SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Direct
repair
of
chronic
distal
biceps
tendon
tears
夽
Bernardo
Barcellos
Terra
∗,
Leandro
Marano
Rodrigues,
André
Luiz
Machado
Lima,
Bruna
Cangini
Cabral,
José
Maria
Cavatte,
Anderson
De
Nadai
HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received29April2015 Accepted11June2015 Availableonline26April2016
Keywords: Tendoninjuries Tenodesis Tendontransfer
Physicalandrehabilitation medicine
a
b
s
t
r
a
c
t
Objective:TopresenttheresultsfromdirecttendonrepairusingEndoButtonand interfer-encescrewsinpatientswithlesionsofthedistalbicepsthathadevolvedoveraperiodof morethan28days.
Methods:BetweenJanuary2012andNovember2013,elevenpatients(allmale)withatorn distalbicepsandatimeintervalbetweeninjuryandsurgeryofmorethan28dayswere evaluated.Thepatients’meanagewas46yearsandthemostcommonmechanismofinjury waseccentricloadingwiththeelbowflexedandsupinated.
Results:Asubjectiveanalysisonpainandfunctionwasconductedusingavisualanalog scaleofpain(VAS)andtheMayoElbowPerformanceScore(MEPS),beforeandaftersurgery. TheVASshowedadecreaseof5pointsto0.8pointsonaverage.TheMEPSimprovedfrom 69.3pointsbeforetheoperationto97.5pointsafterwards.Themeanflexionwas133.1◦ ontheoperatedside,versus134.3◦.Themeanextensionwas−2.5◦and0◦(operatedside versusnon-operated).Supinationwas88.2◦versus89.5◦andpronationwas82.5◦versus 84.1◦,comparingtheoperatedsideversusthenon-operatedside.Flexionandsupination strengthswereevaluatedwiththeaidofadynamometer,andthemeanflexionand supina-tion strengthswerefoundtobe respectively78.57%and 89.65%of thestrength ofthe non-operatedlimb.
Conclusion: UseofthetechniqueofdirecttendonrepairusingEndoButtonandinterference screwswasshowntobeasafeandeffectivealternativeforrepairingchroniclesionsofthe distalbiceps.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Reparo
direto
das
lesões
distais
crônicas
do
tendão
bicipital
Palavras-chave:
Traumatismosdostendões Tenodese
r
e
s
u
m
o
Objetivo:ApresentarosresultadosdoreparodiretodotendãocomEndoButtoneparafuso deinterferêncianospacientescomlesãodobícepsdistalcomevoluc¸ãomaiordoque28 dias.
夽
StudyconductedintheDepartmentofOrthopedyandTraumatology,HospitalSantaCasadeMisericórdiadeVitória,Vitória,ES,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](B.B.Terra). http://dx.doi.org/10.1016/j.rboe.2016.02.005
304
rev bras ortop.2 0 1 6;51(3):303–312Transferênciatendinosa Medicinafísicaereabilitac¸ão
Métodos: Entrejaneirode2012enovembrode2013,11pacientes(todosdosexomasculino) comrupturadobícepsdistalcomintervalodalesãoecirurgiamaiordoque28dias.Aidade médiafoide46anoseomecanismodetraumamaiscomumfoiumacargaexcêntricacom ocotoveloemflexãoesupinac¸ão.
Resultados: Foifeitaumaanálisesubjetivadadorefunc¸ãocomaEscalaVisualAnalógica deDor(EVA)eoMayoElbowPerformanceScore(MEPS)préepós-operatório.Houveuma diminuic¸ãodaEVAde5pontospara0,8pontoemmédia.OMEPSmelhoroude69,3pontos noprépara97,5pontosnopós-operatório.Amédiadeflexãofoide133,1◦doladooperado contra134,3◦.Amédiadeextensãofoide−2,5◦e0◦(ladooperado×nãooperado).Supinac¸ão foide88,2◦×89,5◦epronac¸ão82,5◦×84,1◦quandocomparadooladooperadoversusolado nãooperado.Aforc¸adeflexãoesupinac¸ãofoiavaliadacomoauxíliodeumdinamômetro everificamosqueaforc¸amédiadeflexãoesupinac¸ãocorrespondia,respectivamente,a 78,57%e89,65%aforc¸adomembronãooperado.
Conclusão: AtécnicadoreparodiretodotendãocomousodeEndoButtoneparafusode interferênciamostra-secomoumaopc¸ãoseguraeeficazparaoreparodiretodaslesões crônicasdobícepsdistal.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Distalbicipitaltendoninjuriesarerelativelyrare,representing only3%ofbicepsinjuries;themostfrequentisthe involve-mentofthelong headofthebicepstendoninits proximal portion(96%).1Often,theinjurymechanismisaneccentric loadwiththeelbowinflexionandsupinationinmalepatients betweenthefifthandsixth decadeoflife.Its pathophysio-logy islittleunderstood, but itis knownthat degenerative tendinopathy, mechanical impact, some endocrinous dis-eases, andthe use ofanabolic steroidsare involvedinthe onsetofthisentity.2
Althoughtheclinicalfindingsareclassic,therarityofthe injuryandthegoodmovementarcpresentedbythepatients leadtoalatepresentationand diagnosis.Historically, con-servativetreatment was suggestedforthe management of acuteinjuries.However,afterbiomechanicalstudies demon-stratedlossofflexionandsupinationforcesofupto30%and 40%,respectively,manyauthorsrecommendedthattheacute anatomicalrepairshouldbepreferredtothenon-anatomical repairwiththebrachialtendon.3Withresultsoflossof supina-tion force ofaround50% aftertransfertechnique withthe brachialistendon,newtechniquesemerged,makingthedirect repairthetreatmentofchoice,primarilyinpatientswhoaim forafullreturntotheiractivities.4
Chronic injuries are often difficult to treat due to ten-don retraction, muscular atrophy, and associated fibrosis. However,theconservativetreatmentpresentsunsatisfactory results. Although there is no consensus on the definition ofthechronicinjury timeinterval,theuse oftendongraft is recommended inchronic ruptures to restore the length and preventflexion contracture ofthe elbow.5 The autolo-gous graft can cause donor-site morbidity, and the use of anallograft still presents risks ofinfection and high costs insomeplaces.Theliteraturefeaturescountlessrepair tech-niquesforacuteinjuriesandgraftreconstructiontechniques forchronicinjuries.However,therearefewstudiesassessing
the results of graftless direct repair treatment for chronic injuries.1,2,6,7
Thisstudyaimedtopresenttheresultsofthemodification ofthetechniquebyBainetal.,8whichconsistsofdirect ten-donrepairwithEndoButtonandinterferencescrewinpatients withdistalbicepsinjurywithevolutionlongerthan28days.
Material
and
methods
FromJanuaryof2012toNovemberof2013,eightpatients(all males)withdistalbicepsruptureandintervalbetweeninjury andpresentationlongerthan28dayswereoperatedbya sin-gleelbowspecialist,afterapprovalbytheethicscommittee oftheinstitution.Thediagnosiswasperformedbasedonthe clinicalhistory,physicalexamination,andadditionalexams (Figs.1–3).
Themeanageofthepatientswas47.5years,andthemost commontraumamechanismwasaneccentricloadwiththe elbowinflexionand supination.Two patientswere injured duringweightlifting(tractortireandloadedweightliftingbar) andoneduringafalltotheground.Themeanintervalfrom thedayofthetraumatosurgerywas71.8days.
TheMayo ElbowPerformanceScore(MEPS)and avisual analog scale for pain (VAS) were applied in the pre- and post-operative periods. The assessmentof the flexion and supinationforces wasperformedonlyinthepost-operative period;thecontralateralsidewasusedforcomparison.
Fig.1–Magneticresonancesagittalcutshowingthedistalbicepsinjury.
306
rev bras ortop.2 0 1 6;51(3):303–312Fig.3–Magneticresonanceaxialcutshowingthedistalbicepsinjury.
measurementprocess.Themeanfollow-uptime,withclinical evaluationandscores,was14months(12–19).
Adescriptive analysis ofthe studied variables was per-formed.Due tonon-normalityofdata, the non-parametric testwasusedfordataanalysis.Forthecomparisonbetween thepre-andpost-surgicalmomentsthroughVASandMEPS, andforcomparisonbetweentheoperatedandnon-operated sidesinflexion,extension,supination,andpronationarcs,as wellassupinationandpronationforces,theWilcoxon non-parametrictestwasused.Fortheentirestatisticalinference, ap-valueof0.05wasconsidered.SPSSforWindowsversion 20.0wasused.
Operatingtechnique
All patients were positioned in horizontal dorsal decubi-tus and underwent plexus block anesthesia+sedation. An Esmarch tourniquet was applied to the root of the limb. A singlecurvilinear incision (Fig. 8) ofapproximately 7cm wasmadelightlydistaltotheantecubitalfossa.TheHenry approachwasusedtoexposetheradialtuberosityin supina-tionand abicortical holewasmadewitha4.5-mmdrill. A fine-tipgougewasusedtoextendtheentrypoint(proximal) accordingtothethicknessofthetendonextremity.If neces-sary,asecond smallincisionwasperformedapproximately 5cm proximal tothe elbowflexuretoisolate theretracted
tendonstump.Theretractedtendonstumpusuallypresented itselfsurroundedbyafibrotictissuealongwithitssheath;it wasdecidednottopreservethelacertusfibrosus.The muscle-tendon junctionwas identifiedafterdissectionand release of peritendinous fibrous tissue.Thisprocedure allowedfor alengthgainofaround2–3cm.Twohigh-resistancethreads werepassedthroughthetendonusingtheKrackowtechnique with1-cmintervalsbetweenthem,inordertobecoupledto theEndoButton.
Abluntdissectionwasperformedwiththefingertorelease the bicepsmusclebelly fromthe deepfascia andfrom the deeperbrachialismuscle.Specialcarewastakeninthe iden-tificationofthelateralcutaneousnerveoftheforearm(branch of the musculocutaneous nerve) that passes between the bicepsandthebrachialis(Fig.9).Then,thetendonrepaired withtheEndoButtonwaspassedthroughtheoriginaltunnel belowtheanteriorantecubitalfossauptotheradial tuberos-ity.Theauthorsavoidedexposingthelateralsideoftheulna asmuchaspossibleduetocomplicationssuchasheterotopic ossification.
Fig.4–Dynamometerusedforforcemeasurements.
totwothreadsofEthibond,which,inturn,weretiedtothe extremityoftheEndoButton’sdrillguidewireandwere exteri-orizedthroughthemobiledorsalcompartmentoftheforearm. Then,theEndoButtonwasflippedandcontrolwasperformed throughfluoroscopy(Fig.10).
Fig.5–Markedstickusedtoaidsupinationforce measurement.
Fig.6–Supinationforcemeasurement.
After confirmation of the correct positioning of the EndoButton, an absorbable interference screw (Smith & Nephew, AndoverMA)was usedtoincrease thecontactof thetendonwiththeproximalholeinthemaximumextension positionachievedbytheelbowatthatmoment(Figs.11–13).
Post-operativeprotocol
A Velpeausling wasplacedon the patientin the immedi-atepost-operativeperiod.Ifitwasobservedthatthepatient presentedsomedifficultyinunderstandingtherehabilitation
308
rev bras ortop.2 0 1 6;51(3):303–312Fig.8–Intraoperativeimageoftheincision.
protocol,aplastercastwiththeelbowin90◦flexionand
neu-tralpositionwasplaced.Passiveflexionandactiveextension movementarcswereinitiatedontheseconddayaftersurgery, atthepainthreshold.Theslingwasusedforcomfortonly. Afterthree weeks, the sling was discontinued; active flex-ionexercisesandpassiveextensionexercisesbeganatfour weeks.Strengtheningexerciseswereinitiatedateightweeks andcounterresistanceexercises,attenweeks.Thereturnto sportsactivitieswasallowedafterapproximatelyfourtosix months,afterwell-performedtrainingofthesportmovement.
Fig.9–Intraoperativeimageofthemusculocutaneous nerve.
Fig.10–Intraoperativefluoroscopicimageofthe positioningoftheEndoButton.
Fig.11–Measurementofthediameterofthebicepstendon stump.
Fig.13–Schematicdrawingshowingtwoimplants.
Patientassessment
Themovementarcwasmeasuredwithamanualgoniometer byanexaminer(surgeon)followingthecriteriaofthe Amer-icanAcademyof OrthopedicSurgeons(AAOS). All patients wereassessedusingtheMEPSandtheVAS.9
Results
The results are presented in Tables 1–3. Throughout the months,allpatientsincreasedthemovementarcs.Themean flexionwasofapproximately133◦,correspondingto99%of
thatofthenon-operatedlimb.Themeanextensionwasof2.5◦
offlexion.Twopatientsremainedwithaflexioncontractureof approximately10◦.Themeansupinationwasof88◦andmean
pronationwasof82.5◦,whichcorrespondedto98.5%and98%
ofthatofthecontralaterallimb.
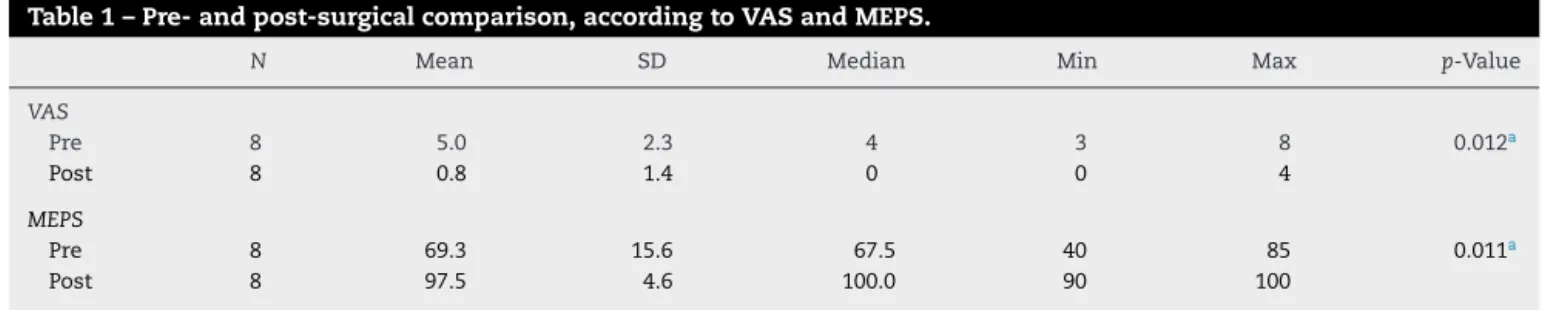
AllpatientsobtainedexcellentresultsintheMEPS,scoring over90◦.ThemeanVASdecreasedfrom5to0.8inthe
post-operativeperiod:astatisticaldifferencewasobservedinboth functionalscores(p<0.05).
The mean flexion force was of17.6N,corresponding to 79.25%ofthatofthenon-operatedside.Themean supina-tionforcewasof2.6N,correspondingto89.75%ofthatofthe non-operatedside.
Complicationssuch asparesthesiainthe lateral faceof theforearm,correspondingtoneuropraxiaofthelateral cuta-neousnerveoftheforearm,wereobservedinonepatientand wereresolvedwithinthreemonths.Therewerenocasesof re-rupture ofthe tendon, fractureofthe radialcortex, and heterotopicossification.
Discussion
Thisseriesofdistalbicepsrupturecasespresentstheclassic epidemiologicalprofileofactivemiddle-agedmales,inwhich the conservativetreatment leadstohigh functionaldeficit. Thesurgicalrepairofthedistalbicepsinjuriesdemonstrates superiorresultswhencomparedwiththeconservative treat-ment.Baker et al. comparedthe conservative and surgical treatment,observingareductioninsupinationforceand resis-tanceof55%and86%,respectively.10
Thereareseveralsurgicaloptionsfortherepairofdistal bicepsruptures.Acuteinjuriescanbetreatedwithprimary repair to the radial bicipital tuberosity or non-anatomical repairwithtendon transferto thebrachialis. Klonzetal.11 compared the transfer to the brachialis tendon with the anatomicalcorrectionthroughsuturewithanchor.Although flexionresistancewasrestored,halfofthepatientsofthe indi-rect repairgrouphad areductionof50%inthe supination force.DeCarlietal.12alsoreportedtheresultsfromindirect repairin23patients,observingareductioninflexion resis-tanceof12%,supinationresistanceof13%,andtotalworkin supinationof25%.Inthepresentstudy,directrepairshowed aflexionandsupinationforceofapproximately80%and90%, respectively,whencomparedwiththecontralateralside.
Distal biceps injuries can be repaired through a single extendedanterioraccessroute(Boyd–Anderson13approach),
Table1–Pre-andpost-surgicalcomparison,accordingtoVASandMEPS.
N Mean SD Median Min Max p-Value
VAS
Pre 8 5.0 2.3 4 3 8 0.012a
Post 8 0.8 1.4 0 0 4
MEPS
Pre 8 69.3 15.6 67.5 40 85 0.011a
Post 8 97.5 4.6 100.0 90 100
310
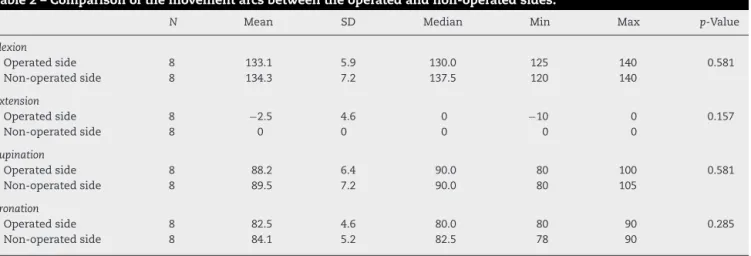
rev bras ortop.2 0 1 6;51(3):303–312Table2–Comparisonofthemovementarcsbetweentheoperatedandnon-operatedsides.
N Mean SD Median Min Max p-Value
Flexion
Operatedside 8 133.1 5.9 130.0 125 140 0.581
Non-operatedside 8 134.3 7.2 137.5 120 140
Extension
Operatedside 8 −2.5 4.6 0 −10 0 0.157
Non-operatedside 8 0 0 0 0 0
Supination
Operatedside 8 88.2 6.4 90.0 80 100 0.581
Non-operatedside 8 89.5 7.2 90.0 80 105
Pronation
Operatedside 8 82.5 4.6 80.0 80 90 0.285
Non-operatedside 8 84.1 5.2 82.5 78 90
Significantdifferenceswerenotobservedbetweentheoperatedandnon-operatedsidesintheassessedmovementarcs.
with two accesses (modified Boyd–Anderson approach), or evenamodifiedendoscopicaccess.Theauthorsusedan ante-rior approach with an incision lightly distal to the elbow flexure,andtherewasnoneedforasecondproximal inci-siontoisolatetheretractedtendonstump.Specialcaremust betakenwhenisolatingthesensorybranchofthe musculo-cutaneousnerve.
Directfixation methodsrangefrom the traditionalbone troughtotherepairwithmodern devices,suchasanchors, EndoButton, and interference screws. The choice of reha-bilitationprotocols willdependpartiallyonthestrength of thereconstructionorrepair.Weinsteinetal.14monitored32 patients treatedusing the technique oftwoincisions with boneanchors. Thepost-operativeprotocol establishedfour weeksofimmobilizationwithasplintandfourmonthsof pro-tectedactivities.Nonetheless,themovementamplitudewas restoredandaDASHscoreof4±7wasobtained.Ciletal.15 also reported the results of the two-incision approach in 21patients,excludingchronicruptures.Theirpost-operative protocolstimulated the startofamplitudeofmovement in the first or second post-operative day, withthe resistance limitedtoonepoundforthefirstsixweeksandtwopounds forthefirstthreemonths.Flexingandpronosupinationwere restored,withmovementarcsfrom0◦ to145◦ andfrom74◦
to75◦,respectively.ThemeanDASHscoreinthatstudywas
3.6±3.6.Thepresentpatientswereimmobilizedonlywitha slingforthreeweeks.Activemovementofwristandfingers
wasallowedinthefirstpost-operativedayand,afterthethird week,passiveflexionandactiveextensionexercisesas toler-ated.Theflexion-extensionandpronosupinationmovement arcsrangedfrom2.5◦to133◦andfrom82.5◦to88.2◦,
respec-tively.
The technique with EndoButton, described for the first time by Bain et al., was efficient in the acute repair, with superior pulloutstrengths whencomparedwithequivalent methods.13,14That,inacertainway,allowsformobilizationin theimmediatepost-operativeperiodandpromotesanearly, gradualextensiongain,withpracticallycompleteextension recovery.Despitethistheoreticaladvantage,thestudies pub-lishedonthetechniquewithEndoButtonhadrehabilitation programswithlimitedorstagedreturntomovement.3,15,16In thepresentstudy,thepatientswithaslingwereallowedto beginmobilizationaroundthethirdweek.Thatallowedthe patientstorecoveralmosttotalextensioninfiveweeks;the authorsbelievethatthiscontributedtotheexcellent move-mentamplitudeobtained.Intwocases,aplastercastwasleft fortwoweeksasaprecautionmeasureduetothecognitive difficultypresentedbythepatients.
Direct repair inchronic ruptures with retracted tendon waspreviouslyreportedas“impossiblewithoutlimitingthe extension.”Tendonretractionshaveforcedsomeauthorsto useinterpositionautografttorecoverpriorelbowextension. Graftusewasrecommendedincaseswheretherepaircould notbereachedbythe nativetendonbeyond70◦ offlexion.
Table3–Forcecomparisonsbetweenoperatedandnon-operatedsides.
N Mean SD Median Min Max p-Value
Flexionforce
Operatedside 8 17.6 2.9 18.1 13.2 21.4 0.012a
Non-operatedside 8 22.4 2.6 22.5 18.1 25.5
Supinationforce
Operatedside 8 2.6 0.5 2.6 2.0 3.9 0.327
Non-operatedside 8 2.9 0.5 2.9 2.0 3.9
Significantdifferenceswereobservedintheflexionforcebetweentheoperatedandnon-operated.Thenon-operatedsidepresentedbigger force.
Bainetal.16usedEndoButtontorepair12acuteinjuriesand onechronicinjury,throughautologoussemitendinosusgraft toprovideretraction. Themovementamplitude duringthe follow-upwasof5–146◦,withpronosupinationof81–80◦.The
forcewasmeasuredsubjectivelyat5/5.Despitetheevolution timeofthepresentpatients,interferencescrewswereplaced withapproximately90–110◦offlexion,andyetnocasesof
flex-ioncontractureorsignificantextensiondeficitwereobserved. Inlaterepairs,evenwithwidemobilization,theretracted tendonextremitycanonlybebroughttotheradialinsertion withmaximum elbowflexion.8,15,17,18 Thehigherthe elbow flexion,themoredifficultitistoinsertinterferencescrewsor toperformsuturesinthevolarsurface.Theadvantageofthe EndoButtonisthatitallowsforthepassageofthetendonby theradiustobedoneblindly,withtractiononthetendonand theEndoButtonmaintainedinthelineoftraction.Thepassage ofthethreadscanbeperformedusingabluntguidewirewith diameteroflessthan2mm,whichmakesinjuryof neurovas-cularstructuresunlikely.ThetechniquewiththeEndoButton issafe. Cadaver studies show that the posteriorinterbone nerveisdistalaround7–14mmtotheplaceofthepassageof theEndoButton.19,20AstheEndoButtonisflipped,theelbow canbeextendedandthepassageofthetendoninthebonecan beseendirectlyfortheinsertionoftheinterferencescrew.
Although the authors have been able to reposition the tendoninallcases,thereisthepossibilityofexcessive fibro-sisformationorpoorqualityresidualtendon. Sincethat is assessedonlyinthe intraoperativeperiod, it isprudent to prepareaninformedconsentformtoharvestatendongraftif necessary.Inthepresentoperatedcases,allrepairedtendons managedtoreachtheradialtuberositywithoutgreattension, whichtheauthorsbelievetobearesultoftheintegrityofthe lacertusfibrosusinthevastmajorityofthecases.
Complicationratesofupto31%werereportedafteracute repair.21,22Themainrisksareinjuryofthelateralcutaneous nerveofthe forearmand ofthe posteriorand radial inter-bonenerve,inadditiontosurgicalwoundinfection,flexion contracture,and heterotopic ossification.Similar complica-tionrateswereobservedforoneortwoincisions,eventhough anadditionalsynostosisriskhasbeenreportedwithasecond posteriorapproachversustheincreaseoftheriskofparalysis ofthe radialnerveinthe single-incision method.The ear-liertherepair,thelowerthecomplicationrisk.Bissonetal.23 demonstratedacomplicationrateofupto40%whentherepair tookplace 14 daysor moreafterthe injury, versus 20% in earlyrepair.Therateofcomplicationsinthe presentstudy waslower,despitethefactthattherepairswerelate(28–180 days).Nopatientpresentedinjuryoftheposteriorinterbone nerve.Thelateralcutaneousnerveoftheforearmwasadhered tothedeepfaceofthe bicepsandatriskwhenthemuscle wasmobilized.Despitethecaretaken,onepatientdeveloped transitoryneuropraxiaofthelateralcutaneousnerveofthe forearm,whichwasresolvedwithinthreemonths.
Thetechniqueofthedirectrepairofdistalbicepschronic injuries allows for a good fixation of the tendon, as well asmovementarcrecoveryandgoodflexionandsupination forces,withlowratesofcomplication.
Thesmallnumberofcases,typeofstudy(caseseries with-outcomparativesample),andthecostofthetechnique(dueto theuseoftwoimplants)areweaknessesofthepresentstudy.
Fig.14–Cosmeticaspectoftheincision.
Thestrengths ofthe studyincludethelowmorbidityof theprocedure,avoidinguseofgraftsdespitethefactthatthe injurieswerechronic;thesingleaccessroute,whichallowsfor visualization andisolationofneurovascular structures;and thegoodcosmesis(Fig.14).Therigidandmoreresistant fix-ationofthetendonwithtwoimplantsallowsforanearlier rehabilitationwithoutplasterimmobilization.
Conclusions
Chronic injuriesofthe distalbicepscan leadtofunctional deficitsinyoungadultswhoperformanyphysicalorathletic activity.Theuseofthedirectrepairtechniquewith EndoBut-tonandinterferencescrewsisasafeandefficientoptionfor chronicinjuriesofthedistalbicepswithoverfourweeksof evolution.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.McDonaldLS,DewingCB,ShupePG,ProvencherMT. Disordersoftheproximalanddistalaspectsofthebiceps muscle.JBoneJointSurgAm.2013;95(13):1235–45. 2.GeaneyLE,MazzoccaAD.Bicepsbrachiitendonruptures:a
reviewofdiagnosisandtreatmentofproximalanddistal bicepstendonruptures.PhysSportsmed.2010;38(2):117–25. 3.MazzoccaAD,BurtonKJ,RomeoAA,SantangeloS,AdamsDA,
312
rev bras ortop.2 0 1 6;51(3):303–3124. D’AlessandroDF,ShieldsCLJr,TiboneJE,ChandlerRW.Repair ofdistalbicepstendonrupturesinathletes.AmJSportsMed. 1993;21(January(1)):114–9.
5. FlintJH,WadeAM,GiulianiJ,RueJP.Definingthetermsacute andchronicinorthopaedicsportsinjuries:asystematic review.AmJSportsMed.2014;42(1):235–41.
6. KettlerM,TingartMJ,LungerJ,KuhnV.Reattachmentofthe distaltendonofbiceps:factorsaffectingthefailurestrength oftherepair.JBoneJointSurgBr.2008;90(1):103–6.
7. RiosCG,MazzoccaAD.Interferencescrewwithcortical buttonfordistalbicepsrepair.SportsMedArthrosc. 2008;16(3):136–42.
8. BainGI,PremH,HeptinstallRJ,VerhellenR,PaixD.Repairof distalbicepstendonrupture:anewtechniqueusingthe Endobutton.JShoulderElbowSurg.2000;9(2):120–6. 9. BrobergMA,MorreyBF.Resultsofdelayedexcisionofthe
radialheadafterfracture.JBoneJointSurgAm. 1986;68(5):669–74.
10.BakerBE,BierwagenD.Ruptureofthedistaltendonofthe bicepsbrachii,operativeversusnon-operativetreatment.J BoneJointSurgAm.1985;67(3):414–7.
11.KlonzA,EggersC,ReilmannH.Proximalanddistalbiceps tendonrupture–anindicationforsurgery?Unfallchirurg. 1998;101(9):735–9.
12.DeCarliA,ZanzottoE,VadalàAP,LuzonD,DiSalvoM, FerrettiA.Surgicalrepairofthedistalbicepsbrachiitendon: clinicalandisokineticlong-termfollow-up.KneeSurgSports TraumatolArthrosc.2009;17(7):850–6.
13.BoydH,AndersonL.Amethodforreinsertionofthedistal bicepsbrachiitendon.JBoneJointSurgAm.1961;43:1041–3. 14.WeinsteinDM,CicconeWJ2nd,BucklerMC,BalthropPM,
BuseyTD,EliasJJ.Elbowfunctionafterrepairofthedistal
bicepsbrachiitendonwithatwo-incisionapproach.J ShoulderElbowSurg.2008;17Suppl.1:82S–6S.
15.CilA,MertenS,SteinmannSP.Immediateactiverangeof motionaftermodified2-incisionrepairinacutedistalbiceps tendonrupture.AmJSportsMed.2009;37(1):130–5.
16.BainGI,JohnsonLJ,TurnerPC.Treatmentofpartialdistal bicepstendontears.SportsMedArthrosc.2008;16(3):154–61. 17.BosmanHA,FincherM,SawN.Anatomicdirectrepairof
chronicdistalbicepsbrachiitendonrupturewithout interpositiongraft.JShoulderElbowSurg.2012;21(10): 1342–7.
18.DillonMT,BollierMJ,KingJC.Repairofacuteandchronic distalbicepstendonrupturesusingtheEndoButton.Hand (NY).2011;6(1):39–46.
19.KettlerM,LungerJ,KuhnV,MutschlerW,TingartMJ.Failure strengthsindistalbicepstendonrepair.AmJSportsMed. 2007;35(9):1544–8.
20.EamesMH,BainGI,FoggQA,vanRietRP.Distalbicepstendon anatomy:acadavericstudy.JBoneJointSurgAm.
2007;89(5):1044–9.
21.KlonzA,LoitzD,WöhlerP,ReilmannH.Ruptureofthedistal bicepsbrachiitendon:isokineticpoweranalysisand complicationsafteranatomicreinsertioncomparedwith fixationtothebrachialismuscle.JShoulderElbowSurg. 2003;12(6):607–11.
22.LoitzD,KlonzA,ReilmannH.Techniqueofdistalbiceps tendonrepairusingalimitedanteriorapproach. Unfallchirurg.2002;105(9):837–42.