REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
A
randomised
comparative
study
of
the
effect
of
Airtraq
optical
laryngoscope
vs.
Macintosh
laryngoscope
on
intraocular
pressure
in
non-ophthalmic
surgery
Bikramjit
Das
a,∗,
Rajiv
Kumar
Samal
b,
Arup
Ghosh
b,
Ratul
Kundu
baDepartmentofAnaesthesiology,Govt.MedicalCollegeandS.T.M.Hospital,Uttarakhand,India
bDepartmentofAnaesthesiology,InstituteofPostGraduateMedicalEducationResearch,WestBengal,India
Received31March2014;accepted3July2014 Availableonline27October2014
KEYWORDS
Airtraq; Haemodynamic response;
Intraocularpressure; Macintoshblade
Abstract
Background: Wecomparedintraocularpressurechangesfollowinglaryngoscopyandintubation withconventionalMacintoshbladeandAirtraqopticallaryngoscope.
Methods:Ninetyadultpatientswererandomlyassignedtostudygrouporcontrolgroup.Study group(n=45)---Airtraqlaryngoscopewasusedforlaryngoscopy.Controlgroup(n=45)--- con-ventionalMacintoshlaryngoscopewasusedforlaryngoscopy.Preoperativebaselineintraocular pressurewasmeasuredwithSchiotztonometer.Laryngoscopywasdoneaspergroupprotocol. Intraocularpressureandhaemodynamicparameterswererecordedjustbeforeinsertionofthe deviceandsubsequentlythreetimesatanintervalofoneminuteafterinsertionofthedevice. Results:Patientcharacteristics,baselinehaemodynamicparametersandbaselineintraocular pressurewerecomparableinthetwogroups.Followinginsertionoftheendotrachealtubewith Macintosh laryngoscope,therewas statisticallysignificantriseinheart rateandintraocular pressurecomparedtoAirtraqgroup.TherewasnosignificantchangeinMAP.Eightpatientsin Macintoshgrouphadtongue-lip-dentaltraumaduringintubation,whileonly2patientsreceived upperairwaytraumainAirtraqgroup.
Conclusion: WeconcludethatAirtraqlaryngoscopeincomparisontoMacintoshlaryngoscope resultsinsignificantlyfewerrisesinintraocularpressureandclinicallylessmarkedincreasein haemodynamicresponsetolaryngoscopyandintubation.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](B.Das).
http://dx.doi.org/10.1016/j.bjane.2014.07.004
PALAVRAS-CHAVE
Airtraq; Resposta hemodinâmica; Pressãointraocular; LâminaMacintosh
EstudocomparativorandomizadodoefeitodolaringoscópioópticoAirtraqvs.
laringoscópioMacintoshsobreapressãointraocularemcirurgianãooftálmica
Resumo
Justificativa:Comparamosasalterac¸õesdepressãointraocularapóslaringoscopiaeintubac¸ão comlâminaMacintoshconvencionalelaringoscópioópticoAirtraq.
Métodos: Noventapacientesadultosforamrandomicamentedesignadosparaosgruposestudo oucontrole.Nogrupoestudo(n=45),olaringoscópioAirtraqfoiusadoparalaringoscopiaeno grupocontrole(n=45),olaringoscópioMacintoshconvencionalfoiusadoparalaringoscopia.A pressãointraocularfoimensuradanopré-operatóriocomtonômetroSchiotz.Alaringoscopiafoi realizadadeacordocomoprotocolodecadagrupo.Pressãointraoculareparâmetros hemod-inâmicosforamregistradoslogoantesdainserc¸ãododispositivoetrêsvezesapósainserc¸ão dodispositivo,comintervalodeumminuto.
Resultados: Ascaracterísticasdospacientes,osparâmetroshemodinâmicosbasaiseaPIObasal foramcomparáveisnosdoisgrupos.Apósainserc¸ãodotuboendotraquealcomo laringoscó-pioMacintosh,houveum aumentoestatisticamentesignificativodafrequênciacardíacaeda pressãointraocular em comparac¸ãocom ogrupo Airtraq. Nãohouve alterac¸ãosignificativa daPAM.OitopacientesdogrupoMacintoshsofreramtraumadelíngua-lábio-dentaldurantea intubac¸ão,enquantoapenasdoispacientessofreramtraumadasviasaéreassuperioresnogrupo Airtraq.
Conclusão:ConcluímosqueolaringoscópioAirtraq,emcomparac¸ãocomolaringoscópio Mac-intosh,resultouemelevac¸õessignificativamentemenoresdaPIOeemaumentosclinicamente menosacentuadosdarespostahemodinâmicaàlaringoscopiaeintubac¸ão.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
TrachealintubationwithtraditionalMacintoshlaryngoscope is associated with increase in intraocular pressure (IOP) alongwithtachycardiaandhypertension.Theseeffectsare notdesirableinpatientswithraisedintra-ocularpressure. TheAirtraq(ProdolMeditecS.A.,Vizcaya,Spain)isanovel opticallaryngoscopethathasbeendevelopedtofacilitate trachealintubation.1Asaresultoftheexaggerated curva-ture of the blade and an internal arrangement of optical components,aviewoftheglottisisprovidedwithout align-mentoftheoral,pharyngealandlaryngealaxes.2Asaresult, intubationis muchless stimulating tothepatient. There-fore,Airtraqopticallaryngoscopeassistedintubationcould beapreferabletechniquewhichoffersadvantagesinterms ofintraocularpressureandcardiovascularstability.
In this study, we compared the effects of IOP to intubation with conventional Macintosh laryngoscope and Airtraq optical laryngoscope (Fig. 1). We also compared haemodynamicchangesandpost-operativeairwaytrauma.
Materials
and
methods
Followingapproval bytheHospitalEthicsCommittee,and written informed patient consent to participate in the study,westudied90ASAphysicalstatusI---IIIpatients,aged between18and65years,scheduledforsurgicalprocedures requiringtrachealintubation,inarandomised,singleblind, controlledclinical trial.Patientswere notincluded ifrisk factorsforgastricaspirationand/orriskfactorsfordifficult
14.2 14.7
19.8
26.05
1 2 3 4
Figure 1 Comparison of IOP between Macintosh and
Air-traq. (1) Airtraq pre-insertion; (2) Macintosh pre-insertion; (3)Airtraqimmediatepost-insertion;(4)Macintoshimmediate post-insertion.
intubation(MallampatticlassIIIorIV;thyromentaldistance lessthan6cm;interincisordistancelessthan4.0cm)were present,patientswerewithraisedintra-ocularpressureor wheretherewasahistoryofrelevantdrugallergy.Alldata werecollectedbyanindependent,unblendedobserver.
(NIBP),pulseoximetry,endtidalcarbondioxide(EtCO2)and
volatile anaesthetic levels, was continuously performed. Prior to induction of anaesthesia, all patients were given fentanyl (2g/kg) intravenously.A sleepdose of propofol (2---3mg/kg) wastitratedtoinduce anaesthesia.Following induction of anaesthesia, all patients’ lungs were man-ually ventilated with sevoflurane (2.0%---2.5%) in oxygen, atracurium0.50mg/kgwasadministered,andthe trachea wasintubated3minlater,byananaesthetist,experienced in the use of both laryngoscopes. Thereafter, the lungs weremechanically ventilatedforthe durationofthe pro-cedure and anaesthesiawas maintainedusing sevoflurane (1.25---1.75%)inamixtureofnitrousoxideandoxygenina 2:1ratio.
EtCO2 waskept below 40mmHg.No other medications
wereadministered,orproceduresperformed,duringthe 5-mindatacollectionperiodfollowingtrachealintubation.
IOPwasmeasuredinboththeeyes(previouslyprepared withlubricanteyedrop)justbeforeinsertionofthedevice andsubsequentlythreetimesatanintervalofoneminute afterinsertionofthedeviceusingSchiotztonometer(The Diagnostic Company: Riester, Germany). Haemodynamic parameterswhichincluded heart rate,mean,systolicand diastolic blood pressure were recorded simultaneously at the time of measuring IOP. Blood staining of the device wasnotedafterremovalandtongue-lip-dentaltraumawere recordedinthepost-anaesthesiacareunit.
Sample size wasselectedtodetect aprojected differ-ence of 25% between the groups with respect to IOP for a typeI error of 0.05 and a power of 0.9 andthe power ofanalysiswasbasedonapreviousstudyof IOP measure-mentwithMacintosh laryngoscope.3 Dataarerepresented asmean±SD.Betweengroupcomparisonsweredoneusing Student’sttestandnon-parametricMann---Whitneytestin casedatadidnotfollownormaldistribution.Airwaytrauma wascomparedusingFisher’sexacttest.pvalue<0.05was consideredsignificant.
Result
Atotal of90 patientswere studied,45 in eachsubgroup. Nosignificantdifferencesbetweenthesubgroupswereseen withregardtoage,sex,andweight(Table1).
Table1 Demographicparameters.Dataaremean(SD).
Macintosh(n=45) Airtraq(n=45)
Age(years) 40.25(9.44) 44.15(11.22) Weight(kg) 69.10(5.22) 63.65(10.78)
Male:female 29:16 32:13
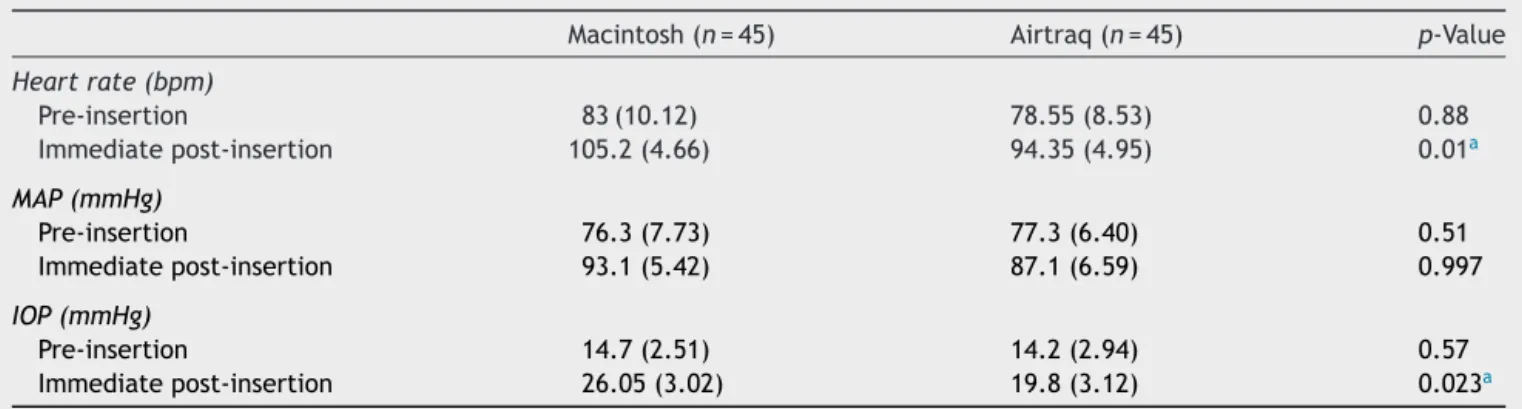
There was no significant difference in heart rate (p=0.88),meanbloodpressure(p=0.51)andIOP(p=0.57) before insertion of the airway devices between the two groups (Table 2). Following insertion of the endotracheal tube with Macintosh laryngoscope, there wasstatistically significant rise in heart rate compared to Airtraq group. There was no significant change in MAP (p=0.997). The IOP measured after intubation in Macintosh group was 26.05±3.02mmHgand 19.8±3.12mmHg inAirtraq group andthiswasstatisticallysignificant(p=0.023)(Table2).
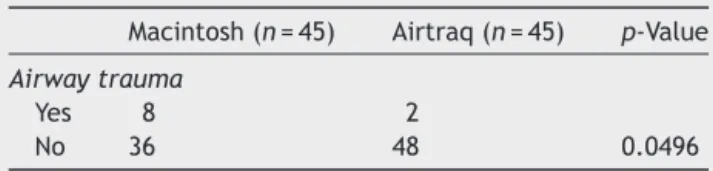
EightpatientsinMacintoshgrouphadtongue-lip-dental trauma during intubation, while only 2 patients received upper airwaytrauma in Airtraq group. This was also sta-tisticallysignificant(p=0.0496)(Table3).
Discussion
Directlaryngoscopyandtrachealintubationhavebeen con-stant concerns with regard to regular occurrence of the pressor responses associated with it. The haemodynamic responses,manifestingasincreaseinheartrateandblood pressure, are due to reflex sympatho-adrenal discharge provoked by epilaryngeal and laryngotracheal stimulation subsequenttolaryngoscopyandtrachealintubation.3---6The stressresponsetotrachealintubationandextubationisalso associatedwithincreasein IOP.7---11 The mechanismof IOP riseissecondary toincreasedsympatheticactivity. Adren-ergicstimulationcausesvasoandvenoconstriction,andan increaseincentralvenouspressure,whichhasaclose rela-tionshipwithIOP.12 Inadditionadrenergic stimulationcan also produce an acute increase in IOP, by increasing the resistancetotheoutflowofaqueoushumourintrabecular meshworkbetweenanteriorchamberandSchlemn’scanal.13 Thisexplainsthecloserelationshipbetweenhaemodynamic andIOPresponsewhichwasalsoseeninourstudy.
Table2 Comparisonofthemeasuredparametersbetweenthetwogroups.Dataaremean(SD).
Macintosh(n=45) Airtraq(n=45) p-Value
Heartrate(bpm)
Pre-insertion 83(10.12) 78.55(8.53) 0.88
Immediatepost-insertion 105.2(4.66) 94.35(4.95) 0.01a
MAP(mmHg)
Pre-insertion 76.3(7.73) 77.3(6.40) 0.51
Immediatepost-insertion 93.1(5.42) 87.1(6.59) 0.997
IOP(mmHg)
Pre-insertion 14.7(2.51) 14.2(2.94) 0.57
Immediatepost-insertion 26.05(3.02) 19.8(3.12) 0.023a
Bpm,beatsperminute;MAP,meanarterialpressure;IOP,intra-ocularpressure.
Table3 Comparisonofairwaytrauma.
Macintosh(n=45) Airtraq(n=45) p-Value
Airwaytrauma
Yes 8 2
No 36 48 0.0496
The acute increase in IOP may be dangerous for patientswithimpendingperforationofeye,perforatingeye injuries,glaucoma,etc.Thisproblemhasdrawnthe atten-tion of many workers to study the attenuation of these responseswithsomepre-treatmentorbysomealternative tolaryngoscopy and trachealintubation, viz. LMA. Ligno-caine pre-treatment, either intravenous or nebulised has been used toattenuate ocular and systemicresponses to laryngoscopyandtrachealintubation.7,9,10Intranasal nitro-glycerinehasalsobeenevaluatedtopreventincreaseinIOP associatedwithtrachealintubation.11LMA,asanalternative toendotracheal tube hasattractedtheattention ofmany workerswithregardstoIOPchanges,asitobviatestheneed for laryngoscopy and tracheal intubation. Holden et al.14 werethe firsttocompare theIOP changesusing LMAand endotrachealtube andtheir observationsaswell asthose ofLambetal.15revealedasignificantlysmallerincreasein IOPusingLMAbothonplacementandremovalascompared toendotrachealintubation.Similarresultswerereportedby Whitfordetal.16andDumanetal.17
Inourstudywefoundthattherewassignificantincrease inheart rate andIOP after airwayinstrumentation in the Macintosh group compared to the Airtraq group. But the increaseinMAPisnotsignificant.Thesefindingsofourstudy areinaccordancewiththestudyofCasatietal.18 Thetwo maincauses of haemodynamicresponses totracheal intu-bationarestimulitooropharyngealstructuresproducedby laryngoscopy, and stimuli to the larynx and trachea sec-ondarytotube insertion.19 Apossible explanationforwhy theAirtraqmaybetterattenuatethehaemodynamicstress responsecomparedtoMacintoshisthatitminimally stimu-latestheairwaystressreceptors.
ArterialpressureplaysaroleincontrolofIOPbuthasa relativelyminorroleifthearterialpressureisinthe physio-logicalrange.20,21InpatientswithaninitialIOP>11mmHg, nocorrelationwitharterialpressurewasfoundbutagood correlation existed between the IOP and central venous pressure(CVP).22 Inourstudy,thebaselineIOPinboththe groupswasmorethan11mmHgandnosignificant correla-tionwas found between MAP andIOP in Airtraqgroup. A significantriseinIOPwasfoundinMacintoshgroup,which couldbeaconsequenceofgreaterpressorresponseto laryn-goscopeguided trachealintubation. We didnot studythe correlationofIOPwithCVPbecauseCVPmonitoringwasnot indicatedintheallottedcases.
In our study MAP in the Macintosh group was not increased significantly compared to the Airtraq group. Greater sympathetic stimulation is required to increase arterial blood pressure than to increase heart rate and IOP.23 As patients were premedicated with fentanyl and inducedwithpropofol,thatamountofsympathetic stimula-tionwasnotreached.So,heartrateandIOPwereincreased
significantlyinMacintoshgroup,butMAPwasnotincreased significantly.
IOPisalsoknowntoincreaseafterariseinPaCO2asa
resultofchoroidalvasodilatationorelevationofCVPor pos-siblyacombinationofboththemechanisms.24 Weensured Normocapnia throughout the intra-operative period (end tidalCO2=35---40mmHg).
We found a significant rise in IOP post-Airtraq guided intubation from the pre-insertion values (mean IOP=14.2mmHg),withtherisebeing19.8mmHg.Themean rise in IOP was within the normal range of 10---20mmHg, which should notbe deleterious toa normal eye but can beharmfulforapatientwithglaucomaorhypertension.
Increasednumber ofairwaytraumain Macintoshgroup resulted from greater force required to visualise laryn-geal opening.25 This would have alsoprobablyresulted in increasedIOPduetoraisedarterialpressureaswellasraised CVP.Butwedidnotmeasureanydirectcorrelationbetween airwaytraumaandraisedIOPinthisstudy.
Conclusion
We concludethatAirtraqopticallaryngoscope wouldbea betteroptionofendotrachealintubationthantheMacintosh laryngoscopeinpatientshavingraisedintraocularpressure. Haemodynamicpressorresponseandairwaytraumaarealso lesswithAirtraq.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Nishikawa K, HukuokaE, KawagishiT, et al. Efficacyof the Airtraqlaryngoscope.JAnesth.2011;25:93---7.
2.DhonneurG, AbdiW,Amathieu R,et al.Optimisingtracheal intubationsuccessrateusingtheAirtraqlaryngoscope. Anaes-thesia.2009;64:315---9.
3.AlexanderR,HillR,LiphamWJ,etal.Remifentanylprevents anincreaseinintraocularpressureaftersuccinylcholineand trachealintubation.BrJAnaesth.1998;81:606---7.
4.Prys-Roberts C, Greene LT, Meloche R, et al. Studies of anaesthesiainrelationtohypertension:haemodynamic conse-quencesofinductionandendotrachealintubation.BrJAnaesth. 1971;43:531---6.
5.Derbyshire DR, Chmielewski A, Fell D, et al. Plasma cate-cholamine responses to tracheal intubation. Br J Anaesth. 1983;55:855---9.
6.Shribman AJ, Smith G, Achola KJ. Cardiovascular and cat-echolamine responses to laryngoscopy with and without intubation.BrJAnaesth.1987;59:295---9.
7.Mostafa SM, Wiles JR, Dowd T, et al. Effects of nebulized lignocaineon theintraocular pressure responsesto tracheal intubation.BrJAnaesth.1990;64:515---7.
8.RobinsonR,WhiteM,McCannP,etal.Effectofanaesthesiaon intraocularbloodflow.BrJOphthalmol.1991;75:92---4.
10.DrengerB,PeerJ.Attenuationofocularandsystemicresponses totrachealintubationbyintravenouslignocaine.BrJ Ophthal-mol.1987;71:546---8.
11.MahajanRP,GroverVK,SharmaSL,etal.Intranasal nitroglyc-erinandintraocularpressureduringgeneralanesthesia.Anesth Analg.1988;67:631---6.
12.KilickanL,BaykaraN,GurkanY,etal.Theeffectonintraocular ofendotrachealintubationorlaryngealmaskairwayuseduring TIVAwithout theuse ofmuscle relaxants.ActaAnaesthesiol Scand.1999;43:343---6.
13.LanghamME,KitazawaY,HartRW.Adrenergicresponsesinthe humaneye.JPharmacolExpTherap.1971;179:47---55.
14.HoldenR,MorsmanCDG,ButlerJ,etal.Intra-ocularpressure changesusing thelaryngeal mask airway and tracheal tube. Anaesthesia.1991;46:922---4.
15.LambK, JamesMFM,Janicki PK. Thelaryngeal maskairway forintraocularsurgery:effectsonforintraocularpressureand stressresponses.BrJAnaesth.1992;69:143---7.
16.WhitfordAM,HoneSW,O’HareB,etal. Intraocularpressure changesfollowinglaryngealmaskairwayinsertion---a compar-ativestudy.Anaesthesia.1997;52:794---6.
17.DumanA,OgunCO,OkesliS.Theeffectonintraocularpressure oftrachealintubationorlaryngealmaskairwayinsertionduring sevofluraneanaesthesiainchildrenwithouttheuseofmuscle relaxants.PaediatrAnaesth.2001;11:421---4.
18.Casati A, Aldegheri G, Fanelli G, et al. Lightwand intuba-tion does not reduce the increase in intraocular pressure associated withtracheal intubation. JClinAnesth. 1999;11: 216---9.
19.TsaiPB,ChenB.Haemodynamicresponsestoendotracheal intu-bationcomparingtheAirwayscope,GlidescopeandMacintosh laryngoscope.InternetJAnaesthesiol.2010;24.
20.MacriFJ. Vascular pressurerelationships and theintraocular pressure.ArchOpthalmol.1961;65:571---4.
21.MurphyDF.Anesthesiaandintraocularpressure.AnesthAnalg. 1985;64:520---30.
22.Tsamparlakis J, Casey TA, Howell W, et al. Dependence of intraocular pressure on induced hypotension and pos-ture during surgicalanaesthesia. Trans Ophthalmol SocU K. 1980;100:521---6.
23.BajwaSS,KaurJ,SinghA,etal.Attenuationofpressorresponse anddosesparingofopioidsandanaestheticswithpre-operative dexmedetomidine.IndianJAnaesth.2012;56:123---8.
24.PetounisAD,ChondreliS,Vadaluka-SekiotiA.Effectof hyper-capnea and hyperventilation on human intraocular pressure duringgeneralanaesthesiafollowingacetazolamide administra-tion.BrJOpthalmol.1980;64:422---5.