w w w . r b o . o r g . b r
Original
Article
Analysis
of
using
antirotational
device
on
cephalomedullary
nail
for
proximal
femoral
fractures
夽
,
夽夽
Marcelo
Itiro
Takano,
Ramon
Candeloro
Pedroso
de
Moraes
∗,
Luis
Gustavo
Morato
Pinto
de
Almeida,
Roberto
Dantas
Queiroz
HospitaldoServidorPúblicoEstadualdeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9May2013 Accepted16May2013
Keywords:
Hipfractures
Fracturefixation,internal Bonenails
a
b
s
t
r
a
c
t
Objective:Toanalyzetheinfluenceoffemoralneckdiameterinthepositioningofthesliding
screwincefalomedularesnailsfortreatmentofunstabletranstrochantericfractures.
Methods:Prospectivelythroughout2011,patientswithunstablefracturestranstrochanteric
undergoingosteosynthesiswithcephalomedullarynailusingantirotacionaldevice.They wereevaluatedforsex,ageandfractureclassificationaccordingtoTronzo.Throughdigital radiographsanglereduction,tipapexdistance(TAD),stemdiameterandmeasuresbetween thepositioningofthescrewsandthelimitsofthecervixweremeasured.
Results:Ofthe58patients,42(72.4%)werefemaleand16(27.6%)weremale.33patients
wereclassifiedasTronzoIII(56.9%),6patientsasTronzoIV(10.4%)and19 asTronzoV (19.8%).Themajoritywereinbetweentheeighthandninthdecadeoflife.Theaverage reductionintheanglewas130.05◦forfemalesand129.4◦formales.TheTADaveragewas
19.7mmforfemalesand21.6formales.Theaveragediameteroftheneckandheadvary withstatisticalsignificancebetweenmenandwomen.In19patientstheplacementofthe slidingboltcanbeoptimal.Iftheidealpositioningwasnotpossible,themeandisplacement fornon-infringementofhighercorticalneckwas4.06mm.
Conclusion: Theoptimalplacementwouldnotbepossibleforthemajorityofthepopulation,
fortheaveragediameteroftheneckofthesample.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Análise
do
emprego
do
parafuso
antirrotacional
nos
dispositivos
cefalomedulares
nas
fraturas
do
fêmur
proximal
Palavras-chave:
Fraturasdoquadril Fixac¸ãointernadefraturas Pinosortopédicos
r
e
s
u
m
o
Objetivo:analisarainfluênciadodispositivoantirrotacionalnoposicionamentodoparafuso
deslizantedashastescefalomedularesusadasnotratamentodasfraturas transtrocanteri-anas.
夽Pleasecitethisarticleas:TakanoMI,deMoraesRCP,deAlmeidaLGMP,QueirozRD.Análisedoempregodoparafusoantirrotacional nosdispositivoscefalomedularesnasfraturasdofêmurproximal.RevBrasOrtop.2014;49:17–24.
夽夽
StudyconductedatHipGroup,DepartmentofOrthopedicsandTraumatology,HospitaldoServidorPúblicoEstadualdeSãoPaulo,SP, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.C.P.deMoraes).
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Métodos:estudoprospectivodesériedecasoscompostapor58pacientescomdiagnósticode fraturastranstrocanterianasinstáveissubmetidosàosteossíntesecomhaste cefalomedu-lardotadadedispositivoantirrotacional.Acasuísticafoiavaliadaquantoasexo,idadee classificac¸ãodafratura.Osparâmetrosradiográficosavaliadosnopós-operatórioimediato foram:ângulodereduc¸ão,limitesanatômicos,distância“ponta-ápice”(TAD),deslocamento doparafusodeslizanteemrelac¸ãoaoeixocentraldocolofemoraleposicionamentodo dispositivoantirrotacional.
Resultados: houvepreponderânciadosexofeminino,commaiorianaoitavaenonadécadas
devida.ForamclassificadoscomoTronzoIII33pacientes(56,9%),seiscomoTronzoIV(10,4%) e19comoTronzoV(19,8%).Oângulodereduc¸ãomédionosexofemininofoi130,5◦e129,4◦
nomasculino.Odiâmetromédiodocoloedacabec¸avarioucomsignificânciaestatística entrehomensemulheres.OTADmédiofoide19,7mmnosexofemininoe21,6mmno masculino.Em10pacientes(17,85%)oTADfoisuperiora25mm.Em19pacientes(33,9%)a colocac¸ãodoparafusodeslizantepoderiaocorrernoeixocentraldocolo.Odeslocamento médiodoimplanteparanãoviolac¸ãodacorticalsuperiordocolofoide4,06mmdoeixo central.
Conclusão: noimplanteestudado,dotadodedispositivoantirrotacional,oposicionamento
doparafusodeslizantenoeixocentraldocoloestácondicionadoadiâmetromínimode 34mmdocolofemoral.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thetranstrochantericfracturescorrespondtoextracapsular fracturesoftheproximalfemurincludedbetweenthegreater and lesser trochanters.1,2 Of the annual 250,000 proximal
femoralfracturesintheU.S.A.,25%aretranstrochanteric.3,4
Eachyear,indevelopedcountries thislesion affectsonein every1000people.Itisestimatedthatin2050theincidence willbethreetimeshigher3,5andtheannualcostofUS$8
bil-lionwillbeduplicated.3,6Thus,worldwidethesefracturesare
consideredasamajorpublichealthproblem.1,2
Thesearethemostfrequentfractures,withhigher associ-atedmortalityrate(12–41%inthefirstsixmonths),7and90%
ofthem,arisingfrom low-energytrauma,occur inpatients olderthan65years.8
Usually,thetreatmentissurgical.Onlyexceptionallythe procedurewillbeconservativeinpatientswithcomorbidities thatcontraindicateanesthesia,surgery,orboth.1,8,9Itis
essen-tialthatthestabilityofthefracturebedetermined,sothat thesurgeoncanproperlychoosethemethodtobeemployed. Unstablefracturesarethoselesionsinvolvingthe posterior-medialcortexandthatfeaturereversetraceorsubtrochanteric extension.1,8 Recently,thecritical importanceofthelateral
cortexinregionalstabilitywasrecognized.10–13
In stable fractures, the implant of choice is the slid-inghipscrew(DHS);however,becauseofthebiomechanical advantages of intramedullary location, cephalomedullary implantshavebeenadvocatedforthetreatmentofunstable fractures.1,14–17
Both for DHS and for cephalomedullary pins, placing the sliding screw in the correct position is crucial to the successofosteosynthesis.ThemethodofBaumgartner corre-spondstotheparameterofgoodpositioningcurrentlymore accepted.1Anatomicalcharacteristicsofcertainpopulations
and factors related to the experience of the surgeon were
relatedtoaplacementnotalwaysconsidered“ideal”forthese implants.18–20
In the evolution process ofcephalomedullary pins, the anti-rotationaldeviceevolvedinordertoprovideadditional stabilitytothesystem,bothatthetimeofits implementa-tionandinmaintainingthereductionuntiltheconsolidation. However,thepresenceofananti-rotationaldeviceisrelated toearlycomplicationsarisingfromitsposition,andlater,like asa“Zeffect.”1,21
Thepresentstudyaimedtoanalyzetheinfluenceoftheuse ofanti-rotationaldeviceincephalomedullarypinsusedinour institutionintheaveragedisplacementoftheslidingscrew initspositioningalongthecentralaxisofthefemoralneck. Furthermore, our study aims to determine the percentage ofpatientswhosetip-apexdistancewasbeyondthe recom-mendedmeasure,andtherelationofminimumdiameterof femoralneckforimplantpositioning.
Materials
and
methods
ThestudywassubmittedtoandapprovedbytheEthicsand ResearchCommitteeofHospitaldoServidorPúblicoEstadual deSãoPaulo(HSPE).Allpatientssignedaninformedconsent toparticipate.
FromJanuarytoDecember2011,acaseseriescomprised of58patientsadmittedtotheemergencyroomoftheHSPE withpreoperativeradiographicdiagnosisofunstableproximal femurfracturewasprospectivelyanalyzed.Theparticipants were evaluated forage, gender, and fracture classification. AccordingtotheclassificationofTronzo,13fracturestypeIII,
Type I
Type III
Type IV Type V
Type III variant Type II
Fig.1–Tronzo’sclassification.
orthopedictablebytheclosedfocustechnique,withtheaidof fluoroscopy.
Weusedpinswithadistaldiameterof10or12mmandwith asingleproximaldiameterof17mm,mediolateralangleof6◦
andcervicodiaphysealangleof130◦betweentheneckandthe
intramedullarynailscrews.Thechoiceofimplantwastaken afterpreoperativeplanning,accordingtothe cervicodiaphy-sealangleoftheproximalendofthecontralateralfemurand thediameterofthemedullarydiaphysealregion.Allpatients receivedantithromboticandantibioticprophylaxis.
Twocaseswere excludedbecause,duringthe operation, it wasdecidednotto usethe anti-rotationaldevice. These
patientswereconsideredonlyintheassessmentofgender, ageandTronzo’sclassification.
Intheimmediatepost-operativeperiod,plaindigital radio-graphies (anteroposterior[AP] and profile [P] views) of the pelvisand ofthe hipipsilateral totheosteosynthesiswere obtained,accordingtothestandardizationproposedby Pole-sello etal.22 InAPview,thepatient waspositionedsupine
withthelegsininternalrotationof15–20◦andwiththebeam
ofX-raysdirectedatthemidlinejustabovethepubic symphy-sis.InAcelin’sprofileview,thepatientwaspositionedsupine with90◦offlexionofthecontralateralhip,withtheX-raytube
angledat45◦craniallyinthehorizontalplane,towardtheroot
oftheaffectedthigh(Fig.2).
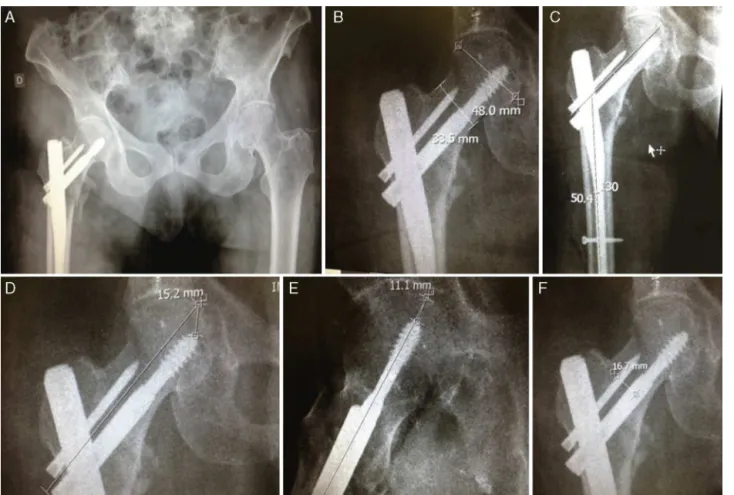
With theuse offiling and transmissionsystem Impax® (version6.3.1.7501,AGFAHealthCareNV),themeasures(in millimeters)ofthediameterofthefemoralheadatits great-estaxis,diameteroftheneckinits smallerthickness(AB), angleofreduction,distancebetweenthecenterofthesliding screwandthetopedgeoftheanti-rotationaldevice(ZX),and distancefromthecenteroftheslidingscrewtotheinferior marginoftheneck(XB)weredigitallyobtainedintheAP posi-tion.Thecentralaxisoftheneckwasdeterminedusingthe midpointofthesmallerthicknessofthefemoralneck(AB).
Thedistancefromthetipofthescrewtotheapexofthe femoralheadwasassessedinAPandP(TipApexDistance, TAD)views,accordingtoBaumgartnerandSolbert method.
Fig. 3shows schematicallythepointsofreferenceusedfor these measurements, and Fig. 4 demonstrates the use of digitaltoolsoftheImpax® programforobtainingthe afore-mentionedmeasures.
ThevalueofZX(15mm)isconstantandsuppliedbythe manufacturer.Suchinformationwasconfirmedinanimplant samplewiththeuseofauniversalcaliper(Fig.5).Toensure reliabilityofthedataobtained,weappliedasindividual cor-rectionfactorforeachmeasurementmadetherelationofthe measurementofZXobtainedonthedigitalradiographyversus valueprovidedbythemanufacturer.
Consideringasidealthepositioningoftheslidingscrew onthecentralaxisoftheneck,weexaminedthefeasibilityof thispositioninginoursamplewiththeanalysisofthe mini-mumneckdiameterrequiredanditsrelationtothesizeofZX. Then,weattributedtheminimumdistanceof2mmfromeach
Z
X
B
A B'
Fig.3–Referencepointsfortheproposedmeasures.AB: diameterofthefemoralneckinitssmallerthickness.AB′:
radiusofthefemoralneck.X:axisofslidingscrew.Z:line tangenttotheupperedgeoftheanti-rotationaldevice.ZX: distancefromtheaxisofthescrewtotheupperedgeofthe anti-rotationaldevice.
Fig.5–TruemeasureofdistanceZX,withuniversalcaliper.
osseousmarginanddeterminedtheequation:AB=(ZX+2)2. AsthevalueofZXcorrespondsto15mm,theminimumsizeof thefemoralneckforsuchpositioningis34mm.Then,we cal-culatedthepercentageofthesampleinwhichthepositioning hereconsideredasidealcouldbeobtained.
Wemeasuredtheaverageseparationoftheslidingscrew inrelationtothecentralaxisoftheneckinsituationswhere anoptimumpositioningcannotbeachieved.
The analyses of the quantitative variables were evalu-atedstatisticallywithrespecttothemean,median,standard
Fig.4–UseofImpax®forthetakingofmeasures.(A)APradiographofthepelvis,asdescribed.(B)Diameteroftheneckand
Table1–Agedistributionbygender.
Gender Mean Median Standarddeviation Minimum Maximum Pvalue
Age
F 81.83 84.00 10.23 48.00 97.00 0.0743
M 77.07 77.00 6.23 68.00 90.00
Table2–AssociationbetweengenderandTronzo’sclassification(P=0.7744).
Tronzo Gender Total
F M N %
N % N %
III 24 57.1 9 56.3 33 56.9
IV 5 11.9 1 6.3 6 10.3
V 13 31.0 6 37.5 19 32.8
Total 42 100.0 16 100.0 58 100.0
Table3–Intraoperativeparametersrelatedtothereductionandimplantpositioning.
Gender Mean Median Standarddeviation Minimum Maximum Pvalue
Angleofreduction(AP)
F 130.05 132.00 10.42 108.00 158.00 0.8755
M 129.40 131.00 9.81 108.00 144.00
TAD
F 19.70 20.10 6.82 1.90 38.50 0.2401
M 21.67 21.90 6.82 2.40 30.00
deviation, minimum, and maximum. In the comparison betweenthegenders,weappliedthenonparametricWilcoxon test.Thequalitativevariableswereevaluatedfordistribution ofabsoluteand relativefrequencies,and theirassociations weretestedbyPearsonChi-square testorFisherexacttest, whentheapproximationofthefirsttestwasnotappropriate. Thesignificancelevelusedinthesetestswas5%,andoptional two-tailedhypothesesalwayswereconsidered.
Results
Ofthe58patientsintheseries,42(72.4%)werewomenand 16(27.6%)men.Intheanalysisoftheagedistribution,mostof thestudypatientswerebetweentheeighthandninthdecades oflife,andtherewasnostatisticallysignificantdifferencein thecomparisonbetweengenders(Table1).
Regardingtheclassificationofthefractureandaccording toTable2,33(56.9%)patientsweregroupedasTronzoIII,six (10.4%)asTronzoIV,and19(19.8%)asTronzoV.Theassociative analysisbetweenTronzo’sclassificationandgenderrevealed nostatisticallysignificantdifference.
With the help of standard X-rays, we obtained data concerningtheangleofreductionachievedduringthe intra-operatoryperiodand theimplantpositioning;nostatistical significance was demonstrated when comparing gender, accordingtoTable3.
RegardingtheTAD,itwasobservedthatin46cases(82.15%) thevaluesweresmallerthan25mm,thusbeingconsidered ideal.
A comparisonofneckand head diametervalues ofthe selectedpatientsshowedstatisticallysignificantdifferences betweengenders,whichalsooccurredforthemeasureofZX (Table4).
Table4–Diameteroffemoralheadandneckobtainedaccordingtogender.
Gender Mean Median Standarddeviation Minimum Maximum Pvalue
Head(AP)
F 49.41 50.00 3.04 43.80 55.10 0.0084
M 53.05 54.40 4.45 43.60 58.80
Neck(AB)
F 34.69 34.30 2.99 28.90 41.80 0.0086
M 37.23 38.00 4.19 26.70 43.10
ZX(implant)
F 16.75 16.80 1.85 11.90 22.00 0.0192
Table5–Spreadsheetwithvaluesobtainedafterapplyingtheindividualcorrectionofmeasurementfactor.
Nr. Age Gender AB reduction AB′ ZX Correctionfactor TAD Tronzo Neck
1 85 F 42 139 20.9 22 1.466666667 17.9 V 28.5
2 78 F 33 121 16.5 20.5 1.366666667 20.1 III 24.07
3 74 F 31 147 15.3 20.6 1.373333333 13.3 III 22.28
4 48 F 35 158 17.5 17.1 1.14 12.6 III 30.61
5 89 F 36 141 18 15.8 1.053333333 20.2 III 34.08
6 97 F 35 140 17.7 15.3 1.02 18.6 III 34.7
7 70 F 33 141 16.6 17.2 1.146666667 20.3 V 23.09
8 77 M 43 142 21.6 15.2 1.013333333 19.7 V 42.53
9 79 F 35 136 17.7 16.1 1.073333333 19.7 V 31.21
10 89 F 33 131 16.7 15.4 1.026666667 18.6 V 32.53
11 78 M 35 144 17.3 12.8 0.853333333 16.2 V 40.54
12 94 F 34 117 16.8 17.5 1.166666667 12.2 III 28.71
13 92 F 40 115 20 16 1.066666667 11 III 37.5
14 90 M 40 131 19.8 16.5 1.1 24.8 V 35.9
15 80 F 41 135 20.5 18 1.2 23 V 34.16
16 85 F 36 115 17.9 20.8 1.386666667 22.5 III 25.74
17 92 F 37 136 18.6 17.5 1.166666667 17.6 IV 31.81
18 79 F 37 140 18.7 16.7 1.113333333 22 IV 33.59
19 92 F 32 108 15.8 16.8 1.12 22 III 28.12
20 74 F 35 125 17.5 18 1.2 26 V 29.16
21 93 F 39 133 19.4 11.9 0.793333333 21 III 27.54
22 87 F 30 125 15.1 15.3 1.02 29.1 III 30
23 73 F 30 110 15.2 0 28.3 IV Excluded
24 63 F 29 122 14.5 17.8 1.186666667 15.4 III 24.35
25 69 M 41 123 20.7 17 1.133333333 26.3 IV 36.52
26 79 M 42 119 20.8 15.1 1.006666667 30 III 41.32
27 80 F 39 143 19.3 15.4 1.026666667 20.1 III 37.59
28 86 F 34 130 17.2 17.4 1.16 25.3 IV 29.65
29 75 M 38 127 19 15.5 1.033333333 24.7 III 36.67
30 90 F 38 126 18.8 17.4 1.16 29.3 III 32.41
31 64 F 33 132 16.3 13.9 0.926666667 16.3 III 34.74
32 92 F 37 119 18.3 17.2 1.146666667 29 III 31.83
33 84 F 33 139 16.7 16 1.066666667 15.3 III 31.31
34 91 F 31 113 15.3 16.3 1.086666667 19.5 III 28.06
35 77 F 30 135 14.8 15 1 14.1 V 29.6
36 87 F 33 121 16.5 15.5 1.033333333 17 III 31.93
37 77 M 38 120 19.2 17 1.133333333 20.1 V 33.79
38 86 F 36 122 17.8 15.2 1.013333333 23.2 V 35.03
39 66 F 33 137 16.5 14.9 0.993333333 30 IV 33.12
40 72 M 37 128 18.6 11.6 0.773333333 21.9 III 47.97
41 76 M 39 134 19.5 17.7 1.18 2.4 III 33.05
42 74 F 34 135 16.9 16.5 1.1 24.6 V 30.72
43 70 M 39 134 19.7 14.7 0.98 28.4 III 40.1
44 95 F 34 123 17.2 17.5 1.166666667 1.9 V 29.4
45 90 F 34 127 16.9 16.8 1.12 16.9 III 30.08
46 81 F 33 116 16.7 16.9 1.126666667 23.2 III 29.64
47 68 M 35 134 17.7 14.6 0.973333333 21 III 36.26
48 73 F 37 125 18.7 16.9 1.126666667 13 V 33.19
49 82 M 31 132 15.7 15.8 1.053333333 17.5 V 28.71
50 78 F 33 133 16.5 16.1 1.073333333 38.5 V 30.74
51 90 M 35 124 17.4 0 20.1 III Excluded
52 75 M 27 108 13.4 17.1 1.14 28.9 V 23.42
53 85 F 32 132 16 15.3 1.02 20.3 III 31.37
54 87 M 35 123 17.7 16.1 1.073333333 18.6 III 32.88
55 84 F 37 125 18.4 16.8 1.12 24 III 32.76
56 72 F 37 136 18.7 15.8 1.053333333 20 III 35.5
57 81 M 38 142 19 14.6 0.973333333 24.5 III 39.04
58 80 F 34 138 16.8 17.8 1.186666667 32 V 28.23
Applyingthecorrectionfactorforeachindividual measure-ment,valuestakenasrealwere obtained.Thesevaluesare showninTable5.
Given the corrected diameter of the femoral neck, it was found that an ideal positioning would be
possible in 19 patients with CI (95%)=21.8%; 47.8% (Table6).
Table6–Percentageofpatientswhoseplacementofthe systemcouldbeideal.
Idealpossible? Nr. % %valid
Not 37 63.8 66.1
Yes 19 32.8 33.9
Total 56 96.6 100.0
Excluded 2 3.4
Total 58 100.0
Discussion
Thetreatment ofunstable transtrochanteric fractures with useofcephalomedullarypinspresentsbiomechanical advan-tages due to its intramedullary location, such as reducing the bendingmoment,betterrotational control,shortening, and collapse in varus.1,14–17 Although controversial, there
are reports ofsuperiority ofcephalomedullary pins versus DHSinrelationtoearlyreturntoambulation,reduced sur-gicaltime,and lessblood loss.1,8,19 Thus,atourinstitution
cephalomedullarypinsareappliedinthetreatmentof unsta-blefractures.1
Regarding the epidemiological findings observed in the presentstudy,thereisavastliteratureattestingthefemale predominance and an age close to 80 years in other series.1,9,18,21,23Thisreflectsthedecreaseinbonemineral
den-sity.Wefoundnostatisticallysignificantdifferencebetween theagesofmaleandfemalepatients.
Althoughthepatternfractureofreverseobliquity(Tronzo VorAO31A3)hasbeenreportedasthemostfrequenttype insome case series ofunstable fractures,9,24 most studies
havedescribed asthe mostprevalenttypesthoseclassified asTronzoIIIorIV(orAO31A2),1,18,25,26 whichagreeswith
ourresults.When comparingmalesand females,wefound nostatisticallysignificantdifferencesinrelationtofracture typeaccordingtotheclassificationofTronzo.
AccordingtoWerner-Tutschkuetal.,27themainpredictor
ofthecutoutisunsatisfactoryinitialreduction,especiallyin varus,besidesfavoringTrendelenburggait.
Wefoundameanvalueof130.5◦formen(withastandard
deviation of10.42) and 129.40◦ (9.81)for women, and this
assessmentwasnotstatisticallysignificant.These findings are similar to those foundin another study with unstable transtrochantericfractures.1
There was a statistically significant difference in the comparisonbetweenmaleandfemale gendersinthe mea-surementsrelatedtodiameteroftheheadandneck.When comparing the bone structure of the neck in young and elderlysubjectsofChineseandCaucasianorigin,Wangetal.28
showedthatmale subjectshavelargerdiameters, thatthis value tends to increase with age, being higher in popula-tionsofwhiteorigin.AccordingtoPuetal.,18astheChinese
populationisoflowerstaturethanthatoftheEuropean sub-jects,thelengthoftheproximalfemurandthediameterof thefemoralneckarealsosmaller,whichleadstothe inappro-priatepositioningofthecephalomedullarypin’sspiralblade usedinthestudy,ortoredundancyoftheproximalendofthe pin.Intheutilizationofthecephalomedullarypinusedinour service,theminimumdiameterforanoptimalplacementis 34mm,whichcorrespondstotwicetheZXmeasure,taking intoaccountathicknessofcortical(topandbottom)of4mm. Inourseries,inonly19patients(32.8%)theplacementofthe slidingscrewcouldbeperformedinthesituationregardedas idealbyourmethodology.Extrapolatingtheconfidence inter-valfortheBrazilianpopulation,onlyin21.8–47.8%ofpatients in95%ofthetimetheimplantcouldbeplacedoptimally(i.e., thecenteroftheslidingscrewlocatedalongthecentralaxis oftheneck).
According to Baumgaertneret al.,15 the correctimplant
placementoccurswhenthedistancebetweenthetipofthe sliding screwand thefemoralheadcenterdoes notexceed 25mmafterthesumofthevaluesobtainedonanteroposterior andprofileviews(tip-apexindex,orTAD<25mm).This facili-tatesthetelescopingofthedynamicsystemoftheimplantand reducestheriskofcutout.9Althoughdescribedfor
osteosyn-thesiswithDHS,themethodcanbeusedtoassessthecorrect positioningofthecephalomedullarypins.1However,inpins
withtwoproximalfixationscrews,thereisdifficulty inthe positioningoftheslidingscrewinthecenterofthefemoral headintheanteroposteriorview.Thus,thereisagreater ten-dencyforthepositioningoftheslidingscrewinamoreinferior locationintheAPradiographicview,particularlyinpatients withshortfemoralneckandhead.21Thelocationofthescrews
intheprofilepositionisnotaffected,sincethescrewsare par-allel.Inthe osteosynthesisusingthe cephalomedullarypin inquestion,themeandisplacementnecessaryforthe intro-ductionofthenailwithoutviolatingtheanti-rotationalupper corticalneckwasof4.6mm(i.e.,theamount ofdownward displacement ofthe system, in millimeters, from the axis ofthefemoralneck).Tocalculatetherequireddisplacement ofthesliding screwrelativethecentralaxisoftheneckin situationswherethisoptionisnotpossible,thefollowing for-mula:=displacement required=34mm−necksize (AB) was applied.
Conclusion
Consideringthemean diameteroftheneckinoursample, thepositioningonthecentralaxisoftheneckwouldnotbe possibleforthemajorityofthepopulation.
Consideringtheimplantstudied,theminimumsizeofthe neckwhichallowspositioningthecentralaxisis34mm.
Table7–Displacementofthesysteminrelationtothecentralaxis.
Mean Standarddeviation CI(95%) Median Q25 Q75 Minimum Maximum
Inf.thres. Sup.thres.
Insituations wherethepositioninginthecentralaxisis notpossibleduetotheminimalsizeoftheneck,the down-warddisplacementrequiredcanbecalculatedbytheformula: displacementrequired=34−necksize(AB).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BorgerRA,LeiteFA,AraújoRP,PereiraTFN,QueirozRD. Avaliac¸ãoprospectiva,radiográficaefuncionaldotratamento dasfraturastrocantéricasinstáveisdofêmurcomhaste cefalomedular.RevBrasOrtop.2011;46(4):380–9.
2. GuimarãesFAM,LimaRR,SouzaAC,LivaniB,BelangeroWD. Avaliac¸ãodaqualidadedevidaempacientesidososumano apósotratamentocirúrgicodefraturastranstrocanterianas dofêmur.RevBrasOrtop.2011;46Suppl.1:48–55.
3. KyleRF.Fracturesoftheproximalpartofthefemur.JBone JointSurgAm.1994;76(6):924–50.
4. Fraturatranstrocanteriana.RevAssocMedBras. 2009;55:637–40,
http://dx.doi.org/10.1590/S0104-42302009000600004.Available from:http://www.scielo.br/scielo.php?script=sciarttext&pid= S0104-42302009000600004&lng=en&nrm=iso[accessed 08.05.13].
5. HaidukewychGJ.Intertrochantericfractures:tentipsto improveresults.JBoneJointSurgAm.2009;91(3):712–9.
6. CummingsSR,RubinSM,BlackD.Thefutureofhipfractures intheUnitedStatesNumbers,costs,andpotentialeffectsof postmenopausalestrogen.ClinOrthopRelatRes.
1990;(252):163–6.
7. RusselTA.Intertrochantericfractures.In:BucholzRW, HeckmanJD,Court-BrownCM,Tornetta3rdP,editors. RockwoodandGreen’sfracturesinadults.Philadelphia: LippincottWilliams&Wilkins;2010.p.1597–640.
8. KaplanK,MiyamotoR,LevineBR,EgolKA,ZuckermanJD. Surgicalmanagementofhipfractures:anevidence-based reviewoftheliteratureII.Intertrochantericfractures.JAm AcadOrthopSurg.2008;16(11):665–73.
9. GuimarãesJAM,GuimarãesACA,FrancoJS.Avaliac¸ãodo empregodahastefemoralcurtanafraturatrocantérica instáveldofêmur.RevBrasOrtop.2008;43(9):406–17.
10.KulkarniGL,KulkarniM,KulkarniS.Intertrochanteric fractures.IndianJOrthop.2006;40(1):16–23.
11.GotfriedY.Thelateraltrochantericwall.ClinOrthopRelat Res.2004;425:82–6.
12.MüllerME.Classificationandinternational
AO-documentationoffemurfractures.Unfallheilkunde. 1980;83(5):251–9.
13.TronzoRG.SymposiumonfracturesofthehipSpecial considerationsinmanagement.OrthopClinNAm. 1974;5(3):571–83.
14.SchipperIB,SteyerbergEW,CasteleinRM,vanderHeijdenFH, denHoedPT,KerverAJ,etal.Treatmentofunstable
trochantericfracturesrandomisedcomparisonofgammanail andtheproximalfemoralnail.JBoneJointSurgBr.
2004;86(1):86–9.
15.BaumgaertnerMR,CurtinSL,LindskogDM.Intramedullary versusextramedullaryfixationforthetreatmentof intertrochanterichipfractures.ClinOrthopRelatedRes. 1998;(348):87–9.
16.BridleSH,PatelAD,BircherM,CalvertPT.Fixationof intertrochantericfracturesofthefemur.Arandomized prospectivecomparisonofthegammanailandthedynamic hipscrew.JBoneJointSurgBr.1991;73(2):
330–4.
17.SchipperIB,BresinaS,WahlD,LinkeB,vanVugtAB, SchneiderE,etal.Biomechanicalevaluationoftheproximal femoralnail.ClinOrthopRelatedRes.2002;(405):
277–86.
18.PuJS,LiuL,WangGL,FangY,YangTF.Resultsoftheproximal femoralnailanti-rotation(PFNA)inelderlyChinesepatients. IntOrthop.2009;33(5):1441–4.
19.GadegoneWM,SalphaleYS.Shortproximalfemoralnail fixationfortrochantericfractures.JOrthopSurg. 2010;18(1):39–44.
20.HeinertG,ParkerMJ.Intramedullaryosteosynthesisof complexproximalfemoralfractureswiththeTargonPFnail. Injury.2007;38(11):1294–9.
21.KawataniY,NishidaK,AnrakuY,KunitabeK,TsutsumiY. Clinicalresultsoftrochantericfracturestreatedwiththe Targon®proximalfemurintramedullarynailingfixation
system.Injury.2011;42(Suppl4):S22–7.
22.PoleselloGC,NakaoTS,QueirozMC,DaniachiD,RicioliJunior W,GuimaraesRP,etal.Propostadepadronizac¸ãodoestudo radiográficodoquadriledapelve.RevBrasOrtop.
2011;46(6):634–42.
23.HungriaNetoJO,DiasCR,AlmeidaJDB.Características epidemiológicasecausasdafraturadoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7.
24.ErtürerRE,SönmezMM,SariS,Sec¸kinMF,KaraA,ÖztürkI. Intramedullaryosteosynthesisofinstableintertrochanteric femurfractureswithProflim®nailinelderlypatients.Acta
OrthopTraumatolTurc.2010;46(2):107–12.
25.ChouDT,TaylorAM,BoultonC,MoranCG.Reverseoblique intertrochantericfemoralfracturestreatedwiththe intramedullaryhipscrew(IMHS).Injury.2012;43(6):817–21.
26.SahinS,ErtürerE,ÖztürkI,TokerS,Sec¸kinF,AkmanS. Radiographicandfunctionalresultsofosteosynthesisusing theproximalfemoralnailantirotational(PFNA)inthe treatmentofunstableintertrochantericfemoralfractures. ActaOrthopTraumatolTurc.2010;44(2):127–34.
27.Werner-TutschkuW,LajtaiG,SchmiedhuberG,LangT,PirklC, OrthnerE.Intra-andperioperativecomplicationsinthe stabilizationofper-andsubtrochantericfemoralfracturesby meansofPFN.Unfallchirurg.2002;105(10):881–5.