rev bras hematol hemoter. 2015;37(6):417–419
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Axillary
high-grade
B-cell
non-Hodgkin
lymphoma
presenting
under
the
guise
of
inflammatory
breast
carcinoma
Christian
Ribas
∗,
Marcos
Antônio
Navarro,
Leonora
Z.B.
Pope,
Gilberto
Hornburg
HospitalDonaHelena,Joinville,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4August2015 Accepted31August2015 Availableonline9October2015
Introduction
Non-Hodgkinlymphomas(NHL)areaheterogeneousgroupof lymphoproliferativedisordersoriginating inlymphocytesor naturalkillercellswithmostcasesbeingB-celllymphomas. Thetypicalpresentationisofarapidlyenlargingtumormass atsingleormultiplenodalsitesalthoughupto40%ofpatients mayhavediseaseinitiallyconfinedtoextranodalstructures.1 Inflammatorybreastcarcinoma(IBC)isarareand particu-larlyaggressiveformofbreastcancer,characterizedbyrapid onsetoferythemaandedema(peaud’orange)occupyingat leastone-thirdofthebreast.Thediagnosisismadeon clin-icalgroundsassociatedwithpathologicaldocumentationof invasivecarcinomainthebreastparenchyma.2,3
We describe a female patient with an enlarged, ery-themicandedematousleftbreast,regionaladenopathyand poorly differentiated carcinoma on hematoxylin and eosin (H&E)staining, who after properimagingand immunohis-tochemistryprovedtohaveahigh-gradeaxillaryB-cellNHL presentingundertheguiseofIBC.
∗ Correspondingauthorat:HospitalDonaHelena,SetordeOncologiaClínica,RuaBlumenau,123,89204-250,Joinville,SC,Brazil.
E-mailaddress:[email protected](C.Ribas).
Case
report
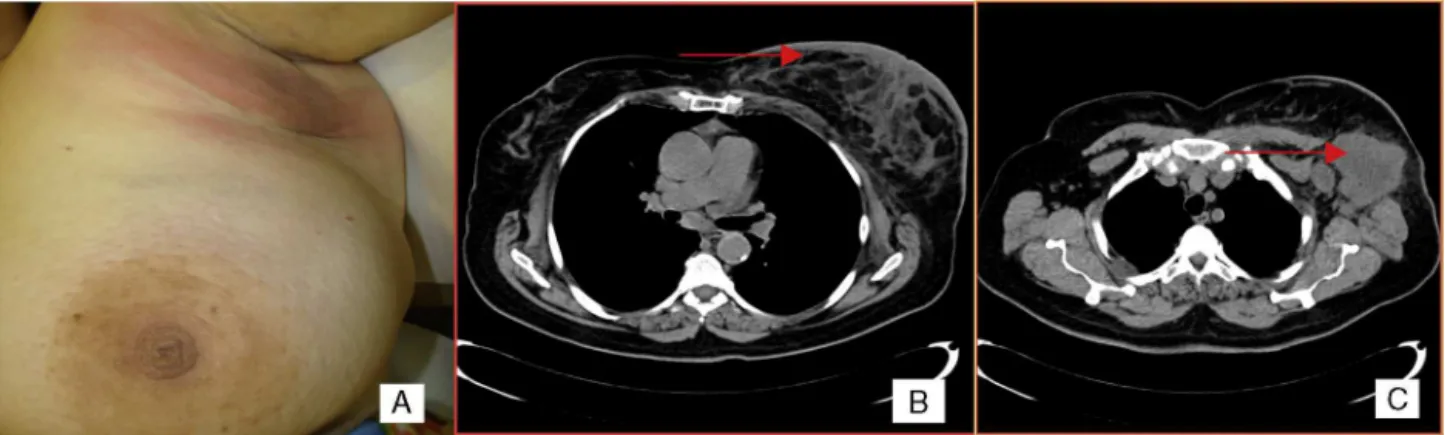
A 66-year-oldwoman presentedwitha3-month historyof left breast enlargement, erythema and peau d’orange skin edema (Figure 1). There was no palpable nodule or nipple discharge.Theerythemaextendedintotheleftaxilla,wherea voluminous,ill-definedmasswasidentified.Noothermasses orlesionsoftherightbreastorelsewherewerenotedonthe exam.Bilateralmammographyandbreastultrasoundshowed abnormalities of the left breast: skin thickening, diffusely hyperechogenic breast parenchyma,dilatedintramammary lymphatics andahypoechogenicmass(extensive adenopa-thy) in the left axilla; no nodules or microcalcifications wereapparent.Suchfindingswerealsoapparentonachest computedtomography(CT)scan(Figure1).Incisionalbiopsy oftheaxillarymasswascarriedout.H&Esections revealed subcutaneousinfiltrationbypoorlydifferentiatedcarcinoma (Figure2).Giventhe changesoftheleft breastreminiscent of IBC, punch biopsy of the breast skin was performed. Resultsshowed dermal angiolymphaticectasia and benign
http://dx.doi.org/10.1016/j.bjhh.2015.08.007
418
revbrashematolhemoter.2015;37(6):417–419Figure1–Clinicalfeatures.(A)Erythemaandpeaud’orangeskinedema.(B)Asymmetricskinthickeningandstromaledema oftheleftbreastonacomputedtomographyscan.(C)Lymphnodemassintheleftaxillaonacomputedtomographyscan.
perivascularlymphocytes; adeep corebiopsy ofthebreast parenchyma showed similar histologic features with no neoplastic cells. The immunohistochemistry panel (CD20+
diffuse; CD3− Ki-67+ in 80% of cells; negativity for the epithelialantigensAE1/AE3,estrogenreceptor,progesterone receptor, Her2-neu) supported the diagnosis of high-grade B-Cell NHL (Figure 2). Significant constitutional symptoms wereabsent.Stagingprocedures(chestandabdominopelvic CT scans, positron emission-computed tomography (PET-CT), cerebrospinal fluid analysis, bone marrow smear and biopsy) revealed stage IVA, high-risk international prog-nosticindex(IPI) 4disease,withmediastinaladenopathies, matted lymph nodes forming a 6.8cm mass involving the adiposetissueoftheleftaxilla,andmultiplesecondarylung and splenic nodules. The patient was treated with eight cycles of systemic chemotherapy (R-CHOP-21: rituximab, cyclophosphamide,doxorubicin,vincristineandprednisone), cyclingevery 21 days, andcentral nervoussystem prophy-laxis with intrathecal methotrexate. The treatment was well tolerated, resulting in complete resolution of breast abnormalities and systemic disease control on interval CT scans.PET-CT attheend ofchemotherapyshowedthe dis-ease had disappearedfrom all sitesapart from a residual,
involuted and metabolically faint left axillary adenopathy, withonlyextensivecoagulativenecrosisonresection.Three years after the diagnosis,the patient remains in complete remission.
Discussion
NHLareaheterogeneousgroupoflymphoproliferative disor-derswithdistinctclinicalandpathologicfeatures.InBrazil, theyareamongthetwelvemostfrequentcancersinbothmen andwomen,withanestimatedincidenceof9918newcases in2015.4,5
DiffuselargeB-celllymphomaisthemostcommonNHL, accountingforaround30%ofadultcasesinwesterncountries. Although a percentage of NHL patients may initially have diseaseconfinedtoextranodalstructures,thetypical presen-tation is of a rapidly enlarging tumor mass ata single or multiplenodalsites.1
IBC is a relatively rare clinicopathologic entity that accountsfor2%ofinvasivebreastcancers.2 IBCrepresents the mostaggressivetypeofbreastcancer,being character-ized byrapidonset oferythemaandedema(peaud’orange)
revbrashematolhemoter.2015;37(6):417–419
419
occupyingatleastone-thirdofthebreast.Theskinchanges arecaused bydermallymphaticinvolvementbymalignant cells,whosepresenceonpunchbiopsyispathognomonicof IBC.Despitetheoccasionalabsenceofapalpablebreastmass, mostcasesofIBChavelocoregionaldisease(metastases to axillary/supraclavicularnodes)andabout30%havestageIV metastaticdiseaseatdiagnosis.Thediagnosisisbasedon clin-icalcharacteristicswithessentialpathologicalconfirmationof invasivecarcinoma.3
Theclinical characteristicsofIBCare ratherunusualfor NHLs, being occasionally reported in uncommon cases of primaryorsecondarybreastinvolvementbylymphomas.6,7 NodalaxillaryNHL,however,mayalsotakeontheappearance of IBC,8 even in the absence of direct breast involve-ment as highlighted herein. Presumably, this would occur because oflymph-vascular engorgement and the resultant skinchanges.
Although,byroutineH&Estainingourpatienthadthe ini-tialdiagnosisofinvasivecarcinoma,whichmakeslymphoma lessplausible,NHLmaysometimesappearaspoorly differ-entiatedcarcinomabyconventionalhistology.Negativityfor cytokeratins(e.g.AE1/AE3)andstrongpositivityforthe leuko-cytecommonantigenandCD20allowthediagnosisofB-cell NHLtobemade.9
Astheincidenceoflymphomas, particularlyB-cell lym-phomas,isincreasingworldwide,1itisimportanttobeaware oftheirmostuncommonpresentations.AxillarynodalNHL withreactive breast/skin changes should then beincluded among the differential diagnoses of IBC, together with otherentitiessuchasacutemastitis,breastlymphomaand extramammarycarcinomasmetastatictothebreast;such dis-tinctionisofparamountimportancesincetheprognosesand managementaresubstantiallydiverse.
r
e
f
e
r
e
n
c
e
s
1.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriSA,SteinH, etal.WHOclassificationoftumoursofhaematopoieticand lymphoidtissues.Lyon:IARC;2008,310p.
2.HanceKW,AndersonWF,DevesaSS,YoungHA,LevinePH. Trendsininflammatorybreastcarcinomaincidenceand survival:thesurveillance,epidemiology,andendresults programattheNationalCancerInstitute.JNatlCancerInst. 2005;97(13):966–75.
3.DawoodS,MerajverSD,ViensP,VermeulenPB,SwainSM, BuchholzTA,etal.Internationalexpertpaneloninflammatory breastcancer:consensusstatementforstandardizeddiagnosis andtreatment.AnnOncol.2011;22(3):515–23.
4.FerlayJ,SoerjomataramI,ErvikM,DikshitR,EserS,MathersC, etal.GLOBOCAN2012v1.0,cancerincidenceandmortality worldwide:IARCCancerBaseNo.11[Internet].Lyon,France: InternationalAgencyforResearchonCancer;2013.Available from:http://globocan.iarc.fr
5.Estimate/2014–cancerincidenceinBrazil.RiodeJaneiro: INCA;2014.Availablefrom:http://www.inca.gov.br[cited 04.04.15].
6.KrishnanC,MolineS,AndersK,WarnkeRA.Intravascular ALK-positiveanaplasticlarge-celllymphomamimicking inflammatorybreastcarcinoma.JClinOncol.
2009;27(15):2563–5.
7.KeltenC,KabukcuS,SenN,TekeZ,YarenA,ErdemE,etal. SecondaryinvolvementofthebreastinT-cellnon-Hodgkin lymphoma,anunusualexamplemimickinginflammatory breastcarcinoma.ArchGynecolObstet.2009;208(1):149–52.
8.TaubmanK,MacKayM.Axillarylymphomamasqueradingas inflammatorybreastcancer.BiomedImagingIntervJ. 2006;2(3):e36.