REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
REVIEW
ARTICLE
Medication
errors
in
anesthesia:
unacceptable
or
unavoidable?
Ira
Dhawan
a,∗,
Anurag
Tewari
b,
Sankalp
Sehgal
c,
Ashish
Chandra
Sinha
daDepartmentofAnesthesia,PGIMER,Chandigarh,India
bCincinnatiChildren’sHospitalandMedicalCenter,Cincinnati,OH,USA
cDrexelUniversityCollegeofMedicine,HahnemannUniversityHospital,DepartmentofAnesthesiologyandPerioperative
Medicine,Philadelphia,PA,USA
dDrexelUniversityCollegeofMedicine,AnesthesiologyandPerioperativeMedicine,Philadelphia,PA,USA
Received23August2015;accepted28September2015 Availableonline16May2016
KEYWORDS
Medicalerrors; Patientsafety; Drugerrors;
Qualityimprovement
Abstract Medicationerrorsarethecommoncausesofpatientmorbidityandmortality.Itadds
financialburdentotheinstitutionaswell.Thoughtheimpactvariesfromnoharmtoserious adverseeffectsincludingdeath,itneedsattentiononprioritybasissincemedicationerrors’are preventable.Intoday’sworldwherepeopleareawareandmedicalclaimsareonthehike,itis ofutmostprioritythatwecurbthisissue.Individualefforttodecreasemedicationerroralone mightnotbesuccessful untilachange intheexistingprotocolsandsystemisincorporated. Often drug errorsthatoccur cannotbereversed. Thebest way to‘treat’ drug errorsisto preventthem.Wrongmedication(duetosyringeswap),overdose(duetomisunderstandingor preconceptionofthedose,pumpmisuseanddilutionerror),incorrectadministrationroute, underdosingandomissionarecommoncausesofmedicationerrorthatoccurperioperatively. Drugomissionandcalculationmistakesoccur commonlyinICU.Medicationerrorscanoccur perioperativelyeitherduringpreparation,administrationorrecordkeeping.Numeroushuman andsystemerrorscanbeblamedforoccurrenceofmedicationerrors.Theneedofthehouristo stoptheblame---game,acceptmistakesanddevelopasafeand‘just’cultureinordertoprevent medicationerrors.ThenewlydevisedsystemslikeVEINROM,afluiddeliverysystemisanovel approach inpreventing drug errorsdueto mostcommonlyused medicationsinanesthesia. Similardevelopments alongwithvigilant doctors,safeworkplacecultureandorganizational supportalltogethercanhelppreventtheseerrors.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeAnestesiologia. Thisisanopenaccess articleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](I.Dhawan).
http://dx.doi.org/10.1016/j.bjane.2015.09.006
PALAVRAS-CHAVE
Errosmédicos; Seguranc¸ado paciente; Errosde medicamentos; Melhoradaqualidade
Errosdemedicac¸ãoemanestesia:inaceitávelouinevitável?
Resumo Oserrosdemedicac¸ãosãoascausasmaiscomunsdemorbidadeemortalidadedos
pacientes. Alémdisso, esseserrosaumentamosencargosfinanceirosdainstituic¸ão. Embora oimpactovariedenenhumdanoaefeitosadversosgraves,incluindooóbito,éprecisoestar atentoàordemdeprioridadesporqueoserrosdemedicac¸ãosãoevitáveis.Naatualidade,com aspessoascienteseos processosmédicos emevidência,frear esseproblemaédeextrema prioridade.Oesforc¸oindividualparadiminuiroserrosdemedicac¸ãopodenãoobtersucesso atéqueumamudanc¸anosprotocolosesistemasexistentessejaincorporada.Muitasvezes,os errosdemedicac¸ãoocorridosnãopodemserrevertidos.Amelhormaneirade‘‘tratar’’esses erroséimpedi-los.Oserrosdemedicac¸ão(devidoàtrocadeseringa),deoverdose(devido amal-entendidooupreconcepc¸ãodadose,malusodebombaeerrodediluic¸ão),deviade administrac¸ãoincorreta,desubdosagemedeomissãosãocausascomunsdeerrodemedicac¸ão queocorremnoperíodoperioperatório.Aomissãoeerrosnocálculodemedicamentosocorrem comumenteemUTI.Oserrosdemedicac¸ãopodemocorrernoperíodoperioperatório,tanto duranteapreparac¸ãoeadministrac¸ãoquantonamanutenc¸ãoderegistros.Umgrandenúmero deerroshumanosedosistemapodeserresponsabilizadopelaocorrênciadeerrosdemedicac¸ão. Anecessidadedomomentoépararojogodaculpa,aceitaroserrosedesenvolverumacultura segurae‘‘justa’’paraevitaroserrosdemedicac¸ão.Ossistemasrecém-criadoscomoo VEIN-ROM,umsistemadeadministrac¸ãodelíquidos,éumanovaabordagemnaprevenc¸ãodeerrosde medicac¸ãodevidoaosmedicamentosmaiscomumenteusadosemanestesia.Desenvolvimentos semelhantes,juntamentecommédicosvigilantes,umaculturadelocaldetrabalhoseguroe apoioorganizacional,todosemconjuntopodemajudaraevitaresseserros.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradeAnestesiologia. Este ´eum artigo Open Access sob umalicenc¸a CC BY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
‘‘Toerrishuman’’
Ananesthesiologistmayinjectuptohalfamilliondifferent drugs in his/her professionaltenure. The chance of mak-inganinadvertenterroriseasilyfathomable.Anesthetized patientswithunpredictablephysiologicalreserveswouldnot display or verbalize any symptoms that an awake patient would,suchashypotension,bronchospasm,arrhythmiasor cardiacarrest.Anysucherrormaycauseirreversible dam-age/s.Whenpatientsconsentforanesthesia,theytrustthat ourtrainingis adequate, judgmentisuncompromised and competencevalidated.Itisthisresponsibilityforwhichwe standaccountable.
Medicationerrorssignificantlyaugmentthefinancialcost tohumantragedy.Batesetal.1foundthatabouttwooutof
every100in-patientsexperienceapreventableadversedrug event,resultinginanaverageincreaseofhospitalcostsby $4700peradmissionorabout$2.8millionannuallyfora700 bed hospital. Therefore medicalerrors should be priority asanurgent, critical,andwidespreadpublichealth prob-lem.Systemsneedtobeengineeredtoreducethelikelihood ofmedicationmisidentificationthroughapproachessuchas revisionofstandardsforlabelingofdrugampoulesandvials andthedevelopmentofadvancedelectronic/digital mech-anismsthatallow‘‘double-checking’’ordrugverificationin theoperatingroom.2
Morepeoplediefrommedicalerrorsthanmotorvehicle accidents, breast cancer, or HIV, but unfortunately these
statistics never appropriately figure in public media or deliberations.Afewhorrificcasesoferroneousdrug admin-istrationdomakethenewsheadlines,eitherbecausethey involveacelebrityorduetotheiregregiousnature. Unfor-tunately,theyconstitute only the tipof theiceberg. The objectiveofthisreviewistodiscusssafetywhile adminis-teringdrugstopatientsunderanesthesia.
Incidence
Withanaimtoestablishthefrequencyandnatureofdrug administrationin anesthesia, Websteretal.3 performed a
study based on 7794 anesthesiologist responses from two hospitals. They documented that the frequency of drug administrationerror(ofanytype)peranestheticcase was 0.0075(0.75%or1per133anesthetics)withthetwolargest categories of errors involving incorrect doses (20%) and substitutions (20%), hence concluding that ADE (adverse drug effects) during anesthesia is considerably more fre-quentthanpreviouslyreported.
Sakaguchi et al.4 studied the incidence of anesthesia
Table1 Incidenceofmedicationerrorsinkeystudies.
Study Studyperiod Numberofanesthetics
delivered
Incidenceof drugerror
Percentageof drugerror
Websteretal.3 Feb1998---Oct1999 10,806 81 0.75%
Sakaguchietal.4 1993---2007 64,285 50 0.078%
Llewellynetal.5 Jul2005---Jan2006 30,412 111 0.37%
Cooperetal.6 Aug2007---Feb2008 10,574 52 0.49%
Zhangetal.7 Mar2011---Sep2011 24,380 179 0.73%
InSouthAfrica,Llewellynetal.5 reportedanincidence
of0.37%(111incidencesfor30,412anestheticsor1per274) withaconclusionthatneithertheexperienceofthe anes-thetistnortheemergentnatureof thesurgeryinfluenced theincidenceandnearly40%ofallerrorsoccurreddueto misidentificationofdrugampoules.Nomajorcomplication attributabletoADE-adversedrugeffectswasreported.
Cooperetal.6 reportedamedication error rateduring
anesthesiaof0.49%(52errorsfrom10,574caseformsor1 per203anesthetics)andatwo-foldincreaseintheratesby anesthesia-in-training providers compared to experienced provider, most commonly due to incorrect dose and drug substitution.
Zhangetal.,7inaprospectiveincident-monitoringstudy
in China reported a medication error rate of 0.73% (179 errorsduring16,496anesthetics),thelargestcategorybeing omission, incorrect dosage and substitutions, collectively accountingfor more than 65% of all errors.These led to seriouscomplications in at least twoand inadvertent ICU admissions for five patients. The incidence of medication errorsfromtheabove mentioned studieshave been com-pliedinTable1.
Whencombiningthe3prospectivestudyfindingsof Web-steretal.,3Llewellynetal.,5andCooperetal.,6244errors
were reported in 51,504 administered anesthetics. That gaveusacombinedincidenceof1in211medicationerrors inanesthesiapractice.8
Based on a limited number of prospective studies, theestimatedincidenceof medicationerror inanesthetic practicerangesfrom0.33%to0.73%6,7percaseand
unfor-tunatelythisratehasnotchangedsubstantiallyoverthelast 15years.4
The CriticalCareSafetyStudyreportedan overallrate of 80.5 medication errorsassociated with harm per 1000 patient-daysinmedicalandcoronary-carepatients.9Inthe
SEE2study,therateofparenteralmedicationerrorswas745 per1000patient-days.10
InasystematicreviewbyWilmeretal.11 toassess
inci-denceofdrugeventsinintensivecareunits(ICUs),therates ofmedicationerrors(MEs)variedfrom8.1to2344per1000 patient-days,and adverse drug events(ADEs) from5.1 to 87.5per1000patient-days.ThedefinitionsofADEandMEin thestudiesvariedwidelywhichcouldhavebeenthecause ofthisvastvariationinincidence.
Historicalperspectiveofmedicationerrors
Look-alike,sound-alikedrugs,12,13 confusing,inaccurateor
incompletedruglabelsandpackaging,13swappingofsyringe
labels,14,15 swappingofsyringesandampoules,4unlabelled
syringes,16 andfailureof drug-dosecalculation,17 have all
beenreported.
Asystemfailure,thathadprofoundimplicationsfor anes-thesia in the United Kingdom, was the case of Woolley andRoe,in whichtwopatients wereleftparaplegicafter undergoingspinalanesthesiaatChesterfieldRoyalHospital in 1947.18 Atthat time,their injurieswere thoughttobe
duetomicroscopiccracksinthelocalanestheticampoules, through which phenol seemed to have seeped during the sterilization process. In fact, it appeared that a batch of reusablespinalneedleshadnotbeenremovedfromabath of acidicdescalerandboiled indistilledwaterbeforeuse becauseamemberofstaffhadcalled-insick,andwas off-duty,19aclassicsystemfailure.Afatalitywasreportedwhen
theflowrateofapatient’sepiduralpumpwasincreasedto 125mL/h by a‘ward nurse’who hadintended togivean intravenous fluid bolus, despite the pump being correctly labeled and the patient receiving parenteral fluids via a gravity-feddripset.20
High profile cases of fatalities caused by accidental injectionofintrathecal vincristinehaveresultedinblame, chargesandconvictionsfortheindividualsinvolvedrather than recognition that they result from system failures.21
Overdoseofanticoagulantsresultinginhemorrhage, admin-istrationofantibioticstopatientswithpreexistinghistoryof allergytosuchantibiotics,failuretoprescribeprophylaxis againstvenous thromboembolismandadversedrugevents withopioids,theophylline,antimicrobials,anticonvulsants, anticancerdrugsandmusclerelaxantsarewellknown.22---26
Drugsmostcommonlyinvolved inseriouserrorswere hep-arin, epinephrine, potassium chloride and lidocaine, the last being implicated in most fatalities.27 The accidental
injectionofintrathecal vincristineratherthan methotrex-ateduringchemotherapyforacutelymphoblasticleukemia hasdevastatingconsequencesandseemstohaveoccurred withdepressingregularity.28
Wrong medication wasthe most common type of drug error(48%)occurringperioperatively,followedbyoverdose (38%), incorrect administration route (8%), under dosing (4%) and omission (2%). Opioids, cardiac stimulants, and vasopressorswerethemostcommonculprits.Forty-two per-centofwrongmedicationadministrationoccurredfollowing syringeswap,Drugampouleswapoccurredin33%,andthe wrongchoiceofdrugwasmadein17%.Thefirst,second,and thirdmostfrequentcausesofoverdoseinvolveda misunder-standingorpreconceptionofthedose(53%),pumpmisuse (21%),anddilutionerror(5%).4
astudy byLatifetal.29 The mostcommonerrortypewas
omission(26%). Among harmful errors, dispensing devices (14%)andcalculationmistakes(9.8%)weremorecommonly identifiedtobethecauseintheICUcomparedtothenon-ICU setting.
Medico-legalconsequences
Medicalerrorscanhaveprofoundramificationsforpatients and families. Once the error has reached the patient, the medical provider, patient and their families are helpless. It adds significant cost to medical treatment, increasesmorbidity(disability)andmayevenleadto mor-tality.Employers,consumersandtaxpayersareincreasingly demanding that providers of medical care be held more accountable, particularlyas thecosts of health insurance continuetorise.Severalorganizationshavedevelopedand devotedexclusivelytoenhancepatientsafety.Hospitalsand doctorscanendupfootingupwardsofmilliondollar settle-mentsformedicalmalpracticecases.
It isachillingreality ---oneoften overlookedinannual mortality statistics: Preventable medicalerrors persist as then◦3‘killer’intheU.S.---precededonlybyheartdisease
andcancer---claimingthelivesofsome400,000peopleeach year.30
Ninety-three claims (with a total cost £4,915,450)
filed under ‘‘anesthesia’’ in the NHS Litigation Authority database between 1995 and 2007, alleging patient harm directlybydrugadministrationerrororbyanallergic reac-tion,wereanalyzed.Allegederrorswerecategorizedusing systemsemployedbytheNationalCoordinatingCouncilfor Medication Error Reporting and Prevention, the American Society ofAnesthesiologistsClosedClaimsProjectandthe UKHealthandSafetyExecutive.Theseverityofoutcomein eachclaimwascategorizedusingadaptedNationalPatient SafetyAgencydefinitions.Sixty-twoclaimsinvolvedalleged drug administration errors(total cost £4,283,677) and 15
resultedin severeharmordeath. Halfallegedthe admin-istrationofthe wrongdrug,in most(16) aneuromuscular blocker. Of the claims alleging the wrong dose had been given(25),nineallegedopioidoverdoseincludingby neurax-ialroutes.Themostfrequentlyrecordedadverseoutcomes were ‘awake-paralysis’ (19 claims; total cost £182,347)
and respiratory depression requiring intensive care treat-ment(13claims;totalcost£2,752,853). Thirty-oneclaims
involved allergicreactions (total cost631,773 pounds). In 20 claims,the patientallegedly receiveda drugtowhich theywere known tobe allergic (totalcost £130,794). All
claimsinwhichitwaspossibletocategorizethenatureof theerrorinvolved‘humanerror’.Fewerthanhalftheclaims appearedlikelytohavebeenpreventablebyan‘‘ideal dou-blecheckingprocess’’.31
Definition
Many investigators have adopted James Reason’s classifi-cation from 1990, which draws widely from the aviation and nuclear industries as well as medicine32 in which he
classifiederrorsas‘‘slips’’,‘‘lapses’’and‘‘mistakes’’.‘‘A slip results from a failure in the execution of an action, whetherornottheplanbehinditwasadequatetoreachits
objective’’.32 Slips are said to be skill-based, occurring
duringtheexecutionofsmooth,automatedandhighly inte-gratedtasksthatdonotrequireconsciouscontrolorproblem solving.33 Forexample, writing the ‘‘year’’ incorrectly in
thedateshortlyafteranewyearisaslip.21‘‘Lapsesinvolve
memoryfailure,and may onlybe apparent tothe person whoexperiencesthem’’,32 an examplebeingforgettingto
administerantibioticprophylaxis priortotourniquet infla-tion.Slipsandlapsesoccurwhenactionsdonotgoasper theplan,mistakeshappenwhenaplanprovesinsufficient. Theoperatoriscognizantoftheproblemandbeginstouse rulesorknowledgetosolveit.‘‘Amistakeislikelytooccur when knowledge or rules are lacking’’.32 For example an
anesthesiologistwascondemnedofmanslaughterafter fail-ingtoidentifyadisconnectedtrachealtubeforaprolonged period,untilthepatientexperiencedacardiac arrestand unfortunatelyperished.21,34
Whatisamedicationerror?
The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) defines medica-tion error as ‘‘A medication error is any preventable event that may cause or lead to inappropriate medica-tion use or patient harm while the medication is in the control of the health care professional, patient or con-sumer.Sucheventsmayberelatedtoprofessionalpractice, health care products, procedures, and systems, includ-ing prescribing; order communication; product labeling, packaging, and nomenclature; compounding; dispensing; distribution; administration; education; monitoring; and use’’. The Council urges medication errors researchers, softwaredevelopers, andinstitutionstouse this standard definitiontoidentifyerrors.
Classification
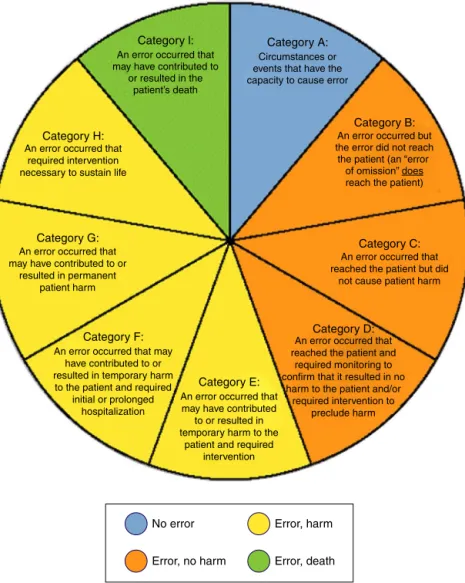
Moyenetal.35 compiledafewdefinitionsintheyear2008
(Table 2).On July16th,1996, NCCMERPadopted a Medi-cationErrorIndexthatclassifiesanerroraccording tothe severity of the outcome (later revised in Feb 20, 2001). The index considers factors such as whether the error reached the patient and, if the patient was harmed, to whatdegree(Fig.1).Wehavesimplifiedandgivena prac-ticalclassificationofmedicationerrorsduringanesthesiain
Table3.Medicationerrorscanoccureitherduring prepara-tion,administrationorrecordkeeping.
Genesis
of
error
TheGenericErrorModelingSystemdistinguishesfailuresin decisionmaking(mistakes)fromfailuresin the implemen-tationofdecisions(actionfailures).32Actionfailures,often
madeunconsciously,aretypicallyslipsorlapses.Thalerand Sunsteinhave presented a viewthat placesless emphasis onthedistinctionbetweenactionsanddecisions,andmore emphasisonthedegreetowhich theunderlyingcognitive processesareautomatic orconscious.36 Inthis view,
Table2 DefinitionscompiledbyMoyenetal.35in2008.
Nearmiss Theoccurrenceofanerrorthatdidnot resultinharm.
Slip Afailuretoexecuteanactiondueto routinebehaviorbeingmisdirected Lapse Afailuretoexecuteanactiondueto
lapseinmemoryandaroutinebehavior beingomitted.
Medicalerror Thefailureofaplannedactiontobe completedasintendedortheuseofa wrongplantoachieveanaim. Medication
error
Anyerrorinthemedicationprocess, whetherthereareanyadverse consequencesornot.
Adversedrug event(ADE)
Anyinjuryrelatedtotheuseofadrug. Notalladversedrugeventsarecaused bymedicalerrororviceversa. Preventable
ADE
Harmthatcouldhavebeenavoided throughreasonableplanningorproper executionofanaction.
errormay,ironically,havetheoppositeeffect. Taken col-lectively,akeymessageofthissubstantialbodyofresearch isthatsimplytryinghardertoavoiderrorsisunlikelytobe successfulonitsown:itisalsonecessarytomakeprocesses andsystemssafer.38
Cooperandcolleagues6haveidentifiedseveralrisk
fac-tors in a critical incident analysis to study preventable mistakes. Maximum errorswere due toeither inadequate experience(16%)orduetoinadequatefamiliarityto equip-ment or device (9.3%) whereas haste and inattention or carelessness, each amounted to 5.6% of errors during anesthesia.39 Inthe parallelworldof aviation,specifically
ontheflightdeck;withverysimilarsafetyanderrorissues, these sametrends are reflected.The top three causes in both environments are identical; unfamiliarity with situ-ation, unfamiliarity withequipment and failure tofollow yourownprescribedsafetyprotocols(pre-flightcheckversus machinecheck).
Variousotherfactorsexistinoperatingroomsgivingrise toahighincidenceofmedicationerrorsduringthe conduc-tionofanesthesia.Lackofstaff,overtimeandoddworking hours,inattention,poorcommunication,carelessness,haste
Category l: Category A:
Category B:
Category C:
Category D:
Category E: Category F:
No error
Error, no harm
Error, harm
Error, death Category G:
Category H: An error occurred that
required intervention necessary to sustain life
An error occurred that may have contributed
to or resulted in temporary harm to the
patient and required intervention An error occurred that may
have contributed to or resulted in temporary harm
to the patient and required initial or prolonged
hospitalization An error occurred that may have contributed to or
resulted in permanent patient harm
An error occurred that reached the patient but did
not cause patient harm
An error occurred that reached the patient and
required monitoring to confirm that it resulted in no
harm to the patient and/or required intervention to
preclude harm Circumstances or events that have the capacity to cause error
An error occurred but the error did not reach the patient (an “error
of omission” does reach the patient) An error occurred that
may have contributed to or resulted in the
patient’s death
Table3 Practicalclassificationofmedicationerrorsduring anesthesia.
Errorsduring Errorsobserved
Preparationof thedrug
Similarlookingvials/ampoulesplaced together(misidentificationof ampoules)
Unlabeledsyringes
Notcheckingthelabel(including expirydate)priortoadministration Differentconcentrationinthesyringe andincorrectlabel.(Incorrect dilutionsesp.relevantinpediatric patients).
Administration ofthedrug
Nearmisses.
Wrongpatientidentification. Incorrectdose(inadequateorin excess)esp.inpediatricpatients. Differentpersonnelforpreparation andadministrationofdrug. Syringeswap.
Wrongrouteofadministration. Incorrecttimingofadministration. Omission,repetitionorsubstitution ofdrug.
Recordingof thedrug delivered
Adverseeventnotrecognized. Reluctanceamongstdoctorstoadmit theerror.
Failuretoreportanerrorduring medication.
andfatiguearethecommonfactorsrelatedtomedicaland paramedicalpersonnel.19,40---45Causesofmedication
admin-istrationerrorsaretabulatedasunsafeacts,localworkplace cultureandorganizationaldecisionsinTable4.46
Table 4 Causes of medication administration errors in
hospitals.46
Category Causes
Unsafeacts Slipsandlapses
Rule/knowledgebasedmistakes Violations
Others Local
workplace factors
Patient
Policiesandprocedures Wardbasedequipment Healthandpersonality Trainingandexperience Communication
Interruptionanddistraction Workloadandskillmix Generalworkenvironment Medicinesandsupplystorage Localworkingculture
Supervisionandsocialdynamics Organizational
decisions
Highlevel/strategicdecisions.
Possiblemanagementoferroneousdrug administration
Trainingofanesthesiologistsbeginswithpreparation, label-ingandarrangingdrugs beforestart ofacase. Errorsmay occur due to multiple reasons; lack of experience, low vigilance (especially during maintenance of anesthesia), inappropriatelabeling/identification/selection or stressful operation theater milieu. Medication errors by anesthesi-ologists in operation theater or intensive care units can unfortunatelybefatal.Sincetheseerrorsarepreventable and potentially lethal, every attempt should be made to reducetheseerrorsinordertoprovidesafeanesthesia.
Oftendrugerrorsthatoccurcannotbereversed.Thebest wayto‘treat’drugerrorsistopreventthem.Morethanhalf
Table5 RecommendationsbyJensenetal.48
1 Thelabelonanydrugampouleorsyringeshould becarefullyreadbeforeadrugisdrawnupor injected.
2 Legibilityandcontentsoflabelsonampoulesand syringesshouldbeoptimizedaccordingtoagreed standardsinrespectofsomeoralloffont,size, colorandtheinformationincluded(NB,there maybesomedisagreementonthedetailofhow thisshouldbeachieved).
3 Syringesshouldbelabeled(alwaysoralmost always).
4 Formalorganizationofdrugdrawersand workspaceshouldbeusedwithattentionto: tidiness;positionofampoulesandsyringes; separationofsimilarordangerousdrugs;removal ofdangerousdrugsfromtheoperatingtheaters. 5 Labelsshouldbecheckedspecificallywitha
secondpersonoradevice(suchasabarcode readerlinkedtoacomputer)beforeadrugis drawnuporadministered.
6 Errorsinintravenousdrugadministrationduring anesthesiashouldbereportedandreviewed. 7 Managementofinventoryshouldfocuson
minimizingtheriskofdrugerror(e.g.;adrug safetyofficerand/orapharmacistshouldbe appointedfortheoperatingtheatersandany changesinpresentationshouldbenotifiedahead oftime).
8 Similarpackagingandpresentationofdrugs contributetoerrorandshouldbeavoidedwhere possible.
9 Drugsshouldbepresentedinprefilledsyringes (wherepossible)ratherthanampoules(eitherfor emergencydrugsoringeneral).
10 Drugsshouldbedrawnupandlabeledbythe anesthetistwhowilladministerthem. 11 Colorcodingbyclassofdrugaccordingtoan
agreednationalorinternationalstandardshould beused---ofthesyringe,partofthesyringe,orof thesyringeorampoulelabels.
Table6 BriefdescriptionofsimilaritiesanddifferencesbetweenISO26825:2008andtheLabelingrecommendations.46
ISO26825:2008(or relatedstandards)
Labelingrecommendations
Clinicalsituationswhere labelsshouldbeusedin anestheticpractice
Onsyringescontaining medicationsusedduring anesthesia
Allothermedicationsandallcontainersandlines preparedoradministeredbyanesthesiologists, including:
Infusions
Injectionsforuseonthesterilefield
Medicationsinsyringesthatwillaccompanypatients tootherclinicalareas
Linesandcatheters Informationrequired Pre-printedgeneric
nameofmedication
Dependsonlabeltype.Forbags,bottlesandsyringes labelinclusionsareasfollows:
Concentrationofsyringe contents
Patientname(givennameandfamilyname) PatientIdentifier(ID)
Activeingredient/s(medicine/s)addedtothebagor syringe
Amountofmedicine/sadded(includingunits) Volumeoffluid(mL)---totalinbag,orsyringe Concentration(units/mL)
Diluent(forsyringes) Dateandtimeprepared Preparedby(signature) Checkedby(signature)
Routeofadministration(wherenotspecifiedby wordingandcolor)
Colorcodingand borderindicativeof medicationclass
Routeofadministration
Table7 APSFconsensusrecommendationsforimprovingmedicationsafetyintheoperatingroom.49
Standardization High-alertdrugs(suchasphenylephrineandepinephrine)shouldbeavailablein standardizedconcentrations/diluentspreparedbypharmacyinaready-touseform thatisappropriateforbothadultandpediatricpatients.Infusionsshouldbe deliveredbyanelectronicallycontrolledsmartdevicecontainingadruglibrary. Ready-to-usesyringesandinfusionsshouldhavestandardizedfullycompliant machine-readablelabels.
Technology Everyanesthetizinglocationshouldhaveamechanismtoidentifymedicationsbefore drawinguporadministeringthem(barcodereader)andamechanismtoprovide feedback,decisionsupport,anddocumentation(automatedinformationsystem). Additionalideas.
Pharmacy/prefilled/premixed Routineprovider-preparedmedicationsshouldbediscontinuedwheneverpossible. Clinicalpharmacistsshouldbepartoftheperioperative/operatingroomteam. Standardizedpre-preparedmedicationkitsbycasetypeshouldbeusedwhenever possible.
Culture Establisha‘‘justculture’’forreportingerrors(includingnearmisses)anddiscussion oflessonslearned.
Establishacultureofeducation,understanding,andaccountabilityviacurriculum andCME.
EstablishacultureofcooperationandrecognitionofthebenefitsofSTPCwithinand betweeninstitutions,professionalorganizations,andaccreditationagencies.
APSF,AnesthesiaPatientSafetyFoundation.
of surveyed people believed that suspendingdoctors who have committed clinical errors is an effective prevention strategy.47 Therearevariousevidence-based
recommenda-tionsofwhichafewarequotedinTables5---7.46,48,49
orvialat thetimeofdrawingupanymedication.Alllines andcathetersshouldbelabeled.Anymedicineorfluidthat cannotbeidentified(e.g.,inanunlabelledsyringeorother container)shouldbeconsideredunsafeanddiscarded.37
Intheeraofroboticandmoreadvancedsurgeries,itis timethat anesthesiology advances in engineering thereby enhancingsafepatientcare. Theenvisionedfluiddelivery system, namedVEINROMdistinguishes thefactthat prime causeofEDA is theadaptationof theuniversalLeur lock-ing mechanism to all prevalent intravenous drug delivery systems. Presently all kinds of syringe ports on the fluid deliverysystemareabletointerlockwithanysyringenozzle bynatureoftheinherentLeurdesign,thuspredisposingan adverseeventtooccur.VEINROMproposesonesyringeport foreachofthesevenmostcommondrugcategoriesusedin anesthesiologyandcriticalcare.50
Conclusion
Allmedicalerrorsdonot causeharm.Noanesthesiologist intentionallyexecutesamistake,buterrorsareunforgiving asthey can costa human life. In an erawhere patients’ knowledge and awareness about diseases and their man-agement isincreasing,clinicians need tobe morevigilant toavoidunfortunateoutcomesandmedico-legalclaims.All effortsshouldbemadeinreportingandpreventionof medi-caldrugerrors.
Current safety protocols in intravenous drug delivery havenotchangedoverthepast60years.Wethinkitistime toincorporateelectronicanddigitalconceptstoencourage evolutionofanesthesia-relateddrugdeliverysystem.
Weinferthat‘‘toerrmaybehuman,butinhealthcare, toerrrepeatedlyisfoolishandperhapscriminal’’.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BatesDW,SpellN,CullenDJ,etal.Thecostsofadversedrug eventsinhospitalizedpatients.JAMA.1997;277:307---11.
2.OrserBA,HylandS,DavidU,etal.Reviewarticle:improving drugsafetyforpatientsundergoinganesthesiaandsurgery.Can JAnesth.2013;60:127---35.
3.WebsterCS,MerryAF,LarssonL,etal.Thefrequencyandnature ofdrugadministrationerrorduringanaesthesia.Anaesth Inten-siveCare.2001;29:494---500.
4.Sakaguchi Y, Tokuda K, Yamaguchi K, et al. Incidence of anesthesia-relatedmedicationerrorsovera15-yearperiodina universityhospital.FukuokaIgakuZasshi.2008;99:58---66.
5.LlewellynRL, GordonPC, WheatcroftD,et al.Drug adminis-trationerrors:aprospectivesurveyfrom threeSouthAfrican teachinghospitals.AnaesthIntensiveCare.2009;37:93---8.
6.CooperL,DiGiovanniN,SchultzL,etal.Influencesobservedon incidenceandreportingofmedicationerrorsinanesthesia.Can JAnesth.2012;59:562---70.
7.ZhangY,DongYJ,WebsterCS,etal.Thefrequencyandnature ofdrugadministrationerror duringanaesthesiaina Chinese hospital.ActaAnaesthesiolScand.2013;57:158---64.
8.Cooper L, Nossaman B. Medication errors in anesthesia: a review.IntAnesthesiolClin.2013;51:1---12.
9.Rothschild JM, Landrigan CP, Cronin JW, et al. The Critical CareSafetyStudy:theincidenceandnatureofadverseevents and serious medical errorsinintensive care.Crit CareMed. 2005;33:1694---700.
10.ValentinA,CapuzzoM,GuidetB,etal. Errorsin administra-tionofparenteraldrugsinintensivecareunits:multinational prospectivestudy.BMJ.2009;338:b814.
11.Wilmer A, Louie K, Dodek P, et al. Incidence of
med-ication errors and adverse drug events in the ICU: a
systematic review. Qual Saf Health Care. 2010;19:e7,
http://dx.doi.org/10.1136/qshc.2008.030783.
12.OrserB.Reducingmedicationerror.CMAJ.2000;162:1150---1.
13.Skegg PD. Criminal prosecutions of negligent health profes-sionals the New Zealand experience. Med Law Rev. 1998;6: 220---46.
14.Fasting S, Gisvold SE. Adverse drug errors in anaesthesia and the impact of coloured syringe labels. Can J Anesth. 2000;47:1060---7.
15.Perri M, Morris S. Critical incident involving syringe labels. Anaesthesia.2007;62:95---6.
16.Stabile M, WebsterCS, Merry AF. Medication administration in anaesthesia. Time for a paradigm shift. APSF Newslett. 2007;22:44---7.
17.Orser BA, Chen RJ, Yee DA. Medication errors in anaes-theticpractice, asurvey of687practitioners.Can JAnesth. 2001;48:139---46.
18.CopeRW.TheWoolleyandRoecase;Woolleyand Roeversus MinistryofHealthandothers.Anaesthesia.1954;9:249---70.
19.MaltbyJR,HutterCD,ClaytonKC.TheWoolleyandRoecase. BrJAnaesth.2000;84:121---6.
20.Sayers P. Fatal epidural infusion. Anaesth Intensive Care. 2000;28:112.
21.Ferner RE. Medication errorsthat have led to manslaughter charges.BrMedJ.2000;321:1212---6.
22.CurrieM,MackayP,MorganC,etal. TheAustralianIncident Monitoring Study. The ‘wrong drug’ problem in anaesthesia: ananalysisof2000incidentreports.Anaesth IntensiveCare. 1993;21:596---601.
23.Lesar TS, BricelandL, Stein DS. Factors relatedto errorsin medicationprescribing.JAMA.1997;277:312---7.
24.BordunLA, ButtW. Drugerrorsinintensive-care. J Paediatr ChildHealth.1992;28:309---11.
25.KanjanaratP,WintersteinAG,JohnsTE,etal.Natureof pre-ventableadversedrugeventsinhospitals:aliteraturereview. AmJHealthSystPharm.2003;60:1750---9.
26.RossLM,WallaceJ,PatonJY.Medicationerrorsinapaediatric teachinghospitalintheUK:fiveyearsoperationalexperience. ArchDisChild.2000;83:492---6.
27.Edgar TA, Lee DS, Cousins DD. Experience with a national medication error reporting program. Am J Hosp Pharm. 1994;51:1335---8.
28.FernandezCV,EsauR,HamiltonD,etal.Intrathecalvincristine, an analysis of reasons for recurrent fatal chemotherapeutic errorwithrecommendationsforprevention.JPediatrHematol Oncol.1998;20:587---90.
29.LatifA,RawatN,PustavoitauA,etal.Nationalstudyonthe distribution,causes,andconsequencesofvoluntarilyreported medicationerrorsbetweentheICUandnon-ICUsettings.Crit CareMed.2013;41:389---98.
30.JamesJTA.Newevidence-basedestimateofpatientharms asso-ciatedwithhospitalcare.JPatientSaf.2013;9:122---8.
31.CranshawJ,GuptaKJ,CookTM.Litigationrelatedtodrugerrors inanaesthesia:ananalysisofclaimsagainsttheNHSinEngland 1995---2007.Anaesthesia.2009;64:1317---23.
32.ReasonJ.Humanerror.Cambridge:CambridgeUniversityPress; 1990.
34.Regina respondent and Adornako appellant. House of lords appealcases,vol.1;1995.p.171---90.
35.Moyen E, Camire E, Stelfox HT. Clinical review: medication errorsincriticalcare.CritCare.2008;12:208.
36.ThalerR,SunsteinC.Nudge:improvingdecisionsabouthealth, wealthandhappiness.NewHavenYaleUniversityPress;2008.
37.WegnerDM. Ironic processesof mentalcontrol.Psychol Rev. 1994;101:34---52.
38.MerryAF,ShippDH,LowingerJS.Thecontributionoflabelling tosafemedicationadministrationinanaestheticpractice.Best PractResClinAnaesthesiol.2011;25:145---59.
39.KothariD,GuptaS,SharmaC,etal.Medicationerrorin anaes-thesiaandcriticalcare:acauseforconcern.IndianJAnaesth. 2010;54:187---92.
40.CooperJB,NewbowerRS,LongCD,etal.Preventable anaes-thesia mishaps: a study of human factors. Anesthesiology. 1978;49:399---406.
41.Abeyasekhra A, Bergman IJ, Kluger MT, et al. Drug error in anaesthesia practice: a review of 896 reports from the Australian incident monitoring study database. Anaesthesia. 2005;6:220---7.
42.MerryAF,WebsterCS,MathewDJ.Anew,safetyoriented, inte-grateddrugadministrationandautomatedanaesthesiarecord system.AnesthAnalg.2001;93:385---90.
43.Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failure in anaesthesia management. Considerationsforpreventionanddetection.Anaesthesiology. 1984;60:34---42.
44.Sinha A, Singh A, Tewari A. The fatigued anesthesiologist: a threat to patient safety? J Anaesthesiol Clin Pharmacol. 2013;29:151---9.
45.TewariA,SolizJ,BillotaF,etal.Doesoursleepdebtaffect patients’safety?IndianJAnaesth.2011;55:12---7.
46.KeersRN,WilliamsSD, CookeJ,etal. Causesofmedication administrationerrorsinhospitals:asystematicreviewof quan-titativeandqualitativeevidence.DrugSaf.2013;36:1045---67.
47.BlendonRJ,DesRochesCM,BrodieM,etal.Viewsof practic-ingphysiciansandthepubliconmedicalerrors.NEnglJMed. 2002;347:1933---40.
48.Jensen LS, Merry AF, Webster CS, et al. Evidence-based strategies for preventing drug administration errors during anaesthesia.Anaesthesia.2004;59:493---504.
49.EichhornJH.Medicationsafetyintheoperatingroom:timefor anewparadigm.APSFSummitConferenceProceedings.APSF Newslett.2010;25:1---20.