SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Randomized
clinical
trial
between
proximal
row
carpectomy
and
the
four-corner
fusion
for
patients
with
stage
II
SNAC
夽
Marcio
Aurelio
Aita
∗,
Edison
Kenji
Nakano,
Henrique
de
Lazari
Schaffhausser,
Walter
Yoshinori
Fukushima,
Edison
Noboru
Fujiki
FaculdadedeMedicinadoABC,DepartamentodeOrtopediaeTraumatologia,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2September2015 Accepted29January2016 Availableonline20August2016
Keywords:
Wrist Pain
Scaphoidbone Arthrodesis
a
b
s
t
r
a
c
t
Objective:TocomparetheoutcomesofpatientswithstageIISNACsubmittedtosurgical treatmentbyproximalrowcarpectomy(PRC)orfour-cornerfusion(FCF).
Method:Twenty-sevenpatientsaged18–59years(mean37.52years)wereincluded.Thirteen patientsunderwentPRCinGroupA,and14underwentFCFofthewristinGroupB. Evalua-tionsweremadebeforeandaftersurgerywithfollow-upbetween45and73months.Range ofmotion(ROM);painassessmentwithavisualanalogscale(VAS);gripstrength;disability ofthearm,shoulder,andhand(DASH);andreturntoworkwereevaluated.
Results:GroupApatientshad68.5%andGroupBpatients,58.01%oftheROMofthe con-tralateralside.TheVASscorewas2.3inGroupAand2.9inGroupB.Gripstrengthwas78.67% and65.42%,respectively,relativetothesidenotaffected.TheDASHscorewas11forPRC and13forFCF.InGroupA,9/13(69.23%)andinGroupB,8/14(57.14%)patientsarecurrently working.Complicationsweresymptomaticosteoarthritisinthemid-carpaljointinGroup AandlooseningofascrewinGroupB.
Conclusion:Theclinicalandfunctionalresultsdonotpresentstatisticallysignificant differ-encesforbothanalyzedmethods.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Ensaio
clínico
randomizado
entre
ressecc¸ão
da
fileira
proximal
(carpectomia)
e
artrodese
dos
quatro
cantos
nos
pacientes
portadores
de
SNAC
no
estágio
II
Palavras-chave:
Punho Dor
Ossoescafoide Artrodese
r
e
s
u
m
o
Objetivos:Compararosresultadosclínicosefuncionaisdospacientescomdiagnósticode
ScaphoidNonUnionAdvancedColapse(SNAC),noestágioII,submetidosàressecc¸ãodafileira proximaldocarpoouàartrodesedosquatrocantos.
Método:Foramincluídosnoestudo27pacientes,commédiade37,52anos(18-59).Treze foramsubmetidosàcarpectomiaproximalnoGrupoAe14àartrodesedosquatrocantos
夽
StudyconductedattheHandandMicrosurgeryGroup,DepartmentofOrthopedicsandTraumatology,FaculdadedeMedicinadoABC, SantoAndré,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.A.Aita).
http://dx.doi.org/10.1016/j.rboe.2016.08.008
noGrupoB.Oseguimentomédiofoide45a73meses.Foramavaliadososarcosde movi-mento,ador,aforc¸adepreensãopalmar,oDisabilityArmShoulderHand(DASH)escoreeo retornoaotrabalho.
Resultados: NoGrupoAospacientesapresentaram68,5%doarcodemovimentonolado nãoafetadoenoGrupoB,58,01%.Naavaliac¸ãosubjetivadador(VAS),obtivemos2,3no GrupoAe2,9noGrupoB.Aforc¸adepreensãopalmarfoide78,67%noGrupoAdolado nãoacometidoede65,42%noGrupoB.ODASHescorenoGrupoAfoi11enoGrupoB, 13.Quantoaotrabalho,69,23%(9/13)dospacientesnoGrupoAe57,14%(8/14)noGrupoB retornaramaalgumaatividadelaboral.Ataxadecomplicac¸õesnoGrupoAfoide(1/13)e noGrupoB,de7,1%(1/14).
Conclusões: Osresultadosclínico-funcionaisestudadosnãoapresentamdiferenc¸as estatís-ticasparaosdoismétodosanalisados.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Scaphoidfractureisacomplexinjury,representingthemost incidentinjuryamongcarpalbones;sometimes,itisnot diag-nosed and evolves with high rates of complications, such aspseudarthrosis, necrosisofthe proximalpole, and even osteoarthritisoftheentirewrist.Pseudarthrosis,ifuntreated, causes aburden on the radialside ofthe carpus, promot-ing degeneration ofthe radioscaphoid joint, mainly inthe radialstyloidprocess, which leadsto alocal impact. With evolution,theoutlineofthescaphoidisworndown,which affects the scaphocapitate and capitolunate joints, caus-ingproximalmigrationofthecapitateandpromotescarpal derangement,1–3describedasscaphoidnon-unionadvanced
collapse(SNAC).Toguidetreatmentofthisdisease,the clas-sificationaccordingtothestagesofWatsonandRyu1isused.
Thedevelopmentstagesaredescribedasfollows:
1. Stylo-scaphoidosteoarthritis–SNACstageI;
2. Stylo-scaphoid+radioscaphoidosteoarthritis–SNACstage II;
3. Stylo-scaphoid+lunocapitateosteoarthritis–SNACstage III;
4. Stylo-scaphoid+lunocapitate osteoarthritis+radiolunate osteoarthritis–SNACstageIV.
No published study has concluded which is the best method for treating this disease; arthrodesis carpectomy and four-corner fusion (FCF) are the most studied meth-ods.Thesesurveysshownoscientificevidence,4–8sincethey
areretrospectivestudies,non-randomized,andincludeother degenerativediseasesofthecarpus,suchaspost-traumatic osteoarthritisofthe wrist,Kienböckdisease,and scapholu-nate advanced collapse(SLAC). Other randomizedstudies9
thataddressedthesameconditionsotherthanSNAC10were
alsonon-conclusive.
Onlypatients withthe disease in stageII may undergo salvagesurgery,2,11–13whichpreservessomedegreeof
move-ment, as do carpectomy14–18 and FCF.1,19–21 Patients in
stageI should undergo reconstructive surgery,such asthe correctionofthescaphoidnon-union3and/orradial
styloidec-tomy.Thosewhohaveradiographicchangesoflunocapitate
joint (stage III) cannot undergo carpectomy, only partial wrist arthrodesis.11,19,22–24 Patients in stage IV have the
best treatment option in salvage surgeries, such as total fusion,2,11,25or totalwristarthroplasty, whoseindicationis
stillcontroversial.26
Bothforcarpectomy18,27,28 andFCF,29studiespresented
satisfactory long-term clinical and functional results, with approximatelytenyearsoffollow-up.Buttherearestill ques-tionsaboutwhatisthebestmethodoftreatmentforpatients withpain,lossofhandgripstrength,andrangeofmotion lim-itationtoperformdailylifeorprofessionalactivities.Forthese reasons,theauthorsdecidedtoperformthisclinicaltrial.
Thisstudyaimedtocomparetheclinicalandfunctional outcomes ofpatients with stageII1 SNAC who underwent
proximalrowcarpectomy(PRC)orFCF.
Methods
From2005toDecember2014,78patientstreatedinthe out-patientclinicsoftheHandandMicrosurgeryDepartmentand diagnosedwithSNACwereevaluated.Only27metinclusion criteriaandwereincludedinthestudy;theyunderwent physi-calexamination,plainradiographsinposteroanterior(PA)and lateral (P), computed tomography,and magnetic resonance imaging(MRI)oftheaffectedwrist.
Inclusioncriteriawereadultpatientsaged18–60years,of bothgenders, withclinical andimagingdiagnosis ofSNAC (Fig. 1), instageII, who signedtheinformed consentform andtheconflictofinterestprotocol,aspertheResearchEthics Committeedecision.Patientswithassociatedwristdiseases, suchasbonemetabolicdiseases,orwhohadundergoneany priorsurgicalprocedure,orthosewhohadbilateralconditions onthewrists,wereexcluded.
Functionalassessmentwasconductedbythe profession-alsfromtheHandOccupationalTherapyDepartmentofthe institution,whodidnothaveaccesstoinformationregarding thegrouptowhichthepatientbelonged.
Fig.1–Preoperativetests:(a)wristX-rayinposteroanterior(PA);(b)X-rayinprofile(P);(c)coronaltomographicsliceofthis wrist.
Clinicalanalysisofpain wasmadewiththe visual ana-log scale(VAS) from 0to10,forsubjectiveevaluation. The assessment of quality of life was made with the DASH questionnaire.13
Randomization was done by drawing lots with a coin: heads,thepatientwouldundergoPRC(Fig.2);tails,FCF(Fig.3). Therefore, patientswere dividedinto twogroups, Aand B. Group A(heads) underwent resection ofthe proximal row
(Table1),withinterpositionofthedorsalwristcapsule.14–18
PRC
surgical
technique
Dorsalandoblique surgicalapproach,usingthebaseofthe secondmetacarpalboneandthedistalradioulnarjoint,was thesameforbothgroups.
A single transverse opening of the dorsal capsule was made; a flap was created to contour the head of the capitate.15,16
Atthatmoment,proximalcarpectomywasmadewiththe removalofthescaphoid,lunate,andtriquetrum.
Aradiusstyloidectomy,ofatmost2mm,wasmandatory. Then,thedorsalcapsulewasinterposedandtheflapwas sutured in the palmar capsule, followed by sutures ofthe planesandskin.
Subsequently,postoperativefluoroscopyand radiographs ofthewristweremadeforpost-operativecontrol.
FCF
surgical
technique
Patients in Group B (Table 2) were treated using the FCF technique:theyunderwenttwodorsalarthrotomies,onefor resectionofthescaphoidboneandtheotherforfixationof thefourcorners.
Aftertheremovalofthescaphoidboneandthepreparation ofthegraftofthesamebone,thefourcornerswereopened.
Atthispoint,athickcavityofsimilarthicknesstocarpal boneswascreatedinthecenterofthefourcorners,wherethe scaphoidgraft wasplaced.Thefour cornerswereprepared withaspecialmillprovidedbythemanufacturer.Thelunate andtriquetrumwereappropriatelyreducedwithprovisional Kirschnerwires.
Allfourbones(lunate,capitate,hamate,andtriquetrum) were stabilized with a special plate (conventional carpal button®bySBI®, orblockedcarpalbuttonbyBiotech®)and screws.15–17
Postoperative
period
of
Groups
A
and
B
Forcompletionoftheprocedure,wristfluoroscopyand radio-graphywereperformedtoassessthepositionoftheimplant andscrews.
A plastercast was made around the wrist, which was removedinthefirstweekaftersurgery.
Patients were clinically and radiographically evaluated beforesurgeryandthenonamonthlybasis.However,inthe presentstudy,onlythepreoperativeandcurrentvalueswere usedforstatisticalanalysis.Allpatientsunderwent rehabili-tationattheHandOccupationalTherapyDepartmentofthe institution,withthesameprotocol,fromthefirstweekafter thesurgery,whentheimmobilizationwasremoved,until dis-chargefromthedepartment.
GroupAcomprised13patientswithameanof32.38years, whounderwentPRC(Fig.2).
GroupBcomprised14patientswithameanof40.43years, whounderwentFCF(Fig.3).
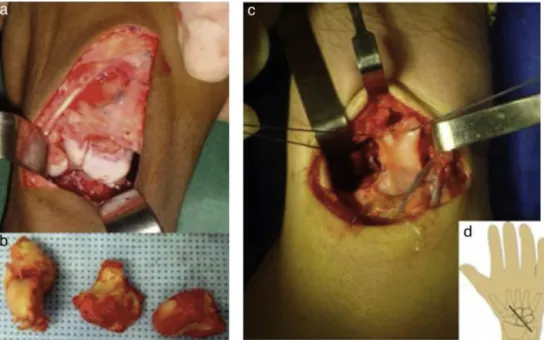
Fig.2–Intraoperativeaspectofresectionoftheproximalcarpalrow.(a)Dorsalaccesstothewrist;(b)scaphoid,lunate,and triquetrumremoved;(c)makingoftheflapinthewristdorsalcapsule,whichwasusedtocoattheheadofthecapitate;(d) planningthewristaccessroute.
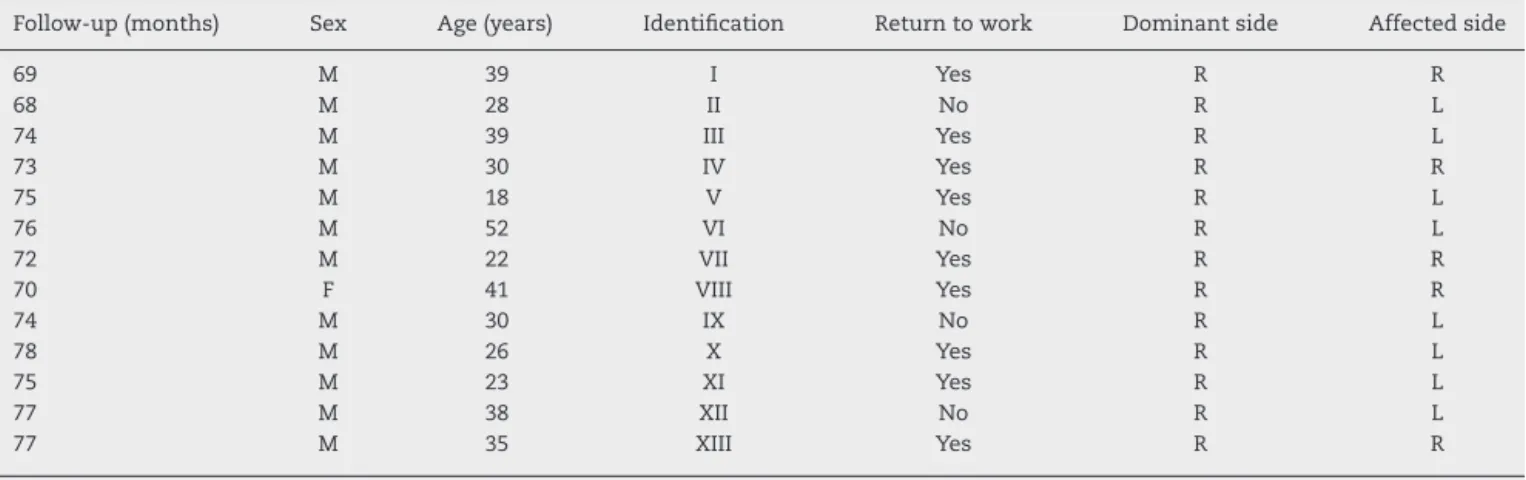
Table1–Epidemiologicaldistributionandpostoperativefollow-upofpatientsundergoingproximalcarpectomy(Group A).
Follow-up(months) Sex Age(years) Identification Returntowork Dominantside Affectedside
69 M 39 I Yes R R
68 M 28 II No R L
74 M 39 III Yes R L
73 M 30 IV Yes R R
75 M 18 V Yes R L
76 M 52 VI No R L
72 M 22 VII Yes R R
70 F 41 VIII Yes R R
74 M 30 IX No R L
78 M 26 X Yes R L
75 M 23 XI Yes R L
77 M 38 XII No R L
77 M 35 XIII Yes R R
Source:Hospital’sSAME.
Table2–Epidemiologicaldistributionandpostoperativefollow-upofpatientsundergoingfour-cornerarthrodesis(Group B).
Follow-up(months) Sex Age(years) Identification Returntowork Dominantside Affectedside
77 M 56 I Yes R R
77 M 25 II Yes R L
81 M 40 III Yes R L
71 F 39 IV No R L
75 F 30 V Yes R R
78 M 33 VI Yes R R
74 M 45 VII No R R
76 M 34 VIII Yes R L
68 M 54 IX No R L
69 M 48 X Yes R L
68 M 37 XI No R R
78 M 36 XII Yes R R
70 M 48 XIII Yes R R
67 M 41 XIV No R L
Source:Hospital’sSAME.
value(p)wasequaltoorgreater than5%(0.050),a statisti-callynon-significantdifferencewasobservedanditwasnot marked.Fornonparametricvariables,Fisher’sexacttestwas used.
Results
ThevaluesofGroupAforrangeofmotionwere68.50%,and forhandgripstrength,78.67%,bothcomparedwiththe unaf-fectedside;GroupB,whichunderwentFCF,presentedrangeof motionof58.01%,andhandgripstrengthof65.42%.The sub-jectiveassessmentofpainwas2.3inGroupAand2.9inGroup B.TheDASHscorewas11forGroupAand13forGroupB.In relationtoreturntowork,64.3%(9/14)and84.61%(11/13)of patientsinGroupsAandB,respectively,performsomework activity(Tables3–5).
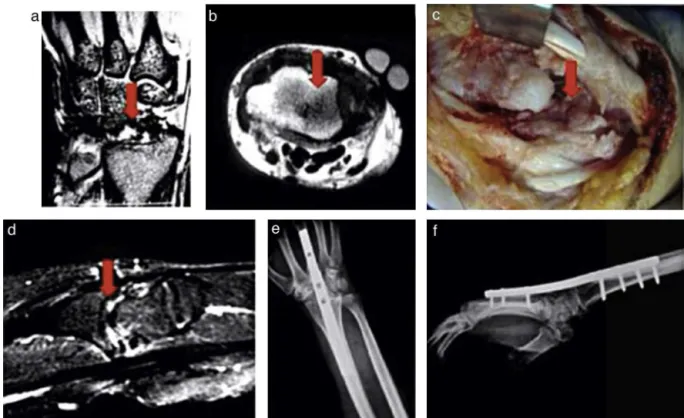
The complication rate observed in Group A was 7.69% (1/13), a patient diagnosed with symptomatic osteoarthri-tis in the radiocarpal joint (Fig. 4) who required total wrist arthrodesis; in Group B, this rate was 7.1% (1/14),
composedbyasinglepatientwithdiagnosisof pseudarthro-sis of the four corners and loosening of the screws. This patient was satisfied with his wrist functional outcome (Fig.5).
Table3–Clinicalandfunctionalresults–comparative analysisbetweengroups.
Parameters Carpectomy Arthrodesis
(GroupA) (GroupB)
Pain(VAS) 2.3 2.9
DASH 11 13
Force(kgf) 78.67% 65.42
ROM(◦) 68.50% 58.01%
Returntowork 84.61% 64.30%
Complications 7.69% 7.10%
VAS,VisualAnalogScore;DASH,DisabilitiesoftheArm,Shoulder andHand;ROM,rangeofmotion.
Table4–Statisticalresultsofparametricvariables.
Variable Group n Mean Standarddeviation Significance
(p)
Follow-uptime A 13 74 3.37 0.846
B 14 74.21 2.79
Age A 13 32.38 9.39 0.039*
B 14 40.43 8.94
Preoperativepain A 13 7.54 2.50 0.645
B 14 8.21 1.81
Postoperativepain A 13 2.3 3.55 0.769
B 14 2.9 3.45
PreoperativeDASH A 13 99.62 24.46 0.331
B 14 91.71 18.00
PostoperativeDASH A 13 47.62 15.47 0.697
B 14 45.00 10.93
Preoperativestrength A 13 40.38 17.11 0.827
B 14 40.64 19.88
Postoperativestrength A 13 78.5 18.89 0.145
B 14 56.0 11.69
PreoperativeROM A 13 80.54 54.75 0.132
B 14 50.64 28.55
PostoperativeROM A 13 108.85 36.29 0.593
B 14 118.36 39.76
n,numberofpatients;DASH,DisabilitiesoftheArm,ShoulderandHand;ROM,rangeofmotion.
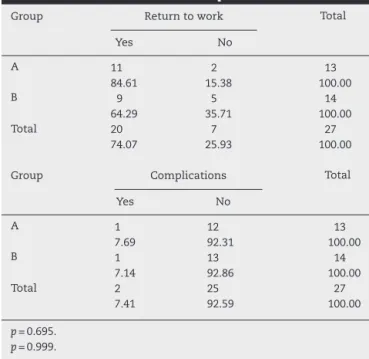
Table5–Statisticalresultsofnonparametricvariables.
Group Returntowork Total
Yes No
A 11 2 13
84.61 15.38 100.00
B 9 5 14
64.29 35.71 100.00
Total 20 7 27
74.07 25.93 100.00
Group Complications Total
Yes No
A 1 12 13
7.69 92.31 100.00
B 1 13 14
7.14 92.86 100.00
Total 2 25 27
7.41 92.59 100.00
p=0.695. p=0.999.
Discussion
The present authors agree with Mulford and Krimmer7,11:
thesearethetwomostcommonlyusedmethodsinthe treat-mentofSNAC.Thus,bothhavetheiradvantages.
Accordingtotheliterature,4–7,18,19,29FCFhasasadvantages
inrelationshiptoPRCthemaintenanceofcarpalheightand preservationoftheradiolunatejointand,asdisadvantages, thesteeperlearningcurve,greaterincidenceofcomplications withtheuseofcircularplates,19–21andhighercost.
AccordingtoImbriglia,18PRCdoesnotpreservethe
mid-carpaljoint,andcanleadtodegenerationoftheradiusorthe headofthecapitate.
In order to protect the radio-capitate joint space, the authorschosetoperformaninterpositionofthedorsalwrist capsule15,16 and earlier joint mobility, with the removalof
immobilization aftera periodnot longer than oneweek.17
However,otherauthors27,28 haveobservedlong-termresults
ofdegenerativeradiographicalterationontheradiusoreven onthe headofthecapitate, withoutclinicalconsequences. In the present study, one patient from Group Apresented radiographicalterationsoftheradiallunatefossa,withclinical repercussionsoneyearaftersurgery.
Inthepresentstudy,carpalbutton®andbonegraftinblock were usedforFCF.Mantovannietal.,19 andMerrelletal.,20
whoalsousedcircularplatesintheirresearch,andsuggested modificationstothetechnique,suchasusingblockgraft har-vest from the scaphoidor metaphysis ofthe distalradius, showedsuperiorresultswithlowerrateofcomplicationthan thatobservedbyKendalletal.21 Therewere nostatistically
significantdifferencesinfunctionalparametersafteroneor tenyearspostoperativeinpatientswhounderwentFCF.29In
thepresentstudy,therewasonlyonecaseofpseudarthrosisof thefourcorners,withreleaseofascrewinthecarpalbutton. TherangeofmotioninGroupA(PRC)was68.50%in rela-tiontothecontralateralsideinthepresentstudy;Tomaino et al.4observed64%;Wryicketal.,57%;Cohenand Kozin,6
57%;DiDonnaetal.,2761%;andJebsonetal.,2863%.InGroupB,
58.01%ofwristrangeofmotioncomparedtothenon-affected side was observed; Tomaino et al.4 observed 41%; Wryick
etal.,547%;CohenandKozin,664%;andKendalletal.,21;46%.
Fig.4–Additionalpreoperativeexamsandintraoperativeaspects(complication)ofthesecondproceduretocorrect radio-capitateosteoarthritis.(a)coronalMRIofthewrist;(b)axialMRIofthewrist;(c)intraoperativeimageofradial osteoarthritisandtheintegrityofthecartilageoftheheadofthecapitatebone;(d)sagittalMRIofthewrist;(e)X-rayofthe wrist,inposteroanterior(PA);(f)X-rayofthewristinprofile(P)–totalarthrodesisprocedure.
GroupAinthepresentstudy(78.67%ofthenormalside)are comparedwiththeliterature,Tomainoetal.4observed96%;
Wryicketal.,594%;CohenandKozin,6 71%;Bisnetoetal.,9
47%;Imbriglia,1880%;Didonnaetal.,2791%;andJebsonetal.,28
83%.InGroupB,thehand gripstrength was65.42%ofthe unaffectedside;Tomainoetal.,4observed81%;Wryicketal.,5
74%;CoheneKozin,679%;Bisnetoetal.,973%;andKendall
etal.,2156%.Therewerenosignificantdifferencesinclinical
andfunctionalresults.
The complication rate was 7.69% in Group A and 7.1% in Group B; Tomaino et al.4 observed 0%; Jebson et al.,28
10%; Didonna et al.,27 18%; Cohen and Kozin,6 0%;
Wry-ick et al.,5 11%; Kendall et al.,21 62.5%; and Imbriglia,18
3.7%.Radio-capitatejointdegenerationisfrequent7,27,28(12/26
patients after ten years of follow-up) and asymptomatic in most patients,18 but one patient, an active adult who
returned to work, evolved poorly with radio-capitate joint degeneration,7,12,18andunderwenttotalwristarthrodesis.18,25
Althoughnotstatisticallysignificant,theindicationof carpec-tomy in young adult patients should beavoided. Group B presentedinferiorresultswhencomparedwithstudiesthat used circular plates, and similar results when compared with studies that used Kirschner wires and screws, per-hapsduetheimprovementofthemethodandsafetyofthe technique.7,12,19,20Thecomplicationobservedinthepresent
trial was pseudarthrosis of the four corners; this patient declinedrevisionsurgery,ashewassatisfiedwithhisclinical andfunctionaloutcome.
Asforthereturntowork,resultswereverysimilartothose from theliterature.Return towork activitieswas observed in 69.23% of patients who underwent PRC in the present study;86%inthestudybyCohenandKozin6and80%,inthe
studybyTomainoetal.4OfthepatientswhounderwentFCF
inthepresent study,57.14%returnedtowork;100%inthe studybyTomainoetal.4and86%inthestudybyCohenand
Kozin.6
Therewasnostatisticaldifferencebetweenthegroupsfor this variable.However,the authors believe that the above-mentioned data presentedobjective and subjective values; therefore,theydonotconsidertheresultofthevariable of returntoworktobereliable.
When comparing both methods, the literature4–8,12
presentsaslightsuperiorityinallanalyzedfunctional param-etersofpatientsundergoingPRC,exceptforthestudies by CohenandKozin6andbyBisnetoetal.,9whoobservedbetter
handgripstrengthresultsforpatientsundergoingFCF. Todate,noarticlefeaturesonlypatientswiththe same initialconditionofSNAC,whichleadstowristosteoarthritis. MoststudiesusingFCFforthetreatmentofosteoarthritisdid notstandardizethewristosteosynthesistechniquefor fixa-tionofthefourcorners(whichcombinestheuseofKirschner wires,compressionbolts,orcircularplates).Ofthe aforemen-tionedstudies,onlyonewasrandomized9;nevertheless,itdid
notstandardizetheinitialpathologythatprogressedtocarpal collapse.Onestudy10includedonlypatientswithSLACand
hadshorterhospitalstayandlowercomplicationrateinfavor ofPRC; those authors suggested the use ofthis procedure forstagesIand II. ThestudybyMulford et al.,7 a
system-aticreviewof52articles,alsosuggestedPRCastheprocedure withthe lowest complicationrate; the authors highlighted
radio-capitateosteoarthritis,whichinmostpatientsis asymp-tomatic.
Forthesereasons,somedifferencesinthevariablesstudied maybeobservedwhencomparedwiththoseofthepresent study.
Both are salvage surgeries that present functional and sociallimitations,withdecreasingvaluesinallcriteria ana-lyzedwhencomparingthesewristswiththeuninvolvedside. Inthecomparisonwithothermethodsofsurgicalsalvage treatment, suchasarthroplastyandtotalwristarthrodesis, thepresentstudypresentedsuperiorDASHscoreswhen com-paredwiththestudybyAndersonandAdams26andsuperior
returnwhencomparedwiththatbyWeissandHastings.25
When compared to other procedures of partial wrists arthrodesis,suchasradioscapholunatefusion,whichallows forwristmobilityinthe midcarpaljoint,the resultsofthe presentstudyarealsosuperiortothatobservedbySaffar,22
who observed 57% hand grip strength. Beyermann et al.23
observed aDASHscore24 of25.7.Dimitrios et al.24 showed
good resultsinaretrospectivestudy ofmodifiedmidcarpal arthrodesis,whereinaniliacgraftwasusedtomaintainthe carpal height,observing consolidationinallcases, without complications.
Conclusion
Patientshadclinicalandfunctionalimprovementofthewrist, increased hand grip strength,reduced pain, and improved qualityoflifeaftertreatmentofthisdiseasewithboth meth-odsusedinthistrial.
Clinicalandfunctionalresultsshowednostatistical differ-encesbetweenthetwomethods.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WatsonHK,RyuJ.Evaluationofarthristisofthewrist.Clin
OrthopRelatRes.1986;202:57–67.
2.KrakauerJD,BishopAT,CooneyWP.Surgicaltreatmentof
scapholunateadvancedcollapse.JHandSurgAm.
1994;19(5):751–9.
3.MackGR,BosseMJ,GelbermanRH,YuE.Thenaturalhistory
ofscaphoidnon-union.JBoneJointSurgAm.1984;66(4):504–9.
4.TomainoMM,MillerRJ,ColeI,BurtonRI.Scapholunate
advancedcollapsewrist:proximalrowcarpectomyorlimited
wristarthrodesiswithscaphoidexcision?JHandSurgAm.
1994;19(1):134–42.
5.WyrickJD,SternPJ,KiefhaberTR.Motion-preserving
proceduresinthetreatmentofscapholunateadvanced
collapsewrist:proximalrowcarpectomyversusfour-corner
arthrodesis.JHandSurgAm.1995;20(6):965–70.
6.CohenMS,KozinSH.Degenerativearthritisofthewrist:
proximalrowcarpectomyversusscaphoidexcisionand
four-cornerarthrodesis.JHandSurgAm.2001;26(1):94–104.
7.MulfordJS,CeulemansLJ,NamD,AxelrodTS.Proximalrow
carpectomyvs.fourcornerfusionforscapholunate(SLAC)or
systematicreviewofoutcomes.JHandSurgEur. 2009;34:256–63.
8. WeissKE,RodnerCM.Ostearthritisofthewrist:review
article.JHandSurgAm.2007;32(5):725–46.
9. BisnetoEN,FreitasMC,PaulaEJ,MattarRJr,ZumiottiAV.
Comparisonbetweenproximalrowcarpectomyand
four-cornerfusionfortreatingosteoarthrosisfollowingcarpal
trauma:aprospectiverandomizedstudy.Clinics(SãoPaulo).
2011;66(1):51–5.
10.VanhoveW,DeVilJ,VanSeymortierP,BooneB,VerdonkR.
Proximalrowcarpectomyversusfour-cornerarthrodesisasa
treatmentforSLAC(scapholunateadvancedcollapse)wrist.J
HandSurgEur.2008;33(2):118–25.
11.KrimmerH,KrapohlB,SauerbierM,HahnP.Post-traumatic
carpalcollapse(SLAC-andSNAC-wrist)–Stageclassification
andtherapeuticpossibilities.HandchirMikrochirPlastChir.
1997;29(5):228–33.
12.KiefhaberTR.Managementofscaphulunateadvanced
collapsepatternofdegenerativearthritisofthewrist.JHand
SurgAm.2009;34(8):1527–30.
13.JesterA,HarthA,WindG,GermannG,SauerbierM.Disability
arm,shoulderandhandDASHquestionnaire:determining
functionalactivityprofilesinpatientswithupperextremity
disorders.JHandSurgBr.2005;30(1):23–8.
14.StammTT.Excisionoftheproximalrowofthecarpus.ProcR
SocMed.1944;38(2):74–5.
15.FukushimaWY,FaloppaF.Doenc¸adeKienböck:ensaioclínico
randomizadoentreressecc¸ãodafileiraproximaldocarpo
comeseminterposic¸ãocápsuloligamentardorsal[tese].São
Paulo:UniversidadeFederaldeSãoPaulo(UNIFESP)–Escola
PaulistadeMedicina;2007.
16.HughesTBJr.Proximalrowcarpectomyandamodification
fordorsalcapsularinterposition.OperTechOrthop.
2007;17:94–101.
17.JacobsR,DegreefI,DeSmetL.Proximalrowcarpectomywith
orwithoutpostoperativeimmobilisation.JHandSurgEur.
2008;33(6):768–70.
18.ImbrigliaJE.Proximalrowcarpectomy.Techniqueand
long-termresults.AtlasHandClinics.2000;5:101–9.
19.MantovaniG,MathoulinC,FukushimaWY,ChoAB,AitaMA,
ArgintarE.Fourcornerarthrodesislimitedtothecentreusing
ascaphoidonepiecegraftandadorsalcircularplate.JHand
SurgEur.2010;35(1):38–42.
20.MerrellGA,McDermottEM,WeissAP.Four-cornerarthrodesis
usingacircularplateanddistalradiusbonegrafting:a
consecutivecaseseries.JHandSurgAm.2008;33(5):
635–42.
21.KendallCB,BrownTR,MillonSJ,RudisilLEJr,SandersJL,
TannerSL.Resultsoffour-cornerarthrodesisusingdorsal
circularplatefixation.JHandSurgAm.2005;30(5):
903–7.
22.SaffarP.Radio-lunatearthrodesisfordistalradialintra
articularmalunion.JHandSurgBr.1996;21(1):14–20.
23.BeyermannK,PrommersbergerKJ,LanzU.
Radioscapholunatefusionfollowingcomminutedfracturesof
thedistalradius.JTraumaEur.2001;26:169–75.
24.GiannikasD,KarageorgosA,KarabasiA,SyggelosS.
Capitolunatearthrodesismaintainingcarpalheightforthe
treatmentofSNACwrist.JHandSurgEur.2010;35(3):
198–201.
25.WeissAP,HastingsH2nd.Wristarthrodesisfortraumatic
conditions:astudyofplateandlocalbonegraftapplication.J
HandSurgAm.1995;20(1):50–6.
26.AndersonMC,AdamsBD.Totalwristarthroplasty.HandClin.
2005;21(4):621–30.
27.DiDonnaML,KiefhaberTR,SternPJ.Proximalrow
carpectomy:studywithaminimumoftenyearsoffollowup.
JBoneJointSurgAm.2004;86(11):2359–65.
28.JebsonPJ,HayesEP,EngberWD.Proximalrowcarpectomy:a
minimum10-yearfollow-upstudy.JHandSurgAm.
2003;28(4):561–9.
29.BainGI,WattsCA.Theoutcomeofscaphoidexcisionand
four-cornerarthrodesisforadvancedcarpalcollapseata