w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
CT
enterography
in
the
evaluation
of
Crohn’s
disease
Carlos
Henrique
Marques
dos
Santos
a,∗,
Jovino
Nogueira
da
Silva
Menezes
b,
Thiago
Franchi
Nunes
c,
Letícia
de
Assis
Martins
caServiceofColoproctology,HospitalUniversitárioMariaAparecidaPedrossian,CampoGrande,MS,Brazil bServiceofGeneralSurgery,HospitalUniversitárioMariaAparecidaPedrossian,CampoGrande,MS,Brazil cServiceofRadiology,HospitalUniversitárioMariaAparecidaPedrossian,CampoGrande,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28March2015
Accepted8June2015
Availableonline2October2015
Keywords:
Crohn’sdisease
Enterography Diagnosis
a
b
s
t
r
a
c
t
Proposition:Crohn’sdisease(CD)isachronicinflammatoryprocessthataffectsvariousparts
ofthegastrointestinaltract,fromthemouthtotheanuswithunknownetiologyandvariable
clinicalpresentation.CDdiagnosisisbasedonclinicalandcomplementarytests.Among
thecomplementarytests,enterographywithCTenterographyhasshowngoodresultsin
theevaluationofthisdisease.
Methods:Thepatientsevaluatedweresubmittedtoaquestionnaireontheclinical
manifes-tationsofthediseaseandanCTenterographywasobtained.Thestudieswerereviewedby
anexperiencedradiologistlookingforradiologicalsignsofCD.
Results:Themeanagewas40years,withapredominanceofwomen.Themainclinical
manifestationsarediarrheain24(70%),hematocheziain19(55%),abdominalpainin29
(85%)andweightlossin22(64%)patients.ThemainfindingsonCTenterographywerean
intestinalwallenhancementsignalin23patients(67%),vascularengorgement(vasarecta)
in20(58%),parenteralfatdensificationin14(41%),intestinalwallthickeningin22(64%),
andlymphnodeenlargementin17(50%)ofpatients.
Conclusion: ThisstudyshowedthatCTenterographypresentsagoodassessmentof
intesti-nalinvolvementbyCD.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All
rightsreserved.
Enterografia
por
tomografia
computadorizada
na
avaliac¸ão
da
doenc¸a
de
Crohn
Palavras-chave:
Doenc¸adeCrohn
Enterografia Diagnóstico
r
e
s
u
m
o
Proposic¸ão:Adoenc¸adeCrohn(DC)éumprocessoinflamatóriocrônicoqueacometevários
locaisdotratogastrointestinal,desdeabocaatéoânus,tendoetiologiadesconhecidae
apresentac¸ão clinica variável.Seu diagnósticobaseia- seno exameclinicoe em testes
∗ Correspondingauthor.
E-mail:[email protected](C.H.M.dosSantos).
http://dx.doi.org/10.1016/j.jcol.2015.06.006
complementares.Dentreosexamescomplementares,aEnterografiaporTomografia
Com-putadorizada(Entero-TC)temmostradobonsresultadosnaavaliac¸ãodessadoenc¸a.
Metodologia: Os pacientes avaliados foram submetidos a um questionário sobre as
manifestac¸õesclinicasdadoenc¸aerealizaramEntero-TC.Essesexamesforamanalisados
porumradiologistaexperiente,àprocuradesinaisradiológicosdaDC.
Resultados: Aidade médiafoi de40 anos,compredomíniode mulheres.Asprincipais
manifestac¸õesclínicasforamdiarreiaem24(70%),hematoqueziaem19(55%),dor
abdom-inalem 29(85%)eperdadepesoem22(64%)dospacientes.Osprincipaisachadosna
Entero-TCforamosinalderealcedeparedeintestinalem23pacientes(67%),ingurgitamento
vascular(vasarecta)em20(58%),densificac¸ãodegorduraperientéricaem14(41%),
espes-samentodeparedeintestinalem22(64%)elinfonodomegaliaem17(50%)dospacientes
avaliados.
Conclusão: OpresenteestudomostrouqueaEntero-TCapresentaboaavaliac¸ãodo
acome-timentointestinalpelaDC.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.
Todososdireitosreservados.
Introduction
Crohn’sdisease(CD)isachronicinflammatoryprocessthat
affects variousparts ofthe gastrointestinal tract,from the
mouthtotheanus.1,2CDhasshownanincreaseinits
preva-lence since the second half ofthe twentieth century and,
despitemajoradvancesinunderstandingthebasic
mecha-nismsofinflammationandpathogenesis,itscauseremains
unknown.1
With an extremely variable clinical presentation, CD
exhibitssymptomsandprevalentinjuriesthatdifferaccording
totheirlocation,extent,systemicmanifestationsand
poten-tialcomplications.Ingeneral,CDexhibitsasearlysymptoms:
abdominalpain,associatedwithpersistentdiarrhea,weight
loss,mildfeverandextra-intestinalmanifestations.2
The diagnosis of CD is based on the analysis of
clini-caldata,ashistoryandacompletephysicalandproctologic
examination,besidesendoscopic,radiological,laboratoryand
histologicaltests.3Undoubtedly, colonoscopyhasprovento
bethetestofchoiceforthediagnosisofthisdisease,since
itallowsacompleteevaluationofthelargebowel,ileocecal
valveandterminalileum,areascommonlyaffectedbythe
dis-ease.However,initsmostpart,thesmallintestinecannotbe
evaluatedbythismethod.
Forseveralyears,bariumstudieswereconsideredasthe
goldstandard in theinvestigation ofdiseases ofthe small
intestine,forexample,conventionalenteroclysisand
intesti-naltransit,3 withgreatimpactonthediagnosis,evaluation
oftheir anatomicaldistribution, the presenceof
complica-tionssuchasstencils,fistulae,abscesses,andsignsofacute
exacerbation.4
Withthedevelopmentofimagingstudies,the
enterogra-phy,eitherbycomputedtomographyormagneticresonance
imaging,isreplacing theintestinaltransitand enteroclysis
proceduresintheimagingevaluationofthesmallintestine.
TheadvantageofCTenterographyistoallowavisualization
oftheentiresmallintestine,withoutoverlappingloops,thus
allowing the evaluationofthe intestinal wall, detection of
extra-luminalpathological conditions,andpotential
associ-atedchanges.
Many ofthesefindingsare notseen intraditional
endo-scopicstudies,whichfavorstheprogressivereplacementof
oldmethodsbytheenterographyasthemainmethodof
diag-nosisofinflammatoryboweldisease(IBD).5–8
The early studies with CT enterography showed a high
degreeofsensitivity,above 85%,forthe diagnosis ofactive
CD,whencomparedwithbariumenteroclysis.Recentstudies
havedemonstratedasensitivityrateofupto100%and
speci-ficityof53.9%fortheidentificationofCDinitsactivephase.7
OtherpapershaveshownthatCTenterographyisequivalent
toMRenterographyfortheassessmentofCDactivity.
DespitestudiesshowinggoodresultswithCT
enterogra-phy,therearefewpublicationsonthissubjectinBrazil;thus,
itisessentialtocarryoutthisstudyinourmidst.
Goal
Theaimofthisstudywastoanalyzetheradiologicalfindings
ofCTenterography,relatingthemtotheclinical
manifesta-tionsinpatientswithCD.
Method
The study was approved by the Ethics Committee of the
Federal University of Mato Grosso do Sul. After reading
and signingan informedconsentform, patientsdiagnosed
withCrohn’sdiseasereferredfromColoproctologyOutpatient
ClinicsofHospitalUniversitárioMariaAparecidaPedrossian
and Hospital Regional de Mato Grosso do Sul were
stud-ied.
Patients diagnosed with Crohn’s disease, aged over 18
years,andalreadyevaluatedbycolonoscopywereincluded.
Patients with a known gastrointestinal tract neoplasia,
patientswithgastrointestinalsymptomssuchasnauseaand
vomiting, pregnant women, and patients with allergy to
iodinated contrast or with creatinine above 2.0mg/dl were
excludedfromthisstudy.
All participantsrespondedtoaquestionnaire(Fig.1)on
Crohn’sdisease aboutsymptomsand signs atpresentation
Fig.1–Enterographybycomputedtomographyof abdomen(sagittalsection)showingluminaldilation,wall thickeningandcontrasthyper-uptake.
Regardingthemedication used,thesedrugswere
classi-fiedasimmunosuppressants(azathioprine),salicylates(oral
mesalazine), topical salicylates (mesalazine enemas and
suppositories),corticosteroids(prednisoneandbudesonide),
biologicals (infliximab and adalimumab) and antibiotics
(metronidazoleandciprofloxacin).
An oral neutral contrast, polyethylene glycol solution
(Muvinlax®),commerciallyavailableassachetswith13.125g,
wasusedasperprotocolintheprocedures.Thisproductwas
dilutedasfollows:fivesachets(65.625g)in1500mLofwater
(43.75g/L), administered during 40min. Then, the
partici-pantsunderwentcomputedtomography(CT)oftheabdomen
andpelvis.AnAquilon-64tomographwith64rowsof
detec-tors(ToshibaMedicalSystems,Tokyo,Japan)wasused.The
examinationswereperformedwithmultislicetechniqueand
volumetricacquisition,extendingfromthediaphragmtothe
pubic symphysis, 65s after starting the intravenous
injec-tionofcontrastmedium.Thecontrastwasinjectedatarate
ofapproximately 3mL/sin aproportion of1.5mL/kg, with
a maximum volume of 150mL. The technical parameters
usedinCTscanswereasfollows:collimation64×0.625mm,
pitch=0.891,3-mmthick,120kVp,andmAs=1mm.Coronal
andsagittalreconstructionswereobtained.
Thescans were interpreted bya single radiologist with
extensiveexperience in CT enterography;this professional
wasblindedtoclinical informationathisworkstation.The
evaluatorconductedananalysisastothedegreeof
intesti-naldistension, divided into four areas ofbowel segments:
lefthypocondrium,mesogastrium,pelvisandterminalileum.
Eachregionwasratedaccordingtoascalefrom1to3,as
fol-lows:1–loops<1cmdiameter;2–loopswith1–2cmdiameter;
3–loops>2cmdiameter.Furthermore,theradiologist
classi-fiedtheloopwallsasvisibleornon-visible,alsointhefour
areasconsidered.
Thefollowingfindingsindicativeofdiseaseactivitywere
observed withCT enterography: wallthickening,increased
intestinal wall enhancement, parietal stratification,
par-enteral fat densification,vascular engorgement(vasa recta),
lymphadenomegaly,fistulaeorabscesses.
Data were analyzedusingthe ExcelWindows® program
2007.ThefindingsofCTenterographywere thencorrelated
withtheclinicalfindingsobtainedthroughthequestionnaire
onthedisease.
All informationon the identityofthe research subjects
and onquestionnairescomplied withtheethicalprinciples
ofresearchsetoutintheNationalHealthCouncilResolution
466/12.
Results
Agoodtoleranceofallpatientswithoralcontrastintakewas
noted,andalltestshavebeencompleted,totaling34studies.
Agesrangedfrom18to67years(mean,40years).Ofour34
patients,20(58%)werefemaleand14(42%)weremale.Asfor
raceorcolor,18(52%)reportedCaucasianascend,four(11%)
Black,11(32%)Brown(2%)and1Yellowpatient(Fig.2).
Themainclinicalmanifestationswerediarrheain24(70%),
hematocheziain19 (55%),abdominalpainin29(85%), and
weightlossin22(64%)patients(Fig.3).
Twenty-fivepatients(73.5%)wereunderpharmacological
treatment.Themajordrugsusedwereazathioprine(52%),oral
mesalamine(44%)andprednisone(44%),someoftheseused
incombination(Table1).Ninepatients(36%)wereusingonly
onedrug,especiallysalicylate(44%),while13(38%)wereusing
morethanonedrug(Table2).
ThemainfindingsofCTenterographywereintestinalwall
signalenhancementin23patients(67%),vascular
engorge-ment(vasarecta)in20(58%),perienteralfatdensificationin
14(41%),andbowelwallthickeningin22(64%)(Table3and
Figs.1and4).Lymphadenomegalywasobservedin17(50%)
patients.Abscesseswerealsoseeninfour(11%)patients,with
locationontheleftischioanalfossa,atthecolostomysite,right
Caucasian
Race or Color
Black
Brown
Yellow
Clinical manifestations
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Diarrhea
HematocheziaAbdominal painWeight lossAnal fistula Fever
ConstipationArthropathy
Recurrent UTILaxative use Abdominal mass
Oral lesion
Fig.3–Signsandsymptomspresentedbyourpatientsaccordingtothequestionnaireapplied.Note:somepatients
presentedmorethanoneclinicalmanifestation.
Table1–Medicationincurrentuse.
Drug n %
Azathioprine 13 52
Mesalazinetablet 11 44
Mesalaminesuppository 2 8
Mesalazineenema 3 12
Prednisone 11 44
Adalimumab 4 16
Infliximab 4 16
Ciprofloxacin 2 8
Metronidazole 2 8
Note:somepatientsusedmorethanonemedication.
Table2–Distributionofpatientsbydrugsusedina monotherapyregimen.
Therapy n %
Immunosuppressive 2 22
Salicylate,topical 0 0
Salicylate,oral 4 44
Corticoids 2 22
Biologicals 1 11
Antibiotics 0 0
Total 9 100
Table3–RadiologicalfindingsofCTenterography.
Radiologicalsigns n %
Intestinalwallenhancement 23 67
Intestinalwallthickening 22 64
Vascularengorgement(vasarecta) 20 58
Reactivelymphnodes 17 50
Mesentericfatdensification 14 41
Stenosis 12 35
Targetordoublehalosignal 9 26
Fistulae 5 14
Abscesses 4 11
Note:somestudiespresentedmorethanonefinding.
iliacfossaandinaleftextraperitonealarea.Themostaffected bowelsegmentswereileumandrightcolon(Table4andFig.5).
Thecombinationofperianallesionsinassociationwith
uri-narytractinfectionwaspresentin10(29%)patients;two(5.8%)
weremenandeight(23%)werewomen.Diarrheaandweight
losswereobservedin19(55%)patients.
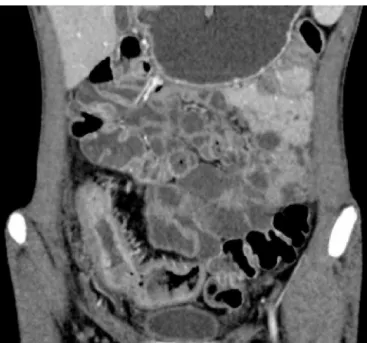
Fig.4–Enterographybycomputedtomographyofabdomen (coronalsection)showingwallthickening,luminal
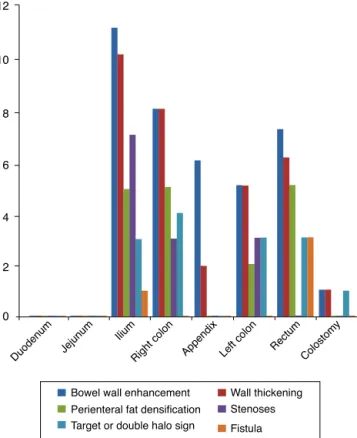
Table4–IntestinalsegmentsaffectedfoundinCT enterography.
Intestinalsegment n %
Duodenum 0 0
Jejunum 0 0
Ileum 11 32
Rightcolon 9 26
Appendix 5 15
Leftcolon 6 18
Rectum 7 21
Colostomy 1 3
Note:somepatientspresentedmorethanoneaffectedsegment.
Withthedevelopmentofimagingstudies,the enterogra-phy,eitherbycomputedtomographyormagneticresonance, isreplacingintestinaltransitandenteroclysisproceduresin theevaluationofthesmallbowelbyimagingprocedures.The advantageofCTenterographyisthatthis procedureallows visualizationoftheentiresmallintestine,withoutloop over-lapping,andalsoallowstheevaluationoftheintestinalwall, detectionofextra-luminalpathologicalconditions,and poten-tialassociatedchanges.
Manyofthesefindings arenotseenintraditional endo-scopicstudies,whichsupportstheprogressivereplacementof oldmethodsbyenterographyasthemainmethodofdiagnosis forinflammatoryboweldisease(IBD).5–8
EarlystudieswithCTenterographyshowedahighdegree
ofsensitivity,above85%,forthediagnosisofactiveCD
ver-susbariumenteroclysis.Recentstudieshavedemonstrateda
Bowel wall enhancement 12
10
8
6
4
2
0
Wall thickening Perienteral fat densification Stenoses
Duodenum Jejunum Ilium
Right colon Appendix Left colon Rectum
Colostomy
Target or double halo sign Fistula
Fig.5–FindingsofCTenterography,accordingtothe affectedsegment.Note:morethanoneinthesamepatient
werefound.
sensitivityrate ofup to100%,and 53.9%specificity forthe
identification ofCD initsactivephase.7 Other publications
haveshownthatCTenterographyisequivalenttoMR
enterog-raphyintheassessmentofCDactivity.
DespitestudiesshowinggoodresultswithCT
enterogra-phy,therearefewpublicationsonthissubjectinBrazil;thus,
itiscriticalthatthisstudyiscarriedoutinourmidst.
Discussion
CTenterographyhasaclinicalapplicationintheevaluation
ofpatientswithCD,toconfirmthediagnosisofthedisease
oritsextensionandcomplicationsintheassessmentofsmall
bowel.3Nowadays,CTenterographyconstitutesanexcellent
optionforreplacementoflower-accuracyradiological
meth-odsandasanalternative versusendoscopiccapsule,avery
expensivetechnology.
Asinother studies,2 wealsoobservedpredominanceof
female patients(58%), and higherincidenceinCaucasians,
followedbyBrown,Yellow,andBlackpatients.
Inthispaper,thesectorsmostaffectedbyCDlesionswere
ileum(32%)followedbyrightcolon(26%).Iftheinvolvement
ofcecalappendix(14%)isincluded,aclearpredominanceof
involvementintheileocecaltransitionwillbenoted,
accord-ing to the literature. The large intestine was the second
mostaffectedarea,alsoaccordingtoobservationsbyother
authors.9–11
The most observed radiological signs in this study
were intestinalwallenhancementand thickening,vascular
engorgement,reactivelymphnodes,andperienteralfat
den-sification, which is inagreement with the literature,since
Costa-Silvaetal.3andIlangovanetal.12foundsimilarresults.
Considering that, at its inception, DC usually presents in
theinflammatoryform,onecanreallyexpectthatthereare
largenumbersofpatientswithwallthickeningandvascular
engorgement. Whereasmostofourpatientsevaluated had
recentdiagnoses,actuallytheseweretheexpectedfindings.
Inthisstudy,thesechangeswereobservedin88%ofpatients.
Afifietal.13alsoobservedthesekeyfindingsinpatientswith
active Crohn’s disease. Moreover, these authors compared
thesechanges versussurgical evaluationofpatients
under-going resection due to CD, and founda good clinical and
radiologicalcorrelation.
Thereseemstobenolargedifferenceinaccuracywhen
comparingCTenterographyversusMRenterography,except
that tomography is superior in detecting infectious
com-plications; and for this reason, often this technique is
recommendedasfirstchoiceintheevaluationofthe small
intestine, immediately after diagnosis, as well as in cases
wherethereissuspicionofabdominalabscesses.Inthe
fol-lowingrevaluations,maybethereisagreateradvantagewith
theuseofresonance,becausethistechniquedoesnotexpose
thepatienttoionizingradiation.Inthisstudy,wechosetouse
CTenterographybecausethisistheprocedureavailableinour
environment–afactthatisalsoobservedinmostBrazilian
medicalcenters,especiallyamongpublictertiary hospitals,
wherethereisamuchhighernumberoftomographsin
Perianal lesions associated with urinary tract infection
werepresentin10(29%)patients,two(5.8%)menandeight
(23%)women.Diarrheaandweightlosswereobservedin19
(55%)patients.Suchanassociationmayberelatedtothe
mal-absorptionsyndromeobservedinCDpatients.2
Importantly, cross-sectional studies reflect certain
momentsofthesample;thus,changesmayoccurinseveral
aspectsanalyzedover time,and withtheinclusion ofnew
patients.
Conclusion
Thestudy allowsonetoobservethatthe mainradiological
findingsofCTenterographywereintestinalwallenhancement
andthickeningandvascularengorgement,mainlyaffecting
theileumandrightcolon.Themainclinicalmanifestations
inourpatientswerediarrheaandabdominalpain.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. Habr-GamaA,CerskiCTS,MoreiraJPT,CasertaNMG,Oliveira JúniorO,AraújoSEA.DiretrizesdaAssociac¸ãoMédica Brasileira.Doenc¸adeCrohnintestinal:manejo.RevAssoc MedBras.2011;57:10–3.
2. SantosSMR[TeseMestrado]Doenc¸adeCrohn:Etiopatogenia,
aspetosclínicos,diagnósticoetratamento.Porto,Portugal.:
UniversidadeFernandoPessoa;2013.Availablefrom:
http://hdl.handle.net/10284/4100
3.Costa-SilvaL,MartinsT,PassosMCF.Enterografiapor tomografiacomputadorizada:experiênciainicialnaavaliac¸ão dasdoenc¸asdointestinodelgado.RadiolBras.2010;43:303–8.
4.GlickSN.Critériosdeadequac¸ãodeexamesdeimageme radioterapia.SãoPaulo:ColégioBrasileirodeRadiologia;2005. p.309.
5.D’IppolitoG,BragaFA,ResendeMC,BretasEAS,NunesTF, RosasGQ,etal.Enterografiaportomografia
computadorizada:umaavaliac¸ãodediferentescontrastes oraisneutros.RadiolBras.2012;45:139–43.
6.HanauerSB,SandbornW.PracticeParametersCommitteeof theAmericanCollegeofGastroenterology.Managementof Crohn’sdiseaseinadults.AmJGastroenterol.2001;96:635–43.
7.CakmakciE,ErturkSM,CakmarkciS.Comparisonofthe resultsofcomputerizedtomographicanddiffusion-weighted magneticresonanceimagingtechniquesininflammatory boweldiseases.QuantImagingMedSurg.2013;3:327–33.
8.AmitaiMM,Ben-HorinS,EliakimR,KopylovU.Magnetic resonanceenterographyinCrohn’sdisease:aguideto commonimagingmanifestationsfortheIBDphysician.J Crohn’sColitis.2013;7:603–15.
9.FariaLC,FerrariMLA,CunhaAS.Aspectosclínicosdadoenc¸a deCrohnemumcentrodereferênciaparadoenc¸as
intestinais.GEDGastroenterolEndoscDig.2004;23:151–64.
10.HardtMR,KotzePG,TeixeiraFV,LudvigJC,MallutaEF, KleinubingHJr,etal.Epidemiologicalprofileof175patients withCrohn’sdiseasesubmittedtobiologicaltherapy.J Coloproct.2012;32:395–401.
11.Kleinubing-JuniorH,PinhoMSL,FerreiraLC,BachtoldGA, MerkiA.Outpatientsprofilewithinflammatorybowel disease.ABCDArqBrasCirDig.2011;24:200–3.
12.IlangovanR,BurlingD,GeorgeA,GuptaA,MarshallM,Taylor SA.CTenterography:reviewoftechniqueandpracticaltips. BrJRadiol.2012;85:876–86.