand distinctionoftheabdominalmusclelayersbecauseof obe-sity.Needle-relatedvisceralorgandamagecanbeprevented bytheintra-abdominalapplicationof aTAPblockby visu-alising the visceral organs during open surgeries.13 In our
study,nocomplicationswereobservedfollowingeitherUSG orsurgicalTAPblocks,whereassurgicalblockdurationwas significantlyshorterwiththe surgicalTAP blockthan with theUSGblock.
There wereseveral limitations of this study. First,the levelofsensorialblockwasnotconfirmedafterblockade, andonlypost-operativeVASwasassessedasapartof block-adesuccessevaluation.However,thisevaluationcouldnot be completely performed because patients administered generalanesthesiaareunlikelytoprovidereliableresponses regarding sensorial block during the early post-operative periodandatlatertimes,particularlyinT7---L1dermatome regionin which blockade wasprovided and wasenclosed withplaster.SecondforcomparingTAPblockmethods,there isalackofacontrolgroupwithoutblockinwhichonlyPCAis administered.Here,ourprimaryobjectivewastocompare theefficacy andcomplications between USG and surgical TAPblocks.Wedidnotincludeathirdcontrolgroupbecause ofalackofappropriatepregnantwomenwhometthestudy criteria; the mean time to first post-operative analgesic requirementandtotalanalgesicconsumptioninthis popu-lationshasbeenreportedbyseveralpreviouslyconducted studies.
Conclusion
USGandsurgicalTAPblocksweresafeandhadsimilar effi-cacyinprovidingpost-operativeanalgesiainobesepregnant womenfollowingcesareansectionundergeneralanalgesia. Surgical TAP block is an efficacious, safe and rapid tech-nique, particularly in patients in whom sensory blockade istechnicallychallenging, anddoesnot requireadditional equipment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TanTT,TeohWH,WooDC,etal.Arandomisedtrialofthe anal-gesicefficacyofultrasound-guidedtransversusabdominisplane blockaftercaesareandeliveryundergeneralanaesthesia.Eur JAnaesthesiol.2012;29:88---94.
2.PatelSA,GotkinJ,HuangR,etal.Transversusabdominisplane block for postoperative analgesia aftercesarean delivery. J MaternFetalNeonatalMed.2012;25:2270---3.
3.KwokS, Wang H,Sng BJ.Post-caesarean analgesia.JTrends AnaesthCritCare.2014;4:189---94.
5.ChandonM,BonnetA,BurgY,etal.Ultrasound-guided transver-sus abdominis planeblock versus continuouswound infusion for post-caesarean analgesia:a randomisedtrial. PLOSONE. 2014;9:e103971.
6.RafiAN.Abdominalfieldblock:anewapproachviathelumbar triangle.Anaesthesia.2001;56:1024---6.
7.Farooq M, Carey M. A case of liver trauma with a blunt regionalanesthesianeedlewhileperformingtransversus abdo-minisplaneblock.RegAnesthPainMed.2008;33:274---5. 8.Hebbard P, Fujiwara Y, Shibata Y, et al. Ultrasound-guided
transversus abdominis plane block. Anaesth Intensive Care. 2007;35:616---7.
9.LancasterP,ChadwickM.Livertraumasecondaryto ultrasound-guidedtransversusplaneblock.BrJAnaesth.2010;104:509---10. 10.Weiss E, Jolly C, Dumoulin JL, et al. Convulsions in 2 patientsafterbilateralultrasound-guidedtransversus abdomi-nisplaneblocksforcesareananalgesia.RegAnesthPainMed. 2014;39:248---51.
11.Canovas L, Lopez C, Castro M, et al. Contribution to post-caesareananalgesiaofultrasound-guidedtransversusabdominis planeblock.RevEspAnestesiolReanim.2013;60:124---8. 12.Zhao X, Tong Y, RenH, et al. Transversus abdominis plane
blockfor postoperativeanalgesiaafterlaparascopic surgery: a systematic review and meta-analysis. Int JClin Exp Med. 2014;7:2966---75.
13.Owen DJ, Harrod I, Ford J, et al. The surgical transversus abdominis plane block-a novel approach for performing an establishedtechnique.BJOG.2011;118:24---7.
14.Elamin G, Waters PS, Hamid H, et al. Efficacy of a laparascopically delivered transversus abdominis planeblock technique during elective laparascopic cholecystectomy: a prospective double-blind randomised trial. J Am Coll Surg. 2015;221:335---44.
15.ElHachemL, SmallE,ChungP,etal.Randomizedcontrolled double-blindtrialoftransversusabdominisplaneblockversus
trocarsiteinfiltrationingynecologiclaparoscopy.AmJObstet Gynecol.2015;212,182.e1-9.
16.El-DawlatlyA,Al-DohayanA. ˙Inside-outtransversusabdominis planeblock.SaudiJAnaesth.2014;8:315---6.
17.Eslamian L, Jalili Z, Jamal A, et al. Transversus abdominis planeblockreducespostoperativepainintensityandanalgesic consumptioninelectivecesareandeliveryundergeneral anes-thesia.JAnesth.2012;26:334---8.
18.WittelsB, ScottDT,SinatraRS. Exogenousopioids inhuman breastmilkand acuteneonatalneurobehavior:apreliminary study.Anesthesiology.1990;73:864---9.
19.McKeenDM,GeorgeRB,BoydJC,etal.Transversusabdominis planeblockdoesnotimproveearlyorlatepainoutcomesafter cesareandelivery:arandomizedcontrolledtrial.CanJAnesth. 2014;61:631---40.
20.FuscoP,ScimiaP,PaladiniG,etal.Transversusabdominisplane blockforanalgesiaaftercesareandelivery.Asystematicreview. MinervaAnestesiol.2015;81:195---204.
21.YuN,LongX,Lujan-HernandezJR,etal.Transversus abdominis-planeblockversuslocalanestheticwoundinfiltrationinlower abdominalsurgery: asystematicreviewand meta-analysisof randomizedcontrolledtrials.BMCAneshesiol.2014;14:121. 22.Walter CJ, Maxwell-Armstrong C, Pinkney TD, et al. A
ran-domisedcontrolled trialof theefficacyofultrasound-guided transversusabdominisplane(TAP)blockinlaparoscopic colo-rectalsurgery.SurgEndosc.2013;27:2366---72.
23.RaoDP,RaoVA.Morbidlyobeseparturitientchallengesforthe anaesthesiologist,includingmanagingthe diffucultairway in obstetrics.Whatisnew?IndianJAnaesth.2010;54:508---21. 24.BelavyD, Cowlishaw PJ,Howes M, et al. Ultrasound-guided
transversusabdominisplaneblockforanalgesiaaftercaesarean delivery.BrJAnaesth.2009;103:726---30.