ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Alcohol,
smoking
and
illicit
drug
use
in
pediatric
systemic
lupus
erythematosus
patients
Marlon
van
Weelden
a,b,
Lígia
B.
Queiroz
c,
Daniela
M.R.
Lourenc¸o
a,
Katia
Kozu
a,
Benito
Lourenc¸o
c,
Clovis
A.
Silva
a,c,∗aPediatricRheumatologyUnit,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil bMedicalFaculty,VUUniversity,Amsterdam,Netherlands
cAdolescentUnit,SchoolofMedicine,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received18June2015 Accepted13October2015 Availableonline28February2016
Keywords: Alcohol Smoking Bullying Puberty
Childhoodonsetsystemiclupus erythematosus
a
b
s
t
r
a
c
t
Objective:Toevaluatealcohol,smokingand/orillicitdruguse,andhistoryofbullyingin adolescentchildhood-onsetsystemiclupuserythematosusandhealthycontrols.
Methods:174adolescentswithpediatricrheumaticdiseaseswereselected.All ofthe34 childhood-onsetsystemiclupuserythematosuspatientsand35healthycontrols partici-patedinthisstudy.Across-sectionalstudyincludeddemographic/anthropometricdataand pubertymarkersassessments;structuredquestionnaireandCRAFFTscreeninginterview. Results:McNemartestsindicatedanexcellenttest–retestreliabilityofthestructured ques-tionnaire(p=1.0).Themediancurrentagewassimilarbetweenchildhood-onsetsystemic lupuserythematosuspatientsandcontrols[15(12–18)vs.15(12–18)years,p=0.563].The medianofmenarcheagewassignificantlyhigherinchildhood-onsetsystemiclupus erythe-matosuspatientscomparedtocontrols[12(10–15)vs.11.5(9–15)years,p=0.041],particularly inthosethatlupushadoccurredbeforefirstmenstruation[13(12–15)vs.11.5(9–15)years, p=0.007].Theotherpubertymarkerandsexualfunctionparametersweresimilarinboth groups(p>0.05).Alcoholusewassimilarinbothchildhood-onsetsystemiclupus erythe-matosuspatientsandcontrols(38%vs.46%,p=0.628).AtrendoflowerfrequencyofCRAFFT score≥2(highriskforsubstanceabuse/dependence)wasevidencedinchildhood-onset sys-temiclupuserythematosuspatientscomparedtocontrols(0%vs.15%,p=0.053).Bullying wasreportedsimilarlyforthetwogroups(43%vs.44%,p=0.950).Furtheranalysisinlupus patientsregardingalcohol/smoking/illicitdruguseshowednodifferencesindemographic data,pubertymarkers,historyofbullying,sexualfunction,contraceptiveuse,disease activ-ity/damagescores,clinical/laboratorialfeaturesandtreatments(p>0.05).
∗ Correspondingauthor.
E-mail:[email protected](C.A.Silva).
http://dx.doi.org/10.1016/j.rbre.2016.02.001
Conclusion: Thisstudyshowedhighfrequenciesofearlyalcoholuseinlupusadolescents andhealthycontrols,despiteofapossiblelowriskforsubstanceabuse/dependencein childhood-onsetsystemiclupuserythematosuspatients.
©2016ElsevierEditoraLtda.Allrightsreserved.
Uso
de
álcool,
tabaco
e
drogas
ilícitas
por
pacientes
com
lúpus
eritematoso
sistêmico
pediátrico
Palavras-chave: Álcool Tabagismo Bullying Puberdade
Lúpuseritematososistêmicode inícionainfância
r
e
s
u
m
o
Objetivo: Avaliar o uso de álcool, tabaco e/ou drogas ilícitas e a história de bully-ing entreadolescentes com lúpuseritematoso sistêmicopediátrico (LES-p) e controles saudáveis.
Métodos:Selecionaram-se174adolescentescomdoenc¸asreumatológicaspediátricas.Todos os34pacientescomLES-ie35controlessaudáveisparticiparamdesteestudo.Umestudo transversal incluiuavaliac¸õesdedadosdemográficos/antropométricose marcadoresda puberdade,umquestionárioestruturadoeaentrevistadetriagemCrafft.
Resultados: TestesdeMcNemarindicaramumaexcelenteconfiabilidadeteste-retestedo questionárioestruturado(p=1,0).Amedianadaidadeatualfoisemelhanteentrepacientes comLES-iecontroles[15(12a18)vs.15(12a18)anos,p=0,563].Amedianadaidadena menarcafoisignificativamentemaiorempacientescomLES-iemcomparac¸ãocomos con-troles[12(10a15)vs.11,5(9a15)anos,p=0,041],particularmentenaquelasemquemo lúpusocorreuantesdaprimeiramenstruac¸ão[13(12a15)vs.11,5(9a15)anos,p=0,007]. Osoutrosmarcadoresdapuberdadeeparâmetrosdefunc¸ãosexualforamsimilaresnos doisgrupos(p>0,05).OusodeálcoolfoisemelhanteentrepacientescomLES-iecontroles (38%vs.46%,p=0,628).Evidenciou-seumatendênciademenorfrequênciadepontuac¸ão≥ 2noCrafft(altoriscoparausoabusivo/dependênciadesubstâncias)empacientescomLES-i emcomparac¸ãocomoscontroles(0%vs.15%,p=0,053).Obullyingfoirelatadoem frequên-ciasemelhantenosdoisgrupos(43%vs.44%,p=0,950).Umaanálisemaisaprofundada emrelac¸ãoaousodeálcool/tabaco/drogasilícitasempacientescomlúpusnãomostrou diferenc¸asnosdadosdemográficos,marcadoresdapuberdade,históriadebullying,func¸ão sexual,usode anticoncepcionais,escoresdeatividade/danosda doenc¸a,características clínicas/laboratoriaisetratamentos(p>0,05).
Conclusão: Esteestudomostrouumaaltafrequênciadeusoprecocedeálcoolem ado-lescentescomlúpusecontrolessaudáveis,apesardeum possívelbaixoriscoparauso abusivo/dependênciadesubstânciasempacientescomLES-i.
©2016ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Childhood-onset systemic lupus erythematosus (c-SLE) is a rare disease that occurs mainly in adolescents. Adoles-cence is a transitional period of physical and psycholog-ical development that may be associated with high-risk behaviors.1
In this regard, alcohol, smoking and illicit drug use is a relevant public health issue in healthy adolescents with high risk for substance abuse/dependence2 and sex-ualdysfunction.3Furthermore,adolescentsmaysufferfrom bullyingvictimizationwithpoorerhealthstatusand psycho-logical distress.4 However, the concomitant assessment of theseadolescenthealthproblemswasnotperformedinc-SLE population.
Therefore,theobjectiveofourstudywastoassessalcohol, smokingand/orillicitdruguseinadolescentc-SLEpatients
andhealthycontrols.Wealsoevaluatedthepossible associ-ationsbetweenalcohol,smokingand/orillicitdruguseand: demographicdata,bullying,clinicalfeatures,puberty mark-ers, sexualfunction, contraceptiveuse, disease parameters andtreatmentsinlupuspopulation.
Materials
and
methods
Patientsandcontrols
toparticipate.Allofthemparticipatedinthiscross-sectional study and fulfilled the American College ofRheumatology classification criteria for SLE.5 The control group included 35healthyfemaleadolescentsfollowed-upinourUniversity Hospitalattheeducationalandpreventivegroupofthe Ado-lescentUnit.Thesecontrolvolunteersweresubjectedtothe sameexclusioncriteria.LocalEthicsCommitteeofour univer-sityhospitalapprovedthisstudy.
Pubertymarkers,sexualfunctionand alcohol/smoking/illicitdruguse,andbullying
Thisstudy includeddemographic/anthropometric dataand puberty markers assessments; a structured questionnaire evaluated sexual function and alcohol, smoking and illicit drug use, bullying and the PortugueseCRAFFT (mnemonic acronym of car, relax, alone, forget, friends, trouble) screen (CRAFFT/CEASER) version.6,7 These aspects were performed blinded to clinical, laboratorial and treatment assessments.
Socio-demographicandanthropometricdata
Current age, gender, years of education, weight and heightwere evaluated.Bodymassindex (BMI)was defined by the formula: weight in kilograms/height in square meters.
The Brazilian socio-economic classes were classified accordingtotheABEP(Associac¸a˜oBrasileiradeEmpresasde Pesquisa).8
Pubertymarkersassessments
Secondarysexualcharacteristicswereclassifiedaccordingto Tannerpubertalchangesinbothgenders.9Ageatfirst men-struation(menarche)andfirstejaculation(spermarche)were registeredbasedonmemoryrecollection.
Structuredquestionnaire
Apilotstudywascarriedoutin30consecutiveadolescents whoweretestedandthenretested1–2monthslaterin Febru-ary and April 2014, to evaluate response reliability of the aforementioned questionnaire, covering the following fea-tures:sexualfunctionandalcohol/smokingandillicitdrugs use.
Sexualfunctionevaluationincluded:presenceandageat firstsexualintercourse,sexualintercourseinthelastmonth, useofmalecontraception(condom)inthefirstsexualactivity, oralandemergencycontraceptiveuse,knowledgeofsexual activity by parents and number of sexual partners in life. Bothhealthycontrolsandc-SLEpatientshavearoutine ori-entationaboutsexualfunctionandbirthcontrols,emotional problemsand drugsissuesinthe Adolescent andPediatric RheumatologyUnitsofourUniversityHospital.Barrier meth-odsareencouragedforourentiremaleandfemalesexually activec-SLEpatient.Althoughitslong-termuseisassociated withdecreasedbonemineraldensity,depot medroxyproges-terone acetateinjection (every three monthsadministered inourDayHospital)isourpreferablemethodindicatedfor
all sexually active c-SLE patient, due to adequate adher-ence. Progestin-only pills may be also used, although the mainissuerelatedtoitsusebyadolescentsispoor compli-anceduetomenstrualirregularity.Orallevonorgestrelisalso indicatedasanemergencycontraceptionmethodinfemale c-SLE.
Alcohol/smokingandillicitdrugsuseassessmentinvolved: age atalcoholinitiation, numberof daysofalcoholuse in the last30days,age atsmoking initiation,number ofdays using cigarettesinthelast 30days,age atillicitdrug initi-ation and number ofdays usingillicitdrugs inthe last 30 days.Useofillicitinhalantsdrug(gluesniffing,aerosoland solvent) and illegal drugs [marijuana, stimulants (cocaine, crack and speed), LSD, opiates, heroin and ecstasy] were systematicallyassessed.Bullying,whichisdefinedas recur-rentexposuretoemotionaland/orphysicalaggression,was registeredbasedonmemoryrecollection.Thequestionnaire wasgivenintheabsenceoflegalguardians,relativesand/or friends.
CRAFFTscreening
The Portuguese version of physician-conducted CRAFFT (CRAFFT/CEASER) screen wasused and consistsof9 ques-tions developedtoscreen adolescents forhigh-riskalcohol and drugsuse.6Thisquestionnaireisdivided intwo parts. PartAincludesthreequestionsregardingtheuseofalcohol, marijuana,hashish oranothersubstanceinthelasttwelve months.Iftheadolescentresponded“no”toallthree ques-tions,onlythequestionrelatedto“Car”oftheB-partshould beasked.Iftheadolescentanswered“yes”tooneofthe open-ingquestions,allofthequestionsofpartBshouldbeasked. TheB-partcontainedsixquestions,whicharesignsof prob-lematicsubstanceuse,suchas:1.“Haveyoueverriddenina cardrivenbysomeone(includingyourself)whowas“high”or hadbeenusingalcoholordrugs?”,2.“Doyoueveruse alco-holordrugstorelax,feelbetteraboutyourself,orfitin?”,3. “Doyoueverusealcoholordrugswhileyouarebyyourself, oralone?”,4“Doyoueverforgetthingsyoudidwhileusing alcoholordrugs?”,5.“Doyourfamilyorfriendsevertellyou thatyoushouldcutdownonyourdrinkingordruguse?”,6. “Haveyouevergottenintotroublewhileyouwereusing alco-holordrugs?”.Onepointwasrelatedtoeach answer“yes” intheB-partofthequestionnaire.Atotalscoreof≥2 indi-catedhighriskforsubstanceabuse/dependenceandaneed foradditionalassessment.7
c-SLEclinical,laboratorialandtreatmentassessments
SLEclinicalmanifestationsweredefinedas:articular involve-ment(non-erosivearthritis),mucocutaneouslesions(malaror discoidrash,oralulcersorphotosensitivity),serositis (pleu-ritis or pericarditis), neuropsychiatric diseases (seizure or psychosis), renalinvolvement(proteinuria≥0.5g/24h, pres-ence ofcellularcasts,and/orpersistent hematuria≥10 red blood cells per high power field), and hematologic abnor-malities (hemolyticanemia,leukopenia withawhite blood cell count<4000/mm3, lymphopenia<1500/mm3 ontwo or
Erythrocyte sedimentation rate (ESR) was performed by Westergreenmethodand C-reactive protein(CRP) by neph-elometry. Anti-double-stranded DNA (anti-dsDNA) autoan-tibodywas detectedbyindirect immunofluorescenceusing Crithidialuciliaeassubstrate.
Diseaseactivity wasevaluated accordingtoSLEDisease Activity Index2000(SLEDAI-2K).10 Cumulativedamagewas measured by SLE International Collaborating Clinics/ACR DamageIndex(SLICC/ACR-DI).11
Dataconcerningtheuseandcurrentdosageofprednisone, hydroxychloroquine,methotrexate,azathioprine,intravenous cyclophosphamide,mycophenolatemofetilandintravenous immunoglobulinwerealsodetermined.
Statisticalanalysis
Thetest–retestreliabilityofthestructuredquestionnairewas verifiedusingtheMcNemar test.Resultswerepresentedas themean±standarddeviation(SD)ormedian(range)for con-tinuousandnumber(%)forcategoricalvariables.Datawere comparedbyttestorMann–Whitneytestincontinuous vari-ablestoevaluatedifferencesbetweenc-SLEandcontrols,and betweenSLEsubgroups.Forcategoricalvariables,differences wereassessedbyFisher’sexacttestorPearsonchi-squaretest. SpearmanrankcorrelationcoefficientwasusedforCRAFFT scoreandagecorrelations.Thelevelofsignificancewassetat 5%(p<0.05).
Results
McNemartestsindicatedanexcellenttest–retestreliabilityof thestructuredquestionnaire(p=1.0).
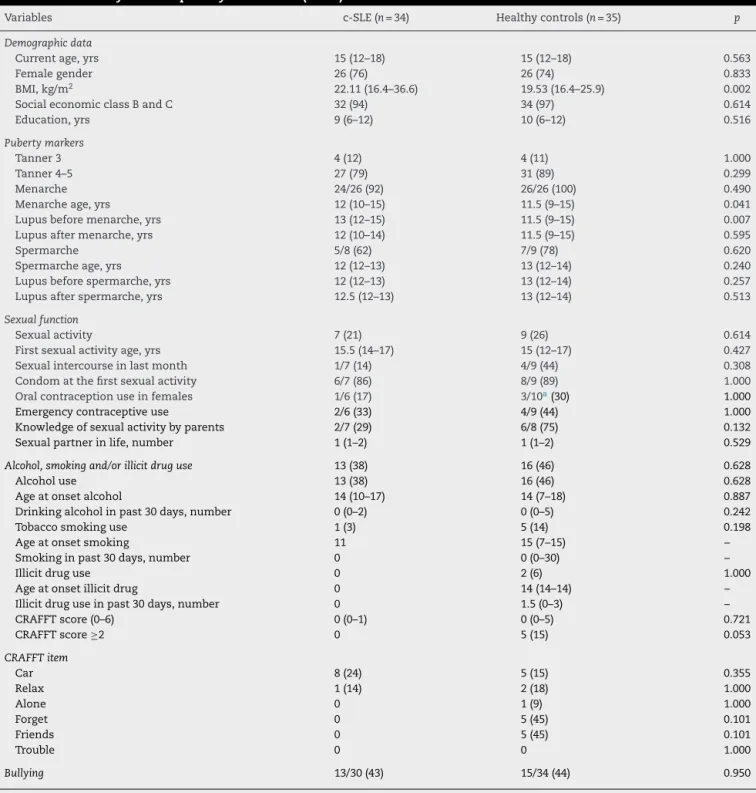
Table1includesdemographicdata,pubertymarkers, sex-ualfunction,alcohol,smokingandillicitdruguse,andbullying in c-SLE and controls. The median current age was simi-lar between c-SLE patients and controls [15 (12–18) vs. 15 (12–18)years,p=0.563],likewisethefrequencyoffemale gen-der(76% vs.74%,p=0.833).BMIwassignificantlyhigher in c-SLEpatientscomparedtocontrols[22.11(16.4–36.6)vs.19.53 (16.4–25.9)kg/m2,p=0.002].
Themedianofmenarcheagewassignificantlyhigherin c-SLEpatientscomparedtocontrols[12(10–15)vs.11.5(9–15) years,p=0.041],particularlyinthosethatlupushadoccurred beforemenarche [13 (12–15) vs. 11.5 (9–15) years, p=0.007] (Table1).
Thefrequenciesofalcohol,smokingand/orillicitdruguse werehighandsimilarinbothc-SLEpatientsandcontrols(38% vs.46%,p=0.628).Marijuanawasusedbytwohealthycontrols andnoneinc-SLEpatients(0%vs.6%,p=1.000).Themedian ofCRAFFTscorewasalikeinbothgroups[0(0–1)vs.0(0–5), p=0.721],whereasatrendoflowerfrequencyofCRAFFTscore ≥2wasevidencedinc-SLEpatientscomparedtocontrols(0% vs.15%,p=0.053).Bullyingwasreportedsimilarlyinthetwo groups(43%vs.36%,p=0.572)(Table1).
Furtheranalysisoflupuspatientsthatusedalcohol, smok-ing and/or illicitdrug compared tothose that didnot use these substances showed no differences in demographic data,pubertymarkers,sexualfunctionparameters, contra-ceptiveuse,historyofbullying,lupusclinicalmanifestations,
SLEDAI-2K,SLICC/ACR-DI,ESR,CRPandanti-dsDNA autoan-tibodies(p>0.05).Currentuseandcurrentdoseofprednisone, hydroxychloroquine,methotrexate,azathioprine,intravenous cyclophosphamideandmycophenolatemofetilwerealso sim-ilarinbothgroups(p>0.05).
NocorrelationswereevidencedbetweenCRAFFTscorein bothc-SLEandhealthycontrolsgroups(n=69)and:current age(p=0.249),ageofalcoholonset(p=0.800)andageonsetof sexualintercourse(p=0.297).
Discussion
Our study showedhigh frequenciesofearlyalcoholuse in adolescents with c-SLE and in healthy controls, despiteof a possiblelow riskforsubstance abuse/dependencein the formergroup.
The majoradvantageofthis study wasthe assessment ofastructuredquestionnairewithhightest–restest reliabil-itythatevaluatedsexualfunction,licitandillicitsubstance useandbullying.CRAFFTscore,whichisascreeningtoolfor high-riskalcoholordrugsuseinteenagers,wasalsoapplied.12 Furthermore,ahealthycontrolgroupwithsimilarage, gen-derandsocio-economicclasswasrelevant,sincethesedata were associated with bullying, alcohol and illicit drugs in adolescents.2,12–15However,themajorlimitationsofthisstudy werethesmallnumberofsubjectsrecruitedinonlyone Pedi-atricRheumaticservice,acrosssectionaldesignandnonuse ofastandardizedself-completionquestionnairefordifferent typesofbullying.4Inaddition,therewasnosamplesize cal-culationforthisstudy,whichdoesnotallowgeneralizingof theseresults,especiallyinaresearchthatwasbasedonlyon thequestionnaireandnotformedicaltestsoramoredetailed history.
Alcohol consumptionwas high in the present study,as expected in adolescents with c-SLE and healthy controls. Prevalence of alcohol use in adolescents varied from 23% to 68%, using distinct methodological procedures, such as questionnairesor structured interviews.14,16 Thisfinding is probablyrelatedtolow-costand easyaccesstoadolescents inourcountry,inspitetheeffortsofBrazilianhealthy pub-licpolicy.Theageofalcoholonsetwasalsoearlyinourc-SLE patients(14years),differentfromanationalsurveyperformed inBrazilianadolescents(15.8years).14
Incontrasttoalcoholintake,smokingandmarihuanawere rarelyusedbylupusandhealthyadolescents,probablydueto thepredominanceoffemales.Indeed,malegenderwas asso-ciatedwithanincreasedriskforillegaldruguse.14Theillicit orlicitdrugusedidnotinfluencesexualfunctionparameters andcontraceptiveuse,differentlyfromanotherstudy.3These substancesseemednottointerferewithdiseasemarkersand treatmentsinc-SLEpatients.
Table1–Demographicdata,pubertymarkers,sexualfunction,alcohol,smokingandillicitdruguse,andbullyingin childhood-onsetsystemiclupuserythematosus(c-SLE)andcontrols.
Variables c-SLE(n=34) Healthycontrols(n=35) p
Demographicdata
Currentage,yrs 15(12–18) 15(12–18) 0.563
Femalegender 26(76) 26(74) 0.833
BMI,kg/m2 22.11(16.4–36.6) 19.53(16.4–25.9) 0.002
SocialeconomicclassBandC 32(94) 34(97) 0.614
Education,yrs 9(6–12) 10(6–12) 0.516
Pubertymarkers
Tanner3 4(12) 4(11) 1.000
Tanner4–5 27(79) 31(89) 0.299
Menarche 24/26(92) 26/26(100) 0.490
Menarcheage,yrs 12(10–15) 11.5(9–15) 0.041
Lupusbeforemenarche,yrs 13(12–15) 11.5(9–15) 0.007
Lupusaftermenarche,yrs 12(10–14) 11.5(9–15) 0.595
Spermarche 5/8(62) 7/9(78) 0.620
Spermarcheage,yrs 12(12–13) 13(12–14) 0.240
Lupusbeforespermarche,yrs 12(12–13) 13(12–14) 0.257
Lupusafterspermarche,yrs 12.5(12–13) 13(12–14) 0.513
Sexualfunction
Sexualactivity 7(21) 9(26) 0.614
Firstsexualactivityage,yrs 15.5(14–17) 15(12–17) 0.427
Sexualintercourseinlastmonth 1/7(14) 4/9(44) 0.308
Condomatthefirstsexualactivity 6/7(86) 8/9(89) 1.000
Oralcontraceptionuseinfemales 1/6(17) 3/10a(30) 1.000
Emergencycontraceptiveuse 2/6(33) 4/9(44) 1.000
Knowledgeofsexualactivitybyparents 2/7(29) 6/8(75) 0.132
Sexualpartnerinlife,number 1(1–2) 1(1–2) 0.529
Alcohol,smokingand/orillicitdruguse 13(38) 16(46) 0.628
Alcoholuse 13(38) 16(46) 0.628
Ageatonsetalcohol 14(10–17) 14(7–18) 0.887
Drinkingalcoholinpast30days,number 0(0–2) 0(0–5) 0.242
Tobaccosmokinguse 1(3) 5(14) 0.198
Ageatonsetsmoking 11 15(7–15) –
Smokinginpast30days,number 0 0(0–30) –
Illicitdruguse 0 2(6) 1.000
Ageatonsetillicitdrug 0 14(14–14) –
Illicitdruguseinpast30days,number 0 1.5(0–3) –
CRAFFTscore(0–6) 0(0–1) 0(0–5) 0.721
CRAFFTscore≥2 0 5(15) 0.053
CRAFFTitem
Car 8(24) 5(15) 0.355
Relax 1(14) 2(18) 1.000
Alone 0 1(9) 1.000
Forget 0 5(45) 0.101
Friends 0 5(45) 0.101
Trouble 0 0 1.000
Bullying 13/30(43) 15/34(44) 0.950
Theresultsarepresentedinn(%)andmedian(range). CRAFFT,car,relax,alone,forget,friends,trouble;screeningtest.
adolescentsbescreenedforbothhigh-risksexualbehavior, aswellasfordrugsandalcoholuseaspartofroutinevisit.17
Of note, bullying is unwished, repeated and aggressive behaviorinschooladolescentsthatinvolvesarealorperceived powerimbalance.Adolescentswithchronicdiseaseshavean increasedriskofpeervictimization,reinforcingtherelevance ofthequalityofaninclusiveeducationsystem.4Furthermore, bullyingmaycausehigherratesofdepressionandanxiety,18 andmayinfluenceadherenceinpatients.19Futureprospective study,recruitinglargersampleandevaluatingtheseaspects, willbenecessaryinc-SLEpopulation.
We have confirmed our previous observations of late menarche age20,21 and normal spermarche age22 in c-SLEpatients compared with healthy Brazilian adolescents. Endocrine-disruptingeffectsofalcoholandsmokingusemay influencepubertaldevelopment,23 howeverthisaspectwas notevidencedinthepresentstudy.
Inconclusion,thisstudyshowedhighfrequenciesofearly alcoholuseinlupusadolescentsandhealthycontrols,with apossiblelowriskforsubstanceabuse/dependenceinc-SLE patients.Therefore,ourstudyemphasizedaroutinescreening forsubstanceuseinallc-SLEadolescents.24
Funding
ThisstudywassupportedbygrantsfromFundac¸ãodeAmparo àPesquisadoEstadodeSãoPaulo (FAPESP2011/12471-2to CAS), Conselho Nacional de Desenvolvimento Científico e Tecnológico(CNPq303422/2015-7-1AtoCAS),Federico Foun-dation(toCAS),andNúcleodeApoioàPesquisa“Saúdeda Crianc¸aedoAdolescente”daUSP(NAP-CriAd)toCAS.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
Acknowledgements
OurgratitudetoUlyssesDoria-Filhoforthestatisticalanalysis. WethankDr.J.R.KnightandDr.P.SchramofBostonChildren’s Hospital,Mass,USA,forsupplyingthePortugueseversionof CRAFFTscreen(CEASER)instrument.
r
e
f
e
r
e
n
c
e
s
1. SilvaCA,AvcinT,BrunnerHI.Taxonomyforsystemiclupus erythematosuswithonsetbeforeadulthood.ArthritisCare Res(Hoboken).2012;64:1787–93.
2. AtilolaO,StevanovicD,BalharaYP,AvicennaM,KandemirH, KnezR,etal.Roleofpersonalandfamilyfactorsinalcohol andsubstanceuseamongadolescents:aninternationalstudy withfocusondevelopingcountries.JPsychiatrMentHealth Nurs.2014;21:609–17.
3. MialonA,BerchtoldA,MichaudPA,GmelG,SurisJC.Sexual dysfunctionsamongyoungmen:prevalenceandassociated factors.JAdolescHealth.2012;51:25–31.
4.SentenacM,GavinA,GabhainnSN,MolchoM,DueP, Ravens-SiebererU,etal.Peervictimizationandsubjective healthamongstudentsreportingdisabilityorchronicillness in11Westerncountries.EurJPublicHealth.2013;23:421–6.
5.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum.1997; 40:1725.
6.KnightJR,SchramP.PortugueseversionofCRAFFTscreen (CEASER);2014.Availableat:http://www.ceasar-boston.org/ CRAFFT/pdf/CRAFFT Portuguese.pdf[accessed17.07.14]. 7.KnightJR,SherrittL,ShrierLA,HarrisSK,ChangG.Validityof
theCRAFFTsubstanceabusescreeningtestamongadolescent clinicpatients.ArchPediatrAdolescMed.2002;156:
607–14.
8.ABEP(Associac¸a˜oBrasileiradeEmpresasdePesquisa)2008. Availableat:www.abep.org–[email protected][accessed 17.07.14].
9.MarshallJC,TannerJM.Variationsinpatternsofpubertal changesinboysandgirls.ArchDisChild.1970;45: 13–23.
10.GladmanDD,Iba ˜nezD,UrowitzMB.Systemiclupus erythematosusdiseaseactivityindex2000.JRheumatol. 2002;29:288–91.
11.GladmanD,GinzlerE,GoldsmithC,FortinP,LiangM,Urowitz M,etal.Thedevelopmentandinitialvalidationofthe SystemicLupusInternationalCollaboratingClinics/American CollegeofRheumatologydamageindexforsystemiclupus erythematosus.ArthritisRheum.1996;39:363–9.
12.MenezesAH,DalmasJC,ScarinciIC,MacielSM,CardelliAA. Factorsassociatedwithregularcigarettesmokingby adolescentsfrompublicschoolsinLondrina,Paraná,Brazil. CadSaudePublica.2014;30:774–84.
13.PatrickME,WightmanP,SchoeniRF,SchulenbergJE. Socioeconomicstatusandsubstanceuseamongyoung adults:acomparisonacrossconstructsanddrugs.JStud AlcoholDrugs.2012;73:772–82.
14.MadrugaCS,LaranjeiraR,CaetanoR,PinskyI,ZaleskiM,Ferri CP.Useoflicitandillicitsubstancesamongadolescentsin Brazil–anationalsurvey.AddictBehav.2012;37:
1171–5.
15.TippettN,WolkeD.Socioeconomicstatusandbullying: ameta-analysis.AmJPublicHealth.2014;104:
e48–59.
16.BarbosaFilhoVC,CamposWD,LopesAdaS.Prevalenceof alcoholandtobaccouseamongBrazilianadolescents:a systematicreview.RevSaudePublica.2012;46:
901–17.
17.LevySJ,KokotailoPK,CommitteeonSubstanceAbuse. Substanceusescreening,briefintervention,andreferralto treatmentforpediatricians.Pediatrics.2011;128:
e1330–40.
18.CalveteE.Emotionalabuseasapredictorofearly maladaptiveschemasinadolescents:contributionstothe developmentofdepressiveandsocialanxietysymptoms. ChildAbuseNegl.2014;38:735–46.
19.JulianLJ,YelinE,YazdanyJ,PanopalisP,TrupinL,CriswellLA, etal.Depression,medicationadherence,andservice utilizationinsystemiclupuserythematosus.Arthritis Rheum.2009;61:240–6.
20.FebronioMV,PereiraRM,BonfaE,TakiutiAD,PereyraEA, SilvaCA,etal.Inflammatorycervicovaginalcytologyis associatedwithdiseaseactivityinjuvenilesystemiclupus erythematosus.Lupus.2007;16:430–5.
22.VecchiAP,BorbaEF,BonfáE,CocuzzaM,PieriP,KimCA,etal. Penileanthropometryinsystemiclupuserythematosus patients.Lupus.2011;20:512–8.
23.PeckJD,PeckBM,SkaggsVJ,FukushimaM,KaplanHB. Socio-environmentalfactorsassociatedwithpubertal developmentinfemaleadolescents:theroleofprepubertal
tobaccoandalcoholuse.JAdolescHealth.2011;48: 241–6.
24.BrittoMT,RosenthalSL,TaylorJ,PassoMH.Improving rheumatologists’screeningforalcoholuseandsexual activity.ArchPediatrAdolescMed.2000;154: