www.jped.com.br
ORIGINAL
ARTICLE
Associations
between
the
practice
of
bullying
and
individual
and
contextual
variables
from
the
aggressors’
perspective
夽
,
夽夽
Wanderlei
Abadio
de
Oliveira
a,∗,
Marta
Angélica
Iossi
Silva
a,
Jorge
Luiz
da
Silva
a,
Flávia
Carvalho
Malta
de
Mello
a,
Rogério
Ruscitto
do
Prado
b,
Deborah
Carvalho
Malta
caEscoladeEnfermagemdeRibeirãoPreto(EERP),UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
bSchoolofMedicine,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
cSchoolofNursing,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received16January2015;accepted15April2015 Availableonline28June2015
KEYWORDS Schoolhealth; Bullying; Familyrelations; Risk-taking
Abstract
Objectives: ToestimatetheprevalenceofbullyingamongBrazilianstudentsfromthe
aggres-sor’sperspectiveandtoanalyzeitsassociationwithindividualandcontextualvariables.
Methods: Thiswas across-sectional population-basedstudy carried outwith data fromthe
NationalSurveyonStudentHealth.Atotalof109,104studentsattendingeightgradeinpublic andprivateschoolswereincluded.Datawerecollectedthroughaself-appliedquestionnaire. Amodel ofassociationbetweenbullyingandvariables inthefollowingdomainswastested: sociodemographics,riskbehaviors,mentalhealth,andfamilycontext.Univariateand multi-variateanalyseswerealsoperformed.
Results: Theprevalenceofaggressorsinbullyingsituationswas20.8%.Thefollowingvariables
remainedassociatedinthefinalmultivariatemodel:malegender(OR:1.87;95%CI:1.79---1.94), lowerparticipationof16-year-oldstudents(OR:0.66;95%CI:0.53---0.82),andstudentsfrom privateschools(OR:1.33;95%CI:1.27---1.39).Mostaggressorsreportedfeelinglonely(OR:1.22; 95%CI:1.16---1.28),insomniaepisodes(OR:1.21;95%CI:1.14---1.29),andahighprevalenceof physicalviolence inthefamily(OR:1.9795%CI:1.87---2.08).Aggressorsmissedclassesmore frequently(OR:1.45;95%CI:1.40---1.51),andtheyregularlyconsumedmoretobacco(OR:1.21;
夽 Pleasecitethisarticleas:deOliveiraWA,SilvaMA,daSilvaJL,deMelloFC,doPradoRR,MaltaDC.Associationsbetweenthepractice
ofbullyingandindividualandcontextualvariablesfromtheaggressors’perspective.JPediatr(RioJ).2016;92:32---9.
夽夽
StudyassociatedwiththeMinistryofHealthandUniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](W.A.deOliveira).
http://dx.doi.org/10.1016/j.jped.2015.04.003
95%CI:1.12---1.31),alcohol(OR:1.85;95%CI:1.77---1.92),andillegaldrugs(OR:1.91;95%CI: 1.79---2.04);theyalsodemonstratedincreasedsexualintercourse(OR:1.4995%CI:1.43---1.55) andregularexercise(OR:1.20;95%CI:1.16---1.25).
Conclusions: Thedataindicatethatbullyingisanimportantaspectthataffectsthe
learning-teachingprocessandthestudents’health.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Saúdeescolar; Bullying;
Relac¸õesfamiliares; Assunc¸ãoderiscos
Associac¸õesentreapráticadebullyingevariáveisindividuaisedecontexto naperspectivadosagressores
Resumo
Objetivos: Estimar aprevalência de bullying, sob a perspectiva do agressor, em escolares
brasileiros,eanalisarsuaassociac¸ãocomvariáveisindividuaisedecontexto.
Métodos: Estudotransversal,debasepopulacional,comdadosdaPesquisaNacionaldeSaúdedo
Escolar.Participaram109.104estudantesdo9◦anodoEnsinoFundamentaldeescolaspúblicas eprivadas.Acoletadedadosocorreupormeiodeumquestionárioautoaplicável.Foitestado modelodeassociac¸ãoentreobullyingevariáveisnosseguintesdomínios:sociodemográfico, comportamentosderisco,saúdementalecontextofamiliar,bemcomorealizadasanalisesuni emultivariada.
Resultados: Aprevalênciadeagressoresemsituac¸õesdebullyingfoide20,8%.Nomodelofinal
multivariado permaneceramas seguintesvariáveis associadas:sexo masculino(OR: 1,87;IC 95%:1,79-1,94), menorparticipac¸ãodeescolaresde16 anos(OR:0,66; IC95%:0,53-0,82), estudantesdeescolaprivada(OR1,33IC95%1,27-1,39).Amaioriadosagressoresrelatouse sentirsolitário(OR:1,22;IC95%:1,16-1,28),comepisódiosdeinsônia(OR:1,21;IC95%: 1,14-1,29) e altaprevalência desofrer violência físicafamiliar(OR: 1,97IC 95%:1,87-2,08). Os agressoresfaltammaisàsaulas(OR:1,45;IC95%:1,40-1,51),consomemregularmentemais tabaco(OR:1,21;IC95%:1,12-1,31),álcool(OR:1,85;IC95%:1,77-1,92)edrogasilícitas(OR: 1,91;IC95%:1,79-2,04),temrelac¸ãosexualOR:1,49IC95%1,43-1,55)epraticamatividade físicaregular(OR1,20IC95%1,16-1,25).
Conclusões: Osdadosindicamqueapráticadobullyingéaspectorelevantequeinterfereno
processoensino-aprendizagemenasaúdedosescolares.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Bullying is a form of violence that occursbetween peers at school, characterized by intentionality and repeatabil-ity in a relational context of power imbalance.1 As it
affectsallmembersoftheschoolcommunity,bullying has a negative impact on the institutional environment, the teaching-learningprocess,andthedevelopmentandhealth of school-aged children and adolescents. The increasing prevalence of bullying episodes in different cultures and itsconsequencesforthoseinvolved havemadeit apublic healthproblem.2,3
Bullyingexperiencesalsoincreasetheadoptionof health-riskbehaviorsbystudents,suchasconsumptionofalcohol andotherdrugs,aswellasearlysexualintercourse,aspects that are broadly disclosed in the scientific literature.4 It
is recognized,however, thattherehave been few studies assessingspecificissuesassociatedtostudentsidentifiedas aggressors,ratherthanfocusingonthevictimsandthe con-sequencesforthisgroupofstudents.Inthissense,several methodologicalapproachesshouldbeconsideredtobetter understand the variables associated withpeer aggression
practices,aswellasthewaytheyaffectthehealthy devel-opmentoftheaggressorstudents,inordertocontributeto thecreationofeffectiveinterventionprogramsthatinclude differenttypesofinvolvementinbullyingpractices.1,3,4
Thisstudybringsaninnovativecontributiontothe scien-tificliterature,asitincludesidentificationoftheprevalence of Brazilian students who reported practicing bullying in schools,focusingonthespecificcharacteristicsofthisgroup of students. Thus, the objective was to verify the pres-enceofassociationsbetweenthepracticeofbullyingwith sociodemographic variables (age, gender, ethnicity/self-declaredskincolor,andtypeofschool---publicorprivate), aswell asmental health (feeling of loneliness, insomnia, andlack offriends),familycontextvariables(experiences domesticviolence andfamilysupervision), andhealth-risk behaviors(physicalinactivity,tobaccouse,consumptionof alcoholand/orillicitdrugs,andsexualintercourse).
Method
Health(PesquisaNacionaldeSaúdedoEscolar-PeNSE),from ApriltoSeptember2012.Thesampleconsistedofstudents attendingeighthgradeofelementaryschoolduringtheday in public and private schools located in urban and rural areas,inanumberofmunicipalitiesacrossthecountry.The choiceoftheeighthgradeofelementaryschoolwasjustified as representing the minimal schooling deemed necessary toanswertheself-administeredquestionnaireusedindata collection.
The information for sample calculation was obtained fromthe2010SchoolCensus.Theprobabilisticsampling pro-cesswasused andthe sampling planconsisted of schools (primary sampling units) and schools classes (secondary samplingunits).Atotalof134,310studentswereenrolledin theeighthgradeintheselectedclasses.Ofthese,132,123 studentswereconsideredregularlyattendingstudentsand 110,873 werepresent in the classroom on theday of the interview.Theonlycriterionforinclusioninthesamplewas tobepresentonthedayofdatacollectionandvoluntarily accepttoparticipate.Thefinalsampleincluded109,104 stu-dents,representing83%ofthoseconsideredeligibleforthe study.5Inthissample,86%ofstudentswereagedbetween
13and15years,47.8%weremalesand52.2%females,with 17.2%studentsattendingprivateand82.8%publicschools.5
Data were collectedthrough smartphone devices, into which structured, self-administered questionnaires were entered,dividedintothematicmoduleswithavaried num-berofquestions.Thecollectiontoolwasanepidemiological survey that has not been validated, created in partner-shipwithprofessionalsfromdifferentinstitutionsandwith diverse backgrounds. The collection was carried out by agents of the Brazilian Institute of Geography and Statis-tics(InstitutoBrasileirodeGeografiaeEstatística[IBGE]), adequatelytrainedfor thispurpose, in schools duringthe schoolperiod.
The sociodemographic characteristics that were col-lected and considered for this study were age, gender, ethnicity/self-declaredskincolor,andtypeofschool(public orprivate).Thevariablebullyingwasobtainedthroughthe question:‘‘INTHELAST30DAYS,haveyouverballyabused, ridiculed,teased,intimidated,ormadefunofanyofyour classmates at school so that he or she was hurt, upset, offended,orhumiliated?’’.Theresponseswerecategorized asNO(never,rarely,sometimes)andYES(mostofthetime, always).
Mental health variables (feelings of loneliness, insom-nia,andlackoffriends),familycontext(domesticviolence andfamilysupervision---monitoringofactivities,knowledge aboutstudents’activitiesintheir freetime,school atten-dancecontrolandperformance) andhealth-riskbehaviors (missingclasses,tobaccoandalcoholuse,illicitdrugs,and sexualintercourse) wereinvestigated by means of occur-rence and frequency. Data were measured in scales in accordancetothequestions,whichvariedaccordingtothe frequencyandbytheYESandNOcategory.
Atthedataanalysis,weightedfrequenciesandrespective 95%confidenceintervals(95%CI)wereinitiallyestimatedfor sociodemographiccharacteristics,practiceofbullying,and other assessed variables.Subsequently, all variableswere dichotomizedforpurposesofcomparisonwiththepractice ofbullying.Logisticregressionanalysiswasperformed, cal-culatingtheestimatedoddsratiosandtheirrespective95%
CIs. These analyses were performed usingSPSS software, version 20, usingthe proceduresof the Complex Samples Module,adequateforanalysisofdataobtainedbycomplex sampling.6
PeNSEwasapprovedby theResearchEthicsCommittee of the Ministry of Health, EdictNo. 192/2012, pertaining toregistryNo.16805 ofCONEP/MS. Additionally, students whovolunteeredtoparticipateinthesurveyagreedtothe informedconsentdisplayedonthefirstpageofthe smart-phoneusedfordatacollection.
Results
The results show that involvement in bullying situations asaggressors was reportedby 20.8% of assessed students (n=22,694). The sociodemographic characteristics of this groupofstudentsaredepictedinTable1.
School bullies were more often aged 15 years (OR: 1.34; 95% CI: 1.12---1.61) and 14 years (OR 1.25, 95% CI: 1.04---1.49). The boys practiced more bullying in compar-ison to girls, a proportion nearly two times higher (OR: 1.86;95%CI:1.81---1.92).Regardingtheethnicfactorofthe sample(ethnicity),theethnicdistributionoftheaggressors wassimilar,butwithahigherprevalenceofblackstudents (OR: 1.14; 95% CI: 1.09---1.19) and Asians (OR: 1.10; 95% CI:1.02---1.19)andlowerprevalenceofmixed-racestudents (OR:0.92;95%CI:0.89---0.95%).Additionally,practiceof bul-lyingwasassociatedwithstudyinginaprivateschool(OR: 1.22;95%CI:1.17---1.26).Table2shows thedistributionof aggressorsstudentsaccordingtohealth-riskbehaviors.
Itwasalsoverifiedthat mostaggressorsreported feel-ing lonely (OR:1.27; 95% CI:1.22---1.32), having insomnia (OR:1.45;95%CI:1.39---1.52),andnothavingfriends(OR: 1.10; 95% CI: 1.02---1.19); in addition, a high prevalence of them suffered domestic violence (OR: 2.54; 95% CI: 2.44---2.65).Beinganaggressorwasinverselyassociatedwith familysupervision(OR:0.55;95%CI:0.53---0.56).The aggres-sors missedalmost twiceasmuchclass(OR:1.83;95%CI: 1.78---1.89).Table3showsthebehaviorsassociatedwithlicit andillicitdrugexperimentationbyaggressors,aswellasthe practiceofsexualintercourseandphysicalactivity.
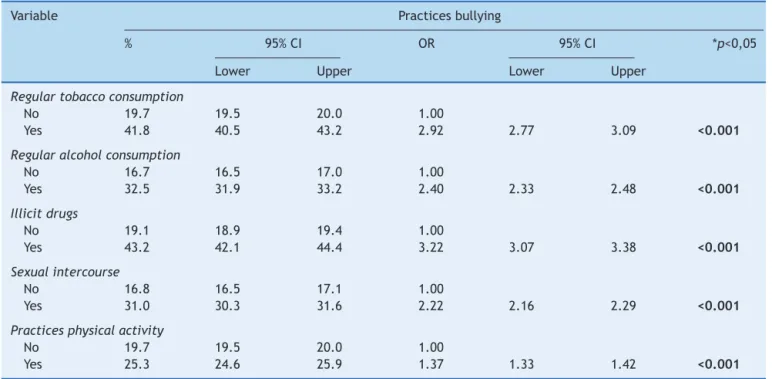
Theaggressorsusedtobaccothreetimesmoreregularly (OR:2.92;95%CI:2.77---3.09);reportedmorethantwicethe regularalcoholconsumption(OR:2.40;95%CI:2.33---2.48), andmorethanthreetimestheuseofillicitdrugs(OR:3.22; 95% CI:3.07---3.38).Sexualintercourse wasalsomore fre-quent(OR:2.22;95%CI:2.16---2.29),aswellasthepractice of physicalactivity (OR:1.37;95%CI:1.33---1.42). Table4
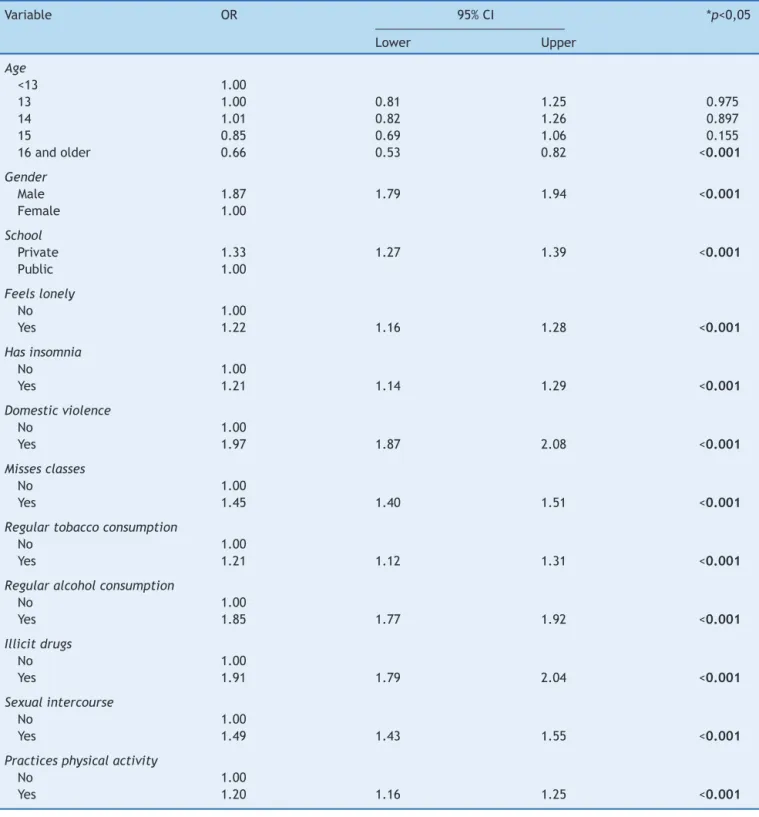
shows theresultsobtained afteradjustmentforall model variables.
Table1 Socio-demographiccharacteristicsofstudentsidentifiedasaggressors.
Variable % 95%CI OR 95%CI *p<0,05
Lower Upper Lower Upper
Age
<13 17.7 15.2 20.5 1.00
13 19.4 18.6 20.2 1.12 0.93 1.34 0.225
14 21.1 20.4 21.9 1.25 1.04 1.49 0.015
15 22.4 21.5 23.3 1.34 1.12 1.61 0.001
16andolder 20.4 19.7 21.1 1.19 0.99 1.43 0.058
Gender
Male 26.2 25.6 26.7 1.86 1.81 1.92 <0.001
Female 16.0 15.7 16.3 1.00
Ethnicity
White 21.0 20.6 21.4 1.00
Black 23.2 22.4 24.0 1.14 1.09 1.19 <0.001
Asian 22.6 21.3 23.9 1.10 1.02 1.19 0.012
Mixed-race 19.7 19.2 20.2 0.92 0.89 0.95 <0.001
NativeBrazilian 22.1 20.7 23.5 1.07 0.99 1.16 0.111
School
Private 23.6 22.9 24.3 1.22 1.17 1.26 <0.001
Public 20.3 20.0 20.5
Discussion
This study found a prevalence of one-fifth of all students whoreportedpracticingbullyingagainstclassmates.There was a predominance of male students, who studied in private schools. The aggressors reported more insomnia, loneliness, and lack of friends. In the family and school
context,there wasa high prevalence of adolescents who suffer domestic violence from family members and fre-quently miss classes. All variables related to health-risk behaviors demonstrated statistical significance (smoking, alcoholconsumption,illicitdrugs,earlysexualintercourse), aswell asthe practiceof regularphysical activity.These resultsallow understandingof thefactorsassociated with
Table2 Mentalhealthandfamilycontextvariablesoftheaggressors.
Variable % 95%CI OR 95%CI *p<0,05
Lower Upper Lower Upper
Feelslonely
No 20.2 19.9 20.4 1.00
Yes 24.3 23.6 24.9 1.27 1.22 1.32 <0.001
Hasinsomnia
No 20.2 19.9 20.4 1.00
Yes 26.9 26.0 27.7 1.45 1.39 1.52 <0.001
Friends
Oneormore 20.8 20.5 21.0 1.00
Doesnothave 22.4 21.1 23.8 1.10 1.02 1.19 0.013
Domesticviolence
No 18.9 18.7 19.1 1.00
Yes 37.2 36.2 38.2 2.54 2.44 2.65 <0.001
Familysupervision
No 26.8 26.4 27.2 1.00
Yes 16.6 16.2 17.0 0.55 0.53 0.56 <0.001
Missesclasses
No 18.08 17.82 18.34 1.00
Table3 Aggressors’health-riskbehaviors.
Variable Practicesbullying
% 95%CI OR 95%CI *p<0,05
Lower Upper Lower Upper
Regulartobaccoconsumption
No 19.7 19.5 20.0 1.00
Yes 41.8 40.5 43.2 2.92 2.77 3.09 <0.001
Regularalcoholconsumption
No 16.7 16.5 17.0 1.00
Yes 32.5 31.9 33.2 2.40 2.33 2.48 <0.001
Illicitdrugs
No 19.1 18.9 19.4 1.00
Yes 43.2 42.1 44.4 3.22 3.07 3.38 <0.001
Sexualintercourse
No 16.8 16.5 17.1 1.00
Yes 31.0 30.3 31.6 2.22 2.16 2.29 <0.001
Practicesphysicalactivity
No 19.7 19.5 20.0 1.00
Yes 25.3 24.6 25.9 1.37 1.33 1.42 <0.001
aggressive behaviors of Brazilian students in relation to classmates.
The identification of malestudents asthose whomost oftenpracticebullying isalsosupported byother studies. Thiscanbeexplainedbythedepictionofpowerand dom-inationthattheroleof aggressormayrepresent, whichis sociallyexpectedincontemporaryculture.3,4,7Thestudies
alsoindicatethat deficitsinsocial skills, morefrequently observedinboysthan ingirls, cancausethemtobecome directlyinvolvedwithbullyingorsituationsthatcanbe iden-tifiedassuch.8,9
Studiesindicatethattheaggressorsareusuallyolder,in highergrades,andmale.1,3,10Thesefindingswereconfirmed
inastudycarriedoutinPortugal,whichfoundthat differ-entlyfromthevictims,theaggressorstendedtobeolder ---between13and15years---andinhighergrades.10
Specif-ically in Brazil, a recent study found that older students (13and14years)weremorelikelytobeaggressivetoward youngerstudents.3
The current study foundnoassociation withage; how-ever,whenadjustingforallmodelvariables,studentsolder than16yearswerelesslikelytopracticebullying.The eth-nicity/skincolorwasalsonotassociatedwithbullying,being a modulationfactor only for the victims, associated with discriminationandprejudice.8,11
Theassociation withprivateschools,maintainedinthe finalmodel,differsfromthesocialimagerythatassociates violenceinschoolstosociallyandeconomicallyvulnerable communities.Inthissense,astudyperformedinArgentina showedthatbullyingis moreprevalentinprivateschools. Thestudyinvolvedtheparticipationof1690studentsfrom 93publicandprivateschools.Inprivateschools, 28.3%of the students reported being the target of cruelty or dis-criminatoryactions,whereasinpublicschoolsthisratewas 17.2%.12
The association between feelings of loneliness and insomnia reported by aggressors points to the possibility of a psychological disease status, but is divergent from studies13,14indicatingthatvictimshavethehighestratesof
social isolation, anxiety,depression,and lowself-esteem. These dataexplicitlywarnabout thedevelopmentof psy-chologicaldistresspicturesthathavean impactonquality of life,health, and developmentofstudents identifiedas bullies.15 These findingssuggest that both the victim and
theaggressorhavefeelingsofmentaldistress.
Thesedataareaddedtothepredominantreportmadeby aggressor studentsof lackof friends,an aspect confirmed by Brazilian studies that showed that the aggressors are notnecessarilypopularstudents.16,17 Internationally,
stud-iesusuallyassociatetheaggressivebehaviortopopularity,a positive opinion of oneself,littleempathy toward others, and a sense of superiority,8,9,18 characteristics that stand
outamidstthegroupofpeers,resultinginmoreclassmates beingdrawntoindividual.
Thedatarelatedtothelikelihoodoftheaggressor suffer-ingphysicalviolenceinthefamilyenvironmentandhaving little family supervision were similar to those found in otherstudies.19---21Ingeneral,domesticviolence,abuse,and
maltreatment situations are predictors of involvement in bullying situations asaggressors.22 It is inferred that the
experienceof violence inthe familyenvironment encour-ageschildrenandadolescentstodisplayaggressivebehavior atschool.
Theresultsthatassociatedaggressorsandschool absen-teeismhavealsobeenconfirmedbyotherstudies.Generally, these students’ school performance is low and theyhave a negative attitude toward school, teachers, and the teaching-learningprocess.23 Incontrast,schoolfailureand
Table4 Finalmultivariatemodeloftheassociationbetweenmentalhealthandfamilyvariablesandhealthriskbehaviorsin adolescentaggressors.
Variable OR 95%CI *p<0,05
Lower Upper
Age
<13 1.00
13 1.00 0.81 1.25 0.975
14 1.01 0.82 1.26 0.897
15 0.85 0.69 1.06 0.155
16andolder 0.66 0.53 0.82 <0.001
Gender
Male 1.87 1.79 1.94 <0.001
Female 1.00
School
Private 1.33 1.27 1.39 <0.001
Public 1.00
Feelslonely
No 1.00
Yes 1.22 1.16 1.28 <0.001
Hasinsomnia
No 1.00
Yes 1.21 1.14 1.29 <0.001
Domesticviolence
No 1.00
Yes 1.97 1.87 2.08 <0.001
Missesclasses
No 1.00
Yes 1.45 1.40 1.51 <0.001
Regulartobaccoconsumption
No 1.00
Yes 1.21 1.12 1.31 <0.001
Regularalcoholconsumption
No 1.00
Yes 1.85 1.77 1.92 <0.001
Illicitdrugs
No 1.00
Yes 1.91 1.79 2.04 <0.001
Sexualintercourse
No 1.00
Yes 1.49 1.43 1.55 <0.001
Practicesphysicalactivity
No 1.00
Yes 1.20 1.16 1.25 <0.001
sustainableschoolenvironmentcanpromotechangesinthe students’behavior andin thedevelopmentprocess. How-ever, schoolperformance,failure,andabandonment were notspecificobjectsofthisinvestigation.
Otherhealth-riskbehaviorsassociatedwithbullyingare alsoobservedintheliterature.Studiesindicatethat aggres-sorshave antisocialbehavior, inwhichdisregardforsocial rules and norms prevail, and evenconflicts withthe law, aswellasuse ofalcohol andother drugs. These behavior
problemsmayworsenovertimeanddevelopintosituations of crime and violence.1,4 In the United States, a
cross-sectionalstudyidentifiedahigherprobabilityofalcoholuse amongstudentsinvolvedinbullying,whencomparedto stu-dentswhowerenotinvolved.4Anotherstudyconductedin
Barcelonaverifiedthis typeof behavioror alcohol and/or druguseamongstudentsidentifiedasbullies.24 Thesedata
behavior.23Thesestudentsmayalsoinitiatetheirsexuallife
earlierin adolescenceor moreoftenpracticeunprotected sex,23asalsoverifiedbythisstudy.
Regarding physical activity, it was verified that it was associatedwiththe aggression process.This resultdiffers fromthatof other studies; for instance, a US study eval-uating the effect of physical activity programs onschool environmentfoundthatbullyingwasassociatedwithfewer daysandhoursofphysical activity practice.Several stud-ieshave shownthebenefitsofhealth promotionprograms focusingonphysicalexerciseandhowtheycancontributeto decreaseepisodesofthisphenomenon.25Otherstudiesmust
bedevelopedtoconfirmthesefindingsamongBrazilian stu-dents,aiming to understand these mechanisms.Programs for the inclusion of adolescents are important to reduce violence.25
Itwasconcludedthatstudentsidentifiedasbullies are morelikelytodevelopbehaviorsthatmakethemvulnerable tohealth risks.26,27 In addition,at the basis of the
bully-ingpracticeareculturalissuesthatreinforceintoleranceto diversity,lack ofrespect,andacontinuingsystem of hier-archyand power in socialrelations. These characteristics havefavoredthe banalization,trivialization,andincrease of this kind of violence that affectschildren and adoles-cents in different socio-cultural contexts. This is verified whenobservingtheuse ofviolence withinthe familyasa predictor for the development of aggressive behaviors at school,forinstance.Theseexperiencesinanimportant set-tingofdevelopmentculminatebymodulatingthewaythese studentsconnectsociallyandhowtheyrespondtodifferent demandsinlife.
Overall, the data indicate that students who practice bullying in Brazil may have emotional difficulties, prob-lematicrelationship withpeers,difficultiesin adapting to the schoolenvironment, and higher consumption of alco-holandother drugs,which areaspectsthat caninterfere withtheteaching-learningprocessandthestudents’health. Giventhe widerangeof social aspectsand risk behaviors associatedwithstudentsidentifiedasbullies,which influ-encenotonlythe individualdevelopmentofstudentsand their health, but alsothe context in which they and the other membersof the schoolcommunity live,approaches are needed that encompass all these aspects, thus con-tributing to the development of a society and culture of non-violence,in defenseof lifeandof individualand col-lectivehealth.
Somelimitationsofthisstudyshouldbenoted.The over-allstudycoveredawiderangeoftopicsrelatedtostudents’ healthanddetailedinformationaboutthepracticeof bul-lyingwasnot obtained. This is a typical characteristic of studies with population-based designs, which allow map-ping general aspectsand indicate prospectsfor research, interventions, and health practices. The study also was basedexclusivelyonthe students’self-reports,whichcan result in socially expected responses and different inter-pretationsaboutthepracticeofbullying.Furthermore,the toolusedfordatacollectiondidnotincludequestionsthat differentiatedthe types ofbullying behaviors, whichmay havehindered theidentification ofmoresubtlepractices. Additionally, the analyzed data areof cross-sectional ori-gin and therefore do not indicate causal associations or directinfluencesofvariablesincludedinthestudy.Finally,
althoughbullyingisaglobalphenomenon,theresultsofthis studycannotbegeneralizedtoothersocioculturalcontexts besidesthatofBrazil.
It is noteworthy that studies on bullying are a recent development in Brazil. The importance of knowing how thisphenomenonoccursamongBrazilianstudents,sothat the proposed interventions will be effective, has been demonstrated.Therefore,studieswithdifferentdesignsare necessarytounderstandthephenomenon,mainlyfromthe health andeducationcontexts, andtoprovidesubstantial evidence for intervention plans and models. These stud-ies can broadly delineate multidisciplinary performance, aswell asindividualandcontextual factors thatcan con-tribute to the development of violent and health-risk behaviors.
Funding
BrazilianMinistryofHealth.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OlweusD.Schoolbullying:developmentand someimportant challenges.AnnuRevClinPsychol.2013;9:751---80.
2.JonesSN,WaiteR,ClementsPT.Anevolutionaryconcept anal-ysisofschoolviolence:frombullyingtodeath.JForensicNurs. 2012;8:4---12.
3.RechRR,HalpernR,TedescoA,SantosDF.Prevalenceand char-acteristicsofvictimsandperpetratorsofbullying.JPediatr(Rio J).2013;89:164---70.
4.Peleg-OrenN,CardenasGA,ComerfordM,GaleaS.An associa-tionbetweenbullyingbehaviorsandalcoholuseamongmiddle schoolstudents.JEarlyAdolesc.2012;32:761---75.
5.MaltaDC,PortoDL,CrespoCD,SilvaMM,deAndrade SS,de MelloFC,etal.BullyinginBrazilianschoolchildren:analysis oftheNationalAdolescentSchool-basedHealthSurvey(PeNSE 2012).RevBrasEpidemiol.2014;17Suppl1:92---105.
6.SPSSInc.Released2009.PASWStatisticsforWindows,Version
20.0.Chicago:SPSSInc.
7.SilvaMA, Pereira B, Mendonc¸a D,Nunes B, de OliveiraWA. The involvement of girls and boys with bullying: an analy-sis of gender differences. Int J Environ Res Public Health. 2013;10:6820---31.
8.Caravita SC, Di Blasio P, Salmivalli C. Early adolescents’ participation in bullying: is ToM involved? J Early Adolesc. 2010;30:138---70.
9.SalmivalliC,VoetenM.Connectionsbetweenattitudes,group norms,and behaviourinbullyingsituations.IntJBehavDev. 2004;28:246---58.
10.Sebastião J. Violência na escola: uma questão sociológica. Interacc¸ões.2009;5:35---62.
11.PegueroAA, Williams LM.Racial and ethnicstereotypes and bullyingvictimization.YouthSoc.2013;45:545---64.
12.D’AngeloLA,FernándezDR.Clima,conflictosyviolenciaenla escuela.BuenosAires:UNICEF,FLACSO;2011.
14.Arseneault L, Bowes L, Shakoor S. Bullying victimization in youthsandmentalhealthproblems:‘muchadoaboutnothing’? PsycholMed.2010;40:717---29.
15.KnowlerC, Frederickson N. Effects ofan emotional literacy intervention for students identified with bullying behaviour. EducPsychol.2013;33:862---83.
16.LisboaCS,KollerSH.Factoresprotectoresyderiesgoparala agresividadyvictimizaciónenescolaresbrasile˜nos:elroldelos amigos.In:BergerC,LisboaCS,editors.Agresiónencontextos educativos:reportesdelarealidadlatinoamericana.Santiago: EditorialUniversitaria;2009.p.161---83.
17.BinsfeldAR,LisboaCS.Bullying:umestudosobrepapéissociais, ansiedadeedepressão nocontexto escolardo Suldo Brasil. Interpersona.2010;4:74---105.
18.CaravitaSC,CillessenAH.Agenticorcommunal?Associations betweeninterpersonalgoals,popularity,andbullyinginmiddle childhoodandearlyadolescence.SocDev.2012;21:376---95.
19.Tortorelli MF, Carreiro LR, Araújo MV. Correlac¸ões entre a percepc¸ão da violência familiar e o relato de violência na escolaentrealunosdacidadedeSãoPaulo.PsicolTeorPrat. 2010;12:32---42.
20.FosterH,Brooks-GunnJ.Neighborhood,familyandindividual influencesonschool physicalvictimization. JYouthAdolesc. 2013;42:1596---610.
21.ZottisGA,SalumGA,IsolanLR,ManfroGG,HeldtE.Associations between childdisciplinarypractices andbullying behaviorin adolescents.JPediatr(RioJ).2014;90:408---14.
22.BowesL, ArseneaultL,MaughanB,TaylorA,CaspiA,Moffitt TE.School, neighborhood, and family factors are associated withchildren’sbullyinginvolvement:anationally representa-tivelongitudinal study.J Am AcadChild AdolescPsychiatry. 2009;48:545---53.
23.ZaineI,ReisMJ,PadovaniRC.Comportamentosdebullyinge conflitocomalei.EstudPsicol(Campinas).2010;27:375---82.
24.Garcia-ContinenteX,Pérez-GiménezA,EspeltA,NebotAdell M.Bullyingamongschoolchildren:differencesbetweenvictims andaggressors.GacSanit.2013;27:350---4.
25.RomanCG,Taylor CJ. Amultilevel assessmentof school cli-mate,bullyingvictimization,andphysicalactivity.JSchHealth. 2013;83:400---7.
26.MaltaDC,doPradoRR,DiasAJ,MelloFC,SilvaMA,daCostaMR, etal.BullyingandassociatedfactorsamongBrazilian adoles-cents:analysisoftheNationalAdolescentSchool-basedHealth Survey(PeNSE2012).RevBrasEpidemiol.2014;17:131---45.