Study conducted at the Clinical Center of Speech-Language, Pathology and Audiology, Pontifícia Universidade Católica de Minas Gerais – PUC – Belo Horizonte (MG), Brazil.
(1) Speech-Language, Pathology and Audiology Department, Pontifícia Universidade Católica de Minas Gerais – PUC Minas – Belo Horizonte (MG), Brazil. Conflict of interests: No
Authors’ contribution: TRS, main researcher: research development, schedule development, literature survey, data collecting and analysis, article writing, article submission and procedures; FAMD, advisor: research development, schedule development, data analysis, correction of the article writings, approval of the final version.
Correspondence adress: Tatiana Rocha Silva. R. Boninas, 1070, Pompeia, Belo Horizonte (MG), Brazil, CEP: 30280-220. E-mail: [email protected] Received: 10/23/2012; Accepted: 9/11/2013
Amplitude of distortion product otoacoustic emissions
and the use of hormonal contraceptives: preliminary
study
Amplitude das emissões otoacústicas produto de distorção e o
uso de contraceptivos hormonais: estudo preliminar
Tatiana Rocha Silva1, Fernanda Abalen Martins Dias1
ABSTRACT
Purpose: To verify differences of otoacoustic emissions responses in women using and not using hormonal contraception. Methods: Partici-pated in this study 30 female individuals, 15 using a hormonal contracep-tive method and 15 that do not use hormonal contraception. All without hearing complaints and hearing within normal limits. Data collection was performed by: transient otoacoustic emissions and distortion product otoacoustic emissions. Results: There was no difference between the amplitude of distortion product otoacoustic emissions for frequencies 1 kHz, 1.4 kHz, 2.8 kHz, 4 kHz and 6 kHz in the right ear between the groups. The frequency of 2 kHz tended to the difference between the amplitude of distortion product otoacoustic emissions between the group of women not using hormonal contraception and use. In the left ear there was no difference between the amplitude of distortion product otoacoustic emissions for frequencies 1 kHz, 1.4 kHz, 2 kHz, 2.8 kHz, 4 kHz and 6 kHz between the groups. Conclusion: No differences were observed in the amplitude of distortion product otoacoustic emissions by use of hormonal contraceptives.
Keywords: Contraceptive agents; Hearing; Hair cells, auditory; Otoa-coustic emissions, spontaneous; Ear, inner
RESUMO
Objetivo: Identificar se há diferença na amplitude das emissões oto-acústicas de mulheres que utilizam e que não utilizam contraceptivo hormonal. Métodos: Participaram da pesquisa 30 mulheres, sendo 15 que utilizam o método contraceptivo hormonal e 15 que não o utilizam, todos sem queixa auditiva e com audição dentro dos padrões de nor-malidade. A coleta de dados foi realizada por meio das emissões otoa-cústicas transientes e pelas emissões otoaotoa-cústicas produto de distorção. Resultados: Não houve diferença entre os valores de amplitude das emissões otoacústicas produto de distorção para as frequências de 1 kHz, 1,4 kHz, 2,8 kHz, 4 kHz e 6 kHz, na orelha direita, nos grupos estudados. Na frequência de 2 kHz houve tendência à diferença entre os valores de amplitude das emissões otoacústicas produto de distorção, comparando-se o grupo de mulheres que não usam contraceptivo hor-monal e o grupo das que usam. Na orelha esquerda, não houve diferença entre os valores de amplitude das emissões otoacústicas produto de distorção para as frequências de 1 kHz, 1,4 kHz, 2 kHz, 2,8 kHz, 4 kHz e 6 kHz, nos dois grupos analisados. Conclusão: Não foram observadas diferenças na amplitude das emissões otoacústicas produto de distorção pelo uso de contraceptivo hormonal, nos grupos estudados.
INTRODUCTION
The otoacoustic emissions evoked by transient stimuli and the otoacoustic emissions distortion products, in individuals with hearing within normal limits, may vary according to the frequency being tested, or between subjects. However, in the analysis intraindivíduo, the amplitude is remarkably consistent. Thus, exposures to noise, drugs, disease or efferent excitation may be monitored(1-6).
The changes that occur during the menstrual cycle can influence the functioning of the cochlear active mechanism and can be evaluated by means of the amplitude of otoacoustic emissions. In the normal menstrual cycle, the frequency of the emission of the response captured decreases before menstrua-tion and increases after the flow starts. The lack of ovulamenstrua-tion, whether natural or induced by contraceptive medication, reduces the fluctuation of the characteristics of spontaneous otoacoustic emission during the cycle(1,7).
The contraceptive use can cause various adverse reactions, such as: immunological changes, metabolics, nutritional, psychiatric, vascular, ocular, gastrointestinal, cutaneous and subcutaneous, renal/urinary, changes in central nervous system, in the reproductive system and hearing changes(7,8). The running
of the inner ear depends of the integrity of the labyrinthine flui-ds. The hormonal changes arising of the contraceptive use may result in commitment of the homeostasis of the labyrinthine fluids, because there is influence in the enzymatic processes and in the actions of neurotransmitters(8,9).
In study realized about dizziness premenstrual, researchers suggest change peripheral vestibular due to fluid retention in the luteal phase of the ovarian cycle. The authors observed, also, that the increase of hormones reaches the inner ear(10,11).
There are studies that correlate changes of the inner ear with the action of hormones. A study reports that the use of oral con-traceptives can occasion degradation of the thresholds hearing, without changing the acoustic reflex(12). Another study, reports
cases of sudden deafness, arising of the use of estrogen and progesterone(13). The use prolonged these hormones can lead
to changes hearing of character sensorineural, in frequencies acute, beyond commitment vestibular total or partial(14).
In a case study, observed that an young presented sudden sensorineural hearing loss, preceded by tinnitus, that was recovered after treatment(13). Some researchers argue that the
contraceptive use does not determine significant hearing im-pairment, but favors the occurrence of tinnitus(15). However,
there are studies that report degradation significant auditory and consistent, in some frequencies, in women that contraceptive use, when compared to women that do not use contraceptives(16).
Currently, the oral contraceptives present less estrogen and progesterone. According to some authors, the reduction of the doses these hormones decreased feelingly the frames of changes hearing(13).
Therefore, this search justified by possibility of understand
and determine the relationship between the activity of the hair cells external and the use of hormonal contraceptives. Thus, the objective of the study was to analyze the amplitude of the otoacoustic emissions distortion products in women that use and that not using hormonal contraception.
METHODS
The procedures in this study were approved by the Research Ethics Committee of Pontifícia Universidade Católica de Minas Gerais (PUC Minas), under protocol number CAAE 0342.0.213.000-10.
This research characterized by a pilot study, of descriptive typology, of qualitative and quantitative analysis. Were invited to participate of the study 60 female subjects. These, eight refused to participate of the research, ten not attend for the eva-luation and the other 12 were excluded of the study by present hearing loss, hearing complaints and/or previous ear disease.
Were included in the research 15 women that have used hormonal contraceptive method compound by estrogen and progesterone, by a period equal or upper to six months and 15 women that not used the hormonal contraceptive method. The sample, therefore, was composed by 30 women, in the age range of 18-25 years.
The research participants were selected in the undergraduate courses offered by the Instituto de Educação Continuada – IEC da Pontifícia Universidade Católica de Minas (PUC Minas) and in the social environment of the researchers, by means of the non-random sampling technique, of the type convenience sampling.
The participants of the research were communicated per-sonally about the objectives of the research, the absence of damage to your health, the guarantee of confidentiality of their identities or any other characteristics which could identify them, and on the roadmap of the research. Being properly informed, all signed the Consent Term.
The data collection was carried in the Clinical Center for Speech – Language Pathology and Audiology of PUC Minas. All the individuals were submitted to basic audiologic evalu-ation. This evaluation consisted of: anamnesis, otoscopy, pure tone audiometry, logoaudiometry, tympanometry and research of acoustic reflexes.
reflexes were performed through the middle ear analyzer, model AZ7, of the brand Interacoustics®.
Were used as inclusion criteria to constitute the study group (control group and research group), individuals without hearing complaints and/or previous ear disease and with audiometry assessment within the normal range: pure tone thresholds by air conduction to 25 dBNA, in the frequencies of 250 Hz to 8 kHz, and pure tone thresholds by bone conduction to 15 dBNA, in the frequencies of de 500 Hz to 4 kHz, with difference between the thresholds of air conduction and bone conduction less or equal to 10 dB, tympanometric curve type A and presence of acoustic reflexes in the frequencies of 500 Hz, 1, 2 and 4 kHz.
Then, the individuals were submitted to research of transient evoked otoacoustic emissions and otoacoustic emissions distor-tion products. Each participant underwent only to an evaluadistor-tion of the otoacoustic emissions transient and an evaluation of the otoacoustic emissions distortion products. Firstly, realized the registry of otoacoustic emissions transient in an of the ears and, then, the registry in the other ear. Posteriorly, realized the registry of otoacoustic emissions distortion products in an of the ears and, then, the registry in the other ear. Therefore, the data collection was performed of way alternating between the ears. It is noteworthy that, due to major methodological difficulty, the phase of the menstrual cycle was not carried in consideration during the research of the otoacoustic emissions in each group.
The transient otoacoustic emissions were performed with non-linear stimulus, type click, with intensities from 80 e 85 dBNPS. The number of stimuli utilized during the registry of the otoacoustic emissions transient not suffered variation (260 series) and the procedure had time of duration of, in the maximum, 75 second in each ear. It was considered level of noise below 16 dB NPS.
In the otoacoustic emissions distortion products, the frequencies f1 and f2 were presented simultaneously, in the intensities of 65 dB and 55 dB, respectively, in the relation f2/ f1=1,22. The frequencies f2 investigated were 1; 1.4; 2; 2.8; 4 and 6 kHz. The registry of the otoacoustic emissions distortion products was suspended when the amplitude of responses not suffered variation in two consecutive scans. The procedure had time of duration of, in the maximum, 200 second in each ear.
To the realization these procedures, was used the otoa-coustic emission analyzer model ILO version 6, of the brand Otodynamics®.
The transient evoked otoacoustic emissions were found to be present when the amplitude of the frequencies of 1 and 1.4 kHz were greater or equal to 3 dB, and of the frequencies of 2, 2.8 and 4 kHz, were greater or equal to 6dB, reproducibility having values greater than 50% and values of stability of the adjustment of the probe greater than 70%. Only individuals who had transient evoked otoacoustic emissions present were included in the study.
The otoacoustic emissions distortion products were found to be present when the difference between the amplitude and
the noise was major or equal to 3 dB, in the frequencies of 1 and 1.4 kHz and when the difference between the amplitude and the noise was major or equal to 6 dB, in the frequencies of 2; 2.8; 4 and 6 kHz.
Then the data collected were tabulated and subjected to statistical analysis. The statistical analysis was performed by of the software MINITAB 16. Initially was performed the des-criptive analysis, that understood measures of central tendency (mean and median), of dispersion (standard deviation) and of position (maximum and minimum).
Besides descriptive statistics was performed the inferential statistics by of the test t of Student, to comparison of two inde-pendent samples. . It was adopted the level of significance of 5% (p≤0.05). It was considered as trend to statistical significance the results significant at level of 10% (p≤0.10).
RESULTS
The mean age of the study population was 21.7 years (stan-dard deviation 2.23), in the group of the women that not using hormonal contraceptive and of 23.5 years (standard deviation 1.68), in the group of the women that have used hormonal contraceptive.
In the descriptive analysis, observed that, in the group of the women that not using hormonal contraceptive, the amplitude of the otoacoustic emissions distortion products was major in the frequency of 6 kHz, in both ears. The mean of the values of amplitude of the frequency of 6 kHz was of 19.67 to the right ear and of 18.33 to the left ear (Table 1).
In the tonal audiometry, observed hearing threshold with intensity level more high in the frequency of 6 kHz, in both ears. The mean of the values of hearing threshold in the frequency of 6 kHz, was of 11.67 to the right ear and of 14.67 to the left ear.
Already in the group of the women that have used hormonal contraceptive, verified that the amplitude of the otoacoustic emissions distortion products was major in the frequency of 4 kHz, in both ears. The mean of the values of amplitude of the frequency of 4 kHz was of 19.56 to the right ear and of 19.49 to the left ear (Table 2).
In the tonal audiometry, observed hearing threshold with intensity level more high in the frequency of 6 kHz, in both ears. The mean of the values of hearing threshold in the fre-quency of 6 kHz, was of 11.67 to the right ear and of 12.67 to the left ear.
In the tonal audiometry observed that the mean of the inten-sity level of the threshold, in the right ear, was more high in the frequencies of 0.25 kHz, 0.5 kHz, 1 kHz, 2 kHz and 3 kHz, in the group of the women that have used hormonal contraceptive. Already in the left ear, the mean of the intensity level of the threshold was more high in the frequencies of 0.25 kHz, 0.5 kHz, 2 kHz, 3 kHz and 4 kHz, in the group of the women that have used hormonal contraceptive.
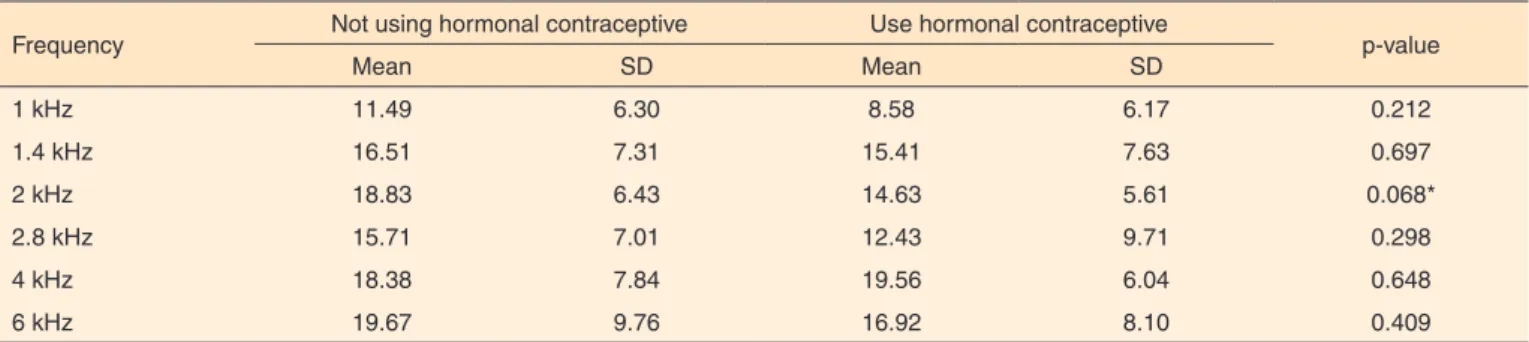
In the statistical analysis inferential verified that there was no difference between the values of amplitude of the otoacous-tic emissions distortion products to the frequencies of 1 kHz, 1.4 kHz, 2.8 kHz, 4 kHz and 6 kHz, in the right ear, between the group of women that not using hormonal contraceptive and the group of the that used. In the frequency of 2 kHz, there was a trend to difference between the values of amplitude of the
otoacoustic emissions distortion products, to the two groups studied (Table 3).
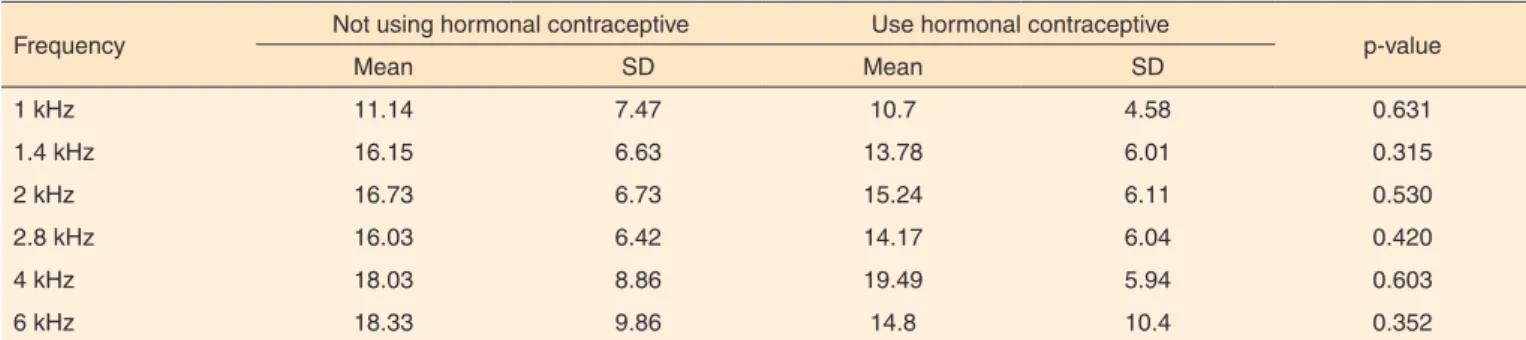
In the left ear, observed that there was no difference between the values of amplitude of the otoacoustic emissions distortion products to the frequencies of 1 kHz, 1.4 kHz, 2 kHz, 2.8 kHz, 4 kHz and 6 kHz, between the groups (Table 4).
In the tonal audiometry, there was no difference between the intensity level of the hearing threshold to the frequencies of 0.25 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz and 8 kHz, in the right ear, between the group of women that not using hormonal contraceptive and the group of the that used. In the frequency of 0.5 kHz, there was a trend to difference between the intensity level of the hearing threshold in the two groups studied (Table 5).
In the left ear, observed that there was no difference between
Table 1. Measures of central tendency, dispersion and position, by frequency, to the values of amplitude of the otoacoustic emissions distortion products in the group that not using hormonal contraceptive
Frequency Mean Median SD Minimum Maximum
RE LE RE LE RE LE RE LE RE LE
1 kHz 11.49 11.14 9.9 11.8 6.30 7.47 2 -1.3 22.9 24.5
1.4 kHz 16.51 16.15 15.8 15 7.61 6.63 4.3 7.8 29.3 30.9
2 kHz 18.83 16.73 17.7 16.4 6.43 6.73 4.9 8.6 31.7 34.4
2.8 kHz 15.71 16.03 14.9 16.1 7.01 6.42 5.5 7.1 27 28.2
4 kHz 18.38 18.03 20.1 20.4 7.84 8.86 5.6 1.5 29 29.9
6 kHz 19.67 18.33 19.3 17 9.76 9.86 2.6 6 36.2 35
Note: SD = standard deviation; RE = right ear; LE = left ear
Table 2. Measures of central tendency, dispersion and position, by frequency, to the values of amplitude of the otoacoustic emissions distortion products in the group that use hormonal contraceptive
Frequency Mean Median SD Minimum Maximum
RE LE RE LE RE LE RE LE RE LE
1 kHz 8.58 10.07 6.7 8.8 6.17 4.58 -3.2 3.9 18.6 22
1.4 kHz 15.41 13.78 13.8 15.3 7.63 6.01 1.6 2.3 26.7 23.1
2 kHz 14.63 15.24 15.7 13.3 5.61 6.11 3.2 6.2 22.3 29.1
2.8 kHz 12.43 14.17 14.2 12.2 9.71 6.04 -17.2 6.3 24.1 23.6
4 kHz 19.56 19.49 22 21.3 6.04 5.94 6 6.6 26.4 26.5
6 kHz 16.92 14.8 18.3 13.8 8.10 10.4 -1 -1.6 33.9 32.7
Note: SD = standard deviation; RE = right ear; LE = left ear
Table 3. Comparison between the groups to the values of amplitude of the otoacoustic emissions distortion products in the right ear
Frequency Not using hormonal contraceptive Use hormonal contraceptive p-value
Mean SD Mean SD
1 kHz 11.49 6.30 8.58 6.17 0.212
1.4 kHz 16.51 7.31 15.41 7.63 0.697
2 kHz 18.83 6.43 14.63 5.61 0.068*
2.8 kHz 15.71 7.01 12.43 9.71 0.298
4 kHz 18.38 7.84 19.56 6.04 0.648
6 kHz 19.67 9.76 16.92 8.10 0.409
Test t (p≤0,05)
*Trend towards statistical significance (p≤0.10) – Test t
the intensity level of the hearing threshold to the frequencies of 0.25 kHz (p=0.895), 0.5 kHz (p=0.479), 1 kHz (p=0.515), 2 kHz (p=0.874), 3 kHz (p=0.511), 4 kHz (p=0.801), 6 kHz (p=0.568) and 8 kHz (p=0.721), between the groups.
In the separate analysis of the data for each group, veri-fied that, in the group of the women that not using hormonal contraceptive, there was no difference between the values of amplitude of the otoacoustic emissions distortion products between the right ear and the left ear, in the frequencies of 1 kHz (p=0.898), 1.4 kHz (p=0.891), 2 kHz (p=0.391), 2.8 kHz (p=0.897), 4 kHz (p=0.911) and 6 kHz (p=0.712). In the group of the women that have used hormonal contraceptive, also there was no difference between the values of amplitude of the otoacoustic emissions distortion products, between the right ear and the left ear, in the frequencies of 1 kHz (p=0.461), 1.4 kHz (p=0.521), 2 kHz (p=0.779), 2.8 kHz (p=0.561), 4 kHz (p=0.974) and 6 kHz (p=0.545).
In the tonal audiometry, observed that, in the group of the women that not using hormonal contraceptive, there was no difference between the intensity level of the hearing threshold, between the right ear and the left ear, in the frequencies of 0.25 kHz (p=0.417), 0.5 kHz (p=0.707), 1 kHz (p=0.207), 2 kHz (p=0.416), 3 kHz (p=0.676), 4 kHz (p=1.000), 6 kHz (p=0.303) and 8 kHz (p=0.289). In the group of the women that have used hormonal contraceptive, also there was no difference between the
intensity level of the hearing threshold, between the right ear and the left ear, in the frequencies of 0,25 kHz (p=0,760), 0,5 kHz (p=0,431), 1 kHz (p=0,600), 2 kHz (p=0,545), 3 kHz (p=0,232), 4 kHz (p=0,748), 6 kHz (p=0,769) and 8 kHz (p=0,224).
In the analysis of entire sample, independent of the use of hormonal contraceptive, verified that also there was no difference between the values of amplitude of the otoacoustic emissions distortion products, between the ears, in the frequen-cies of 1 kHz (p=0.719), 1.4 kHz (p=0.581), 2 kHz (p=0.651), 2.8 kHz (p=0.564), 4 kHz (p=0.910) and 6 kHz (p=0.490). In the tonal audiometry, also there was no difference between the intensity level of the hearing threshold, between the ears, in the frequencies of 0.25 kHz (p=0.410), 0.5 kHz (p=0.788), 1 kHz (p=0.610), 2 kHz (p=0.302), 3 kHz (p=0.271), 4 kHz (p=0.846), 6 kHz (p=0.362) and 8 kHz (p=0.101).
DISCUSSION
The transient otoacoustic emissions and distortion products can be detected in individuals with normal hearing(2). Thus,
this can be the justification to the absence of significant diffe-rences in the amplitude response of the otoacoustic emissions distortion products, between women that used and that not using hormonal contraceptive, as all presented hearing within the normal range.
Table 4. Comparison between the groups to the values of amplitude of the otoacoustic emissions distortion products in the left ear
Frequency Not using hormonal contraceptive Use hormonal contraceptive p-value
Mean SD Mean SD
1 kHz 11.14 7.47 10.7 4.58 0.631
1.4 kHz 16.15 6.63 13.78 6.01 0.315
2 kHz 16.73 6.73 15.24 6.11 0.530
2.8 kHz 16.03 6.42 14.17 6.04 0.420
4 kHz 18.03 8.86 19.49 5.94 0.603
6 kHz 18.33 9.86 14.8 10.4 0.352
Test t (p≤0,05)
Note: SD = standard deviation
Table 5. Comparison between the groups to the intensity level of the hearing threshold in the tonal audiometry in the right ear
Frequency Not using hormonal contraceptive Use hormonal contraceptive p-value
Mean SD Mean SD
0.25 kHz 7.33 6.22 9 5.07 0.489
0.5 kHz 6 3.38 9.33 4.95 0.0422#
1 kHz 4.33 3.71 6.33 5.16 0.235
2 kHz 4 4.30 5 4.22 0.523
3 kHz 4.33 4.16 4.67 5.16 0.847
4 kHz 5.33 6.93 5.33 5.49 1.000
6 kHz 11.67 6.45 11.67 8.38 1.000
8 kHz 7.33 7.98 6 6.60 0.622
Furthermore, the participants of each group were in di-fferent periods of the menstrual cycle. The menstrual cycle is divided in three phases and in each phase there is variation of the hormone levels. Probably, if these phases were take into consideration to interpret the amplitudes response of the otoa-coustic emissions distortion products, the results could present significant differences.
The absence of difference in the amplitude response of the otoacoustic emissions distortion products, between the groups of women that not using and that used hormonal contraceptive, also can be justified by the fact of the otoacoustic emissions be best captured in individuals with thresholds of audibility between 0 e 15 dBNA(6). This study, all groups presented mean
of the values of hearing threshold less than 15 dBNA, in all the frequencies investigated to both ears.
It is noteworthy that the result of the frequencies acute, that presented major amplitude response in the otoacoustic emissions distortion products and intensity level of the hearing threshold uppermost in the tonal audiometry, in the two groups surveyed, not is coherent with the literature consulted, that affirm that the frequencies acute are the first to suffer damage with the use of hormonal contraceptive(14).
Some authors studied the nonlinear of the human cochlea in the frequencies of 0.5 and 4 kHz and suggested that there is an dynamic band more ample and higher gain of the cochlear amplifier in 4 kHz, when compared with 0.5 kHz(5). Other
authors observed that the variation of the thresholds of the growth curves of the otoacoustic emissions were major in the frequencies of 4 and 6 kHz, when compared with the frequency of 2 kHz(6). This higher variation in high frequencies can be
interpreted by the action of the cochlear amplifier. Thus, can also be affected indirectly and be a of the factors that generate major variability in the high frequencies.
In study that evaluated the otoacoustic emissions during the three phases of the female hormonal cycle (follicular, ovulatory and luteal), observed that there was no differences in the ampli-tude response of the otoacoustic emissions distortion products, in the majority of the frequencies tested. The frequency of 6 kHz was the only that presented values of amplitude less than the expected(1).
This absence of significant differences in the amplitude res-ponse of the otoacoustic emissions distortion products, between women that used and that not using hormonal contraceptive, can seem surprising, because a previous study revealed differences of the auditory function, in evaluations varied, as listening dichotic, or spontaneous otoacoustic emission(7). However,
the changes of auditory responses appear be reflex of central activities and the otoacoustic emissions are descendant of pre--neural activities. Specific physiological events of the female appear not cause significant differences in the response of the otoacoustic emissions distortion products, the that implies to not need of consider the use of the hormonal contraceptive to interpret the results of the otoacoustic emissions distortion
products. Independently of the use of contraceptive, the veracity of the responses appears to be stable(3).
It is noteworthy that, in this study, not were observed di-fferences between the amplitude response of the otoacoustic emissions distortion products between the ears, so much in the group that not use how much in the group that use hormonal contraceptive. This result differs of the literature consulted, that observed expressive difference in the values of the amplitude of the otoacoustic emissions distortion products in frequency of 1.5 kHz, between left ear and right, having the right ear, presen-ted the higher values(1). However, in other study consulted, also
not were observed differences between the amplitude response of the otoacoustic emissions distortion products, between the right ear and left(2).
The knowledge about the otoacoustic emissions yet is very recent. The otoacoustic emissions, after being generated in the cochlea, suffer interferences in the path until the probe and can indicate small changes of impedance in the driving system. Thus, reflect the condition of the auditory system, whose fina-lity is capture, conduct and amplify the sound vibrations, with the constant maintenance of the better conditions transducer, ensuring a high index of income to transfer the information contained in the sound energy until the specialized sensory cells, in which the vibrations are converted in electrical im-pulses and transmitted until the auditory cortex. A system so rich and efficacious should, necessarily, contain yet numerous functions partially unknown(4).
In this study, the sample evaluated was small, that may have been determinant to the not significance of the results. The number of participants in similar studies also is reduced. It is noteworthy that, in the period of the evaluation, some participants not attend and that difficult the conclusion of the research in the period of time available.
The number of similar studies also is reduced, confirming the difficulty methodological and logistical this type of study. Thus, other studies must be performed with larger casuistry and having criteria of inclusion different, as type of hormonal contraceptive (oral or injectable), time of use and phase of the menstrual cycle.
CONCLUSION
There was no difference between the amplitude of the otoacoustic emissions distortion products between the women that used and that not using contraceptive. Therefore, the use of hormonal contraceptive not affected the activity of the hair cells external.
REFERENCES
2. Guedes MC, Passos SN, Gomez MVSG, Bento RF. Estudo da reprodutibilidade das emissões otoacústicas em indivíduos normais. Rev Bras Otorhinolaryngol. 2002;68(1):34-8.
3. Yellin MW, Stillman RD. Otoacoustic emissions in normal-cycling females. J Am Acad Audiol. 1999;10(7):400-8.
4. Couto CM, Carvalho RMM. O efeito das orelhas externa e média nas emissões otoacústicas. Rev Bras Otorrinolaringol. 2009;75(1):15-23. 5. Gorga MP, Neely ST, Dierking DM, Kopun J, Jolkowski K,
Groenenboom K, et al. Low frequency and high-frequency cochlear nonlinearity in humans. J Acoust Soc Am. 2007;122(3):1671. 6. Campos UP, Carvalho RMM. Correlação entre os limiares das curvas
de crescimento das EOAPD e tons puros. Braz J Otorhinolaryngol. 2011;77(6):754-60.
7. Penner MJ. Cycle, amenorrhea, and oral contraception: a brief report. Ear Hear. 1995;16:428-32.
8. Mitre EI, Figueira AS, Rocha AB, Alves SMC. Avaliações audiométrica e vestibular em mulheres que utilizam o método contraceptivo hormonal oral. Rev Bras Otorhinolaryngol. 2006;72(3):350-4.
9. Hanna GS. Sudden deafness and the contraceptive pill. J Laryngol Otol. 1986;100(6):701-6.
10. Isbii C, Nisbino LK, Campos CAH. Caracterização vestibular no ciclo menstrual. Braz J Otorhinolaryngol. 2009;75(3):375-80. 11. Gomez MVSG, Caovila HH, Ganança MM. Tonturas pré-menstruais:
avaliação otoneurológica. Feminina. 1993;21:437-44.
12. Abdel Nabi EA, Motawee E, Lasheen N, Taha A. A study of vertigo and dizziness in the premenstrual period. J Laryngol Otol. 1984;98(3):273-5.
13. Bittar RSM. Labirintopatias hormonais: hormônios, esteroides, estrógeno e progesterona. Rev Arq Fund Otorrinolaringol. 1997;4(1):122-6.
14. Bausch J. Effects and side effects of hormonal contraceptives in the region of the nose, throat and ear. HNO. 1983;31(12):409-14. 15. De Domenico ML, Iório MCM. Avaliação audiológica em mulheres
que fazem uso de anticoncepcionais hormonais orais. Pró-fono. 2002;14(3):415-24.