r e v b r a s r e u m a t o l . 2017;57(2):182–184
ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Salivary

2-microglobulin
positively
correlates
with
ESSPRI
in
patients
with
primary
Sjögren’s
syndrome
A
2-microglobulina
salivar
se
correlaciona
positivamente
com
o
ESSPRI
em
pacientes
com
síndrome
de
Sjögren
primária
Felipe
Garza-García
a,
Guillermo
Delgado-García
a,∗,
Mario
Garza-Elizondo
b,
Luis
Ángel
Cece ˜nas-Falcón
c,
Dionicio
Galarza-Delgado
a,b,
Janett
Riega-Torres
b aUniversidadAutónomadeNuevoLeón,HospitalUniversitario,DepartamentodeMedicinaInterna,Monterrey,MexicobUniversidadAutónomadeNuevoLeón,HospitalUniversitario,ServiciodeReumatología,Monterrey,Mexico
cUniversidadAutónomadeNuevoLeón,HospitalUniversitario,ServiciodeAnatomíaPatológica,Monterrey,Mexico
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20June2016 Accepted27September2016 Availableonline14December2016
PrimarySjögren’ssyndrome(pSS)isasystemicautoimmune disorderlargelydistinguishedbylymphocyticexocrinopathy.1 Salivaryand lachrymalglandsare mainlyimpaired inpSS. Salivaisthereforeconsideredanoptimalbiologicalfluidthat closelyreflectstheunderlyingautoimmuneexocrinopathy.1,2 For instance, in those with pSS, 2-microglobulin (B2M) is increased in whole saliva.2 This protein is significantly correlated with lymphocytic infiltration in labial salivary glands.3 The EULAR Sjögren’s syndrome Patient Reported Index(ESSPRI)isapatient-centered measureofsymptoms. This index has been recently shown to be valid, reliable and sensitive tochange in a largecohort of patients with pSS.1TheESSPRIcorrelatedsignificantlywithserumB2Min patients with pSS.4 However, serum and salivary levels of B2Mwerenotcorrelatedinapreviousstudy.5Itiscurrently unknownwhethertheESSPRIisalsocorrelatedwithsalivary
∗ Correspondingauthor.
E-mails:[email protected],[email protected](G.Delgado-García).
B2MinthosewithpSS.Thisisofparticularimportancesince, if thesetwoparameters areindeedassociated,atreatment whichcould decreaseinflammatoryactivitywould improve the patients’symptoms,and alsobecausethe treatmentof chronicdiseases finallyaimstoimprove qualityoflifeand patient-perceivedhealthstatus.6Duetotheaboveissues,this studywasconducted.SalivaryB2Mwasfurthersubanalysed according to the patient-acceptable symptom state (PASS). A cut-off value for salivary B2M to distinguish those who were abovethe thresholdof unsatisfactorysymptom state (ESSPRI≥5)wasalsodetermined.
Inthis observationalstudy,adultpatients(≥18-year-old) with pSSwere enrolled.Thosewithhistory ofHIV, hepati-tis Band C,head and neck radiation therapy, sarcoidosis, amyloidosis, chronic kidney disease, lymphoma, or multi-plemyelomawereexcluded.pSSwasdiagnosedaccordingto
http://dx.doi.org/10.1016/j.rbre.2016.11.001
rev bras reumatol.2017;57(2):182–184
183
theAmericanCollegeofRheumatology(ACR)/Sjögren’s Inter-nationalCollaborativeClinicalAlliance(SICCA)criteria.7 All patientscompletedthe ESSPRI.Thisindexisameanscore of0–10numericalscales forpain, fatigueanddryness fea-tures(includingoral,ocularandglobaldryness).1PASSwas definedasthevaluebeyondwhichpatientsconsider them-selveswell(i.e.,ESSPRI<5).6Thedegreeofhistopathological changewasassessedusingthegradingstandardforlabial sali-varyglandbiopsy.8Writteninformedconsentwasobtained fromall patients, andthe studywas approvedbythe local ethicscommittee.
Ourstudyprotocolwassimilartothatdescribedpreviously byCastroetal.5Salivasampleswerecollectedover15minby passivespittinginto containers.Unstimulatedwhole saliva samples were centrifuged at 14,000×g for 20min at +4◦C priortoassaying.B2Mwasdeterminedbyanenzyme-linked immunosorbentassay (Abcam,Cambridge, UK) and results were expressed as nanograms per milliliter (ng/mL). This assaywasperformedaccordingtothemanufacturer’s instruc-tionmanual.
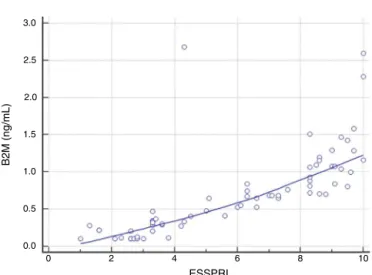
Normality of data distribution was assessed using the Shapiro–Wilktest.Themeasurementofthestrength ofthe association between the variables was explored using the Kendall’s correlationcoefficient. Continuous variables were comparedbetweengroupswiththeMann–WhitneyUtest.A receiveroperatingcharacteristic(ROC)curvewasgeneratedto determinethecutoffvalueintheB2Mwiththehighestlevelof accuracyinidentifyingpatientswithunsatisfactorysymptom state(ESSPRI≥5).Sensitivityandspecificitywerethus calcu-lated.Unless indicatedotherwise, all resultsare expressed asmean±standarddeviationormedian(interquartilerange). StatisticalanalyseswereconductedusingSigmaStat(v.3.5, Erkrath,Germany)orMedCalc (v.14.12.0,Ostend,Belgium), andap-valuebelow0.05(p<0.05)wasconsideredsignificant. Weincluded71consecutivefemalepatientswithpSSaged 53.05±12.19years.Theyhad siccasyndromefor48(24–81) months.Inourpatients,themedianESSPRIwas6.3(3.3–8.6), whilethemedianB2Mwas0.671(0.284–1.072)ng/mL.A signifi-cantpositivecorrelationbetweenESSPRIandsalivaryB2Mwas found(0.759,95%CI0.656–0.837,p<0.0001)(Fig.1).Thedegree ofhistopathologicalchangewasnotsignificantlycorrelated withsalivaryB2M(0.0485,95%CI−0.123to0.237,p=0.55).Data werethensubanalysedintoPASS(n=28)andnon-PASSgroups (n=43).SalivaryB2Mwascomparativelyhigherinthosewho were above the thresholdofunsatisfactory symptom state (0.878[0.682–1.263]vs0.219[0.10–0.324]ng/mL,p<0.0001).The ROCcurveanalysisforsalivaryB2Mshowedanareaunderthe curveof0.965(95%CI0.891–0.994,p<0.0001)withanoptimal cutoffvalueof0.472ng/mL(Fig.2).Sensitivityandspecificity were97.67%and96.30%,respectively.
B2M isanonglycosylated low-molecular-weightprotein, which is part of the major histocompatibility complex I and is particularlyexpressed in lymphocytes. This protein is regulated by interferon and, in turn, this pathway acti-vation is thought to be related to the disease progression ofpSS.9,10 TheincreasedexpressionofB2Minwholesaliva might thus represent both systemic Bcells activation and increasedintraglandular immunoglobulin synthesis, which are peculiarfacetsof pSS.10,11 As notedbefore, the ESSPRI hasbeenvalidatedrecentlyinaninternationalmulticenter
3.0
2.5
2.0
1.5
B2M (ng/mL
)
1.0
0.5
0.0
4 2
0
ESSPRI
8
6 10
Fig.1–Asignificantpositivecorrelationbetweenthe ESSPRIandsalivaryB2Mwasfound(Kendall’stau0.759, 95%CI0.656–0.837,p<0.0001).
cohortofpatientswithpSS.TwoSpanish-speakingcountries were includedinthelatterstudy (includingonefromLatin America).1TheESSPRIhasbeenalsovalidatedintoBrazilian Portuguese.12ThemedianESSPRIinourstudyissimilartothat alreadydescribedbySeroretal.intheirinternational multi-centerstudy.1ThePASSissimilartotheconceptoflow-disease activityfortheEULARSSdiseaseactivityindex(ESSDAI;i.e., ESSDAI<5).Nevertheless,thesetwoindexesdidnot necessar-ilyoverlap,particularlyinpSSwherediseaseactivity(ESSDAI) andpatients’symptoms(ESSPRI)didnotcorrelate.6,13Hence, thesetwoindexescomplementeachotherintheevaluation ofpatientswithpSS.1
B2M (ng/mL)
100
80
60
40
20
0
20
0 40 60
100 - specificity
Sensitivity
80 100
Fig.2–ROCcurveanalysisforsalivaryB2M.Itshowedan areaunderthecurveof0.965(95%CI0.891–0.994,
p<0.0001)withanoptimalcutoffvalueof0.472ng/mL.
184
rev bras reumatol.2017;57(2):182–184OurresultssupportthenotionthatsalivaryB2Mmightact asabiomarkerforanunsatisfactorysymptomstate(Fig.2). PatientswithsystemicfeatureshavehigherscoresonESSPRI, which means that they are more symptomatic.1 Addition-ally,asignificantassociationbetweensalivaryB2M(measured by enzyme-linked immunosorbent assay) and serum anti-Ro/SSA antibodies has been previously reported.11 This is relevantbecause,inpatientswithpSS,theseantibodiesare likelytobestronglyinvolvedinthe clinicalseverityof ker-atoconjunctivitissicca,14 and alsobecause higher levels of these antibodies have been reported in patients with sys-temicfeatures(e.g.,purpura).15Therefore,consideringthese twofindingstogether,higherconcentrationsofsalivaryB2M mayalsodistinguishthosewithsystemicfeatures,whocould benefitmostfromtreatment.6
In summary, there is a significant positive correlation betweenthe ESSPRIand salivaryB2M.Inaddition, salivary B2M iscomparatively higher inthose who were abovethe thresholdofunsatisfactorysymptomstate.Ourresults sug-gest that, inpSS,the intensity ofthe symptoms isindeed associatedwithsB2M.sB2Mmightthusrepresentasimpleand objectivemethodtoaidintheidentificationofthosewithan unsatisfactorysymptomstate.Thelatterisespecially impor-tantinchronicdiseases,suchaspSS,sincetheirtreatment aimstoimprovepatients’qualityoflife.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SerorR,TheanderE,BrunJG,Ramos-CasalsM,ValimV, DörnerT,etal.ValidationofEULARprimarySjögren’s syndromediseaseactivity(ESSDAI)andpatientindexes (ESSPRI).AnnRheumDis.2015;74:859–66.
2. BaldiniC,GalloA,PerezP,MoscaM,AlevizosI,BombardieriS. Salivaasanidealmilieuforemergingdiagnosticapproaches inprimarySjögren’ssyndrome.ClinExpRheumatol. 2012;30:785–90.
3. MichalskiJP,DanielsTE,TalalN,GreyHM.Beta2 microglobulinandlymphocyticinfiltrationinSjögren’s syndrome.NEnglJMed.1975;293:1228–31.
4. PertovaaraM,KorpelaM.ESSPRIandotherpatient-reported indicesinpatientswithprimarySjögren’ssyndromeduring
100consecutiveoutpatientvisitsatonerheumatological clinic.Rheumatology(UnitedKingdom).2014;53:927–31. 5.CastroJ,Jiménez-AlonsoJ,SabioJM,Rivera-CívicoF,
Martín-ArmadaM,RodríguezMÁ,etal.Salivaryandserum
2-microglobulinandgamma-glutamyl-transferasein patientswithprimarySjögren’ssyndromeandSjögren’s syndromesecondarytosystemiclupuserythematosus.Clin ChimActa.2003;334:225–31.
6.SerorR,BootsmaH,SarauxA,BowmanSJ,TheanderE,Brun JG,etal.Definingdiseaseactivitystatesandclinically meaningfulimprovementinprimarySjögren’ssyndrome withEULARprimarySjögren’ssyndromediseaseactivity (ESSDAI)andpatient-reportedindexes(ESSPRI).AnnRheum Dis.2016;75:382–9.
7.ShiboskiSC,ShiboskiCH,CriswellLA,BaerAN,Challacombe S,LanfranchiH,etal.AmericanCollegeofRheumatology classificationcriteriaforSjögren’ssyndrome:adata-driven, expertconsensusapproachintheSjögren’sInternational CollaborativeClinicalAlliancecohort.ArthritisCareRes (Hoboken).2012;64:475–87.
8.ChisholmDM,MasonDK.Labialsalivaryglandbiopsyin Sjögren’sdisease.JClinPathol.1968;21:656–60.
9.PertovaaraM,KorpelaM.Serum2microglobulincorrelates withthenewESSDAIinpatientswithSjögren’ssyndrome. AnnRheumDis.2011;70:2236–7.
10.AsashimaH,InokumaS,OnodaM,OritsuM.Cut-offlevelsof salivarybeta2-microglobulinandsodiumdifferentiating patientswithSjögren’ssyndromefromthosewithoutitand healthycontrols.ClinExpRheumatol.2013;31:699–703. 11.BaldiniC,GiustiL,CiregiaF,DaValleY,GiacomelliC,Donadio
E,etal.Proteomicanalysisofsaliva:auniquetoolto distinguishprimarySjögren’ssyndromefromsecondary Sjögren’ssyndromeandotherSICCAsyndromes.Arthritis ResTher.2011;13:R194.
12.PaganottiMA,ValimV,SerranoÉV,MiyamotoST,GiovelliRA, FerreiraSilvaSantosMCL.Validationandpsychometric propertiesoftheEULARSjögren’sSyndromePatientReported Index(ESSPRI)intoBrazilianPortuguese.RevBrasReumatol. 2015;55:439–45.
13.SerorR,GottenbergJE,Devauchelle-PensecV,DubostJJ,Le GuernV,HayemG,etal.EuropeanLeagueAgainst
RheumatismSjögren’sSyndromeDiseaseActivityIndexand EuropeanLeagueAgainstRheumatismSjögren’sSyndrome Patient-ReportedIndex:acompletepictureofprimary Sjögren’ssyndromepatients.ArthritisCareRes(Hoboken). 2013;65:1358–64.
14.ChungJK,KimMK,WeeWR.Prognosticfactorsfortheclinical severityofkeratoconjunctivitissiccainpatientswith Sjogren’ssyndrome.BrJOphthalmol.2012;96:240–5. 15.HarleyJB,AlexanderEL,BiasWB,FoxOF,ProvostTT,Reichlin