r e v b r a s r e u m a t o l . 2015;55(1):79–82
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Case
report
Macrophage
activation
syndrome
in
a
patient
with
systemic
juvenile
idiopathic
arthritis
Anna
Carolina
Faria
Moreira
Gomes
Tavares
a,∗,
Gilda
Aparecida
Ferreira
b,
Luciano
Junqueira
Guimarães
c,
Raquel
Rosa
Guimarães
a,
Flávia
Patrícia
Sena
Teixeira
Santos
aaHospitaldasClínicas,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
bDepartmentoftheLocomotorSystem,FaculdadedeMedicina,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
cServiceofReumathology,HospitaldasClínicas,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25October2012 Accepted10February2014 Availableonline28November2014
Keywords: Hemophagocytic lymphohistiocytosis Epstein–Barrvirus
Systemic-onsetjuvenileidiopathic arthritis
HLH-04treatmentprotocol
a
b
s
t
r
a
c
t
Machrophage activation syndrome (MAS) is a rare and potentially fatal disease, com-monly associatedwithchronicrheumaticdiseases, mainlyjuvenileidiopathic arthritis. Itisincludedinthegroupofsecondaryformsofhaemophagocyticsyndrome,andother causesare lymphoproliferativediseases andinfections.Itsmostimportantclinicaland laboratorialmanifestationsarenon-remittingfever,splenomegaly,bleeding,impairment ofliverfunction,cytopenias,hypoalbuminemia,hypertriglyceridemia,hypofibrinogenemia and hyperferritinemia.The treatment needstobestarted quickly,andthe majorityof caseshaveagoodresponsewithcorticosteroidsandcyclosporine.TheEpstein–Barrvirusis describedasapossibletriggerformanycasesofMAS,especiallyinthesepatientsin treat-mentwithtumornecrosisfactor(TNF)blockers.Intheserefractorycases,etoposide(VP16) shouldbeadministered,associatedwithcorticosteroidsandcyclosporine.Ourobjectiveis todescribeararecaseofMASprobablyduetoEBVinfectioninasubjectwith systemic-onsetjuvenileidiopathicarthritis,whichachievedcompleteremissionofthediseaseafter therapyguidedby2004-HLHprotocol.
©2014ElsevierEditoraLtda.Allrightsreserved.
Síndrome
de
ativac¸ão
macrofágica
em
paciente
com
artrite
idiopática
juvenil
sistêmica
Palavras-chave:
Síndromehematofagocítica VírusEpstein-Barr
r
e
s
u
m
o
A síndrome deativac¸ão macrofágica(SAM) é umadoenc¸ararae potencialmentefatal, normalmenteassociadaàsdoenc¸asreumáticascrônicas,emespecialaartriteidiopática juvenil.É incluídanogrupodasformassecundárias desíndromehemofagocítica,cujas
∗ Correspondingauthor.
E-mail:[email protected](A.C.F.M.G.Tavares).
http://dx.doi.org/10.1016/j.rbre.2014.02.020
80
rev bras reumatol.2015;55(1):79–82Artriteidiopáticajuvenilforma sistêmica
ProtocolodetratamentoHLH-04
outras causas podem seras doenc¸as linfoproliferativas e infecc¸ões.As manifestac¸ões clínicas e laboratoriais mais importantes são a febre não remitente, esplenomegalia, hemorragias, disfunc¸ão hepática, citopenias, hipoalbuminemia, hipertrigliceridemia e hiperferritinemia. O tratamento deve seriniciado rapidamente,e a maioria dos casos responde bemaoscorticosteroideseà ciclosporina(CSA).OvírusEpstein-Barr (EBV)é descrito comopossível gatilhoparamuitos casosde SAM,especialmente naquelesem tratamentocombloqueadoresdofatordenecrosetumoral(TNF).Noscasosrefratáriosao tratamentoconvencional,etoposide(VP16)deveseradministrado,emassociac¸ãocom corti-costeroideseCSA.Nossoobjetivofoidescreverumcasorarodesíndromehematofagocítica provavelmentesecundáriaàinfecc¸ãopelovírusEpstein-Barr(EBV),empacientecomartrite idiopáticajuvenilsistêmica,confirmadapelasmanifestac¸õesclínicaselaboratoriaistípicas, mielogramaesorologiapositivacontraoEBV,queatingiuremissãocompletaapósinclusão noprotocolodetratamentoHLH-04.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hemophagocytic lymphohistiocytosis (HLH) is a rare and potentiallyfataldisease.Itsannualincidenceis1:50,000 live-borninfants.Itcanbedividedintotwogroups:primaryand secondary.
Macrophage activation syndrome (MAS) is a severe complication of rheumatic diseases that occurs much more frequently in patients with systemic juvenile idio-pathic arthritis (SJIA). It is characterized by fever, hep-atosplenomegaly, cytopenias, liver dysfunction, bleeding diathesis and neurological symptoms, revealing a hetero-geneoussyndrome, which makesits detection harder.The presenceofmacrophagesactivelyphagocytosing hematopoi-etic cellsin the liver, spleen,bonemarrow or lymphnode confirms the diagnosis.1,2 The criteria formulatedfor HLH
diagnosis (Table1)may not beuseful todefine MAS.2 The
greatchallenge is todifferentiate it from the exacerbation oftheunderlyingdisease.1,3,4Theclinicalmanifestationsof
Table1–Diagnosticcriteriaforhemophagocytic lymphohistiocytosis(HLH).
A.MoleculardiagnosiscompatiblewithHLH:pathologicalmutations ofPRF1,UNC13D,Munc18-2,Rab27a,STX11,SH2D1A,orBIRC4 OR
B.5ofthe8criterialistedbelow:
1.Fever(temperaturegreaterthan38.3◦C); 2.Splenomegaly;
3.Cytopenias(involvementofatleast2lineages) 3.1.Hemoglobin<9g/dLor<10g/dLinnewborns 3.2.Platelets<100,000mL
3.3.Neutrophils<1000mL;
4.Hypertriglyceridemia(>265mg/dL)orhypofibrinogenemia (<150mg/dL);
5.Hemophagocytosisinthebonemarrow,spleen,lymphnodesor liver–noevidenceofmalignancy;
6.ReducedorabsentactivityofNKcells; 7.Serumferritin>500ng/dL;
8.IncreasesolubleCD25(>2.400U/mL)
Source:HistiocyteSociety–TreatmentProtocolofTheSecond Inter-nationalHLHStudy2004.
bothshowed40%similarity.5ThepathogenesisofMAS
con-sistsofcytokineoverproductionandexuberantinflammation, leading to uncontrolled macrophage phagocytosis,antigen presentation andpersistent activation ofTlymphocytes.6,7
PrevalenceismoreoftenstudiedinSJIApatients,estimated tobebetween7%and13%.3
MASisincludedinthegroupofsecondaryformsofHLH, whose causes are lymphoproliferative diseases, infections (viral,bacterial,parasiticandfungal)andrheumaticdiseases. Geneticmutations,whichcompromisesecretionofperforins, arethemaintriggerintheprimaryform.
OurobjectivewastodescribeacaseofMASprobablydue toEpstein–Barrvirus(EBV)infectionandshowhowthe appro-priatetreatmentwasessentialforafavorableoutcome.
Case
report
rev bras reumatol.2015;55(1):79–82
81
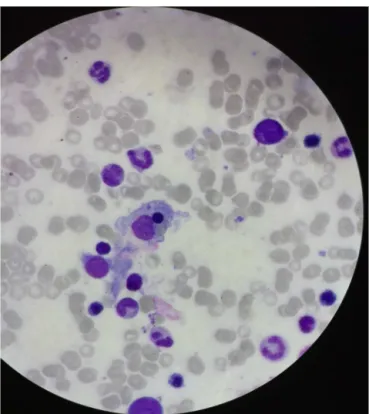
Fig.1–Hemophagocytosisinthebonemarrow.
Credit:Dr.PaulodoValRezende(DepartmentofPediatric
HematologyofHospitaldasClínicasofUniversidade FederaldeMinasGerais).
94×103/L), increasedserum ferritin levels (>1.000ng/mL), elevated triglycerides (445mg/dL) and reduced fibrinogen (96mg/mL).
Shedevelopedsepsisaftertheinitialtreatment,worsening herclinicaland laboratory condition.In additionto antibi-otics,intravenoushumanimmunoglobulin(IVIG)2g/kgwas administered,withnoimprovement.
After cytomegalovirus (CMV) and EBV serology results, the latter positive IgM and IgG, and a lumbar puncture, torule out central nervous system (CNS) involvement, we decidedinconjunctionwiththe Hematologyteam,tostart HLH-04 treatment protocol: dexamethasone, etoposide (VP 16), in addition to CSA, for eight weeks. After the fourth weekof treatment protocol, there was febrile neutropenia (total leukocyte count 0.87×103/L), and hair rarefaction, both complications that were already expected with this treatment.
Thediseaseremitted aftereightweeks.Herlast labora-toryassessmentshowednormalizationofferritin(270ng/mL), triglycerides (78mg/dL), hemoglobin (13.7g/dL), fibrinogen (250mg/mL),AST(23U/L)andALT(34U/L).Thepatientis cur-rentlytakingPDN5mg/dayandCSA6mg/kg/day.
Discussion
and
conclusion
The purpose of this case report is motivating rheuma-tologists to consider MAS when faced with patients with fever, hepatosplenomegaly, impairment of liver function and cytopenias, so treatment can be quickly initiated. It
is important to emphasize that the diagnosis of MAS is often a challenge as it may mimic a flare of the under-lying disease.There are no validated criteria fordiagnosis of MAS.6 Ravelli et al.2 proposed diagnostic guidelines
for MAS complicating SJIA, based on expert consensus. Clinical and laboratory findings that were more sensi-tive to MAS differentiation from flares of the underlying disease were selected. The most frequent findings were thrombocytopenia,hyperferritinemia,elevatedliverenzymes, leukopenia,bonemarrowhemophagocytosis,persistentfever, drop in the erythrocyte sedimentation rate, hypofibrino-genemia and hypertriglyceridemia.2 In our patient, the
presence of bleeding, daily and non-remitting fever, pan-cytopenia and reduced fibrinogen serum levels stood out, which led us to consider a diagnosis other than SJIA activation.
We consider that there was a combination of triggers. Immunosuppressionwithsyntheticandbiologicaldrugs, per-sistentdiseaseactivity,andEBVinfectionhascontributedtoa severeandlife-threateningdisease.TheSJIAtherapy,mainly MTXbutalsoETN,5,6 mighthavebeenthetrigger.Biological
drugshavebeendescribednotonlyasapossibletreatment forMAS,butalsoassyndrometriggeringfactors.6
Currently,the treatmentformacrophageactivation syn-dromeisbasedoncorticosteroidsandCSA.CSAhasproved effective inpatientswith severedisease and corticosteroid resistant,6,7 thatiswhyitwasintroducedearlyinthe
treat-ment.Humanintravenousimmunoglobulinisanalternative therapy,6,8 also ineffective inour patient. There are a few
reportsofeffectivenessofinterleukin-1antagonists, partic-ularlyanakinra9(unavailableinourcountry)inthosepatients
refractorytoconventionaltreatment.Sincethediseasewas refractorytotheinitialtherapy,wewere motivatedtolook forothercauses,likethepossibleassociationwithEBV infec-tion,consideredtobeoneofthemajoretiologicalagentsand responsibleforthemostseverecases.8,10,11Sowechosethe
treatmentguidedbytheHLH-04protocol.VP16isimportant, mainly,inrefractorycases,6,8,11–13andshouldbepromptly
ini-tiatedsinceitconfersthemostfavorableprognosisinthese situations.11
The HLH treatment protocol was proposed in 1994 and revisedin2004fortreatmentofprimaryandsecondaryforms, related to infections and malignancies. The specific infec-tioustreatmentappearstohavearesultincasesofvisceral leishmaniasis,cytomegalovirusandbacterialinfections,but thereisnobenefitdescribedindiseaseassociatedwithEBV infection.9,10Thetreatmentwasbasedonthedexamethasone
andVP16association,inaneight-weekinductionperiod.In caseofremission,treatmentshouldbesuspendedaftereight weeks.1,3,12 Otherwise, thesepatientsshould bereferredto
stemcelltransplantation.6,12
82
rev bras reumatol.2015;55(1):79–82Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RavelliA,Magni-ManzoniA,PistorioA,BesanaC,FotiT,
RupertoN,etal.Preliminarydiagnosticguidelinesfor
macrophageactivationsyndromecomplicatingsystemic
juvenileidiopathicarthritis.JPediatr.2005;146:
598–604.
2. DaviS,ConsolaroA,GuseinovaD,PistorioA,RupertoN,
MartiniA,etal.Aninternationalconsensussurveyof
diagnosticcriteriaformacrophageactivationsyndromein
systemicjuvenileidiopathicarthritis.JRheumatol.
2011;38:764–8.
3. DeaneS,SelmiC,TeuberSS,GershwinME.Macrophage
activationsyndromeinautoimmunedisease.IntArch
Immunol.2010;153:109–20.
4. CannaSW,BehrensEM.Notallhemophagocytesarecreated
equally:appreciatingtheheterogeneityofthe
hemophagocyticsyndromes.CurrOpinRheumatol.
2012;24:113–8.
5. FilhoAXC,CorreaFO,SchumanI.Síndromedeativac¸ão
macrofágicasecundáriaàinfecc¸ãoagudapelovírus
Epstein-Barr.RevBrasReumatol.2008;48:
179–83.
6.CassidyJT,PettyRE,LaxerRM,LindsleyCB.Textbookof
pediatricrheumatology:macrophageactivationsyndrome,
45,6thed.ElsevierSaunders;2011.p.674–81.
7.ParodiA,DaviS,PringeAB,PistorioA,RupertoN,
Magni-ManzoniS,etal.Macrophageactivationsyndromein
juvenilesystemiclupuserythematosus:amultinational
multicenterstudyofthirty-eightpatients.ArthrRheumat.
2009;60:3388–99.
8.WeitzmanS.Approachtohemophagocyticsyndromes.Am
SocHematol.2011;1:178–83.
9.MiettunenPM,NarendranA,JayanthanA,BehrensEM,Cron
RQ.Successfultreatmentofseverepaediatricrheumatic
disease-associatedmacrophageactivationsyndromewith
interleukin-1inhibitiontherapy:caseserieswith12patients.
Rheumatology.2011;50:417–9.
10.HenterJI,HorneAC,AricóM,EgelerRM,FilipovichAH,
ImashukuS,etal.ReviewHLH-2004:diagnosticand
therapeuticguidelinesforhemophagocytic
lymphohistiocytosis.PediatrBloodCancer.2007;48:124–31.
11.JordanMB,AllenCE,WeitzmanS,FilipovichAH,McClainKL.
HowItreathemophagocyticlymphohistiocytosis.Blood.
2011;118:4041–52.
12.ShiraishiA,OhgaS,DoiT,IshimuraM,TakimotoT,TakadaH,
etal.Treatmentchoiceofimmunotherapyorfurther
chemotherapyforEpstein–Barrvirus-associated
hemophagocyticlymphohistiocytosis.PediatrBloodCancer.
2011;59:265–70.
13.HenterJI,Samuelsson-HorneAC,AricóM,EgelerRM,Elinder
G,FilipovichAH,etal.Treatmentofhemophagocytic