(1) Universidade Estadual de Campinas/ UNICAMP, Campinas, São Paulo, Brasil.
Conlict of interest: Nonexistent
The impact of oronasal breathing
on perioral musculature
Fabíola Maria Gonçalves Félix Mattos(1)
Fausto Bérzin(1)
Mirian Hideko Nagae(1)
Received on: August 11, 2017 Accepted on: October 20, 2017
Mailing address:
Mirian Hideko Nagae
Av. Paulista 1195/152, Bela Vista CEP: 01310-200 - São Paulo, São Paulo, Brasil
E-mail: [email protected]
ABSTRACT
Purpose: to compare the behavior of perioral muscles in nasal, oral and oronasal
respirators.
Methods: a sample consisting of three distinct groups, equally subdivided into Nasal, Oral and Oronasal Respirators. The behavior of the orbicular muscle of the mouth (upper part) and mentual one was measured by surface electromyography at rest, swallowing and labial isometry.
Results: in all situations investigated, the orbicular muscle of the mouth (upper part) and mental muscle showed no signiicant difference in relation to Root Means Square,
that is, average electrical activity between Oral and Oronasal Respirators. The data sho-wed a signiicant difference in In Nasal Respirators, as compared to the other groups. Conclusion: similarity was seen in the comparison of perioral muscles behavior between oral and oronasal respirators, however, a signiicant difference in relation to
nasal respirators.
INTRODUCTION
The breath, physiological, vital and innate function of the human being, protects the upper airway and allows the satisfactory development of the craniofacial complex if performed correctly1-4. For proper nasal
breathing, lip sealing is indispensable for generating a differentiation system of intra and extra-oral pressures in the so-called Oronasopharyngeal Space. This system, in turn, is responsible for the adequate maintenance of muscle tone5 that favors the correct development of the
oral cavity, since there is a bone and dental response to muscle action6,7.
When, however, nasal respiratory failure due to obstructive or non-obstructive causes occurs, compen-satory mechanisms such as oral breathing can be triggered8,9. In this case, a new pressure condition is
generated and the musculature needs to be readapted5.
In the literature, damages caused by oral breathing due to a new muscular condition are already consecrated10.
As well as the new condition sequelae: open bite, retrognathism, high and narrow palate among others11.
Although, in the oronasal respirator – also called vicious12,13, mixed 14 or partial8,15 – even after clearing
the upper airways, the systematic nasal breathing does not occur. Either by habit or muscle memory the mouth remains ajar. In these cases, muscle activity has never been investigated. Perhaps because it is considered that intra and extra-oral pressure differentiation does not interfere with muscular behavior16. Or because it is associated with chronic diseases of dificult treatment
and continuous control such as rhinitis17,18. Thus, albeit
the oronasal respirator is considered a distinct group19,
it is often disregarded or grouped as an oral respirator. If, however, the musculature in the oronasal respi-rator is compromised in the same way as in the oral respirator, some care must be guaranteed, once the incidence of chronic diseases20,21 is high, such as rhinitis
in children, from 26.6% to 53.3%22. Unfortunately,
when untreated, they can cause similar morphological damage to the mouth respirator, besides compromising orthodontic interventions with relapses or treatment limitations due to inadequate muscular action23.
In particular, two muscles have a signiicant partici -pation with the oral cavity development, the orbicu-laris muscle of the mouth (upper part) and the mental
activities such as suction and swallowing23,24. On the
other hand, the mental muscle23,25, which is
respon-sible for positioning and directing the lower lip23, is
hypertrophied in the oral respirator due to its excessive recruitment when sealing the lips26. With a volume
increase, it tends to accentuate the eversion of the lower lip23 and the buccal inclination of the incisive
teeth27, since its insertion lies in the alveolar eminence
of the canine teeth to the lateral incisors 25.
Due to the expressive participation of the orbicular muscles of the mouth and mentual muscles in skeletal and dental development, this study aims to compare the behavior of the perioral muscles in nasal, oral and oronasal respirators.
METHODS
The study was approved by the Research Ethics Committee of UNICAMP under No. 1,125,115 according to Resolution 466/12 of the National Health Council (CNS). The legal representatives of the selected patients signed the Free and Informed Consent Form for the authorization of data collection.
Sample
It’s consisted of 48 patients, divided equally into three groups: Nasal Respirators (RN), Oral Respirators (ORO) and Oronasal Respirators (RON), aged between 6 and 12 years old, male and female, selected from the waiting list of a Basic Health Unit.
• Inclusion criteria: medical records of otorhinolaryn-gological evaluation of the upper airways.
NASAL RESPIRATOR: clearing of the upper airways with effortlessly sealed lips during rest, chewing and with the tongue contained in the oral cavity28.
ORAL RESPIRATOR: obstruction of the upper
airways, breathing with dificulty through the nose,
showing signs of fatigue, dyspnea and needing to open the mouth to inspire when at rest and chewing28.
ORONASAL RESPIRATOR: clearing of the upper airways, breathing through the mouth and nose, but being able to breathe through the nose without showing signs of fatigue or dyspnea28.
Procedures
The evaluation consisted of the analysis of the medical records for the investigation of otorhinolaryngo-logical opinion regarding the respiratory mode, protocol of Miofunctional Evaluation with Scores (AMIOFE)28
and electromyographic examination. AMIOFE was
also used to deine the respiratory mode28, being this
protocol applied integrally once the observation of the
patient throughout the evaluation is necessary to deine
different respiratory modes.
Figure 1 measures the different respiratory modes. However, in this study, mild oronasal breathing was considered Oronasal Respiration and severe oronasal breathing, Oral Respiration.
Breathing Scores
Nasal breathing Normal (3)
Oronasal breathing Mild (2)
Result of the evaluated subject Severe (1)
Figure 1. AMIOFE Protocol. Speciic cut-off of the “functions” criterion for respiratory mode
In order to deine the different respiratory modes,
the protocol considers the following characteristics:
• Nasal Respiration (normal nasal breathing): lips sealed effortlessly during rest and chewing with the tongue contained in the oral cavity.
• Oronasal breathing (mild oronasal breathing):
breathing through the nose and mouth without showing signs of fatigue or dyspnea.
Oral Respiration (severe oronasal breathing):
breathing with dificulty, showing signs of fatigue,
dyspnea and needing to open the mouth to breathe at rest and chewing.
Surface Electromyography
The study was carried according to the recom-mendations of the European Applications of Surface Electromyography (SENIAM)29. Myosystem and
Myosystem BRI software, version 2.52, 12-bit resolution signal conditioner with 112 dB Common Rejection Mode, 60 Hz and Myosystem Digital Analog Converter, model PCI-DAS 1200, were used.
Bipolar disposable electrodes of Chicopee MA01 (Meditrace, Kendall-LTP) with a diameter of 1cm were
coupled to a preampliier (model PA 1010-VA, 20-fold
gain) to form a differential circuit. This circuit subtracts
the common signal and ampliies the differential signal
of interest to attenuate artifacts and avoid crosstalk30,31.
The monopolar stainless steel reference electrode was
attached to the sternum of the patient. In the other muscles, the inter-electrode distance was 1cm, and in the mental muscle it was positioned in its womb to 2mm below the edge of the lower lip and in the orbicu-laris muscle of the mouth (upper part) in its midline13.
To capture the signal, the sampling frequency was 2 kHz. After collecting, the signals were submitted to
a Butterworth ilter, bandpass of 20-500 Hz, rectii
-cation with low-pass ilter of 4 Hz and calculation of the
average electrical activity of the signal through Root Means Square (RMS)31,32.
The duration of the records was 5 seconds at rest, swallowing and labial isometry, with one-minute interval between the abstractions33. For swallowing,
1ml of water was inserted into the patient’s mouth with a syringe and after 60 seconds the swallowing was requested. Finally, for isometry the patient maintained an eccentric contraction of the lips for 5 seconds. The tests used were Chi-Square, Fisher, ANOVA and Box Plot, and the value considered signiicant was p <0.05.
RESULTS
Sample characterization
In the comparison between NG, GO and GON – regarding to the male and female gender – there was
no signiicant difference between the groups, according
In the electromyographic data between the groups there was similarity between ORO and RON, and a
signiicant difference in relation to RN. Also a signiicant
difference between both muscles. However, there was no correlation between the group and muscle factor.
Regarding age, the data also showed no signiicant
difference between the groups, according to Table 2.
Table 3 below quantiied the values of the electro -myographic examination in the Group / Muscle ratio.
Table 3. Quantitative description of Root Means Square (RMS), mean electric activity of the Groups / Muscle ratio in electromyography
(ANOVA for repeated measures)
Group Variable N Mean Mediam SD Minimum Maximum
RN
rephab (m.orbicular) 16 4.23 3.61 2.30 1.25 7.89
rephab (m.mentual) 16 6.64 7.44 3.36 0.77 11.31
degl (m.orbicular) 16 5.87 5.28 3.57 0.77 13.82
degl (m.mentual) 16 10.88 9.87 9.32 1.74 39.15
labial isometry (m.orbicular) 16 6.72 6.01 5.23 0.65 18.04 labial isometry (m.mentual) 16 30.46 10.82 42.07 2.81 160.77
RO
rephab (m.orbicular) 16 10.33 8.10 7.10 4.09 31.39
rephab (m.mentual) 16 22.32 16.37 21.49 5.45 92.53
degl (m.orbicular) 16 28.37 19.45 28.92 6.42 103.68
degl (m.mentual) 16 52.88 50.07 19.21 27.53 91.48
labial isometry (m.orbicular) 16 69.14 55.02 63.48 6.79 220.53 labial isometry (m.mentual) 16 101.27 70.45 60.16 30.90 205.78
RON
rephab (m.orbicular) 16 6.36 5.67 5.37 1.32 20.08
rephab (m.mentual) 16 15.84 13.76 10.97 5.04 41.13
degl (m.orbicular) 16 25.76 24.53 21.96 3.25 79.66
degl (m.mentual) 16 40.77 43.65 17.87 6.23 71.01
Table 1. Gender-speciic sampling in different respiratory patterns
Gender Groups Total
RN RO RON
Female (freq.) 5 6 4 15
% 31.25 37.50 25
Male (freq.) 11 10 12 33
% 68.75 62.50 75.00
TOTAL 16 16 16 48
RN: Nasal Respirator, RO: Oral Respirator; RON: Oronasal Respirator p: 0.7476 (Chi-Square and Fisher, p <0.05), frequency: %, percentage.
Table 2. Sampling in relation to age
Group N Mean Median SD Minimum Maximum
RN 16 7.94 7.5 2.05 6.0 12
RO 16 6.69 6.0 1.01 6.0 9
RON 16 7.00 6.0 1.37 6.0 10
difference in relation to RN. Finally, in the analysis
separated by group only RN did not present signiicant
difference between the muscles, according to Figure 2 below:
Thus, in the separated analysis the mental muscle presented a difference between the groups; and the orbicularis muscle of the mouth (upper part) presented
similarity between ORO and RON, and a signiicant
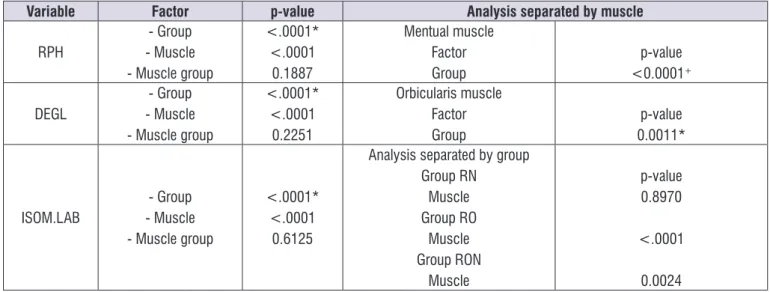
Variable Factor p-value Analysis separated by muscle
RPH
- Group - Muscle - Muscle group
<.0001* <.0001
0.1887
Mentual muscle Factor
Group <0.0001p-value+
DEGL - Muscle- Group - Muscle group
<.0001* <.0001
0.2251
Orbicularis muscle Factor
Group 0.0011*p-value
ISOM.LAB - Muscle- Group - Muscle group
<.0001* <.0001
0.6125
Analysis separated by group Group RN
Muscle Group RO
Muscle Group RON
Muscle
p-value 0.8970
<.0001
0.0024
Figure 2. Electromyographic data between the groups and analysis dismembered by muscle; with variables: RPH (rest in usual position),
DEGL (swallowing) and ISOM. LAB (labial isometry)
The results showed that in the mental and orbicular
muscles of the mouth there was a signiicant difference
for the three studied groups with smaller measures for NG and similar for GO and GON. However, there was no
signiicant difference in relation to the orbicular muscles
of the mouth (upper part) and mentual muscles, but in
GO and GON groups there was a signiicant difference
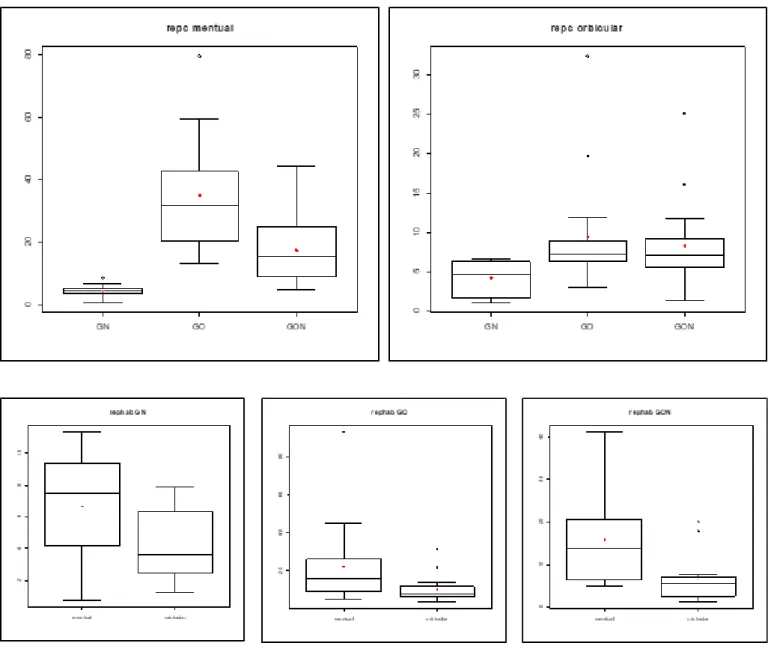
Figure 3. Box Plot for the distribution of the average electrical activity of the electromyographic record in relation to RMS (Root Means
Square) in the usual rest (repc) of the mentual muscle, orbicularis muscle of the mouth (upper part) of nasal, oronasal. ANOVA for repeated measurements. Signiicant difference * (Tukey’s test). * RN ≠ RO / RON
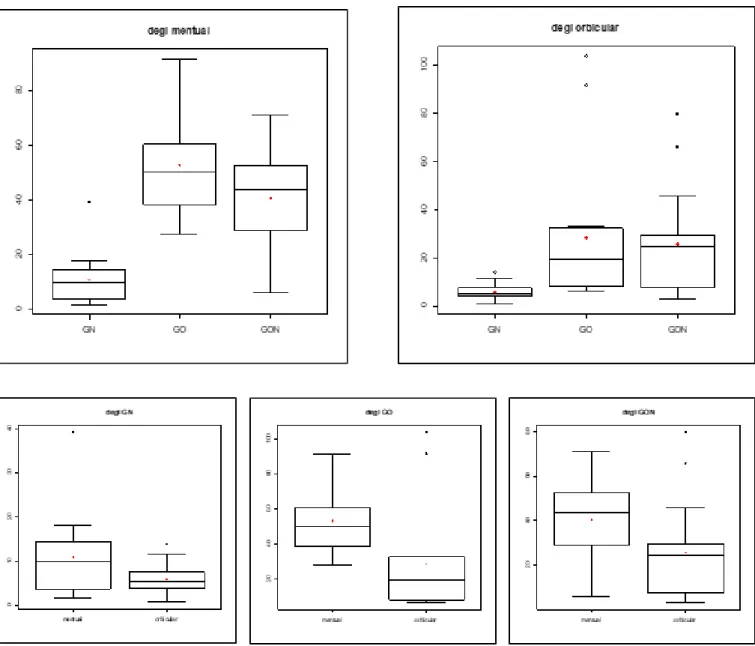
DEGLUTITION
Figure 4. Box Plot for the distribution of the average electrical activity of the electromyographic record in relation to RMS (Root Means
DISCUSSION
The data revealed that the behavior of the perioral musculature in the oronasal respirator is similar and in some muscles even more intense than in the oral respi-rator. To characterize RON as a distinct group some care was taken. Besides the otorhinolaryngological
evaluation, a speciic protocol – Myofunctional Orofacial
average age obtained in the study was ± 7.21 years
old, with no signiicant difference between RN, ORO
and RON, p: 0.1550 (Table 2). Similarly with gender, among the groups RN, ORO, RON, p: 0.07476 (Table 1), whose data go against literature1,2 which disregards
the equal distribution of gender in the group and only
stands out the classiication to presence or absence of
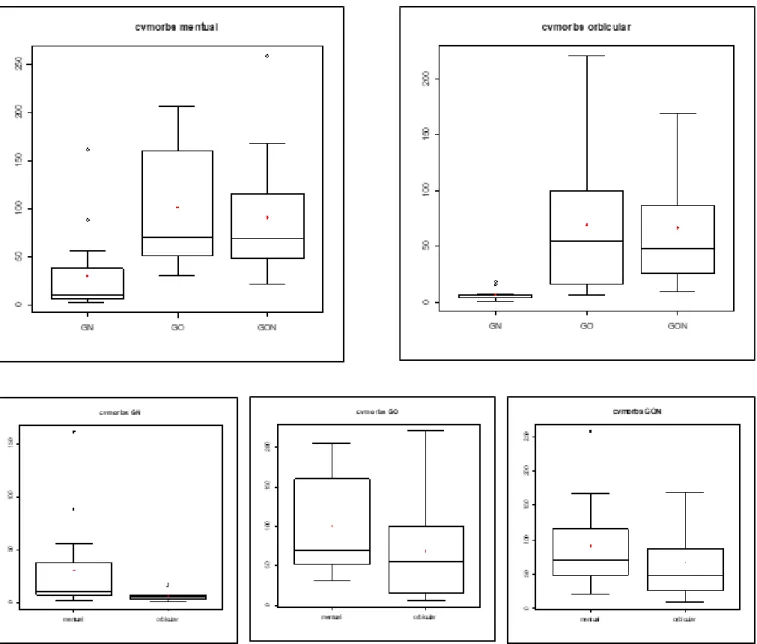
nasal obstruction. ISOMETRY LIP
Figure 5. Box Plot for the distribution of the average electrical activity of the electromyographic record in relation to the RMS (Root Means
Means Square (RMS) was used to measure the average electrical activity of the signal 19. The orbicularis
muscle of the mouth (upper part) presented similarity
between ORO and RON, and signiicant difference in relation to RN. In the mental muscle, a signiicant
difference was found in all the situations investigated34
(Figures 3, 4, 5).
In the usual rest, the literature considers absence of
muscular activity values of up to 5μv35. In this study, the
orbicularis muscle of the mouth (upper part) presented
an average RMS value of 3.61μv considered normal, and the mental muscle, 7.44μv, close to the normality
pattern. In ORO and RON groups, RMS values were much higher in the orbicularis muscle of the mouth (upper part) and in the mentual34 (Table 3). These results conirm that not only intra-oral pressure is different in the ineficient labial sealing, as well as the
behavior of the perioral muscles5.
During swallowing and labial isometry there was also a pattern of similar behavior: GRN low values, GRO and GRON elevated (Figures 3, 4). As muscular dynamics
inluences skeletal and occlusal development, the
obtained data in the GRO and GRON agree with studies associating ORO with cases such as retrognathism and open bite27. The results are reafirmed as the three
situations – habitual rest, swallowing and lip isometry –
presented a proile of similar behavior with progressive
increase of RMS when performed in this sequence due to the need for greater recruitment so the activities could be performed26 (Figures 3, 4, 5).
Another signiicant difference found was regarding
the mental muscle. In the analysis between muscles in ORO and RON groups, in swallowing and isometry,
their activity was high and signiicant (Figures 3,
4, 5)23. Such indings are probably related to two
aspects: anatomical location and function exerted by the muscle. In other words, the insertion in the inferior incisor muscle, which in turn has the function of the labial depression, in the case of ORO, requires the mental muscle to be more recruited to maintain the lip seal. About the function of positioning and directing the lower lip, there is also a need for greater effort because the lips are half open23.
CONCLUSION
In the comparison of the behavior of the perioral muscles between oral and oronasal respirators, there
was similarity but very signiicant difference in relation
to nasal respirators.
ACKNOWLEDGEMENTS
The authors would like to thank Dr Claudia Maria de Felício - Faculdade de Medicina de Ribeirão Preto/ Universidade de São Paulo - Speech Pathology and Audiology undergrade course, for her technical support in the application of the AMIOFE protocol.
REFERENCES
1. Hitos S, Arakaki R, Solé D, Weckx LLM. Oral breathing and speech disorders in children. J Pediatr. 2013;89(4):361-5.
2. Berwig LC, Silva AMT, Côrrea ECR, Moraes AB, Montenegro M, Ritzel RA. Quantitative analysis of the hard palate in different facial typologies in nasal and mouth breathers. Rev. CEFAC. 2012;14(4):616-25.
3. Rodrigues JA, Silva BNS, Baldrighi SEZM, Paranhos LR, César CPHAR. Interference of mouth breathing with orthodontic treatment duration in Angle Class II, Division 1. Rev. odontol. UNESP. 2017;46(3):184-8.
4. Busanello SAR, Dutra APB, Corrêa ECR, Silva AMT. Electromyographic fatigue of orbicular oris muscles during exercises in mouth and nasal breathing children. CoDAS. 2015;27(1):80-8.
5. Knösel M, Jung K, Kinzinger G, Buss O, Engelke W. A controlled evaluation of oral screen effects on intra-oral pressure curve characteristics. European Journal of Orthodontics. 2010;32(5):535-41.
6. Malhotra S, Gupta V, Pandey RK, Singh SK, Nagar
A. Dental consequences of mouth breathing in the pediatric age group. Int J Oral Health Sci. 2013;3(2):79-83.
7. Bueno SB, Bittar TO, Vazquez FL, Meneghim MC, Pereira AC. Association of breastfeeding, paciier
use, breathing pattern and malocclusions in preschoolers. Dental Press J Orthod. 2013;18(1):30. e1-6.
8. Oliveira RLB, Noronha WP, Bonjardim LR. Masticatory performance evaluation in patients with nasal and mouth breathing. Rev. CEFAC. 2012;14(1):114-21.
9. Machado PG, Mezzomo CL, Badaró AFV. Body
posture and the stomatognathic functions in mouth breathing children: a literature review. Rev. CEFAC. 2012;14(3):553-65.
11. Pacheco AB, Silva AMT, Mezzomo CL, Berwig LC, Neu AP. Relation between oral breathing and nonnutritive sucking habits and stomatognathic system alterations. Rev. CEFAC. 2012;14(2):281-9. 12. Migliorucci RR, Passos DCBOF, Berretin-Felix
G. Orofacial myofunctional therapy program for individuals undergoing orthognathic surgery. Rev. CEFAC. 2017;19(2):277-88.
13. Rezende MS, Carvalho LC, Prado RAM, Rocha CBJ,
Silva VR, Lunes DH. Isostretching method effects
on lung function and posture of mouth breathers. ConScientiae Saúde. 2016;15(1):89-95.
14. Brustolin JP, Dalpian DM, Zanatta FBB, Casagrande L. Associação entre história de aleitamento e relatos de hábitos orais e alergia em crianças. Rev. Fac. Odontol. Porto Alegre. 2012;53(2):11-4.
15. Andrada e Silva MA, Marchesan IQ, Ferreira LP, Schmidt R, Ramires RR. Posture, lips and tongue tone and mobility of mouth breathing children. Rev. CEFAC. 2012;14(5):853-60.
16. Engelke W, Jung K, Knösel M. Intra-oral compartment pressure: a biofunctional model and experimental measurements under different conditions of posture. Clin. Oral Investig. 2011;15(2):165-76.
17. Lopes TSP, Moura LFAD, Lima MCMP.
Association between breastfeeding and breathing pattern in children: a sectional study. J Pediatr. 2014;90(4):396-402.
18. Popoaski C, Marcelino TF, Sakae TM, Schmitz LM, Correa LHL. Avaliação da qualidade de vida em pacientes respiradores orais. Arq Int Otorrinolaringol. 2012;16(1):74-81
19. Nagae MH, Alves MC, Kinoshita RL, Bittencourt ZZLC, Gagliardo H. Life quality for mouth and oronasa lbreathing subjects. Rev. CEFAC. 2013;15(1):105-10.
20. Imbaud TCS, Mallozi MC. Frequência de rinite e alterações orofaciais em pacientes com má oclusão dentária. Rev Paul Pediatr. 2016;34(2):184-8.
21. Brandão HV, Vieira GO, Vieira TO, Cruz AA,
Guimarães AC, Camargos CTP et al. Acute viral bronchiolitis and risk of asthma in schoolchildren: analysis of a Brazilian newborn cohort. J. Pediatr. 2017;93(3):223-9.
23. Brodie AG. Muscular factors in the diagnosis and treatment os malocclusions Angle Orthodontist. 1953;23(2):71-7.
24. Sinno MD , Zide BM. Chin ups and downs: Avoiding bad results in chin reoperation. Aesthetic Surgery Journal. 2017;37(3):257-63.
25. Hur MS, Kim HJ, Choi BY, Hu KS, Kim HJ, Lee KS. Morphology of the mentalis muscle and its relationship with the orbicularis oris and incisivus labii inferioris muscles. Journal of Craniofacial Surgery. 2013;24(2):602-4.
26. Schievano D, Rontani RMP, Berzin F. Inluence of
myofunctional therapy on the perioral muscles. Clinical electromyographic evaluations. J. Oral Rehabil. 1999;26(7):264-9.
27. Graber TM. Orthodontics, principles and pratice. 3th ed. Philadelphia: Saunders; 1972.
28. Felicio CM, Ferreira CLP. Protocolof orofacial myofunctional evaluation with scores. Int J Pediatr Otorhinolaryngol. 2008;72(3):367-78.
29. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electr Kinesiol. 2000;10(5):361-74.
30. Cai C, Au IP, An W, Cheung RT. Facilitatory and inhibitory effects of Kinesio tape: fact or fad? J Sci Med Sport. 2016;19(2):109-12.
31. Nagae MH, Bérzin F, Alves MC. Exacerbated activity of the buccinator muscle in subjects Angle Class III malocclusion. Rev Odontol UNESP. 2012;41(6):384-9.
32. Oliveira LF, Palinkas M, Vasconcelos PB, Regalo IH, Cecilio FA, Oliveira EF et al. Inluence of age on the
electromyographic fatigue threshold of the masseter and temporal muscles of healthy individuals . Archives of Oral Biology. 2017;84:1-5. Doi: https:// doi.org/10.1016/j.archoralbio.2017.09.004
33. Po JMC, Kiser JÁ, Gallo LM, Tésenyi AJ, Herbison P, Farella M. Time frequency analysis of chewing activity in the natural environment. J. Dent. Res. 2011;90(10):1206-10.
34. Souza DR, Semeghini LB, Bérzin F. Oral myofunctional and electromyographic evaluation of the orbicularis oris and mentalis muscles in patients with class II/1 a division malocclusion submitted