SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Functional
and
clinical
results
achieved
in
congenital
clubfoot
patients
treated
by
Ponseti’s
technique
夽
Pedro
Augusto
Jaqueto
∗,
Guilherme
Salgado
Martins,
Fernando
Saddi
Mennucci,
Cintia
Kelly
Bittar,
José
Luís
Amim
Zabeu
PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),HospitaleMaternidadeCelsoPierro,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16September2015 Accepted6November2015 Availableonline22September2016
Keywords:
Footdeformities Congenitalabnormalities Clubfoot
Treatmentoutcome
a
b
s
t
r
a
c
t
Objectives: Toanalyzeandevaluatefunctionalandclinicalresultsinpatientswithcongenital clubfoottreatedwithPonseti’stechnique.
Methods:Thisstudyevaluated31patientsdiagnosedwith51congenitalclubfeet,treated betweenApril2006andSeptember2011withPonseti’stechnique.Thepatientswhodid not achieve anequinus correctionwith manipulationweretreated withAchilles teno-tomy.Ananteriortibialtendontransferwasperformedinpatientswhomaintainedresidual adduction.AllplastersweremadebyfellowsandsupervisedbyAnkleandFootChiefs.The techniquewasperformedwithouttheneedforphysicaltherapists,orthotics,andplaster technicians.Patientsweresubmittedtopre-andpost-treatmentexaminationandevaluated underPirani’sclassification.
Results:Malepatientshadanincreasedincidenceandtherightsidewasmoreaffected, whilebilateralinvolvementwasobservedin64.5%ofthecases.Themeannumberofcast changeswas5.8,andAchillestenotomywasnecessaryin26patients.Thereweresignificant deformityimprovementsin46ofthe51treatedfeet(90.2%);Pirani’smeanscoreimproved from5.5to3.6aftertreatment.
Conclusion: ThePonsetimethodwaseffectiveinbothfunctionalandclinicalevaluationof patients,withsignificantstatisticalrelevance(p=0.0001),withasuccessrateof90.2%and meanimprovementinthePirani’sindexof65.5%.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheHospitaleMaternidadeCelsoPierro,PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),Campinas, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](P.A.Jaqueto). http://dx.doi.org/10.1016/j.rboe.2016.09.004
Resultados
funcionais
e
clínicos
alcanc¸ados
em
pacientes
com
pé
torto
congênito
tratados
pela
técnica
de
Ponseti
Palavras-chave:
Deformidadesdopé Anormalidadescongênitas Pétorto
Resultadodotratamento
r
e
s
u
m
o
Objetivos: Analisareavaliarosresultadosfuncionaiseclínicosempacientescompétorto congênitotratadospelatécnicadePonseti.
Métodos: Oestudoincluiu31pacientesdiagnosticadoscom51péstortoscongênitos, trata-dosentreabrilde2006asetembrode2011pelatécnicadePonseti.Ospacientesquenão alcanc¸aramacorrec¸ãodoestadoequinocommanipulac¸ãoforamtratadoscomtenotomia doAquiles.Umatransposic¸ãodotendãotibialanteriorfoifeitanospacientesque man-tiveramumaaduc¸ãoresidual.Todososgessosforamfeitosporresidentesesupervisionados peloschefesdeTornozeloePé.Atécnicafoiaplicadasemanecessidadedefisioterapeutas outécnicosdegesso.Ospacientesforamsubmetidosaexameantesedepoisdotratamento eavaliadosdeacordocomaescaladePirani.
Resultados: Ospacientesdosexomasculinoapresentaramumaumentodeincidênciaeo ladodireitofoiomaisafetado,enquantoqueoacometimentobilateralfoiobservadoem 64,5%doscasos.Amédiademudanc¸asdegessofoide5,8eatenotomiadotendãode Aquilesfoinecessáriaem26pacientes.Houvemelhoriassignificativasdasdeformidades em46dos51dospéstratados(90,2%),aescaladePiranipontuouumavanc¸onamédiade 5,5para3,6apósotratamento.
Conclusão:OmétododePonsetifoieficaznasavaliac¸õesfuncionaiseclínicasdospacientes, comumarelevânciaestatísticasignificante(p=0,0001),comumataxadesucessode90,2% eumavanc¸onaescaladePiranide65,5%.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Congenitalclubfoot(CCF)isadeformitycharacterizedbya complex misalignmentofthe feet,involving bothsoft and bonyparts,withvarusandequinusdeformityofthehindfoot (talipesequinovarus),aswellascavusandadductionofthe midfootandforefoot.1–5Itsincidenceisapproximatelyonein every1000livebirths,withapredominanceofmalesatthe ratioof2:1,andwithbilateralinvolvementin50%ofcases.6,7 CCFhasawidevarietyofclinicalexpressions;some classi-ficationsconsideronlytheclinicalaspects,whileothersalso takeradiographicfeaturesintoaccount.Todate,no classifica-tionhasprevailed.Nonetheless,theliteratureindicatesthat themostusedclassificationisthePirani8scale,whichis sim-plerandmorerecent.
The first reference to CCF treatment was described by Hippocrates (400 BC), who mentioned repeated and gentle manipulations,followedbyimmobilizations.Guerinisknown asthefirstphysiciantouseplasterin1836.Aroundthe20th century,newtechnologiesweredevelopedtosupportthese corrections,suchastheThomasdevice.In1932,Kite9 advo-catedsmoothandrepeatedmanipulationsfollowedbyplaster immobilization, in an attempt to prevent forced and pro-longedcorrections.Thiscombinationbecameknownasthe KitemethodforCCFtreatment.10
Around 1940, Ponseti, after several in-depth studies of thepathological andfunctional anatomyofthe CCF, devel-opedandperfectedhistreatmenttechnique.Ponsetidescribed detailsaboutmaneuversandplasterimmobilization,aswell asfollow-up afterAchillestendonresection, guidedbythe
patient’sage.Healsoidentifiedandpublishedthemost com-monerrorsintreatmentmanagementatthetime.11Themost importantadvantageofthePonsetimethodisthedegreeof mobility achievedattheend oftreatmentwhencompared withothertechniques.10
Hismethodisbasedongentle manipulationsandserial plasterchanges,percutaneousresectionoftheAchilles ten-don, and the use of a foot abduction brace.1,4,12 It has become the preferred method for treating idiopathic CCF in many countries.5,13,14 In the past decade,with its wide acceptance, this method has been extended to be used in older children15,16; complex and refractoryfeet17; recur-rent feet,18 including recurrence after extensive surgical decompression19;relapsedfeet,withouttakingintoaccount non-idiopathiccasessuchasmyelomeningocele,20,21and dis-tal arthrogryposis.22,23 Thefoundationofthe manipulation techniqueconsistsofcorrectingdeformitiesthroughplastic changeofcontractedandshortenedelements,whichhavea highelasticcapacityinchildren,especiallyinthefirstyearof life.Ponsetiadvocatedthatclinicalandphysicalexaminations areparamount;hedidnotvalueimagingexamsinhis assess-ments.Otherauthors,suchasPiranietal.,24usedmagnetic resonanceimaging(MRI)toconfirmthatthePonsetimethod, in additionto correctingthe relationship betweenthe foot bones,alsopromotedmechanicalstimulithatwereimportant andplayedaroleinboneremodeling.
Ponsetitechnique isthat the treatment lasts betweentwo andfourmonths,andmanipulationswithorthosesforfour years,28 while Kites’ technique lasts for approximately 22 months. Herzenberg et al.29 have reported that, with the Ponseti method, only 3% of cases needed posteromedial decompressionsurgery,vs.94%ofcasesinother contempo-rarytechniques.
Thisstudy wasdesignedtoevaluatethe functional and clinicaloutcome ofpatientswithCCF whowere treatedby thePonsetitechnique.
Methods
Aretrospective studyina universityhospitaldiagnosed31 patientswithidiopathicCCFtreatedwiththe Ponseti tech-nique in the Orthopedics Clinic between April 2006 and September2011.Patientspresentingrigidfeetwereexcluded, andthosewithflexiblefeetwereincluded.
Threenewbornswerediagnosedatanotherhospitalbefore screeninginthishospital;sixnewbornsabandonedtreatment. Patientswere identified and selectedfrom the database oftheorthopedicsdepartment;afterselection,theirmedical informationandrecordswerecollected.Datawerethoroughly analyzedusingthePiraniscaletodetectprogressintheuseof thePonsetitechnique.
Patientswereclinicallydiagnosedandtreatedbythefoot andanklegroup,whichalsoanalyzedthe resultsusingthe Piraniscale.Thediagnosisisbasedonclinicaldeformities pre-sentedbypatientsatthetimeofevaluation.Characteristicsof thedeformitiesarecavus,adductus,varus,andequinus.
Severalvariableswereincluded:gender,age,familyhistory, affectedfoot,earlydiagnosis,treatmentonsetandduration, associateddeformities,numberofplasterchanges,needfor tenotomyand type ofanesthesia,Pirani scoresbefore and aftertreatment,aswellasrecurrenceandfollow-uptime.
Clubfoot hasdifferent expressions. There are classifica-tionsthatconsideronlyclinicalaspectsandothersthatalso takeinto account the radiographiccharacteristics.To date, noseverityclassificationsystemhasprevailed.However,the mainclassificationisthePiraniscale,whichissimplerand morerecent,butisstillinthevalidationphase.Itisbasedon asimpleclassificationsystem,consistingofthreevariablesin thehindfootandthreeinthemidfoot.Eachvariablecanbe markedfromzerotoone.
Inorder toassess the resultsobtainedwiththe Ponseti technique,thePiraniscalewasappliedbeforeandafterthe proposedtreatment.9Statisticalanalysiswasdonebya qual-ified practitioner inthe field.TheWilcoxon test forpaired samples(p-value≤0.0001)wasused.
Results
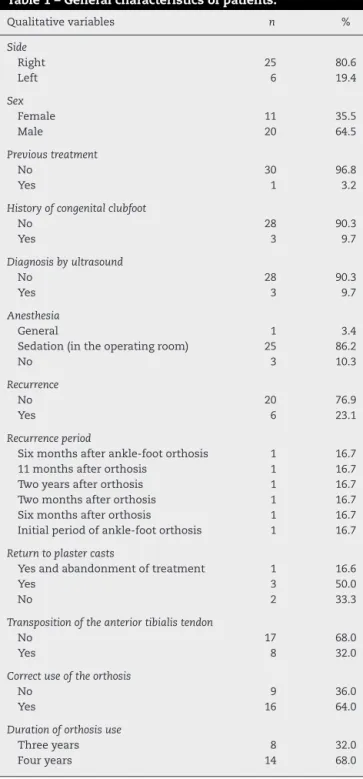
Ofthe 31 patients evaluated, 20 (64.5%)were male and 11 (35.5%) were female. Twenty patients (64.5%) had bilateral involvementand 11 (35.5%), unilateral. Theright side was affectedin25patients(80.6%),andtheleftside,insix(19.4%). Thirtypatients(96.8%)hadnotpreviouslyreceivedtreatment, whileonehadundergoneprevioustreatment(3.2%). Twenty-eightpatients(90.3%)hadnoassociateddeformity,andthree
Table1–Generalcharacteristicsofpatients.
Qualitativevariables n %
Side
Right 25 80.6
Left 6 19.4
Sex
Female 11 35.5
Male 20 64.5
Previoustreatment
No 30 96.8
Yes 1 3.2
Historyofcongenitalclubfoot
No 28 90.3
Yes 3 9.7
Diagnosisbyultrasound
No 28 90.3
Yes 3 9.7
Anesthesia
General 1 3.4
Sedation(intheoperatingroom) 25 86.2
No 3 10.3
Recurrence
No 20 76.9
Yes 6 23.1
Recurrenceperiod
Sixmonthsafterankle-footorthosis 1 16.7
11monthsafterorthosis 1 16.7
Twoyearsafterorthosis 1 16.7
Twomonthsafterorthosis 1 16.7
Sixmonthsafterorthosis 1 16.7
Initialperiodofankle-footorthosis 1 16.7
Returntoplastercasts
Yesandabandonmentoftreatment 1 16.6
Yes 3 50.0
No 2 33.3
Transpositionoftheanteriortibialistendon
No 17 68.0
Yes 8 32.0
Correctuseoftheorthosis
No 9 36.0
Yes 16 64.0
Durationoforthosisuse
Threeyears 8 32.0
Fouryears 14 68.0
(9.7%)hadapositivefamilyhistoryofCCF.Previousdiagnoses weremadebyultrasoundinthreepatients.Duetothe socio-economicstatusofpatients,manydidnotreceiveadequate explanationforanearlydiagnosis.Manyofthemwerefrom
Table2–Ageofthepatientandfollow-upduration.
n Medium Minimum Maximum
Ageatfirst consultation (inmonths)
31 17.9 2.9 144.0
Follow-upperiod (inmonths)
Table3–Results.
n Mean Medium Minimum Maximum
Numberofcastchangesuntiltenotomy 31 5.8 6.0 3.0 9.0
Individualmeasurementbyaffectedfoot n Mean Medium Minimum Maximum
InitialPiraniscale 51 5.5 5.5 3.5 6.0
FinalPiraniscale 51 3.6 3.5 3.0 5.0
other states, which have low-quality ultrasound machines
andinexperiencedexaminers.TenotomyoftheAchilles
ten-donwas necessaryin26 patients(84%).Themeannumber
ofplasterchangestotenotomywas5.8(rangebetween4and 9).Recurrencewasobservedinsix(23.1%)ofthe26patients. Duringfollow-up,sixpatientsabandonedtreatment(19.4%, Table1).Meanageatinitialevaluationwas17.9months(range: 7daysto12years).Themeanfollow-uptimewas30.2months (range:4–50),asshowninTable2.Improvementsofthe defor-mitieswereobservedin46ofthe51treatedfeet(90.2%).The initialPiraniscoreindividualizedbyside(n=51)was5.5(range: 4–6); aftertreatment,the mean was3.6(range: 3–5).These resultshadp-values<0.0001(Table3).
Discussion
Althoughthestudy,theresearchofmedicalrecords,clinical diagnosis,andtreatmentwereconductedinanorderly man-ner,thenumberofpatientsatthepresentationoftheresults wasstilllow,representingonlyasmallportionofallcasesof clubfoottreatedinthisservice.
Nonetheless,familyunderstandingofthetreatmentandits difficulties,whetherphysicalorpsychological,werestrongly emphasizedthroughguidancetoparentsandillustrated book-lets. Itwas observedthat somefamilies had difficulties in understandingtheimportanceoftreatmentanditsgoals.In thesecases,morecarefulmonitoringwasnecessary,aiming tocompletethetreatmentatthedesiredlevels.
Idiopathicclubfootwasdefinedasthosethatdidnothave adefined etiology,and neurologicalclubfootas those with acentral,spinal,orperipheraldisease.Thesepatientswere newborns and presented the hormone relaxin. There was improvementinthestandingposition,butwithpartial recur-rence.
Genderandthepredominanceoftheaffectedsidewerein agreementwiththeliterature,intheratioof2:1betweenmen andwomen,6,7andtherightsidewasthemostaffected.6,7,30 However,thepresentstudyobservedahigherbilateral inci-dence(64.5%)thanthatreportedintheliterature(50%).6,7
Tenotomy of the Achilles tendon was necessary in 26 patients(84%),whichisinagreementwiththecurrent litera-ture(between70%and90%).1,4,13,15,30Inthepresentstudy,the meannumberofplasterchangesbeforetenotomy5,8wassix, whichisalsoinagreementwiththeliterature.1,4,12,13,15,25,26
Recurrencewasobservedinsixpatients.Fourcaseswere idiopathicrecurrences,andtworecurrenceswereassociated withincorrectuseoftheorthosis.
Inallfouridiopathicrecurrencecases,atranspositionof theanteriortibialtendontothethirdcuneiformand percuta-neoustranspositionoftheAchillestendonwasperformed.Six
weeksaftersurgery,theankleandfootorthosiswasapplied, beingusedforsixmonths.
Eightrelapsedfeetwithoutpriortreatmentwereobserved inpatients olderthan 4years.In suchcases,transposition oftheanteriortibialtendonwasperformedaftertheplaster changes,followedbysixmonthsofankleandfootorthosis insteadoftheDenisBrownebar,asthesepatientswerealready walking.Recurrenceofdeformityoccurredinonecase,andan externalcircularfixatorwasused.
The success rate of the present study was 90.2%, very closetothosecitedintheliteratureandinPonseti’soriginal article.4,13,15,25,26 Functionaland clinicaladvanceswerealso observedinthepresenttreatedpatients,witha90.2%success rate(46ofthe51feettreated)andameanimprovementinthe Piraniscaleof65.5%(adecreasefrom5.5to3.6).
Conclusion
The Ponsetimethodwas effectivein thetreatment ofCCF regardingfunctionalandclinicaloutcomes.Furthermore,its effectivenesswas provenandmeasured bythestatistically significantPiraniscaleimprovementsdescribedinthepresent study.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PonsetiIV.Congenitalclubfoot:fundamentalsoftreatment. Oxford:OxfordUniversityPress;1996.
2.SongHR,CarrollNC,NeytJ,CarterJM,HanJ,D’AmatoCR. Clubfootanalysiswiththree-dimensionalfootmodels.J PediatrOrthopB.1999;8(1):5–11.
3.CahuzacJP,BauninC,LuuS,EstivalezesE,SalesdeGauzyJ, HobathoMC.Assessmentofhindfootdeformityby three-dimensionalMRIininfantclubfoot.JBoneJointSurg Br.1999;81(1):97–101.
4.PonsetiIV.Treatmentofcongenitalclubfoot.JBoneJointSurg Am.1992;74(3):448–54.
5.DobbsMB,GurnettCA.Updateonclubfoot:etiologyand treatment.ClinOrthopRelatRes.2009;467(5):1146–53. 6.LochmillerC,JohnstonD,ScottA,RismanM,HechtJT.
Geneticepidemiologystudyofidiopathictalipesequinovarus. AmJMedGenet.1998;79(2):90–6.
7.StewartSF.Club-foot:itsincidence,cause,andtreatment.An anatomical–physiologicalstudy.JBoneJointSurgAm. 1951;33(3):577–90.
Kampala:Global-HELPOrganization;2008.Availablein: https://global-help.org/publications/books/help ponsetiuganda.pdf.
9. KiteJH.Principlesinvolvedinthetreatmentofcongenital clubfoot.JBoneJointSurgAm.1939;21(3):595–606. 10.SizínioHK,BarrosFilhoTEP,XavierR,PardiniJúniorA.
Ortopediaetraumatologia:princípioseprática.PortoAlegre: Artmed;2009.
11.KiteJH.Principlesinvolvedinthetreatmentofcongenital clubfoot.ClinOrthopRelatRes.1972;(84):4–8.
12.PonsetiIV.Commonerrorsinthetreatmentofcongenital clubfoot.IntOrthop.1997;21(2):137–41.
13.PonsetiIV,SmoleyEN.Congenitalclubfoot:theresultsof treatment.JBoneJointSurgAm.1963;45(2):
261–344.
14.BorN,CoplanJA,HerzenbergJE.Ponsetitreatmentfor idiopathicclubfoot:minimum5-yearfollowup.ClinOrthop RelatRes.2009;467(5):1263–70.
15.DobbsMB,GordonJE,SchoeneckerPL.Absentposteriortibial arteryassociatedwithidiopathicclubfoot.Areportoftwo cases.JBoneJointSurgAm.2004;86(3):599–602.
16.MorcuendeJA,DolanLA,DietzFR,PonsetiIV.Radical reductionintherateofextensivecorrectivesurgeryfor clubfootusingthePonsetimethod.Pediatrics.
2004;113(2):376–80.
17.SpiegelDA,ShresthaOP,SitoulaP,RajbhandaryT,Bijukachhe B,BanskotaAK.Ponsetimethodforuntreatedidiopathic clubfeetinNepalesepatientsfrom1to6yearsofage.Clin OrthopRelatRes.2009;467(5):1164–70.
18.PonsetiIV,ZhivkovM,DavisN,SinclairM,DobbsMB, MorcuendeJA.Treatmentofthecomplexidiopathicclubfoot. ClinOrthopRelatRes.2006;451:171–6.
19.BorN,HerzenbergJE,FrickSL.Ponsetimanagementof clubfootinolderinfants.ClinOrthopRelatRes. 2006;444:224–8.
20.NogueiraMP,EyBatlleAM,AlvesCG.Isitpossibletotreat recurrentclubfootwiththePonsetitechniqueafter
posteromedialrelease?Apreliminarystudy.ClinOrthopRelat Res.2009;467(5):1298–305.
21.ChenRC,GordonJE,LuhmannSJ,SchoeneckerPL,DobbsMB. Anewdynamicfootabductionorthosisforclubfoot
treatment.JPediatrOrthop.2007;27(5):522–8.
22.GerlachDJ,GurnettCA,LimpaphayomN,AlaeeF,ZhangZ, PorterK,etal.EarlyresultsofthePonsetimethodforthe treatmentofclubfootassociatedwithmyelomeningocele.J BoneJointSurgAm.2009;91(6):1350–9.
23.vanBosseHJ,MarangozS,LehmanWB,SalaDA.Correctionof arthrogrypoticclubfootwithamodifiedPonsetitechnique. ClinOrthopRelatRes.2009;467(5):1283–93.
24.PiraniS,ZeznikL,HodgesD.Magneticresonanceimaging studyofthecongenitalclubfoottreatedwiththePonseti method.JPediatrOrthop.2001;21(6):719–26.
25.BoehmS,LimpaphayomN,AlaeeF,SinclairMF,DobbsMB. EarlyresultsofthePonsetimethodforthetreatmentof clubfootindistalarthrogryposis.JBoneJointSurgAm. 2008;90(7):1501–7.
26.LaavegSJ,PonsetiIV.Long-termresultsoftreatmentof congenitalclubfoot.JBoneJointSurgAm.1980;62(1):23–31. 27.CooperDM,DietzFR.Treatmentofidiopathicclubfoot.A
thirty-yearfollow-upnote.JBoneJointSurgAm. 1995;77(10):1477–89.
28.SegevE,KeretD,LokiecF,YavorA,WientroubS,EzraE,etal. EarlyexperiencewiththePonsetimethodforthetreatment ofcongenitalidiopathicclubfoot.IsrMedAssocJ.
2005;7(5):307–10.
29.HerzenbergJE,RadlerC,BorN.Ponsetiversustraditional methodsofcastingforidiopathicclubfoot.JPediatrOrthop. 2002;22(4):517–21.