REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
REVIEW
ARTICLE
Current
concepts
on
hemodynamic
support
and
therapy
in
septic
shock
Leonardo
Lima
Rocha,
Camila
Menezes
Souza
Pessoa,
Thiago
Domingos
Corrêa,
Adriano
José
Pereira,
Murillo
Santucci
Cesar
de
Assunc
¸ão,
Eliézer
Silva
∗IntensiveCareUnit,HospitalIsraelitaAlbertEinstein,SãoPaulo,SP,Brazil
Received23September2014;accepted11November2014 Availableonline9July2015
KEYWORDS Septicshock; Hemodynamics; Resuscitation; Fluidtherapy; Vasoconstrictor agents
Abstract Severesepsisandsepticshockrepresentamajorhealthcarechallenge.Muchofthe improvementinmortalityassociatedwithsepticshockisrelatedtoearlyrecognitioncombined withtimelyfluidresuscitationandadequateantibioticsadministration.Themaingoalsof sep-ticshockresuscitationincludeintravascularreplenishment,maintenanceofadequateperfusion pressureandoxygendeliverytotissues.Toachievethosegoals, fluidresponsiveness evalua-tionandcomplementaryinterventions---i.e.vasopressors,inotropesandbloodtransfusion ---may benecessary.Thisarticleisaliteraturereviewoftheavailable evidenceontheinitial hemodynamicsupportofthesepticshockpatientspresentingtotheemergencyroomortothe intensive careunitandthemaininterventionsavailabletoreachthosetargets,focusingon fluidandvasopressortherapy,bloodtransfusionandinotropeadministration.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE Choqueséptico; Hemodinâmica; Reposic¸ãovolêmica; Fluidoterapia; Agentes
vasoconstritores
Conceitosatuaissobresuportehemodinâmicoeterapiaemchoqueséptico
Resumo Asepsegraveeochoquesépticosãoumgrandedesafioparaaassistênciamédica. Grande parte da melhora na taxa de mortalidade associada ao choque séptico está rela-cionada ao reconhecimentoprecoce em combinac¸ãocom areposic¸ão volêmicaoportuna e aadministrac¸ãoadequadadeantibióticos. Osprincipaisobjetivos dareanimac¸ãodochoque sépticoincluemreposic¸ãointravascular,manutenc¸ãoadequadadapressãodeperfusãoe fornec-imentodeoxigênioparaostecidos.Paraatingiressesobjetivos,aavaliac¸ãodaresponsividade do volume e das intervenc¸ões complementares(vasopressores, inotrópicos etransfusão de sangue)podesernecessária.Esteartigoéumarevisãodaliteraturaparaidentificaras evidên-ciasdisponíveisdosuportehemodinâmicoinicialaospacientescomchoquesépticoadmitidos emsaladeemergênciaouunidadedeterapiaintensivaeasprincipaisintervenc¸õesdisponíveis
∗Correspondingauthor.
E-mail:[email protected](E.Silva). http://dx.doi.org/10.1016/j.bjane.2014.11.006
para atingir essas metas, comfoco em terapia comreposic¸ão de líquidos evasopressores, transfusãodesangueeadministrac¸ãodeinotrópicos.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Sepsis,asystemicinflammatoryresponseassociatedtoan infection,isacommondiseasewithanestimatedincidence of 300 cases per 100,000 people and with an incidence increase of 13% per year.1,2 Approximately half of septic patientswilldevelopthemostseverespectrumofthis dis-ease,i.e.severesepsisandsepticshock.3
Septicshockcarriesanaveragein-hospitalmortalityrate around20%anda 90day mortalityratebetween 20%and 50%.4---10InBrazil,the28daymortalityrateachievesaround 50%withanincidencedensityofthirtycasesperthousand patient-days.11
Septicshockisalsoassociatedwithhighburdenof mor-bidityandcosts.TheaveragecostperpatientisUS$22,100, whichaccountsforanannualexpenditureofapproximately seventeenbilliondollarsintheUnitedStatesalone.1 Addi-tionally,thequalityoflifeandcognitivefunctionofsepsis survivorsmaybepermanentlycompromised.12---14Key inter-ventionstoimproveoutcomesinthispopulationofcritically ill patients include early recognition and early onset of adequate therapy, mainly broad-spectrum antibiotics and fluids.15
Theinitialattemptstooptimizehemodynamicsin criti-calcare patientsweredeemed ineffective,increasingthe riskof death.16,17 During thepast decade, the early goal-directed therapy principle encompassing early series of protocolized interventions, i.e. antibiotics, fluids, vaso-pressors, inotropes, red blood transfusion, etc., showed significantreduction ofmortality rate.18 This strategyhas beenrecommendedbyspecialtysocietiesintheirguidelines forseveresepsisandsepticshocktreatmentandhasbeen implementedinemergencydepartmentsandintensivecare unitsinaglobalscale.15
Accordingtotheseguidelines,septicpatientspresenting with signs of persistent hypotension (i.e. mean arterial blood pressure <65mmHg despite initial adequate fluid resuscitation) or tissue hypoperfusion (i.e. arterial lac-tate concentration equal to or higher than 4.0mmol/L) haveahigh riskof deathandthereforemust bepromptly resuscitated.15
Nevertheless, there is increasing evidence coming from new randomized clinical trials challenging the efficacy of the early goal-directed therapy for septic patients.8,9 Therefore, we propose a narrative review of the literature supporting the management of the early stages of septic shock, with special attention to hemodynamics evaluation and evidence-based inter-ventions, taking into account the recently published data.
Objective
Our objective was to perform a narrative review of the availableevidenceonhemodynamicsupportforsepticshock patientsandprovideanoverviewofthekeyavailable inter-ventionsforresuscitation,e.g.fluidtherapy,vasopressors, inotropesandredbloodtransfusion.
Methods
We performed a systematic search in MEDLINE/Pubmed, Embase/OVID, LILACS/Bireme andCochrane Library upto October 2014 using the Medical SubjectHeadings (MeSH) terms ‘‘sepsis’’,‘‘severe sepsis’’AND/OR‘‘septicshock’’ combined with ‘‘central venous pressure’’, ‘‘lactate’’, ‘‘lactate clearance’’, ‘‘mean arterial pressure’’, ‘‘blood pressure’’, ‘‘vasopressors’’, ‘‘norepinephrine’’, ‘‘epinephrine’’, ‘‘vasopressin’’, ‘‘central venous oxy-gen saturation’’, ‘‘blood transfusion’’, ‘‘transfusion’’, ‘‘dobutamine’’,‘‘fluidresponsiveness’’.
WehavelimitedoursearchtoarticleswritteninEnglish, human subjects and clinical trials. We also reviewed the currentSurvivingSepsisCampaignGuidelinesforthe Treat-mentofSevereSepsisandSepticShockandtheirkeyrelated articles.15Additionalstudieswereaddedatauthors’ discre-tion.Onehundredandseventy-ninearticleswereretrieved fromthissearchand furtherfilteredfor qualityand origi-nalitybeforebeingincludedinthisreview.
Hemodynamic
goals
The imbalance between oxygen consumption and oxygen delivery is themain determinant ofthe developmentand progressionof organ dysfunctionin septic shock patients. Therefore,theaimofthehemodynamicinterventions com-monly applied to these patients is to increase oxygen deliverytomatchoxygendemand(Fig.1).
Thecurrentlyrecommendedhemodynamictargetstobe achievedduringtheinitialsix-hourofresuscitationinclude a central venous pressure (CVP) between 8 and 12mmHg in spontaneously breathing patients or between 12 and 15mmHginmechanicallyventilatedpatientsorinthosewith reducedventricularcompliance,ameanarterialblood pres-sure (MAP)≥65mmHg,acentral venous(ScvO2)or mixed
venous (SvO2) oxygen saturations ≥70% and 65%
respec-tively, a lactate clearance ≥10% and an urinary output ≥0.5mL/kg/h(Fig.2).15
400
300
200
100
0 200
Critical DO2 (1)
Critical DO2 (2)
O2ER
Healthy
Lactate Critically ill
Oxygen delivery (mL/min)
Oxygen consumption (mL/min)
400 800 1200
Figure1 Relationshipbetweenoxygendelivery,oxygen con-sumption,oxygenextractionrateandlactateinhealthy(1)and criticallyill(2)patientswithshock.DO2,oxygendelivery;VO2, oxygenconsumption;O2ER,oxygenextractionrate.
The first one, the ProCESS trial, assessed three different resuscitationstrategiesforsepticshockpatients.8Thisstudy showed no 60 day mortality difference when usual care (i.e. nopre-specified protocol), protocol-based early goal directtherapy(i.e.centralvenouslineinsertionwithSvcO2 and CVP guidance) and protocol-based standard therapy (i.e.withoutcentralvenouslineplacementnorScvO2and CVP guidance) were compared.8 In the second study, the ARISEtrial,septicshockpatientswererandomizedforearly goal-directed therapy or usual care (at clinical team dis-cretionandwithoutScvO2measurementduringthefirstsix hoursofresuscitation).9Therewasnodifferenceinthe pri-maryoutcome,which wasmortalityonthe90thday after randomization. Additionally, the early goal-directed ther-apygroup receivedsignificantlymorefluids, vasopressors, inotropes andred blood celltransfusion.9 Athird ongoing trial (ProMISe), addressing the efficacy of the early goal directedinsepticshock completedenrollmentofpatients (Controlled-trials.com:ISRCTN36307479).
Considering these results, it can be assumed that earlyrecognition andtreatmentprovisionfor septicshock patients should be the main concern and priority for cliniciansatthebedside ratherthanstrictlyfollowa goal-directedprotocol.Inthenextsections,wewilldiscussthe mainhemodynamicinterventionsindividually.
Centralvenouspressureandfluidresponsiveness
Centralvenouspressureisthepressurerecordedfromthe right atriumor at thesuperiorvena cava bythe insertion
of a central venous catheter.19 The CVP is determined by a complex interaction between cardiac function and venousreturn,andrepresentsastaticindicatorofcardiac preload.19Centralvenouspressureisnotanaccurate predic-toroffluidresponsivenessincriticallyillpatients.20 Never-theless,ithasbeenusedwidelywiththispurpose(Table1).20 Theevaluationofarterialpulsepressurevariationdueto heart---lunginteractionsrepresentsadynamicandaccurate predictorof fluid responsivenessthat can be usedto dis-criminatebetweenpatientswhowillandwillnotincrease cardiacoutputafterafluidchallenge(Table1).21 However, anarteriallineplacement,absenceofpatient’srespiratory efforts,usually obtainedby deepsedationand neuromus-cular blockers, volume controlled mechanical ventilation withtidal volume between 8 and 12mL/kg, positive end expiratory pressure lower than 10cmH2O and a regular
cardiac rhythm are required for pulse pressure variation assessment.21 Other available methods to address fluid responsivenessincriticallyillpatientsincludebedside ultra-soundanalysisoftheinferiorvenacava22andthepassiveleg raisingtest(Table1).23
Thedistensibilityindexoftheinferiorvenacavais cal-culatedfromthe Mmode ofthe thoracic echocardiogram atthesubcostalwindowasfollows:maximuminferiorvena cava diameter minus minimum inferior vena cava diame-terdividedby maximuminferiorvenacava diameter.22 An inferiorvena cava distensibility indexabove 18%is highly correlatedwitha15% cardiac indexincreaseafter afluid challenge.22Inferiorvenacavaanalysisalsorequiresdeeply sedated,mechanicallyventilatedpatients withmild or no respiratoryeffortandaregularcardiacrhythmtobe accu-ratelyperformed.22
Thepassiveleg-raising testisasequential maneuverin whichthepatientisinitiallyinasemi-recumbentposition andafterwardsbothlegsareelevated45degreesinrelation tothegroundwiththepatientinthesupinepositionforone minute.23Thistestsimulatesafluidchallengeinawaythat bloodfromtheinferiorlimbsismobilizedtotheheart.An increasegreaterthan10%inmeasuredbloodflowishighly predictiveoffluidresponsiveness.23 This maneuvercanbe performed inspontaneously breathingpatients andin the presenceofcardiacarrhythmia.23
Arterialbloodpressure
A mean arterial pressure ≥65mmHg has been
recom-mended during the initial resuscitation of septic shock (Fig. 2).15 However, few studies are available to support this recommendation.6,24---28 This lack of available data is
Table1 Mainmethodsavailabletoaddressfluidresponsivenessincriticallyillpatients.
Methods Cutoffvalues Mechanicalventilation? Arrhythmia? Limitations
CVP4,5 <8---12mmHg No/yes Yes Limitedincriticallyillpatients
PP6 >13% Yes No RVdysfunction
IVCdistensibility7 >18% Yes No UStraining
PLR8 CI>10% No Yes N/A
Oxygen ± ETI and MV
Central venous and arterial catheterization
<8
8-12 mmHg*
MAP
LacCI
No Yes
AND/OR Dobutamine Vasoactive agents‡ Consider albumin 4%-5%
Crystalloids (30 mL/kg)
Goals
achieved? Reevaluation periodically
Transfusion RBC until HCT ≥30% ScvO2
mmHg
<65 mmHg
<70% CVP
Access F-R Sedation ± NMB
(if intubated)
∆PP; ECHO/dIVC; PLR; other
≥65 mmHg
≥10% ≥70%
Figure2 Suggestedgoal-directedtherapyalgorithmforsepticshockresuscitation.Itisimportanttonotethatonlyhemodynamic goalsaredepictedinthisalgorithm. Theothercomponentsofsepsisbundles(e.g. antibiotictherapy,sourcecontrol, etc.)are activatedconcomitantly.ETI, endotracheal intubation;MV, mechanicalventilation; NBM, neuromuscularblockers;CVP, central venouspressure;F-R,fluidresponsiveness;MAP,meanarterialbloodpressure;LacCl,bloodlactateclearance;ScvO2,centralvenous oxygensaturation;PP,pulsepressurevariation;ECHO,hemodynamicechocardiography;dIVC,distensibilityindexoftheinferior venacava;PLR,passivelegraising;RBC,packedredbloodcells;HCT,hematocrit;*,forpatientsundermechanicalventilation;⫽,
norepinephrineisthefirstchoicevasopressor(seetext).
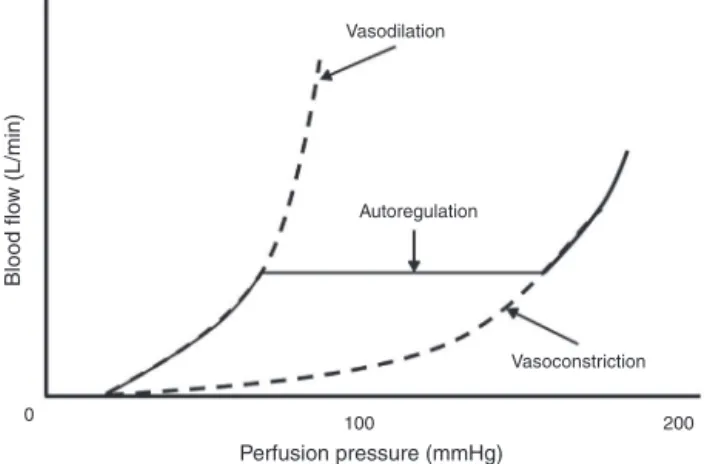
reflectedinthewiderangeofMAPgoals adoptedin stud-iesinvolvingsepticpatients.29Therationalesupportingthe inclusionofarterialbloodpressureinthesepticshock resus-citationalgorithm is basedonthe principle of blood flow autoregulation (Fig. 3). Accordingly, if cardiac output is maintainedconstant,bloodflowtotissuesdoesnotchange untiltheblood pressurefallsbelowacriticalvalue.When thiscriticalvalue isapproached, anyadditionalreduction inarterialpressurewillimpairtissuebloodflow.Since dif-ferentorganshavedistinctcriticalthresholds,theoptimal arterial blood pressure to be achieved remains undeter-mined.
Smallprospectivestudiesaddressedtheeffectsof differ-entMAPlevelsinsepticshockpatients.IncreasingMAPfrom 65to85mmHgdidnotimprovesystemicoxygen consump-tion,skinmicrocirculatorybloodflow,splanchnicperfusion
or renal function, and was associated with a higher left ventricular stroke work index and increased exposure to catecholamines.24,25 Additionally, although increasing MAP from 60 to 90 mmHg26 or from 65 to 85mmHg27,28 with norepinephrineimprovedsystemicoxygendeliveryandthe cutaneoustissuepartial pressureofoxygen, contradictory findingsonsublingualmicrocirculationwerereported.26---28
0 100 200 Vasoconstriction Autoregulation
Vasodilation
Perfusion pressure (mmHg)
Blood flo
w (L/min)
Figure3 Autoregulationofbloodflowtothetissuesdrivenby theperfusionpressurecurve.Insituationsofseverehypotension (meanarterialpressure<50mmHg),bloodflowtothetissuesis decreased,leadingtohypoxia.Ontheotherhand,duringsevere hypertension(meanarterialpressure>150mmHg),thereisan increaseinbloodflowtothetissuesthatcanresultinleakageof bloodcomponentsintotheinterstitialspace.Inbothsituations, whentheautoregulatorythresholdisreached,autoregulation ofthebloodflowmechanismislost.Themeanarterialpressure representstheperfusionpressure.
tofluids,vasopressorsandinotropes,whichhasbeen asso-ciatedwithincreasedincidenceof sideeffects,morbidity and mortality.30 Nevertheless, targeting lower MAP levels mayincreasetheincidenceoftissuehypoperfusionand con-tributetotheprogressionoforgandysfunction.31,32
Mixedvenousandcentralvenousoxygensaturation
In conditions under reduced oxygen delivery, the oxy-gen consumption can be satisfied if the tissue oxygen extraction increasesproportionally.Ifthe oxygendelivery reduction persists, anaerobic metabolism, lactic acidosis and organdysfunction may develop (Fig. 1).33 The mixed venous oxygen saturation is measured in the blood col-lected througha pulmonary artery catheterand itsvalue providesinformationregardingtothesystemicoxygen con-sumption.
Themixedvenousoxygensaturationvaluesarenotequal tothecentralvenous oxygensaturation,whichrepresents theoxygensaturationmeasuredinthebloodcollectedfrom thesuperiorvenacavaattheentrancetotherightatrium.34 Although the differences between ScvO2and SvO2 values can vary across different clinical conditions, the overall trendsofbothmeasurementsaresimilar.35
Assumingarterialoxygensaturationof100%,theoxygen extractionrate(O2ER)canbesummarizedby‘‘1---SvO2’’, inasimplerwaythanusingoxygenconsumptionanddelivery calculationstoguidetherapyatthebedside.33Nevertheless, itisimportanttoempathizethattheoxygenextractionrate needs tobeanalyzed as afunction of the cardiac output andinassociationwithotherperfusionparameters.33Alow mixedvenousoxygensaturationcanbeadequatein compen-satedchronicheartfailurepatientsorinpatientsrecovering fromshock(flowredistribution),andmaybehighand ade-quateinsomechronic cirrhoticpatients.Becauseof that,
therecommendationstoreachScO2≥65%oraScvO2≥70%
representasimplification,onlyvalidduringthefirst6hof septicshock(Fig.2).15
Lactateclearance
The lactate is an intermediate compound of the glucose metabolism, produced in the cytoplasm from pyruvate. In aerobic conditions, the pyruvate is produced via gly-colysis and is metabolized by the mitochondrial aerobic oxidationpathwayvia theKrebs cycle,bypassing the pro-ductionoflactate.Inanaerobicconditions,thedecreased mitochondrialoxidativephosphorylationresultsinaraised pool of pyruvate. This excess of pyruvate is converted intolactate.Lactateproductionoccursinmultipleorgans, such as muscle, skin, brain, intestine and red blood cells and its clearance takes ground in the liver, kid-neys and heart. Thus, an impaired lactate clearance or excessivelactateproduction can resultin high blood lac-tate levels. The normal arterial lactate level is below 2.0mmol/L.36
Inmostshockstates,particularlythosepresenting with lowcardiacoutput,hyperlactatemiareflectsend-organ cel-lular dysoxia due to tissue hypoperfusion. Indeed, even afternormalizingthetraditionalhemodynamicparameters, such as CVP, MAP, cardiac output and SvO2, critically ill patientsmaystillhave ongoing tissuehypoxia (i.e.occult hypoperfusion).37Therefore,lactatehasbeenusedasa sur-rogatemarkeroftissuehypoperfusionandasabiomarkerfor morbidityandmortalityinsepticshockpatients.Both inter-mediate(2.0---3.9mmol/L) and high (≥4.0mmol/L) serum
lactatelevelshavebeen associatedwithincreasedrisk of death.37
The lactate clearanceis defined as the percentage of lactateclearedoveraperiod,usually2---6h,from presenta-tionintheemergencydepartmentorintensivecareunit.38 Foreach10%increaseinlactateclearance,thereisan11% decreaseinthe likelihoodof death.38 Alactate clearance lowerthan 10% fromitsbaseline valueis an independent predictorofincreasedin-hospitalmortality.38Ina multicen-ter,open-label,randomizedcontrolledtrial,Jansenetal. enrolledpatientsadmittedtotheintensivecare unitwith lactate≥3.0mEq/L.39 In onegroup,the resuscitation was
guided by the clearance of lactate (decrease of 20% or moreper2hfortheinitial8h inintensivecareunit).The controlgrouphad onlythe initial lactatemeasureand no lactateguided therapy.The patientsinthelactate-guided treatment group had loweradjusted in-hospitalmortality (hazardratio0.61,95%CI0.43---0.87;p=0.006)and inten-sivecareunitmortality(hazardratio0.66,95%CI0.45---0.98; p=0.037).39
Therapy
Fluids
The correction of hypovolemia and tissue hypoperfusion throughfluidadministrationaimstoincreasetissueoxygen deliverybyincreasingcardiacoutput.Currently,thefluidof choicefor theinitialresuscitationofsepticshockpatients is crystalloids, at an initial fluidchallenge of 30mL/kg.15 Basedondatafromrecentlypublishedtrials,hydroxyethyl starch(HES)shouldnotbeusedforfluidresuscitation.
Severalstudiesandmeta-analyseshaveshownthe dele-teriouseffects of HES compared tocrystalloids for septic shockresuscitation.41---45 Hydroxyethylstarchincreasesthe riskofbleeding,acuterenalfailureandtheneedforrenal replacementtherapy.44,45
TheVISEPtrialassessedthesafetyandefficacyof inten-siveinsulin therapy against conventional therapy and10% HES200/0.5againstRinger’slactateinpatientswithsevere sepsisorsepticshock.41Thisstudywasstoppedprematurely duetothehighriskofhypoglycemiaintheintensiveinsulin therapygroup. The comparisonbetween HES 200/0.5and Ringer’slactatecontinued withall patientsreceiving con-ventionalinsulin therapy. The trial wasstopped afterthe firstinterimanalysis,becauseofincreasedrateofrenal fail-ureandatrendtowardhighermortalityat90daysintheHES group.41
The6Strialenrolledseveresepsispatientstofluid resus-citationwitheither6%HES130/0.42orRinger’sacetate.42 Inthisstudy,HES 130/0.42significantly increasedtherisk ofdeath(51%vs.43%; p=0.03)ordependence ondialysis at90days(22%vs.16%;p=0.04).TheCHESTtrialrandomly assigned7000criticallyillpatientstoreceive6%HES130/0.4 in0.9%salineor0.9%salinealoneforfluidresuscitation.43 There was no significant difference in 90 day mortality betweenthetwogroups.Nevertheless,morepatientswho receivedHES130/0.4neededrenalreplacementtherapy.43 TheCRISTALtrialcomparedcolloids(gelatins,dextrans,HES oralbumin4%or 20%)vs.crystalloids(isotonic/hypertonic salineorRingerlactate)inhypovolemicshockresuscitation (includingsepsis, traumaandno-traumano-sepsis). There wasnodifferencebetweengroupsin28daymortality (rel-ativerisk0.96,95%CI0.88---1.04;p=0.26).46
Administration of albumin should be considered in patientsrequiringsubstantialamountsofcrystalloids.15The largest trial to date that compared hypooncotic albumin (4% solution)with normal saline in a general critically ill populationwasthe SAFEtrial.47 Thisstudy showedno dif-ference28 daymortalitybetween thegroups. Asubgroup analysisincludingonlyseveresepsispatientsdemonstrated thatalbuminadministrationwasindependentlyassociated withmortalityreduction(oddsratio0.71,95%CI:0.52---0.97; p=0.03).48 Nevertheless,thisfindingwasnotconfirmedin themost recenttrialinwhich1818severesepsisand sep-ticshock patients wererandomizedtoreceive either 20% albuminandcrystalloidsolutionorcrystalloidsolutionalone duringICUstay.7
Vasopressors
Systemicvasodilatationandarterialhypotensionare land-marks of severe sepsis and septic shock. When adequate
fluidresuscitationisnotenoughtorestorethearterialblood pressure, vasopressor administration should be initiated (Fig.2).15Ameta-analysisincludingsixrandomizedclinical with1408patientscomparednorepinephrinevs.dopamine asfirst-linevasopressorsinsepticshock.49Dopamine admin-istrationwasassociatedwithahigherriskofdeath(relative risk1.12,95% CI1.01---1.20; p=0.035)anda higherrisk of cardiac arrhythmias(relative risk 2.34,95% CI 1.46---3.77; p=0.001).Basedonthesefindings,norepinephrinehasbeen recommendedasthevasopressorof choiceinsepticshock patients (Fig. 2).15 Alternative vasopressors include low dosesofvasopressin,epinephrine(addedorpotentially sub-stitutedfornorepinephrine)anddopamineinhighlyselected patients(low-riskforarrhythmia).15
Vasopressin,alsoknownasantidiuretichormone,is syn-thesized in the paraventricular and supraoptic nuclei of the hypothalamus and released into the systemic circu-lation from the posterior pituitary gland in response to decreasedintravascularvolumeandincreasedplasma osmo-lality.Thevasoconstrictiveeffectofvasopressinonvascular smooth muscle is mediated by V1 receptors. It is one of the most important stress-related hormones and a rela-tivevasopressindeficiencymaydevelopduringsepticshock progression.50
Lowdosesofvasopressinmaybeaddedtonorepinephrine tomaintainarterialbloodpressureinrefractorysepticshock and todecreaseexposure tonorepinephrine.15 The VASST trial compared the administration of low doses of vaso-pressin(0.01---0.03U/min)vs.norepinephrineinsepticshock patients.51 The authorsreportednosignificant differences betweenthetworespectivegroupsregarding28day mortal-ity(35.4%vs.39.3%;p=0.26),90 daymortality(43.9%vs. 49.6%;p=0.11)ortherateofseriousadverseevents.51The main concern about vasopressin administrationis related todecreasedbloodflow totheheart,intestineandlimbs, especiallywhenhigherdosesareused.50
Epinephrine is a potent ␣- and -adrenergic cate-cholamine that increases MAP by increasing both cardiac output and systemic vascular resistance. Epinephrine administration may also transiently increase the lactate concentration,probablyduetoincreasedaerobicglycolysis throughNa+K+ATPasestimulationwithintheskeletal
mus-clesratherthanthroughtissuedysoxia.52Epinephrinealone was compared to norepinephrine associated with dobut-amine administration in a prospective multicenter study, which included 330 septic shock patients.52 The 28 and 90daymortalityrates,timetohemodynamicstabilization, numberofvasopressor-freedaysandrateofseriousadverse effects did not differ between the study groups. Never-theless, a transient increase in the lactate concentration was observed between days 1 and 4 in the epinephrine group.52
Inotropesandbloodtransfusion
Finally, the Surviving Sepsis Campaign Guidelines rec-ommend red blood cell transfusion aiming to reach an hematocrit of at least 30% (Fig.2).15 Nevertheless, there is no strong evidence that higher hemoglobin targets (>9.0g/dL)arebeneficialintheabsenceofcoronaryheart disease or stroke, and several concerns exist regarding higher oxygen affinity of stored hemoglobin.53,54 The recentlypublishedTRISStrialwasarandomizedcontrolled studythatcomparedtwodifferenthemoglobintransfusion thresholds(≤7.0g/dLand≤9.0g/dL)inalmostathousand
septicshockpatients.10Theauthorsreportednosignificant 90daymortalitydifferencebetweenthegroups(relativerisk 0.94,95%CI0.78---1.09,p=0.44),althoughthelower thresh-oldgroupreceivedhalfofaredbloodcelltransfusionwhen comparedtothehigherthreshold.Additionally,therewas nodifferencein theincidenceof cardiacand non-cardiac ischemicevents.10
Conclusion
Prompt andaggressive treatment of septicshock patients improves morbidity and mortality. Early recognition in additiontofluidresuscitationandproperantibiotics admin-istrationtopatientsarethecornerstoneofthetreatment. Alongwithit,acomprehensiveclinicalbedside evaluation and an accurateassessment of fluid responsiveness seem tobethebestavailableevidence-basedmedicinefor sep-tic shock resuscitation. In the light of the new findings presentedinrecentlypublishedtrials,areviewofthe goal-directedtherapy,asitwasconceived,isnecessary.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
WethankHelenaSpalicforproof-readingthismanuscript.
References
1.AngusDC,Linde-Zwirble WT,LidickerJ, et al.Epidemiology of severe sepsis in the United States: analysis of inci-dence,outcome,andassociatedcostsofcare.CritCareMed. 2001;29:1303---10.
2.GaieskiDF,EdwardsJM,KallanMJ,etal.Benchmarkingthe inci-denceandmortalityofseveresepsisintheUnitedStates.Crit CareMed.2013;41:1167---74.
3.JawadI,LuksicI,RafnssonSB.Assessingavailableinformation ontheburdenofsepsis:globalestimatesofincidence, preva-lenceandmortality.JGlobalHealth.2012;2:010404.
4.MayrFB, Yende S,Angus DC.Epidemiology of severesepsis. Virulence.2014;5:4---11.
5.KaukonenKM, BaileyM,Suzuki S,etal. Mortalityrelatedto severe sepsis and septic shock among critically ill patients inAustralia and New Zealand,2000---2012. JAm MedAssoc. 2014;311:1308---16.
6.Asfar P, Meziani F,Hamel JF, et al. High versus low blood-pressuretargetin patientswithsepticshock. NEnglJ Med. 2014;370:1583---93.
7.Caironi P,Tognoni G, Masson S, et al. Albuminreplacement inpatientswithseveresepsisorsepticshock.NEnglJMed. 2014;370:1412---21.
8.Yealy DM, Kellum JA, Huang DT, et al. A randomized trial ofprotocol-basedcare for earlysepticshock. NEngl JMed. 2014;370:1683---93.
9.Peake SL, Delaney A, Bailey M, et al. Goal-directed resus-citation for patientswithearly septic shock. NEngl JMed. 2014;371:1496---506.
10.Holst LB, HaaseN, WetterslevJ, et al.Lower versus higher hemoglobinthresholdfortransfusioninsepticshock.NEnglJ Med.2014;371:1381---91.
11.SilvaE,PedroMA,SogayarAC,etal.Braziliansepsis epidemio-logicalstudy(BASESstudy).CritCare.2004;8:R251---60. 12.ZhangK,MaoX,FangQ,etal.Impairedlong-termqualityoflife
insurvivorsofseveresepsis:Chinesemulticenterstudyover6 years.Anaesthesist.2013;62:995---1002.
13.CuthbertsonBH,EldersA,HallS,etal.Mortalityandqualityof lifeinthefiveyearsafterseveresepsis.CritCare.2013;17:R70. 14.Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairmentandfunctionaldisabilityamongsurvivorsofsevere sepsis.JAmMedAssoc.2010;304:1787---94.
15.DellingerRP,LevyMM,RhodesA,etal.Survivingsepsis cam-paign:internationalguidelinesformanagementofseveresepsis andsepticshock:2012.CritCareMed.2013;41:580---637. 16.Hayes MA,Timmins AC,YauEH,etal. Elevationofsystemic
oxygendeliveryinthetreatmentofcriticallyillpatients.NEngl JMed.1994;330:1717---22.
17.GattinoniL, BrazziL, PelosiP,etal.Atrialofgoal-oriented hemodynamictherapy incriticallyill patients.SvO2 Collabo-rativeGroup.NEnglJMed.1995;333:1025---32.
18.RiversE,NguyenB,HavstadS,etal.Earlygoal-directedtherapy inthetreatmentofseveresepsisandsepticshock.NEnglJMed. 2001;345:1368---77.
19.MagderS.Centralvenouspressuremonitoring.CurrOpinCrit Care.2006;12:219---27.
20.MarikPE,BaramM,VahidB.Doescentralvenouspressure pre-dictfluidresponsiveness?Asystematicreviewoftheliterature andthetaleofsevenmares.Chest.2008;134:172---8.
21.MichardF.Changesinarterialpressureduringmechanical ven-tilation.Anesthesiology.2005;103:419---28.
22.BarbierC, LoubieresY,Schmit C,et al. Respiratorychanges ininferiorvenacava diameterarehelpfulinpredictingfluid responsiveness in ventilated septic patients. Intensive Care Med.2004;30:1740---6.
23.MonnetX,RienzoM,OsmanD,etal.Passivelegraising pre-dictsfluidresponsiveness inthecritically ill.CritCareMed. 2006;34:1402---7.
24.LeDoux D,Astiz ME, Carpati CM, et al. Effects of perfusion pressure on tissueperfusion in septicshock. Crit CareMed. 2000;28:2729---32.
25.BourgoinA,LeoneM,DelmasA,etal. Increasingmean arte-rialpressureinpatientswithsepticshock:effectsonoxygen variablesandrenalfunction.CritCareMed.2005;33:780---6. 26. JhanjiS,StirlingS,PatelN,etal.Theeffectofincreasingdoses
ofnorepinephrineontissueoxygenationandmicrovascularflow inpatientswithsepticshock.CritCareMed.2009;37:1961---6. 27.DubinA,PozoMO,CasabellaCA,etal.Increasingarterialblood
pressurewithnorepinephrinedoesnotimprove microcircula-torybloodflow:aprospectivestudy.CritCare.2009;13:R92. 28.Thooft A,Favory R, SalgadoDR,etal. Effectsofchangesin
arterialpressureonorganperfusionduringsepticshock.Crit Care.2011;15:R222.
29.SevranskyJE,NourS,SuslaGM,etal.Hemodynamicgoalsin randomizedclinicaltrialsinpatientswithsepsis:asystematic reviewoftheliterature.CritCare.2007;11:R67.
mortality:aposthocanalysisofamulticentertrial.CritCare. 2009;13:R181.
31.CorreaTD,VudaM,TakalaJ,etal. Increasingmeanarterial bloodpressureinsepsis:effectsonfluidbalance,vasopressor loadandrenalfunction.CritCare.2013;17:R21.
32.BadinJ,BoulainT,EhrmannS,etal.Relationbetweenmean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study. Crit Care. 2011;15:R135.
33.VincentJL.Determinationofoxygendeliveryandconsumption versuscardiacindexandoxygenextractionratio.CritCareClin. 1996;12:995---1006.
34.Chawla LS, Zia H, Gutierrez G, et al. Lack of equivalence betweencentraland mixedvenousoxygensaturation.Chest. 2004;126:1891---6.
35.ReinhartK,KuhnHJ,HartogC,etal.Continuouscentralvenous andpulmonaryarteryoxygensaturationmonitoringinthe crit-icallyill.IntensiveCareMed.2004;30:1572---8.
36.Valenza F,Aletti G, FossaliT, et al. Lactateas a markerof energyfailure incriticallyillpatients:hypothesis.CritCare. 2005;9:588---93.
37.MikkelsenME,MiltiadesAN,GaieskiDF,etal.Serumlactateis associatedwithmortalityinseveresepsisindependentoforgan failureandshock.CritCareMed.2009;37:1670---7.
38.NguyenHB,RiversEP,KnoblichBP,etal.Earlylactateclearance isassociatedwithimprovedoutcomeinseveresepsisandseptic shock.CritCareMed.2004;32:1637---42.
39.Jansen TC, van BJ, Schoonderbeek FJ, et al. Early lactate-guidedtherapyinintensivecareunitpatients:amulticenter, open-label,randomizedcontrolledtrial.AmJRespirCritCare Med.2010;182:752---61.
40.JonesAE,ShapiroNI, TrzeciakS,etal. Lactateclearance vs centralvenousoxygensaturationasgoalsofearlysepsis ther-apy: a randomizedclinicaltrial.JAm MedAssoc. 2010;303: 739---46.
41.BrunkhorstFM,EngelC,BloosF,etal.Intensiveinsulintherapy andpentastarchresuscitationinseveresepsis.NEngl JMed. 2008;358:125---39.
42.PernerA,HaaseN,GuttormsenAB,etal.Hydroxyethylstarch 130/0.42versusRinger’sacetateinseveresepsis.NEnglJMed. 2012;367:124---34.
43.MyburghJA,FinferS,BellomoR,etal.Hydroxyethylstarchor salineforfluidresuscitationinintensivecare.NEnglJMed. 2012;367:1901---11.
44.Haase N, Perner A, Hennings LI, et al. Hydroxyethyl starch 130/0.38---0.45versuscrystalloid oralbumin inpatientswith sepsis:systematicreviewwithmeta-analysisandtrial sequen-tialanalysis.BrMedJ.2013;346:f839.
45.ZarychanskiR,Abou-SettaAM,Turgeon AF,et al.Association ofhydroxyethylstarchadministrationwithmortalityandacute kidneyinjuryincriticallyillpatientsrequiringvolume resusci-tation:asystematicreviewandmeta-analysis.JAmMedAssoc. 2013;309:678---88.
46.AnnaneD,SiamiS,JaberS,etal.Effectsoffluidresuscitation withcolloidsvscrystalloidsonmortalityincriticallyillpatients presenting withhypovolemicshock: theCRISTAL randomized trial.JAmMedAssoc.2013;310:1809---17.
47.FinferS,BellomoR,BoyceN,etal.Acomparisonofalbumin andsalinefor fluidresuscitationintheintensivecareunit.N EnglJMed.2004;350:2247---56.
48.FinferS,McEvoyS,BellomoR,etal.Impactofalbumin com-paredtosalineonorganfunctionandmortalityofpatientswith severesepsis.IntensiveCareMed.2011;37:86---96.
49.DeBackerD,AldecoaC,NjimiH,etal.Dopamineversus nor-epinephrineinthetreatmentofsepticshock:ameta-analysis. CritCareMed.2012;40:725---30.
50.RussellJA.Bench-to-bedsidereview:vasopressininthe man-agementofsepticshock.CritCare.2011;15:226.
51.RussellJA,WalleyKR,SingerJ,etal.Vasopressinversus norepi-nephrineinfusioninpatientswithsepticshock.NEnglJMed. 2008;358:877---87.
52.Annane D, Vignon P, Renault A, et al. Norepinephrine plus dobutamineversusepinephrinealoneformanagementofseptic shock:arandomisedtrial.Lancet.2007;370:676---84.
53.HebertPC,WellsG,BlajchmanMA,etal.Amulticenter, ran-domized,controlledclinicaltrialoftransfusionrequirementsin criticalcare.TransfusionRequirementsinCriticalCare Inves-tigators, Canadian Critical CareTrials Group. NEngl J Med. 1999;340:409---17.