REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Efficiency
of
bupivacaine
and
association
with
dexmedetomidine
in
transversus
abdominis
plane
block
ultrasound
guided
in
postoperative
pain
of
abdominal
surgery
Recep
Aksu
a,∗,
Gülc
¸in
Patmano
a,
Cihangir
Bic
¸er
a,
Ertan
Emek
b,
Aliye
Esmao˘
glu
C
¸oruh
baErciyesUniversity,MedicalFaculty,DepartmentofAnesthesiology,Kayseri,Turkey bErciyesUniversity,MedicalFaculty,DepartmentofGeneralSurgery,Kayseri,Turkey
Received25May2016;accepted10August2016 Availableonline1October2016
KEYWORDS
Dexmedetomidine; Bupivacaine; Transversus abdominisplane block;
Lowerabdominal surgery
Abstract
Backgroundandobjectives: Weaimedtoevaluatetheeffectofbupivacaineand
dexmedeto-midineaddedtobupivacaineusedintranversusabdominisplane(TAP)blockonpostoperative
painandpatientsatisfactioninpatientsundergoinglowerabdominalsurgery.
Methods:Patientssubmittedtolowerabdominalsurgerywereenrolledinthestudy.After
anes-thesia induction,ultrasound guidedTAPblockwas performed.TAPblockwas obtainedwith
21mL0.9%salineinGroupC(n=31),20mL0.5%bupivacaine+1mLsalineinGroupB(n=31),
and20mL0.5%bupivacaine+1mLdexmedetomidine(100g)inGroupBD(n=31).
Results:VisualanalogscalescoreswerelowerinGroupBDcomparedtoGroupC,atalltime
points(p<0.05);itwasloweringroupBDthaningroupBat10---24h.InGroupB,itwaslower
thanGroup Cat 2---8h(p<0.05).Total morphineconsumption waslower inGroup BD
com-paredtoothergroupsandloweringroupBthaninthecontrols(p<0.001).Patientsatisfaction
washigherinGroupBDthaninothergroupsandwashigherinbothstudygroupsthaninthe
controls(p<0.001).Nausea-vomitingscores,antiemeticrequirement,oradditionalanalgesic
administrationwerenotsignificantamonggroups(p>0.05).
Conclusions: TheadditionofdexmedetomidinetobupivacaineonTAPblockdecreased
postop-erativepainscoresandmorphineconsumption;italsoincreasedpatientsatisfactioninpatients
undergoinglowerabdominalsurgery.Dexmedetomidinedidnothaveanyeffectonnauseaand
vomitingscoreandantiemeticrequirement.
©2017SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan
openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.Aksu). https://doi.org/10.1016/j.bjane.2016.08.003
PALAVRAS-CHAVE
Dexmedetomidina; Bupivacaína; Bloqueiodoplano transverso abdominal; Cirurgiaabdominal inferior
Eficáciadebupivacaínaeassociac¸ãocomdexmedetomidinaembloqueiodoplano
transversoabdominalguiadoporultrassomnadorapóscirurgiaabdominal
Resumo
Justificativaeobjetivos: Oobjetivodoestudofoiavaliaroefeitodebupivacaínae
dexmedeto-midinaadicionadaàbupivacaínaparabloqueiodoplanotransversoabdominal(TAP)nocontrole
dadoresatisfac¸ãodopacienteapóscirurgiaabdominalinferior.
Métodos: Pacientessubmetidosàcirurgiaabdominalinferiorforamincluídosnoestudo.Apósa
induc¸ãodaanestesia,obloqueioTAPguiadoporultrassomfoirealizadocom21mLdesoluc¸ão
salinaa0.9%noGrupoC(n=31),20mLdebupivacaínaa0,5%+1mLdesoluc¸ãosalinanoGrupoB
(n=31)e20mLdebupivacaínaa0,5%+1mLdedexmedetomidina(100g)nogrupoBD(n=31).
Resultados: OsescoresdaescalavisualanalógicaforammenoresnoGrupoBDcomparadoao
GrupoCemtodosostemposmensurados(p<0,05);foimenornoGrupoBDquenoGrupoBem
10-24horas.NoGrupoB,osescoresVASforammenoresquenoGrupoCem2-8horas(p<0,05).
OconsumototaldemorfinafoimenornoGrupoBDemcomparac¸ãocomoutrosgruposemenor
noGrupoBquenoscontroles(p<0,001).Asatisfac¸ãodopacientefoimaiornoGrupoBDque
nosoutros grupose maiorem ambos osgrupos deestudo quenoscontroles (p<0,001).Os
escoresdenáuseaevômito,necessidadedeantieméticooudeanalgésicosadicionaisnãoforam
significativosentreosgrupos(p>0,05).
Conclusões:Aadic¸ãodedexmedetomidinaàbupivacaínaembloqueioTAPreduziuosescores
dedoreoconsumodemorfinanopós-operatório,alémdeaumentarasatisfac¸ãoempacientes
submetidos àcirurgia abdominal inferior. Dexmedetomidinanão apresentou efeito sobreos
escoresdenáuseaevômitoeanecessidadedeantiemético.
©2017SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum
artigoOpen Accesssobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Openinguinalhernioplastyandopenappendectomysurgery mostlycause mild to severe postoperative pain.1---3 Ifnot
treated, postoperative pain leads to chronic pain and undesirable events ranging from patient discomfort and prolongedimmobilitytothrombolyticphenomenonand pul-monarycomplications.4,5Regardingchronicpainformation,
postoperativepainstate, andnerve injury duringsurgery, aswellasinsufficientearlypostoperativepaincontrol,are amongtheriskfactors.4,6Expectedpainprevalence
follow-ingherniarepairwasdeterminedas54%andpostoperative2 yearcumulativeprevalencewasfoundtobe30%.7
Transver-sus abdominal plane (TAP), one of the peripheral nerve blocks,wasreportedtoreduce postoperativepain follow-ing hysterectomy, colorectal surgery, appendectomy, and inguinalhernioplasty.2,3,8---10
TAP is located between the oblique muscles and the transverseabdominismuscles.OnTAPiliohypogastricnerve liesandanterolateralabdominalwallafferentT6-L1nerves isgotblockedwithblockageofthisarea.1,5
Single and continuous TAP block techs have been suc-cessfully administered for pain control in the repair of inguinal hernia.11,12 However, the duration of single-dose
administeredTAP blockis limited totheeffect of admin-istered local anesthetics. Addition of adjuvant to local anesthesiamayprolongtheblock’sduration.13
Dexmedeto-midineisaselectivealpha-2 adrenergicagonistwithboth analgesicandsedativeproperties.14 Whenadministeredas
a perineural adjuvant, dexmedetomidine reduces initial blockingtimewhilstprolongingsensoryandmotorblockade duration.15
Materials
and
methods
Local ethics approval for the study was received (2014/37). Then the study was recorded on
http://www.clinicaltrials.gov (NCT02064530). After
receiving written consent from the patients, 93 ASA I---II patientsaged 18---65yearswere included inthe study and scheduled for open appendectomy repair or inguinal herniaadministrations.Aplacebo-controlled,randomized, prospective and triple-blinded study was carried out, and blinding wasappliedboth tothe patients andto the investigators and data collection team. Patients were excluded if they: had a history of allergy to bupivacaine and dexmedetomidine; wereor may have been pregnant; hada coagulationdisorder,seriouscardiacandpulmonary disease; had an administration site infection; or were unable to understand the scoring system. Patients were randomized with sealed envelopes. The control group (Group C) (n=31), bupivacaine group (Group B) (n=31) and bupivacaine+dexmedetomidine group (Group BD) (n=31) were determined. The Groups C, B,and BD were given, respectively, 21mL 0.9% NaCl, 20mL 0.5% bupiva-caine (without epinephrine) (Bustesin® 5mg.mL−1, Vem
Pharmaceuticals,Ankara,Turkey)+1mL0.9%NaClsolution, and 20mL 0.5% bupivacaine (without epinephrine) and 100g (1mL) dexmedetomidine (Precedex® 100g.mL−1,
rate(HT)valueswererecorded.Anesthesiawasinducedby administrationof5---7mg.kg−1thiopental(Pental®
,Ulagay, Turkey), 0.6mg.kg−1 rocuronium bromide (Esmeron®
, Schering-Plough,Holland)and1g.kg−1fentanyl(Talinat®,
Vem Pharmaceuticals, Istanbul, Turkey). When muscles were sufficiently relaxed, endotracheal intubation was performed.Patientsweremonitoredandventilatedwithan electronicanesthesiadevice (S/5Avance, DatexOhmeda, Finland).
For anesthesia supply, 4---6% desflurane (Suprane® Liq-uid100%,Abbott,Norway)wasaddedto50%oxygen+50% nitrogenmixture.Itwasprojectedtoadminister1g.kg−1
intravenousfentanylinanycasewhereMAPandHTvaluesgo upto20%overbasalvaluesbeforeinduction.AMAPdecrease of more than 20% was considered to be hypotension. In suchcases,desfluraneconcentrationwouldbereducedand 5mgephedrinewouldbeintravenouslyadministered,if nec-essary. Slowing down of the heart rate to less than 50 beats/min was considered to be bradycardia, and 0.5mg atropine was planned to be administered in these cases. The skin antiseptic was provided with 2% chlorhexidine solution following anesthesia induction. A high-frequency (5---10MHz) ultrasound linear probe (Mindray M7, China) was transversely located on the anterolateral abdominal wall between the iliac crest and the subcostal area, and neurophasia(TAP)between theinternal obliqueand tran-verseabdominiswasidentified.A50mmnerveblockneedle (Braun Melsungen AG, Melsungen, Germany) was concur-rently located on the area and pre-prepared agent was injectedafternegativeaspiration.Theinjectedliquidwas observedonultrasoundtobedistributedinadarkovalform inTAP.SurgicalprocedurestartedafterperformingTAPblock anddistancebetweenstartandstoppointofwoundincision wasrecordedaslengthofincision.
Anesthesia was discontinued following surgical opera-tion and residual block was reversed using 0.02mg.kg−1
atropine (Atropin Sülfat® 0.25mg.mL−1, Biofarma,
Istan-bul, Turkey) and 0.04mg.kg−1 neostigmin (Neostigmine®
0.5mg.mL−1, Adeka,Turkey). When the patientcame out
ofanesthesiaandhadspontaneouslygainedsufficienttidal volumeand motorfunction, theywere transferredto the Postoperative Care Unit (PCU). Onegram of paracetamol (Perfalgan®, Bristol-Myers Squibb, USA) was intravenously administeredasastandardpostoperativeanesthesiaregime and attached to a Patient-Controlled Analgesia (PCA), device solution wasprepared by adding 100mg morphine (Morphine® 10mg.mL−1,Galen,Istanbul,Turkey)to250mL
0.9%NaCl.ThePCAdevicewassettohavea7minlockout timeanda0.5mgbolus.Casesweretransferredtogeneral surgery after 2h follow-up in PCU during the postopera-tiveperiod.Theseverityofpainatrestwasassessedusing a10cmVisual AnalogScale (VAS),scaled fromleft;0=no pain, to right; 10=worst imaginable pain, and recorded post-operative0,2,6,8,10,12,18and24h.
PatientswithaVASscoreofmorethan4during assess-ment were given50mg i.v. diclofenacsodium (Dicloron®,
Abbott,Norway).Thedosesofmorphineandanalgesic con-sumed were recorded. The satisfaction of patients was recorded in the 24th hour following operation. Patient satisfactionassessmentscoreswere:1--- poor,2--- moder-ate,3--- good,4 ---perfect.16 Patientsweremonitoredfor
24h in terms of nausea,vomiting, altered mental status,
hypotension, hypertension, bradycardia, and tachycardia, allofwhich might occurasa resultofthedrugs adminis-tered.Nausea and vomiting assessment scores were: 1 ---none,2 ---nausea,3--- retching,4 ---vomiting. Allpatents having nausea, retching or vomiting were planned to be givenanantiemetic.8Inthepresenceofnausea---vomiting,
it was planned to administer 10mg i.v. metoclopramide HCL(Primperan®,Biofarma,Turkey)first,andthen4mgi.v.
ondansetron(Zofran®,GlaxoSmithKline,Italy)following1h
follow-upifnecessary.The primaryoutcome of thisstudy wastoassessmorphineconsumptionforpost-operative pur-pose.Thesecondaryaimwastomeetpatient’ssatisfaction withrespect to pain scores assessed withVAS within the postoperative 24h period,period of hospitalization, nau-sea,vomitingandantiemetic.To calculatesamplesizefor thestudy,10 cases werepre-studied and theaverages of postoperative24hmorphineconsumptioncalculated.When alphais0.05,andˇ(thefalsenegativerate)is0.20,andthe minimummeandifferenceis6.3mgandexpectedstandard.
Statistical
analysis
DatawasstatisticallyassessedusingtheStatisticalPackage for the Social Sciences (SPSS for Windows, Version 21.0, IBM Corp, Armonk, NY). The Shapiro---Wilk normality test was used to determine whether sample distribution was normal or not. Descriptive statisticsunit number (n) was givenasmean±standarddeviationandmedian(min---max) values.Onewayanalysisofvariance(ANOVA)wasusedto evaluatewhethertherewasadifferenceamonggroups of havingnormaldistribution.To evaluateparametershaving abnormaldistribution,theKruskal---Wallistest, oneof the non-parametrictests,wasused.
Thesignificantoneswerecomparedusingpairwise com-parisons and it was determined that which group has statisticaldifference. A valueof p<0.05 wasaccepted as statisticallysignificant.
Results
No significant difference was observed in age, weight, length,bodymass index,gender, ASA class,surgerytype, surgeryduration,lengthofincision,dischargeduration,or intraoperativetofentanylconsumption(p>0.05)(Table1). WhencomparedtoGroupC,asignificantdecreaseinheart ratewas observed in GroupsB andBD in the 10th,30th, 45th,and60thminutesoftheoperation(p<0.05)(Fig.1). Duringthepostoperativeperiod,theincreasecontinuedin GroupBDin0and24thhincomparisonwithGroup C,and in the 120th min, 6th, and 12thh in comparison to both GroupCandGroupB(p<0.05)(Fig.1).Intheassessment ofheartratewithingroups,afallaccordingtoinitialheart rateswasobservedinthe10th,30th,45th,and60th min-utes of operation in Group B, and at every measurement timeexcludingthepostoperative24hinGroupBD(p<0.05). However,0.5mgatropinewasneededastwoofthepatients’ HRwent below 50beats/min. Nodifference compared to initialvalueswasnoticedinGroupC(p>0.05)(Fig.1).
Table1 Demographiccharacteristics,hospitalstayandintraoperativefentanylconsumption.Dataaregivenasmean(SD)or
number(%).
GroupC
(n=31)
Mean±SD
GroupB
(n=31)
Mean±SD
GroupBD
(n=31)
Mean±SD
p
Age(years) 44.2±13.9 43.5±15.0 43.2±15.0 0.962
Weight(kg) 80.8±14.6 76.3±12.0 77.1±6.9 0.279
Height(cm) 172.6±7.2 171.2±6.5 174.1±7.4 0.290
BMI 27.4±5.0 26.0±3.7 2.0±5.5 0.445
Gender(F/M)
n(%)
7(22.6)
24(77.4)
7(22.6)
24(77.4)
6(19.4)
25(80.6)
0.439
ASA(I/II)
n(%)
24(77.4)
7(22.6)
24(77.4)
7(22.6)
28(90.3)
3(9.7)
0.127
Durationofsurgery(min) 90.3±36.3 77.1±34.6 71.2±21.5 0.054
Lengthofincision(cm) 6.9±1.5 6.8±1.6 7.4±1.6 0.295
Hospitalstay(day/med/min---max) 1(1---2) 1(1---2) 1(1---2) 0.424
I.O.fentanyl(mcg) 101.6±8.9 98.3±8.9 98.4±5.4 0.451
Surgerytype(n) 0.468
Inguinalhernia 21 21 21
Perf.appendectomy 5 4 4
Non-perf.appendectomy 5 6 6
C,control;B,bupivacaine;BD,bupivacaine+dexmedetomidine;ASA,AmericanSocietyofAnesthesiologists;BMI,bodymassindex;I.O., intraoperative;Perf,perfore.
Aa Aa
Aa Aa Aa Aab Aab Aab a
0 10 20 30 40 50 60 70 80 90
PO24 PO12 PO6 PO2 PO0 ATB60 Basale ATB10 ATB30 ATB45
Gropu C HR Group B HR Group BD HR
Figure 1 Heart rate (HR) (beats/min). Data are given as
median (min---max) or mean (SD). ATB, after TAP block;
PO, postoperative; C, control; B, bupivacaine; BD,
bupiva-caine+dexmedetomidine.(a)SignificantdifferencefromGroup
C;(b)significantdifferencefromGroupB;(A)significant
differ-enceinthegroupcomparedtobaselinevalues.
60thminutesoftheoperation,andinthepostoperative6th hourinGroupBD;andinthe12thhourcomparingwithGroup B(p>0.05)(Fig.2).
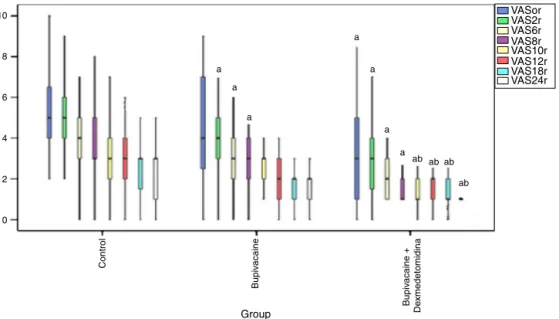
WhileastatisticallysignificantdecreaseinVASscorewas observedonly inGroup BDin comparisonwithGroup Cin post-operative 0min, the decrease in both Group B and GroupBDinbetweenthepostoperative120thminandthe 8thhourwasstatisticallysignificant(p<0.05)(Fig.3).The decreaseinGroupBDinbetweenthe10thand24thh post-operativelywasstatisticallysignificantwhencomparedwith GroupsCandB(p<0.05)(Fig.3).
WhilethepostoperativemorphineconsumptioninGroup BDwaslowatalltimes
120
100
a
a a a a b
80
60
40
20
0
Group C Group B Group BD PO24 PO12 PO6 PO2 PO0 ATB60 Basale ATB10 ATB30 ATB45
Figure2 Meanbloodpressure(MBP)(mmHg).Dataaregiven as median (min---max) or mean (SD). ATB, after TAP block; PO, postoperative; C, control; B, bupivacaine; BD, bupiva-caine+dexmedetomidine.(a)Significantdifferencefromgroup C;(b)significantdifferencefromgroupB.
WhencomparedtoGroupsBandC,itwaslowerinGroup BthanGroupCinthe6th,12th,18thand24thh(p<0.001) (Table2).
There was no significant difference observed among groups in terms ofthe numberofpatients having nausea-vomiting scores, antiemetic requirement, or additional analgesicadministration(p>0.05)(Tables2and3).
10
a
a
a
a
a
a
a ab ab ab
ab
VASor VAS2r VAS6r VAS8r VAS10r VAS12r VAS18r VAS24r
Group 8
6
4
2
0
Control
Bupiv
acaine
Bupiv
acaine +
De
xmedetomidina
Figure3 PostoperativeVASrscores.(a)SignificantdifferencefromgroupC;(b)significantdifferencefromgroupB.VASr,Visuel AnalogScaleatRest.
Table2 Postoperativemorphineconsumption(mg)andadditionalanalgesicneed.Dataaregivenasmean(SD)ornumber.
GroupC(n=31) GroupB(n=31) GroupBD(n=31) p
Postoperativemorphineconsumption
Postop.120min 5.0±1.8 4.6±2.0 2.2±1.3a,b <0.001
Postop.6hour 12.3±4.8 9.9±4.1a 4.3±2.4a,b <0.001
Postop.12hour 19.1±6.6 13.5±4.8a 6.4±3.5a,b <0.001
Postop18hour 23.8±4.7 15.6±4.7a 7.2±3.7a,b <0.001
Postop.24hour 28.8±7.8 17.5±4.6a 8.2±3.9a,b <0.001
Additionalanalgesicneed(n)
0---2h 6 5 2 0.313
2---6h 7 3 4 0.441
6---12h 4 1 0 0.122
12---24h 1 0 1 1.000
C,control;B,bupivacaine;BD,bupivacaine+dexmedetomidine. a SignificantdifferencefromGroupC.
b SignificantdifferencefromGroupB.
Discussion
It has been stated that direct blockade of abdomi-nal area blocks by ilioinguinal and iliohypogastric nerve blocks with abdominal wall neural afferent nerves, TAP block administrationfollowing abdominal surgery, suchas inguinalherniorrhaphyandhysterectomy,provide appropri-atepostoperativepaincontrol.17---19 Inourstudy,TAPblock
administrationappliedafter anesthesiainduction reduced VASscorewhencomparedtothecontrolgroupandat the sametimereducedpostoperativemorphineconsumption.
Inordertoprovideeffectivepostoperativeanalgesiawith TAPblock,ingeneralitshouldbeadministeredsoon after inductionoftheblockandsoonbeforesurgicalincision.19,20
Bharti et al.21 administered TAP block at the end of the
operation in a study they carried out, and reported that it did not prolong timeto first analgesic request in com-parison with the control group; however, they reported
reducedtotalmorphine consumption in thepostoperative 2ndhourandthereafter.Nirajetal.2administeredunilateral
TAP block with 20mL 0.5% bupivacaine in open appen-dectomy. In the control group, the mean 24h morphine consumption was 50mg, compared to28mg in the group inwhichTAPblockwasadministered.Choetal.3 reported
Table3 Patientsatisfactionscores,patientswithnauseandvomittingepisodesandpatientsreceivingantiemetics.Dataare
givenasnumber(%).
GroupC(n=31) GroupB(n=31) GroupBD(n=31) p
Patientsatisfactionscores
Verydissatisfied 0(0) 1(3.2) 0(0)
Somewhatsatisfied 12(39.8) 4(12.9)a 0(0)a,b <0.001
Rathersatisfied 19(61.3) 18(58.1) 17(54.8)
Completelysatisfied 0(0) 8(25.8)a 14(45.1)a
Nauseaandvomiting
None 17(54.8) 22(71.0) 21(65.6)
Nausea 7(22.6) 3(9.7) 6(21.9) 0.129
Retching 6(19.4) 5(16.1) 4(12.5)
Vomiting 1(0.7) 1(0.7) 0(0)
Patientsreceivingantiemetics(n)
0---2h 7(22.6) 5(16.1) 5(16.1) 0.313
2---6h 5(16.1) 4(12.9) 4(12.9) 0.428
6---12h 3(9.7) 2(6.5) 1(3.2) 0.224
12---24h 0(0) 1(3.2) 0(0) 0.667
C,control;B,bupivacaine;BD,bupivacaine+dexmedetomidine. aSignificantdifferencefromGroupC.
b SignificantdifferencefromGroupB.
However,thisresultmaybeduetothelimitednumberof patients.
Erdo˘gan Arıetal.10 administeredTAP blockwith20mL
0.125% bupivacaine in open inguinal herniorrhaphy and administered0.25%bupivacaineattheendofsurgery,and foundthesamepostoperativemorphineconsumption.
However,theydidnotcompareitseffectwith0.5% bupi-vacaine.Salmanetal.19administeredTAPblockwith20mL
0.125%bupivacaineat theendof surgerytopatients with inguinalherniagiventospinalanesthesiaandfoundlower postoperative morphine consumption than in the control group.Inourstudy,weadministeredTAPblockwith20mL 0.5%bupivacaine,and24htotalmorphineconsumptionwas observedtobe60.7%lowerintheTAPblockgroupthanin thecontrolgroup.
TAPblockdurationislimitedtotheactiontimeof admin-istered local anesthesia. In several studies it has been statedthatadditionofdexmedetomidinetolocal anesthe-siaadministeredtocentralneuroaxialandperipheralblock prolonged the local anesthetic action time and reduced anestheticrequest.8,21,22 Agarwaletal.21 indicatedintheir
studythatanalgesiatimewasprolongedupto8hwhenthey added100gdexmedetomidine tobupivacaineina
supra-clavicularblock.Almarakbietal.8statedthatinastudyin
whichtheyaddeddexmedetomidinetobupivacaineinTAP blockinabdominalhysterectomy,thefirsttimetoanalgesic administration was significantly longer than in the group thatdexmedetomidine (470minand280min,respectively) and total 24h morphine consumption was significantly lowerinthisgroup(19mgand29mg,respectively).Inour study,we administeredTAPblock with20mL0.5% bupiva-caine and 100g dexmedetomidine+bupivacaine in open
appendectomyand open inguinal hernia surgery, and the 24h morphine consumption in the control group, bupi-vacaine group and bupivacaine+dexmedetomidine group was28.8mg, 17.5mg,and 8.2mg,respectively. Morphine
consumption in the2---24h periodin both groupsthat TAP administered was significantly lower than in the control group,however,lowermorphineconsumptionwasobserved in the bupivacaine+dexmedetomidine group in all 24h measuringperiods,includingthefirst2h, whencompared to both control and bupivacaine groups. In this regard, dexmedetomidine isconsideredtoinitiateblocktime ear-lierandtoprolongactiontime,therebyreducinganalgesic consumption. In general, VAS measurement is utilized in postoperativepainstudies.
Salmanetal.19foundthatpostoperative24hVASscores
in open inguinal hernia operationswere lowerin the TAP blockwith20mL0.25%bupivacainegroupthaninthe con-trolgroup.Choetal.3assessedpatientsadministeredwith
TAPblockwith20mL0.5%levobupivacaineinopen appen-dectomywithverbalnumericalratingscaleforpainatrest (VNRSr)andoncoughing(VNRSc),andstatedthatVNRSrwas 12handVNRScwaspostoperative3hlowerthanthecontrol group.Nirajetal.2showedthatinopenappendectomy,VAS
assessmentatrestandoncoughinginTAPblock administra-tionwith20mL0.5%bupivacainewaslowerinthe30thmin and 24h postoperativelywhencomparedwiththe control group.
In our VASi scoring studies, there was a significant decreaseinGroupBDin0---24hwhencomparedtothe con-trol group and in 10---24h when comparedto Group B. In theBDgroup,therewasadecreasein2---8hincomparison withthecontrolgroup.WhileinTAPblock,onlybupivacaine administrationprovidedthedecreaseinVASiscoresfor8h, addition of dexmedetomidine prolonged this effectup to 24h. The VASiscore waslowerinthe postoperative0min inthegroupwhichhaddexmedetomidineadded,anditwas considered that dexmedetomidine induces sensorial block onsetearlier,andincreasesblockefficiency.
Akınetal.22 administeredepiduralanalgesiawith
undergoing abdominal surgery. Patient satisfaction scores inthegroup towhich dexmedetomidinewasadministered were significantly higher than in the control group. Kaur etal.23foundnostatisticallysignificantdifferenceinpatient
satisfactionscoresinastudyinwhichtheyadded levobupi-vacainedexmedetomidineinsupraclavicularbrachialplexus block.Inourstudy,therewasasignificantincreasein sat-isfactionscoresin Group Bwhen comparedtothe control groupandinGroupBDwhencomparedtoboththecontrol groupandthebupivacainegroup.Inallgroups,rathet sat-isfiedrateinpatientsatisfactionscoresaresimilar,butin groupBandgroupBDsomewhatsatisfiedratewaslowerand completelysatisfiedratewashigher.So,ingroupBDpatient satisfactionratewashigher.
Inthisstudy,asignificantdecreasewasobservedinHR and MAP valuesrecorded after block, in comparisonwith pre-blockvaluesinGroupBandBD;howevertheeffectwas longerinGroupBD.
The decreaseobservedinhemodynamic datawas long-lasting,and it wasconsidered thatit might be itsrolein blockingresponsetostressfollowingreliefofpostoperative painwithdexmedetomidineeffect.Patientsdidnotrequire treatmentwithvasoactivedrugs.
Only two patients in Group BD had intra-operative atropinerequestduetobradycardia.
Whennausea-vomitingscoreswereassessedinthisstudy, there was no statistically significant difference among groups. Administration of bupivacaine and dexmedetomi-dineforTAPblockdidnotelevatenausea-vomitingscores. Almarakbietal.8indicatedthat50ofsamplesizeincluded
inthestudyandfirstdegreenauseawasobservedin3 sam-plesfromthegroupinwhichdexmedetomidine wasadded tobupivacaineinTAPblock,and11samplesfromthegroup givenbupivacaine,andtherewasnostatisticallysignificant differenceamongsamplesintermsofnausea-vomitingand antiemetictreatment.
As a result, addition of bupivacaine and bupivacaine dexmedetomidine to TAP block following lower abdomen surgeryleadstoadecreaseinHRandMAPnormalclinical levelsofthecases.Addition ofbupivacaine dexmedetomi-dinereducedmorphinerequestsandVASscoresinthe24h postoperative period. Even though additionof only bupi-vacainereduced24hmorphineconsumptionincomparison withthecontrolgroup,itreducedVASscoreseffectivelyfor hours.
Ithasbeenfoundthatpostoperativepatientsatisfaction scoresinthegroupinwhichbupivacainedexmedetomidine wasaddedwashigherthanintheothertwogroups.
Funding
ThisresearchwassupportedbyErciyesUniversityBAPUnit.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
ThisworkwassupportedbyErciyesUniversityBAPFunding.
References
1.Petersen PL,MathiesenO,StjernholmP,etal. Theeffectof transversusabdominisplaneblockorlocalanaesthetic infiltra-tionininguinalherniarepair:arandomisedclinicaltrial.EurJ Anaesthesiol.2013;30:415---21.
2.Niraj G, Searle A, Mathews M, et al. Analgesic efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing open appendicectomy. Br J Anaesth. 2009;103:601---5.
3.ChoS,KimYJ,KimDY,etal.Postoperativeanalgesiceffectsof ultrasound-guidedtransversusabdominisplaneblockforopen appendectomy.JKoreanSurgSoc.2013;85:128---33.
4.AlfieriS,AmidPK,CampanelliG,etal.Internationalguidelines forpreventionandmanagementofpost-operativechronicpain followinginguinalherniasurgery.Hernia.2011;15:239---49. 5.GanaiS,LeeKF,MerrillA,etal.Adverseoutcomesofgeriatric
patientsundergoingabdominalsurgerywhoareathighriskfor delirium.ArchSurg.2007;142:1072---8.
6.Bay-NielsenM,PerkinsFM,KehletH.DanishHerniaDatabase. Painandfunctionalimpairment1yearafteringuinal herniorrha-phy:anationwidequestionnairestudy.AnnSurg.2001;233:1---7. 7.Elahi F, Reddy C,Ho D. Ultrasound guided peripheral nerve stimulationimplantformanagementofintractablepainafter inguinalherniorrhaphy.PainPhysician.2015;18:E31---8. 8.Almarakbi WA, Kaki AM. Addition of dexmedetomidine to
bupivacaine in transversus abdominis plane block potenti-atespost-operativepainreliefamongabdominalhysterectomy patients: a prospective randomized controlled trial. SaudiJ Anaesth.2014;8:161---6.
9.NirajG,KelkarA,HartE,etal.Comparisonofanalgesic effi-cacyoffour-quadranttransversusabdominisplane(TAP)block and continuous posterior TAP analgesia with epidural anal-gesia inpatientsundergoing laparoscopiccolorectal surgery: anopen-label,randomised,non-inferioritytrial.Anaesthesia. 2014;69:348---55.
10.Erdo˘ganArıD,YıldırımArA, Karado˘ganF,et al. Ultrasound-guidedtransversusabdominisplaneblockinpatientsundergoing openinguinalherniarepair:0.125%bupivacaineprovidessimilar analgesiceffectcomparedto0.25%bupivacaine.JClinAnesth. 2016;28:41---6.
11.MiloneM,DiMinnoMN, MusellaM,etal.Outpatientinguinal herniarepairunderlocalanaesthesia:feasibilityandefficacyof ultrasound-guidedtransversusabdominisplaneblock.Hernia. 2013;17:749---55.
12.HeilJW,IlfeldBM,LolandVJ,etal.Ultrasound-guided transver-sus abdominis plane catheters and ambulatory perineural infusionsforoutpatientinguinalherniarepair.RegAnesthPain Med.2010;35:556---8.
13.AmmarAS,MahmoudKM.Effectofaddingdexamethasoneto bupivacaineontransversusabdominisplaneblockforabdominal hysterectomy:aprospectiverandomizedcontrolledtrial.Saudi JAnaesth.2012;6:229---33.
14.CoursinDB, CoursinDB,Maccioli GA.Dexmedetomidine.Curr OpinCritCare.2001;7:221---6.
15.Brummett CM, Norat MA, Palmisano JM, et al. Perineural administrationofdexmedetomidineincombinationwith bupi-vacaineenhancessensoryandmotorblockadeinsciaticnerve block without inducing neurotoxicity in rat. Anesthesiology. 2008;109:502---11.
16.ComezM,CelikM,DostbilA,etal.Theeffectofpre-emptive intravenous dexketoprofen+thoracal epidural analgesia on the chronic post-thoracotomy pain. Int J Clin Exp Med. 2015;8:8101---7.
18.CarneyJ,McDonnellJG,OchanaA,etal.Thetransversus abdo-minis planeblockprovides effective postoperative analgesia inpatientsundergoing totalabdominalhysterectomy. Anesth Analg.2008;107:2056---60.
19.Salman AE, Yetis¸ir F, Yürekli B, et al. The efficacy of the semi-blindapproach oftransversusabdominisplaneblockon postoperativeanalgesiainpatientsundergoinginguinalhernia repair:aprospectiverandomizeddouble-blindstudy.LocalReg Anesth.2013;6:1---7.
20.McDonnell JG, O’Donnell B, Curley G, et al. The analgesic efficacy of transversus abdominis planeblock after abdomi-nalsurgery:aprospectiverandomizedcontrolledtrial.Anesth Analg.2007;104:193---7.
21.BhartiN,KumarP,BalaI,etal.Theefficacyofanovelapproach totransversusabdominisplaneblockforpostoperative analge-siaaftercolorectalsurgery.AnesthAnalg.2011;112:1504---8. 22.AkinS,AriboganA,ArslanG.Dexmedetomidineasanadjunctto
epiduralanalgesiaafterabdominalsurgeryinelderlyintensive carepatients:aprospective,double-blind,clinicaltrial.Curr TherRes.2008;69:16---28.