REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Original
article
Consensus
of
the
Brazilian
Society
of
Rheumatology
for
the
diagnosis,
management
and
treatment
of
lupus
nephritis
Evandro
Mendes
Klumb
a,∗,
Clovis
Artur
Almeida
Silva
b,
Cristina
Costa
Duarte
Lanna
c,
Emilia
Inoue
Sato
d,
Eduardo
Ferreira
Borba
e,
João
Carlos
Tavares
Brenol
f,
Elisa
Martins
das
Neves
de
Albuquerque
a,
Odirlei
Andre
Monticielo
g,
Lilian
Tereza
Lavras
Costallat
h,
Luiz
Carlos
Latorre
i,
Maria
de
Fátima
Lobato
da
Cunha
Sauma
j,
Eloisa
Silva
Dutra
de
Oliveira
Bonfá
e,
Francinne
Machado
Ribeiro
aaDisciplineofRheumatology,FaculdadedeCiênciaMédicas,UniversidadedoEstadodoRiodeJaneiro,RiodeJaneiro,RJ,Brazil bDepartmentofPediatrics,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
cDepartmentoftheLocomotorSystem,FaculdadedeMedicina,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil dDisciplineofRheumatology,FaculdadedeMedicina,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil
eDisciplineofRheumatology,FaculdadedeMedicina,UniversidadedeSãoPaulo,SP,Brazil
fDepartmentofInternalMedicine,UniversidadeFederaldoRioGrandedoSul,PortoAlegre,RS,Brazil
gDisciplineofRheumatology,FaculdadedeMedicina,UniversidadeFederaldoRioGrandedoSul,PortoAlegre,RS,Brazil hDisciplineofRheumatology,FaculdadedeMedicina,UniversidadeEstadualdeCampinas,Campinas,SP,Brazil iServiceofRheumatology,HospitaldeHeliópolis,SãoPaulo,SP,Brazil
jDisciplineofRheumatology,FaculdadedeMedicina,UniversidadeFederaldoPará,Belém,PA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26August2014 Accepted14September2014 Availableonline16January2015
Keywords:
Systemiclupuserythematous Lupusnephritis
Therapeutics Brazil Consensus
a
b
s
t
r
a
c
t
Objective:Todeveloprecommendationsforthediagnosis,managementandtreatmentof lupusnephritisinBrazil.
Method:Extensiveliteraturereviewwithaselectionofpapersbasedonthestrengthof scien-tificevidenceandopinionoftheCommissiononSystemicLupusErythematosusmembers, BrazilianSocietyofRheumatology.
Resultsandconclusions:(1)Renalbiopsyshouldbeperformedwheneverpossibleandifthis procedureisindicated;and,whentheprocedureisnotpossible,thetreatmentshouldbe guidedwiththeinferenceofhistologicclass.(2)Ideally,measuresandprecautionsshouldbe implementedbeforestartingtreatment,withemphasisonattentiontotheriskofinfection. (3)Risksandbenefitsoftreatmentshouldbesharedwiththepatientandhis/herfamily.(4) Theuseofhydroxychloroquine(preferably)orchloroquinediphosphateisrecommendedfor allpatients(unlesscontraindicated)duringinductionandmaintenancephases.(5)The eval-uationoftheeffectivenessoftreatmentshouldbemadewithobjectivecriteriaofresponse (completeremission/partialremission/refractoriness).(6)Angiotensin-convertingenzyme inhibitorsand/orangiotensinreceptorblockersarerecommendedasantiproteinuricagents
∗ Correspondingauthor.
E-mail:[email protected](E.M.Klumb).
http://dx.doi.org/10.1016/j.rbre.2014.09.010
forall patients(unlesscontraindicated). (7)Theidentification ofclinicaland/or labora-torysignssuggestiveofproliferativeormembranousglomerulonephritisshouldindicate an immediate implementation of specific therapy, including corticosteroids and an immunosuppressive agent, even though histological confirmation is not possible. (8) Immunosuppressivesmustbeusedduringatleast36months,butthesemedicationscan bekeptforlongerperiods.Itsdiscontinuationshouldonlybedonewhenthepatientcould achieveandmaintainasustainedandcompleteremission.(9)Lupusnephritisshouldbe consideredasrefractorywhenafullorpartialremissionisnotachievedafter12months ofanappropriatetreatment,whenanewrenalbiopsyshouldbeconsideredtoassistin identifyingthecauseofrefractorinessandinthetherapeuticdecision.
©2014ElsevierEditoraLtda.Allrightsreserved.
Consenso
da
Sociedade
Brasileira
de
Reumatologia
para
o
diagnóstico,
manejo
e
tratamento
da
nefrite
lúpica
Palavras-chave:
Lúpuseritematososistêmico Nefritelúpica
Terapêutica Brasil Consenso
r
e
s
u
m
o
Objetivo:Elaborarrecomendac¸õesparaodiagnóstico,manejoetratamentodanefritelúpica noBrasil.
Método:Revisãoextensadaliteraturacomselec¸ãodosartigoscombasenaforc¸adeevidência científicaeopiniãodosmembrosdaComissãodeLúpusEritematosoSistêmicodaSociedade BrasileiradeReumatologia.
Resultados econclusões: 1)A biópsiarenal deveserfeitasemprequepossível ehouver indicac¸ãoequandonãoforpossível,otratamentodeveserorientadocombasena infer-ênciadaclassehistológica.2)Devemserimplementadosmedidasecuidadosidealmente antesdoiníciodotratamento,comênfasenaatenc¸ãoaoriscodeinfecc¸ão.3)Devem-se compartilharriscosebenefíciosdotratamentocomospacientesefamiliares.4)Ouso dahidroxicloroquina(preferencialmente)oudifosfatodecloroquinaérecomendadopara todosospacientes(excetocontraindicac¸ão)duranteasfasesdeinduc¸ãoemanutenc¸ão. 5)Aavaliac¸ãodaeficáciadotratamentodeveserfeitacomcritériosobjetivosderesposta (remissãocompleta/remissãoparcial/refratariedade).6)Osinibidoresdaenzimaconversora daangiotensinaoubloqueadoresdosreceptoresdaangiotensinasãorecomendadoscomo antiproteinúricosparatodosospacientes(excetocontraindicac¸ão).7)Aidentificac¸ãode sinaisclínicose/oulaboratoriaissugestivosdeGNproliferativaoumembranosadeveindicar inícioimediatodeterapiaespecíficaincluindocorticosteroideseagenteimunossupressor, mesmoquenãosejapossívelcomprovac¸ãohistológica.8)Otempodeusodos imunossu-pressoresdevesernomínimode36meses,maselespodemsermantidosporperíodosmais longos.Asuasuspensãosódeveserfeitaquandoopacienteatingiremantiverremissão completasustentada.9)Deve-seconsiderarNLrefratáriaquandoaremissãocompletaou parcialnãoforalcanc¸adaapós12mesesdetratamentoadequado,quandoumanova bióp-siarenaldeveserconsideradaparaauxiliarnaidentificac¸ãodacausadarefratariedadee decisãoterapêutica.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Systemiclupuserythematosus(SLE)isachronicautoimmune inflammatorydiseasewhichethiopathogenesisinvolves mul-tiplegenesandhormonalandenvironmentalfactors.SLEis a pleomorphicdisease withwide phenotypic variability of presentation, severity and clinical course, usually progres-sing with periods ofactivity and remission. Mostpatients exhibitarelativelybenigncourse,butoverallsurvivalislower, whencomparedtothegeneralpopulation,witha standard-ized mortality ratio from 2.4 to 6.4.1 The main causes of deathare infection,diseaseactivity,cardiovasculardisease,
Therenal involvementin SLEoccurs clinically inabout 60%ofpatientsandcandeterminetubular,interstitial, vas-cular and glomerular changes; but is the involvement of the lattercompartmentthat determines mostofthe signs andsymptomsoflupusnephritis(LN)(B).12 Similarlytothe demonstrations in other systems, LN also shows different degreesofseverity, with periodsofactivity and remission, whichdeterminethechoiceoftherapeuticagentstobeused (B).13Inclinicalpractice,itisnotalwayspossibletoperform akidneybiopsy,althoughthisisarelativelysimpleprocedure whenperformedbyexperiencedprofessionals.14Thebiopsy allowstherecognitionofdiagnosticandprognosticmarkers thatmayinfluencethetherapeuticchoice.For patientsnot undergoingakidneybiopsyandforallpatientsinthecourse ofevolution,clinicalandlaboratorymarkersthathelp charac-terizetheseverityandactivityofGNareused(B),15guiding theuse ofimmunomodulatory and/orimmunosuppressant agents.
Themaingoalofthetreatmentistoachieveacomplete remission (CR),which isassociated witha good long-term prognosis.11,16However,despitecurrenttherapeuticregimens, lessthan50%ofpatientswithLNachieveCRafterthefirst6 monthsoftreatment(B).17–19
Thisconsensusaimstopresent themain recommenda-tionsfortheclinicalmanagementofLN,involvingdiagnosis, prognosis,treatment(inductionandmaintenance),care dur-ingtheuseofpharmacologicalagents, immunosuppression-adjuvanttherapy,refractorycaseapproachesand identifica-tion of associated comorbidities, all contextualized to the realityofourcountry.
Materials
and
methods
Thisconsensuswasdevelopedafterasystematicreviewof theliterature,inassociationwiththeopinionof13 rheuma-tologists with clinical experience in LN, 11 of them being membersoftheSLECommissionofSBR,besidestwoguests (CAAS andEMNA). Thesystematicreviewofthe literature, includingthepriorselectionofanumberofissuespreviously identified by the working group and the voting of recom-mendations,wasperformedaccordingtoamodifiedDelphi method.ThedatabasesincludedMEDLINE, SciELO,PubMed andEMBASEuntilNovember2013.Afterconsiderationofthe data obtained in the literature, the participants expressed theiropiniononeachtopicindiscussionsviaInternet,and votedonrecommendationsconfidentially.Votingoccurredin face-to-facemeetingsheldinMayandJuly2014ina hierar-chicalmanner, accordingtothefollowingalternatives:(a)I completelyagree;(b)Iagreewithsomereservation;(c)Iagree withmanyreservations;(d)Irejectwithreservations;(e)I com-pletelyreject.Incasesofnon-agreementofatleast70% of theparticipants(foroptionsa,borc),newdiscussionswere held,followedbyadjustmentsfortherecommendationand anewroundofvoting,untilthisminimumpercentagewas reached.Foreachrecommendation,thepercentagesof agree-mentamongtheparticipantswereinformed.Whenpossible, thelevelsofevidencewereexpressedaccordingtotheOxford classification:
A–Experimentalorobservationalstudiesofgreater consis-tency.
B–Experimentalorobservationalstudiesoflower consis-tency.
C–Casereports(non-controlledstudies).
D– Opinionwithoutcritical evaluation,basedon consen-suses,physiologicalstudiesoranimalmodels.
Renalbiopsy
Recently, the ACR (American College of Rheumatology)20 and the EULAR (European LeagueAgainstRheumatism), in combinationwithtwoEuropeangroupsofNephrology (Euro-peanRenalAssociation –EuropeanDialysisand Transplant Association)21 publishedrecommendationsforthe manage-ment of SLE patients with renal involvement, based on histologicalfindings.
Arenalbiopsyshouldbeperformedwheneverpossible,20,21 considering that clinical, immunological and laboratory parametersarenotpredictorsofthehistologicalfindings.20–22 Thisproceduremaybetterguidethetreatmentandprognosis, andshouldalwaysbeperformedbyexperiencedandqualified professionals.23
EULAR recommends obtaining a renal biopsy whenever thereisanysignofrenalinvolvement,especiallyproteinuria ≥0.5g/24h accompanied by glomerular dysmorphic hema-turia and/orcellularcasts(C).21 ACRrecommendsa biopsy (unlessstronglycontraindicated)whenevertherearesignsof renalinvolvementwithanelevatedserumcreatininewithno apparentcause(notrelatedtoSLE),proteinuria≥1.0g/24hor anisolatedproteinuria≥0.5g/24hassociatedwithhematuria and/orcellularcasts(C).20WhenGFR<30mL/min,thedecision toobtainabiopsyshouldtakeintoconsiderationthenormal kidneysize(>9cm)and/orevidenceofactiverenaldisease.21
ThehistologicalpatternofLNshouldfollowthenew defi-nitions,revisedbyinternationalsocietiesofnephrologyand pathology,24,25 knownasthe classificationoflupus nephri-tisoftheInternationalSocietyofNephrology/RenalPathology Society2003(ISN/RPS2003)(C)(Table1).Accordingtothese guidelines,glomeruliandthetubulointerstitialregionshould be evaluated, with descriptions of activity and chronicity, besides the vascular component that is usuallyassociated withantiphospholipidantibodysyndrome(APS)(C).20,21,24,25A sampleisconsideredadequateifithasmorethan8glomeruli, and immunofluorescence or immunohistochemistry is rec-ommended to identify complement and immunoglobulin deposits.Ifpossible,electronmicroscopyshouldalsobe per-formed,becausethisexaminationfacilitatestheevaluationof proliferativeandmembranouslesions(C).21,24,25
Usuallythereisnoneedforarepeatbiopsy inthecase ofnewoutbreaksofrenalactivity26,27becausethisprocedure doesnotprovideadditionalinformationaboutrenaloutcomes in the long term.28 However,in patientswithout adequate responsetotreatment, repeatbiopsymayhelpinthe iden-tification ofthe cause ofrefractoriness20,21,29 and assist in therapeuticdecision.21,29
Table1–ClassificationoftheInternationalSocietyofNephrology/RenalPathologySociety2003forlupusnephritis.
ClassI–minimalmesangialLN
Normalglomeruliunderlightmicroscopy(LM),butwithimmunedepositsunderimmunofluorescence(IF).
ClassII–proliferativemesangialLN
PuremesangialhypercellularityofanydegreeormesangialmatrixexpansionunderMOwithimmunedepositsinthemesangium.Theremay befewandisolatedsubepithelialorsubendothelialdepositsvisibleunderIForelectronmicroscopy(EM),butnotunderOM.
ClassIII–focalLN
Activeorinactive,focal,segmentalorglobal,endo-andextracapillaryglomerulonephritis(GN)involving<50%ofallglomeruli,typicallywith subendothelialimmunedeposits,withorwithoutmesangialalterations.Itisfurtherclassifiedinto:A,active;A/C,active/chronic;C,inactive chronic.
ClassIV–diffuseLN
Activeorinactive,segmentalorglobal,endoandextracapillaryglomerulonephritis(GN)involving≥50%ofallglomeruli,typicallywith subendothelialimmunedeposits,withorwithoutmesangialalterations.Itisdividedintosegmentaldiffuse(IV-S),inwhich≥50%of glomeruliinvolvedpresentsegmentallesions(involvinglessthanhalfofthetuft)andintoglobaldiffuse(IV-G),inwhich≥50%ofglomeruli involvedhavegloballesions(involvingmorethanhalfofthetuft).Thisclassincludescaseswithdiffusewire-loopdepositswithlittleorno glomerularproliferation.Itisfurtherclassifiedinto:A,active;A/C,active/chronic;C,inactivechronic.
ClassV–membranousLN
GlobalandsegmentalsubepithelialimmunedepositsoritsmorphologicalsequelaeunderOMandIForEM,withorwithoutmesangialchanges. MayoccurincombinationwithclassIIIorIV.
ClassVI–advancedsclerosis
Globalglomerularsclerosisin≥90%,withnoresidualactivity.
AdaptedfromWeeningetal.,2004.24,25
AB,antibody;GN,glomerulonephritis;IF,immunofluorescence;EM,electronmicroscopy;OM,opticalmicroscopy;LN,lupusnephritis.
proteinuria ≥0.5g/24hassociated withglomerular dysmor-phichematuriaand/orthepresenceofcellularcasts.These changesmustbeconfirmedinasecondbiopsy(Table2).
EvaluationofLNwithoutrenalbiopsy:inferenceof histologicalclassforatherapeuticdecisionand progressionassessment
InmostcasesofNL, clinical,serologicandlaboratory tests cannotaccuratelypredictthehistologicalfindings,norcould theydifferentiateotherpossiblecausesofrenaldisease.20–22 However,thisdatasetcanbeveryusefulintheclinical moni-toringofnephritisand,inparticular,assistinginthediagnosis ofrenaldiseaseactivity.30
Theactiveurinary sediment,definedbythepresenceof hematuria (witha dysmorphic glomerularpattern), leuko-cyturiaand presenceofcellularcasts, isadmittedlyoneof the most important parameters for characterization of an activeglomerulonephritis. Proteinuria,measured in24hor inferredbytherelationshipproteinuria/creatininuria(RP/C) ina random spot urine sample, may alsoindicate inflam-matory activity.30,31 The positivity or increase in titers of anti-dsDNAantibodiesandlowbloodlevelsofcomplement, especiallywithlowlevelsofC3,arealsoconsideredasan evi-denceofrenalinvolvement,buttheseindicatorsshouldnotbe usedinisolationtodefinethiscondition.30Thereductionin glomerularfiltration,nephroticproteinuriaandthepresence ofhypertension(HBP)suggest greater severityandaworse prognosis.32,33
InpatientswithAPSassociatedwithSLE,thepresenceof HBPandrenaldysfunctionshouldbeconsideredasanalert tothepossibilityofavasculopathyassociatedwith antiphos-pholipidantibodies(aPl),especiallywhentherearenosigns ofGNdetectedinurinarysediment.34
Inrecentyears,severalnewnoninvasiveurinary biomark-ers were described, including lidocalin-type prostaglandin D synthase(l-PGDS),␣(1)-acid glycoprotein(AAG),
transfer-rin(TF),ceruloplasmin(CP),neutrophilgelatinase-associated lipocalin(NGAL)andmonocytechemotacticprotein1 (MCP-1).35 Thecombination ofthese biomarkerswith laboratory parametersofrenalfunctionispromisingtohistologicclass inference and toquantifyactivity and chronicity(B).35 The anti-ribosomalPantibody,intheabsenceofanti-dsDNA,has alsobeendescribedaspossiblyassociatedwithmembranous nephritisinSLEpatients,andwithapredictivevalueofbetter renalprognosis(B).36,37
Table2–SBRrecommendationsforlupusnephritismanagement.
Recommendations Agreement
Indicationsforrenalbiopsy
Performarenalbiopsywheneverpossibleandwhenindicated. a)1.0 ElevationofserumcreatininewithnoapparentcauseandpotentiallyassociatedwithSLE. a)1.0 Isolatedproteinuria>1.0g/24h(orRP/C>1.0). a)1.0 Proteinuria≥ 0.5g/24hassociatedwithglomerulardysmorphichematuriaand/orcellularcasts. a)1.0 Note:changesmustbeconfirmedwithasecondtest. a)1.0
Inferenceofhistologicalclass
Possibilitytomakesomeinferencebasedonclinicalandlaboratorycriteria. a)0.54;b)0.46
Creatinineelevation(withnoothercause)associatedwithproteinuria>0.5g/24horRP/C>0.5andrecentHBP and/oractiveurinarysediment:considerasproliferativeGN(classIIIorIV),especiallyifaccompaniedbylow bloodlevelsofcomplementandanti-ds-DNAAB.
a)0.9;b)0.1
Proteinuria>2g/horRP/C>2,withnoactivityinurinarysedimentorhypertension,andmostlywithout anti-ds-DNAABandnormalcomplementlevels,suggestiveofmembranousGN(classV).However,wecannot excludeproliferativelesion.
a)0.9;b)0.1
Proteinuria<1g/24horRP/C<1withnormalcreatinineandwithoutHBPsuggestsmesangialGN(classII). However,wecannotexcludeinitial-stageproliferativeormembranousGN.
a)1.0
AlsoconsiderthepossibilityofothercausesofrenalinjuryatallstagesofevolutionofLN(APSN,renalvein thrombosis,TIN,ATN,diabeticnephropathy,hypertensivenephropathyand/ornephropathysecondaryto infection).
Careforimmunosuppressedpatients
Vaccineupdate. a)1.0
Avoidlivevirusvaccines. a)1.0
Tuberculosis(latentordisease)screening. a)1.0
Continuousevaluationforinfectionsthroughouttheperiodofimmunosuppression. a)1.0 Sharerisksandbenefitsoftreatmentwithpatientandhis/herfamily. a)1.0 Guidanceoncontraception(avoidingestrogens),andrisksofpregnancyduringtreatment. a)1.0
Empiricalantiparasitictreatment. a)1.0
ConsiderprophylaxisforPneumocystisjiroveciiincasesofpreviousinfectionorinpatientswithlymphopenia <500mm3.
a)1.0
Prescribehydroxychloroquineforpatients,unlesscontraindicated. a)1.0 Obtainaninformedandfreeconsentform(IFCF). a)1.0
Responsecriteria
Thetreatmentefficacyevaluationshouldbemadewithobjectivecriteriaofresponse. a)1.0 Completeremission:proteinuria<0.5g/24horRP/C<0.5andnormalGFR;orreduction≤10%ofpreviousvalue
forthepatientorULNofmethod(ifthefirstisnotavailable)andanormalurinalysis.
a)1.0
Partialremission:reduction>50%ofinitialproteinuriawithavalue<3.0g/24horRP/C<3.0,normalGFRor reduction≤10%ofthepreviousvalueofthepatient,orULNofmethod(ifthefirstisnotavailable)anda normalurinalysis.
a)0.9;b)0.1
Agreement:thenumbersineachrecommendationexpressthepercentagesofagreementamongthemembers,accordingtotheclassification used.
AB,antibody;GN,glomerulonephritis;HBP,systemicarterialhypertension;ULN,upperlimitofnormal;APSN,nephropathyofantiphospholipid syndrome;ATN,acutetubularnecrosis;TIN,tubulointerstitialnephritis;RP/C,ratioproteinuria/creatininuriainarandomurinesample;GFR, glomerularfiltrationrate.
Forthe purposeofanalyzingtheresponsetotreatment, weestablishedcriteriathataresimilartothoseadoptedby EULAR21andACR.38Completeremission(CR)wasdefinedas aproteinuria<0.5g/24horRP/C<0.5,andnormalorreduced GFR<10%ofthepreviousvalueofthepatientoroftheupper limitofnormal(ULN)forthemethod(ifthefirstoptionisnot available)andanormalurinalysis.Partialremission(PR)was definedasareductionof>50%oftheinitialproteinuria,with avalue<3.0g/24horRP/C<3.0,andanormalGFRora reduc-tionof<10%ofthepreviousvalueorofULNforthemethod (ifthefirst optionisnotavailable)and anormalurinalysis (Table2).
Careforimmunosuppressedpatients
are: leukopenia/lymphopenia, low blood levels of comple-ment,hypogammaglobulinemia,splenectomy,andtheuseof CSandimmunosuppressants,42usualconditionsduringthe wholetreatmentofLN,sothatacontinuousassessmentmust bemadeforthepresenceofinfectionthroughouttheperiod ofimmunosuppression.
On the other hand, it was demonstrated that the use of hydroxychloroquine (HCLQ) is associated with a lower frequencyofinfectionsinpatientswithSLE.43Duetothe mor-bidityandmortalityrelatedtoinfections,thesharingofrisks andbenefitsoftreatmentwiththepatientandhis/herfamily isstronglysugested,aswellasprovidingspecificclarification onthe medicationsused, includingsigningofanInformed ConsentForm.
Allpatientsshouldalsobecounseledaboutcontraception andpregnancyrisksduringtreatment(Table2).
Vaccination
An update of the vaccination card should always be per-formed, preferably with the disease in an inactive period andbeforethe implementationofanysyntheticor biologi-calimmunosuppressivetherapy.44,45 Vaccineswithoutliving organism–(influenzaIM);pneumococcal;tetanus; diphthe-ria;pertussis;HaemophilustypeB;viral hepatitisAand B, poliomyelitis(inactivated–IPV);meningococcal;HPV;typhoid fever(IM);andrabies–aresafeatanystageoftreatmentand oftendetermineanadequateimmunogenicity.46,47Inthis con-text,themostimportantvaccinesare:
(a) Pneumococcal(23-valentpolysaccharide):mustbe admin-isteredeveryfiveyears48asrecommendedbythePrograma Nacional de Imunizac¸ões (PNI) (National Immunization Program) of Brazil. However, the Sociedade Brasileira de Imunizac¸ão(SBIM)(BrazilianSociety ofImmunization)in agreement with the Centers forDisease Control ofthe UnitedStates,hasrecommendedthatthevaccineusedin immunosuppressedindividualsmustbethe pneumococ-calconjugatevaccine,followedbypolysaccharidevaccine after8weeks(CDC,2011);
(b) Influenza:thevaccinemustbeadministeredannually49; (c) Diphtheriaandtetanus(dT):followPNIguidelines.
Thelivevirus vaccines (MMR, herpeszoster andyellow fever)shouldbeavoidedandusedonlyinspecialcases,after ajointevaluationwithaninfectologist(Table2).42
Antimicrobial
prophylaxis
(a) Tuberculosis:thetreatmentoflatenttuberculosis, espe-ciallyinthecaseofpositiveepidemiologicaldata,should beconsideredincaseswithtuberculintest–PPD≥5mm (ifthepatientisusingCS)orwithachestradiograph sug-gestiveofprioruntreatedtuberculosis.50
(b) Pneumocystisjirovecii:indicationofprophylaxisbeforethe onsetofimmunosuppressionincasesofprevious infec-tionbythisorganismandinpatientswithlymphopenia
<500mm3, especially if associated with a genetic or acquiredhypocomplementemia.51
(c) Antiparasitic agents: before immunosuppression, an empiric treatment with broad spectrum anthelmintics (e.g.,albendazoleor ivermectin)is recommended, espe-ciallyinpatientswithpositiveepidemiologicaldata–an almostuniversalconditioninourcountry(Table2).
Mesangial
glomerulonephritis
(classes
I
and
II)
–
induction
and
maintenance
therapy
FormostpatientswithmesangialGN,thetreatmentisoffered only with CS and HCLQ. However, for those patients who experience persistentproteinuria>1.0g/24h(orRP/C>1.0), onemustconsiderthecombinationofazathioprine(AZA)or mycophenolatemofetil(MMF)(Table3).
Proliferative
glomerulonephritis
–
remission
induction
therapy
Better-qualityrandomizedcontrolledstudiesevaluating dif-ferenttreatmentregimensinLNhadasinclusioncriteriathe confirmationandclassificationofnephritisaccordingtorenal biopsy.Thisapproachhastheadvantageofavoidingan aggres-sive treatmentformild cases,withnoindicativefactorsof severity, aswell astheimplementationofineffective treat-mentsinpatientswithchronicandirreversiblechanges.Itis recognizedthatthetreatmentisurgentanditmustbe inten-sive inproliferativeformsofLN(classesIII andIV, withor without associationwithclassV),inwhichtheriskof pro-gressiontorenalfailureishigh.21Thetargettobeachievedin sixmonths(inductionperiod)isCR.
Since studies published in the 80s, the superiority of cyclophosphamide(CY)hasbeenacknowledged,ascompared totheisolateduseofCSinthetreatmentofPGN.52Theuseof CYforprolongedperiodswasmoreeffectiveforthe preven-tionofrelapseandformaintainingrenalfunction53;however, thisdrugisassociatedwithmultiplesideeffects,particularly gonadalinsufficiency.54
Inacontrolled,randomized,multicentrestudyonLN(class III/IVandV[16%]),theeffectivenessofMMFwasnotinferior tointravenous(IV)CYinaconventionalscheme,55confirming earlierstudies.56,57 Meta-analysesalsoshowedthatCYand MMFhavecomparableefficacy(A).58–60
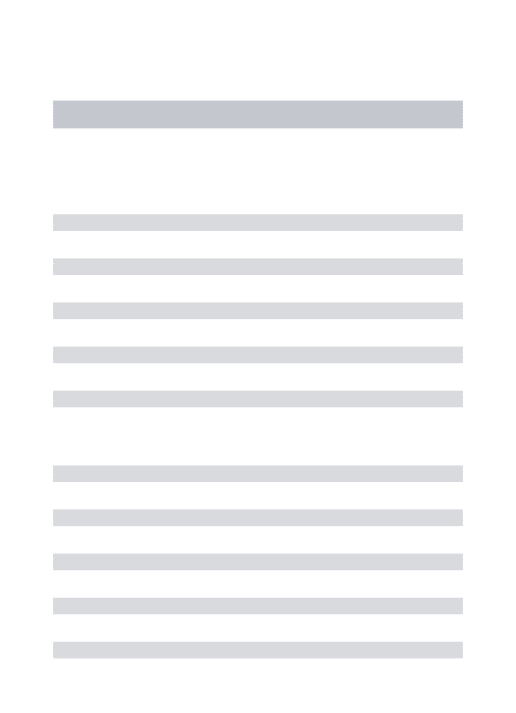
Table3–SBRrecommendationsforthetreatmentoflupusnephritisincludingproliferativeandmesangialtypes.
Recommendations Agreement
Adjuvantmeasuresforallhistologicclasses
Theuseofhydroxychloroquine(preferably)orchloroquineisrecommendedforallpatients(unless contraindicated)duringinductionandmaintenancephases.
a)1.0
ACEinhibitorsand/orARBsarerecommendedasantiproteinuricagentsforallpatients(unless contraindicated).
a)1.0
Preventandtreatriskfactorsforcardiovasculardisease:physicalinactivity,dyslipidemia(LDL<100mg/dL), diabetes,obesity,HBP(BP<130 × 80mmHg)andsmoking.
a)1.0
Encourageadietrichincalciumandconsidersupplementation,whennecessary. a)1.0 ConsidersupplementationofvitaminD(25(OH)(ifvitaminDserumlevels>30ng/mL). a)1.0 Avoidnephrotoxicdrugs,especiallynon-steroidalanti-inflammatoryagents. a)1.0
ProtocolforinductionandmaintenanceinmesangialGN(classesIandII)
Forpatientswithpersistentproteinuria≥1.0g/24horRP/C≥1.0:inductionandmaintenanceofremission, considerAZAorMMF.
a)1.0
ProtocolforinductioninproliferativeGN(classesIIIandIV)
TargettobeachievedinsixmonthsisRC. a)1.0
Theidentificationofclinicaland/orlaboratorysignssuggestiveofproliferativeGNshouldindicatean immediatespecifictherapy,includingCSandanimmunosuppressantagent,evenincaseswhenhistological confirmationisnotpossible.
a)1.0
ThetreatmentshouldbeginwithMPpulsetherapy[0.5–1.0gIV(or10–30mg/kg/dayinPSLEpatients)for3 days].Dosesofprednisonebetween0.5and1.0mg/kg/dayfor3–4weeks,withsubsequentreductionandwith thegoalofachievingadoseof5–10mg/dayfor6months.
a)0.9;b)0.1
InconjunctionwithCS,includeCYIV0.5–1.0g/m2BSAmonthlyfor6months,orCYIV0.5gevery15daysfor3 months,orMMF(2–3g/day).
a)0.9;b)0.1
Inpatientswithseveritycriteria,considerCYasafirstoption,takingintoaccountitsavailability,absorption andtolerancetomedicationandtreatmentadherence.
a)0.9;b)0.1
Lackofresponseorworseningofrenaldiseaseafter3monthsofanappropriatetherapysuggeststheneedto consideranearlychangeoftheinductionprotocol.
a)1.0
After6monthsoftreatmentatthisstage,ifCRorPRwerenotachieved,thepatientshouldbeconsideredas refractorytoinduction;inthiscase,anewtherapywithMPandreplacementofCYbyMMF,orofMMFbyCY, arerecommended.
a)1.0
ProtocolformaintainingproliferativeGN(classesIIIandIV)
AZAorMMFareindicatedforpatientswhohaveachievedCRorPRintheinductionphase. a)1.0 Thesemedicationsmustbeusedforatleast36months,buttheycanbekeptforlongerperiods.Their
suspensionshouldonlybeperformedafterachievingandmaintainingacompleteandcontinuousremission.
a)1.0
Thedosesofcorticosteroidsshouldbereducedprogressivelyand,ifpossible,discontinued,ideallyafter achievingandmaintainingacompleteandsustainedremission.
a)0.9;b)0.1
Agreement:thenumbersineachrecommendationexpressthepercentagesofagreementamongthemembers,accordingtotheclassification used.
AZA,azathioprine;ARB,angiotensinreceptorblockers;ACEI,angiotensin-convertingenzymeinhibitors;CY,cyclophosphamide;CS, cortico-steroids;GN,glomerulonephritis;HBP,systemicarterialhypertension;MMF,mycophenolatemofetil;MP,methylprednisolone;CR,complete remission;PR,partialremission;RP/C,proteinuria/creatininuriaratioinarandomurinesample;BSA,bodysurfacearea;GFR,glomerular filtrationrate.
oftenrandomizedcontrolledtrialsfoundthatlowdosesof CY,whencomparedtohigherdoses,hadsimilarefficacyin reducingrelapses,butwithlowerinfectionrates(A).62
The use of CY PO was evaluated retrospectively in a seriesofpatientswithLN(classIII,IVand V).Thedose of 1.0–1.5mg/kg/dayforanaverageuseof4monthswaseffective incontrollingLN,withfrequencyofsideeffectsandtheneed fordiscontinuationofthemedicamentoccurringinlessthan 10%ofthepatients,withoutdifferenceinresponsebetween Euro-andAfricandescendants.63Previousstudieshaveshown efficacyofCYPOinChinesepatients, comparabletoCYIV (C).64.65
InasubgroupexploratoryanalysisofALMSstudy,itwas observedthatalthoughCYandMMFIVhavepresentedsimilar efficacy,race,ethnicity,andgeographicregionfactorsseemto
haveinfluencedtheresponsetotreatmentofLN.Groupsof AfricanAmericanandHispanicpatientsappeartohavehad abetterresponsetoMMFversusCY,andAsianpatientshad moresideeffectstoMMF.But,asthiswasasubgroupanalysis, theseresultscannotbeconsideredconclusive(C).66
therearevirtually nostudiesdesignedtoevaluatethe effi-cacyofMMFinthesepatientswithseverelyimpairedrenal function.
TheuseofAZAasinductiontherapyinPGNisnot recom-mended,becausestudiesshowedlesseffectivenessversusCY inthisphaseoftreatment.52,69Onestudywithrepeatedrenal biopsyalsoshowedthatAZAwaslesseffectiveinpreventing theevolutiontoglomerularfibrosis.69However,AZAmaybe atherapeuticoptioninLNforEuro-descendantswithout pre-dictorsofseverityandwhodonottolerateCYorMMF,despite thehigherriskofnephritisreactivationwhencomparingthis agenttoCY(C).69
InwomenwithLNwhostillwishtobecomepregnant,it isrecommendedpreferablytheuseofMMF,asCYis associ-atedwithanincreasedriskofinfertility,particularlyinthose womenover30years andthathad aprolongeduse ofthis agent(approximaterisk:60%).However,MMFisformally con-traindicatedduringpregnancybecauseitsteratogenicity;and itmustbeemphasizedtheneedforaneffectivecontraception duringitsuse.TheuseofCYforshorterperiods(6months)in youngwomen,evenathighdoses,isassociatedwithlower ratesofinfertility (4.3–10%),7,54 apercentagesimilar tothe Eurotrialscheme (4.5%).7 Giventhe greater number ofside effectswithMMFuseinAsians,doses≤2g/dayare recom-mendedinthesepatients.Giventhatsomestudiesshowed aworseresponseofCYinAfrican-descendantandHispanic patients, it maybe advantageousthe use ofMMFin these cases.However,weshouldpointoutthatastudyspecifically targetedtotheBrazilianpopulationwiththeuseofthisagent hasnotyetbeenpublished(Table3).
Corticosteroids
AlthoughinmoststudiesCSwereadministeredPOatdoses of0.5–1mg/kg/daywithgradualreduction,pulsetherapyIV withMPforthreedaysatthebeginningoftreatmentcould allowthesubsequentuseoflowerdosesofCSPO,asshown byHoussiau.70Inordertoreducethesideeffectsofhighdoses ofCS,andalsotoallowamorerapidcontrolofthe inflam-matoryprocess,the useofMPatadose of0.5–1.0g/dayIV (or10–30mg/kg/dayforpediatricpatients)for3daysis rec-ommended,keepingtheprednisonedosein0.5–1.0mg/kg/day for3–4weeks,followedbyaprogressivereduction,aimingto achievedosesof5–10mg/dayaftersixmonths.Some extra-renalmanifestationsmayrequiremaintaininghigherdoses forlongerperiods,butduetothehighfrequencyofadverse effectsofCS,everyeffortshouldbemadeforreducingthedaily dose.Patientswithworseprognosisfactors,e.g.,presenceof cellularcrescentsandofnecrosis,aswellasthosewithhigher creatininelevels,shouldreceivehigherdosesofprednisone (1.0mg/kg/day).20
InthecaseofachievingonlyPRafter6monthsofan appro-priatetreatment,theinductionphasemaybeextendedfrom 7to9months,accordingtoclinicaljudgment.
After six months of induction treatment, if CR or PR has not been achieved, the patient is considered with refractory LN and a new induction therapy with MP and replacementofCYbyMMForMMFbyCYisrecommended (Table3).
Proliferative
glomerulonephritis
–
maintenance
treatment
Although thereis noevidence toestablish the duration of theinductionphase,mostauthorsandinternational consen-susesconsidertheperiodofsixmonths.20,71Atthesametime, changing the therapeuticregimenfor thatof maintenance phasedependsonCRorPRachievement.Insomeinstances, evenafterthefirstsixmonthsofinduction,asecondscheme willberequireduntilCRorPRisreached.Controlled stud-ies thathaveaddressedthe durationofthisphasearealso lacking, but most authors agree that it should last 24–48 months.ForpatientswithPGN,therearetwomajor acknowl-edged alternatives for patient maintenance: AZA or MMF, bothassociatedwithlow-doseprednisone(5–10mg/day).The maintenancewithCYIVevery3–4monthshasnotbeenused anymore,duetoitssideeffectsandalsobecausetheavailable options(AZAorMMF)haveprovenreasonablysafe,withfew sideeffectsinthelongterm.
Thesetwoimmunosuppressiveagentswerecomparedin two studies, MAINTAIN72 and Aspreva Lupus Management Study–ALMS.71Thedesignsofthesestudiesweredifferent anddidnotshowthesameoutcomes.TheMAINTAINstudy includedEuropeanCaucasianpatientsanddidnotshow sig-nificant differencesbetweendrugs.On theother hand,the ALMSstudy,whichselectedonlypatientswhohadachieved goodresponsesintheinductionphasewithCYIVorMMFfor sixmonthsandthatoccurredinlittlemorethan50%ofthose patientsincluded,showedsuperiorityofMMFversusAZAin preventingnewepisodesofrenalactivity.
EULARrecommendsthatpatientswithgoodresponsesto induction therapyforLN shoulduse MMF(2g/day)or AZA (2mg/kg/day)foratleastthreeyears,whileotherauthors rec-ommendatleastfiveyears,withdiscontinuationofthedrugin averygradualmannerandundermonitoring.73,74The discon-tinuationofthismedicationshouldbegradualandinitiated alwaysbyCS.21
ACR also recommends that patients who responded to inductiontherapyhaveamaintenancetreatmentwithAZA 2mg/kg/dayorMMF2g/day,combinedwithlowdosesofCS. According toACR,the existing dataare insufficientto rec-ommend the timeto dose reduction or discontinuationof medication(A).20
Insummary,inthemaintenancetherapyofpatientswith PGNwithcompleteorpartialresponseintheinductionphase, theyshouldbetreatedwithAZAorMMF,andthechoiceshould beevaluatedcasebycase.Mycophenolatesodiummayalsobe anoptiontomycophenolatemofetil,ifthereisintoleranceto thislatterdrug.
Facing the possibility of pregnancy, it is preferable to administerAZA,consideringtheteratogenicityofMMF.Dueto thehighcostofMMFandthefavorableresultsforthosemilder formsofLN,patientswithoutmarkersofseverityofLNand whohavehadacompleteresponsecanbetreatedwithAZA asfirstchoiceintheirmaintenancephase.
Membranous
glomerulonephritis
–
induction
treatment
MembranousGN(MGN)ispresentin10–20%ofcases under-goingbiopsy.Thisdiseasecanoccuraloneorinassociation withotherhistologicalclasses.76TheusualexpressionofMGN isthepresenceofproteinuriaandedemawithout concomi-tantsystemicmanifestations,complement consumptionor presenceofanti-ds-DNA(D).77theclassicfeaturesofGN,as hematuria(dysmorphic), cellular casts, HBP and early ele-vation of serum creatinine, are infrequent. As with other classes,MGNcanalsoprogressfroma“silent”type,including aslightlyelevatedproteinuria.78Ontheotherhand,nephrotic syndrome(NS)occursinupto75%ofpatients,79 represent-ing a greater risk of venous thrombosis(3–22%), including renalveins(astillgreaterriskinpatientswithaPl),80,81 coro-naryarterydisease(RR=2.8)andacutemyocardialinfarction (RR=5.5).82TheassociationofMGNwithproliferativeforms determinesaworse prognosisand,even inisolatedforms, 7–53%ofpatientsprogresstoERFin10years(C).80,82Thus, itisunderstoodthatdespiteMGNnotbeingthemost aggres-sivehistologicalclassinLNpatients,weshouldnotconsider itasamildformofrenalinvolvement.
Nonetheless, there are few studies available in the lit-erature, and most of them evaluating small series, with short periods of observation and varied treatment regi-menswithrespectto doses ofCS, concomitant use ofMP, use of angiotensin-converting enzyme inhibitors (ACEI) or angiotensinreceptorblockers(ARBs)andespeciallywith het-erogeneityofresponsecriteria(reductioninproteinuriaversus CR/PRrates).
AZAisoneofthemoreoftenusedimmunosuppressants inthetreatmentofSLEpatientsand,byhavingabettersafety profilethanotheragents,thisdrughasbeenlongusedasa CS-sparingagentand eveninthetreatmentofmilderGNs. However,fewprospectivestudieswith thisdrugwere pub-lished.Inanopen-label,prospective,multicenterstudywith 38AsianpatientsonAZAassociatedwithprednisone(without pulsetherapywithMP,orACEinhibitorsorARBs),theresults wereanalyzedat12monthswithrespecttoCR(whose crite-rionwas:stableorimprovedserumcreatinineandproteinuria <1.0g/24h)orPR(reductioninproteinuriaofatleast50%with sub-nephroticlevel)rates.CRwasachievedin67%andPRin 22%ofpatients(refractorinessin11%).Theauthorsconcluded thattheresultswithAZAweresimilarto,orbetterthan,those obtainedwithotherregimens.83
Evidenceofresponsetocyclosporine(CsA)wasobtained inafewstudies,eachwithasmallnumberofpatients.One open-labelstudyfollowed10patientstreatedwithCsA asso-ciated with prednisone for 24 months. The only response criterion was the intensity of proteinuria decrease, but in somepatients, anincreaseincreatinine,secondary tothis agent,wasobserved.Thus,CsAdoesnotseemtobea suit-ableoption, except forrefractorycases, withits use as an alternativetherapy.84
Insomestudies,CYhasbeenusedforinductionincases of MGN. One of these studies prospectively followed 20 patients with MGN and NS; the induction was done with oralCY(2.0–2.5mg/kg/day)for6monthsincombinationwith
prednisone, with sequential reduction and maintenance withAZA (withoutadjuvant therapywithACEI and/orARB or pulsetherapywithMP).Theresponsewasbasedon the achievement of CR (proteinuria <0.3g/24h, stable serum creatinine and a normalurinalysis) orPR (proteinuria>0.3 and<3.0g/day,astablecreatinine).In12months,CRandPR wereachievedin55%and35%ofpatients,respectively.79
Cyclophosphamide was alsoevaluated in arandomized controlled study comparing this drug with CsA and with prednisonealoneforinductionofremissioninGNMpatients withNS.CYIVwasadministeredeverytwomonthsforone year (0.5–1.0g/m2 BSA) and CsA daily (5mg/kg/day) for 11 months;bothmedicationswereassociatedwithprednisone andACEinhibitors,asdecidedbytheassistantphysician.CR andPRratesobtainedin12monthswithCYwere 40%and 20%,respectively,comparedwith50%forCRand30%forPR obtainedforCsAand13%forCRand23%forPRwith pred-nisonealone.BothimmunosuppressantsweresuperiortoCS used alone(p=0.002);however, throughoutthe observation period(12months),thereweremorerelapseswithCsAversus CY(p=0.02)(B).85
MMFwasusedforinductionofremissioninGNM,although inafewstudieswithasmallnumberofcases,mostofthem withnomorethan20patients.In2010,astudygathereddata fromtwomulticentricrandomizedcontrolledtrials,with sim-ilarprotocolspreviouslypublishedwhichevaluatedresponses of the induction ofremission in 6 monthswith regimens includingCYorMMFinpatientssufferingonlyMGN(n=84). PatientsweretreatedwithCYIV(0.5–1.0g/m2BSAmonthly); MMF was administered at a dose of 2–3g/day, both for 6 months.NopulsetherapywithMPwasused.Themajority ofpatientsweretreated withACE inhibitors.There wasno differencebetweengroupsregardingthepercentagechange inproteinuriaandserumcreatinine,andCRwasachievedby only1(2.5%)patient,whilePRwasachievedby60%ofpatients inbothgroups.Theanalysiswaslimitedtopatientswho com-pletedtreatment(analysisperprotocol);furthermore,23%of caseswerelosttofollowupduringtheobservationperiodafter six months(induction);nevertheless,the authors assumed thattheinductiontreatmentforGNMwithMMFhavebeenas effectiveaswithCY,86althoughinbothgroups(CYandMMF) theratesofcomplete/partialremissionwerelow(B).
MMFwasalsousedforinductionofremissioninpatients withMGNascomparedtotacrolimus(TAC).Yapetal. stud-ied16patientswithGNMandNSwhosetreatmentwasdone with MMF(7 cases) orTAC (9 cases),both associatedwith prednisone, whose initialdose was 0.8mg/kg/day (without associationofACEIorARB).Inbothgroupsanimprovement inproteinuriawasobserved, butremission rateswereonly determinedat24months(CRforMMFandTAC,57%and11%, respectively,andPRforMMFandTAC,11%and44%, respec-tively). Theauthorsdemonstrated thatthe timetoreach a (complete)responsetotreatmentwas15.3monthsforMMF and21.7monthsforTAC.6
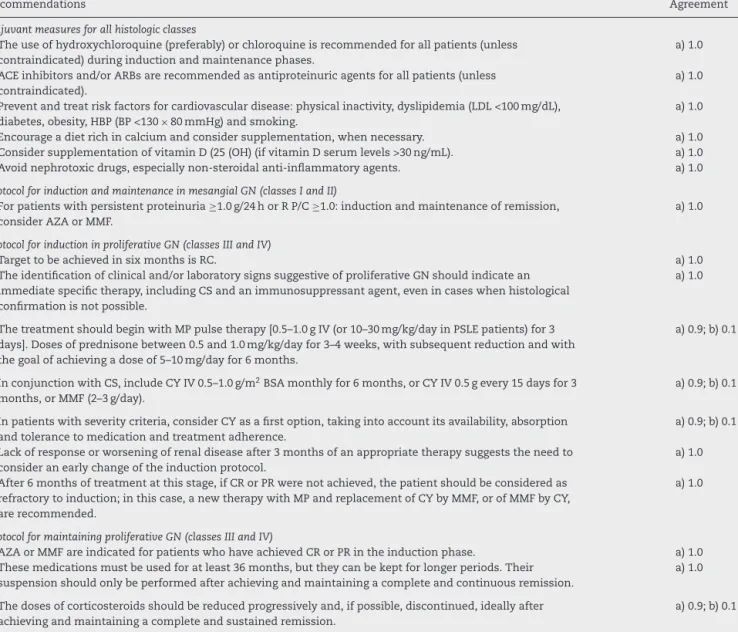
Table4–SBRrecommendationsforthetreatmentofmembranousnephritis.
Recommendations Agreement
ProtocolforinductioninmembranousGN(classV)
CRorPRarethetargetstobeachievedinsixmonths. a)1.0 Immunosuppressantsarerecommendedforallpatients,becausetheyaremoreeffectivethanCSas
monotherapy.
a)1.0
Attentionshouldbegiventotheexclusionofthromboses,includingintorenalveins,whicharefrequently presentwithpositivityforaPl.
a)1.0
ThetreatmentshouldbeginwithMPpulsetherapy[0.5–1.0gIV(or10–30mg/kg/dayinPSLEpatients)for3 days]followedbyprednisone(0.5–1.0mg/kg/day)for3–4weeks,withsubsequentreductionandwiththegoal toachieveadoseof5–10mg/daywithinsixmonths.
a)1.0
InconjunctionwithCS,CYIV0.5–1.0g/m2BSAmonthlyfor6months,orCYIV0.5gevery15daysfor3 months,orMMF(2–3g/day)andAZA(2mg/day)shouldbeincluded.
a)0.9;b)0.1
Lackofresponseafter3monthsofanappropriatetherapyindicatestheneedtoconsideranearlychangeof inductionprotocol.
a)0.9;b)0.1
After6monthsofinductiontreatment,ifCRorPRhavenotbeenachieved,LNisconsideredrefractory,anda newinductiontherapywithMPandanexchangeoftheimmunosuppressiveagent(CY,MMForAZA)are recommended.
a)1.0
ProtocolformaintenanceinmembranousGN(classV)
ThemodificationofthetreatmentregimenforthatofthemaintenancephasedependsonachievingCRorPR. a)1.0 AZAorMMFareindicatedforpatientswhohaveachievedCRorPRintheinductionphase. a)1.0 ForpatientswhohavenotachievedafavorableresponsewithAZAorMMF,switchingtooneanother,orthe
substitutionbyacalcineurininhibitororrituximab,shouldbeconsidered.
a)1.0
Thesemedicationsmustbeusedforatleast36months,buttheycanbekeptforlongerperiods.Their suspensionshouldonlybeperformedafterachievingandmaintainingacompleteandcontinuousremission.
a)1.0
Thedosesofcorticosteroidsshouldbereducedprogressivelyand,ifpossible,discontinued,ideallyafter achievingandmaintainingacompleteandsustainedremission.
a)0.9;b)0.1
Agreement:thenumbersineachrecommendationexpressthepercentagesofagreementamongthemembers,accordingtotheclassification used.
aPl,antiphospholipidantibodies;AZA,azathioprine;CY,cyclophosphamide;CS,corticosteroids;GN,glomerulonephritis;MMF,mycophenolate mofetil;MP,methylprednisolone;LN,lupusnephritis;CR,completeremission;PR,partialremission;BSA,bodysurfacearea.
and amongthe11 patients (38%)achievingcomplete renal remissionin12months,sevenhadbeentreatedwithHCLQ comparedwithfourpatientswithoutHCLQ(p=0.036)(C).87
Insummary,wecanadmitthat,inrelationtoMGN,there existslittlescientificevidencetoguideourclinicaldecisions, butitislikelythatweshouldnotregardthemasmildforms ofLN(Table4).
Membranous
glomerulonephritis
–
maintenance
treatment
JustasinPGN,themaintenancetreatmentincasesofMGN alsoincludesanimmunosuppressiveagentsuchasAZAor MMF,incombinationwithprednisoneatprogressivelylower doses.Except forthe ALMSstudy, thereare no other ran-domizedcontrolledtrialsexaminingAZAinthemaintenance ofremissioninpatientswithMGN.Nevertheless,thisagent hasbeenwidelyusedinmostcentersandMok,in2009, pub-lishedtheresultsofanopen-labelstudywithanobservation periodof12±6years,inwhichallpatientsreceivedinduction withAZAandprednisolone.Attheendofthislong observa-tionperiod,35%hadsufferedrelapses,anddespitetheneed fortheuseofotherimmunosuppressantsandforincreasing dosesofCS,79%ofpatientshadreachedproteinuriavalues
lowerthan1.0g/24hwithpreservationofrenalfunction,and 21%hadaproteinuriahigherthan1.0g/24h,althoughstillin asubnephroticlevel. Thedoublingofserum creatininewas observedin8%andnopatientprogressedtoERF.80Thestudy designwasnotidealand,furthermore,onlyincludedChinese patients;however,longerobservationperiodandthefavorable resultsallowustoadmitthatAZAhaspotentialforuseinthe maintenanceperiod(C).
In the ALMS study,71 which evaluatedthe maintenance phasewithMMForAZA,onlypatientswho hadachieveda favorableresponseintheinductionphasewereincluded.Most patientspresentedPGN,butabout15%exhibitedpureMGN (18casesinMMFgroupand17inAZAgroup),andforthese patients,therearenospecificresponsedata.
TherecommendationsofEULARandACRsuggesttheuse ofeitherofthetwomedications(D).20,21However,thereisno publicationorconsensusestablishingthemaximumtimeof therapy, aswellashowfastshouldbethereductionofthe selectedmedication.
oneconsidersthehighfrequencyofrelapsesduring follow-up.
SomecaseseriessuggesttheuseofTAC,withless nephro-toxicpotentialinthepatient’smaintenance.73,86TACcouldbe usedinspecialcases,suchasinpatientswithnormalrenal function,negativityforaPlandpersistentlyelevated protein-uria(D).
AlthoughtheresultswithCYforthemaintenancephase arenotfavorablecomparedwithAZAorMMF,thismedication canalsobeconsideredasanalternativeofexceptionfor main-tenanceinpatientswithknownpooradherencetotreatment (D).54,88
Although the existing data in the literature are incon-sistent, we understand that, for the maintenance phase, in addition to low doses of prednisone (ideally less than 10mg/day),themostsuitableagentsareAZA(2mg/kg/day)or MMF(2–3g/day)incombinationwithHCLQandanadjuvant therapy,asdiscussedbelow.IncasesofMGNrefractoriness, onecanconsidertheuseofcalcineurininhibitors,especially TACandevenRTX(Table4).21
Renal
involvement
in
the
antiphospholipid
antibody
syndrome
–
diagnosis
and
treatment
RenalinvolvementcanoccurinprimaryorsecondaryAPS,but theimpactonprognosisinNLpatientsisstillcontroversial.89 aPl(anti-cardiolipins,anti-2-glycoproteinIandlupus antico-agulant)maytriggerintrarenalvascularlesions,determining thedevelopmentofanAPSassociatednephropathy(APSN).90 The clinical picture is characterized by HBP, non-dysmorphichematuria,proteinuria andworsening ofrenal function,whichmaybeacute,withrapidprogressionto dial-ysis;orchronic,withslowand progressiveevolution.34,91–93 Acuterenalarterythrombosisevolvesmainlywithanacute, severe,difficult-to-controlhypertension,withorwithoutlow backpain,hematuriaandacuterenalfailure.90Ontheother hand,renalveinthrombosisevolvesmainlywithproteinuria, whichcanreachnephroticlevelsand,ifitoccursina com-pleteandacuteform,maybeassociatedwithasuddenlow backpainandlossofrenalfunction.90
Histopathological findings of APSN occur in 4–40% of SLEpatients, beingmorefrequentinpatientswitha previ-ousdiagnosisofAPS.34,89,91–94 Thromboticmicroangiopathy is the most important acute injury; it is characterized by thepresenceoffibrinthrombiinglomerularcapillariesand arterioles.95 However, this injury is hardly found alone in patientswithSLE, giventhefrequentoverlapping withthe histopathologicalchangesoflupusnephritis.34Thefollowing chronicinjuriesarefrequentlyfound,althoughtheyhaveless specificityforthe diagnosisofAPSN:fibrous intimal hyper-plasiaandthepresenceoforganizedthrombiwithorwithout recanalization, fibrous or fibrocellular occlusion of arteries andarterioles,tubulartireoidizationcharacterizedbyatrophy oftubules with eosinophilic casts, and focal cortical atro-phywithor withoutdepressioninthe contouroftherenal capsule.95 Theassociation ofatleast oneacute orchronic histopathological finding with the presence of aPl defines APSN.95,96
The main differential diagnoses involve clinical condi-tionsassociatedwithclottingdisorderorendothelialinjury, such as thrombotic thrombocytopenic purpura, hemolytic uremicsyndrome,malignanthypertension,diabetes, sclero-dermarenalcrisis,pre-eclampsia(PE),drugtoxicity(CsAand chemotherapics)andrenaltransplantrejection.34,91–96
APSN wasassociatedwithlupusanticoagulant, ACL IgG andbeta2GPI,andevenmoreoftenwhentwoormoreofthese aPlarepresent.However,duringthevasoocclusiveeventthese antibodiesmaybetemporarilyabsent.89,94,96
Echography with color Doppler, scintigraphy with 99m Tc-DMSAand renal-vesselangiographyassistinthe identi-ficationofvascularinvolvement,97butthehistopathological changesnecessaryforthediagnosisofAPSNareidentifiedby renalbiopsy.90
AllpatientswithSLEandaPlmustcontroltheriskfactors for thrombosis: obesity, HBP, smoking, diabetes and dys-lipidemia. Furthermore, these patients should avoid using estrogencontraceptivesand hormone replacementtherapy (D).98Incasesofvenousthrombosis,anticoagulationis indi-catedindefinitelywithanINRbetween2.0and 3.0(B).99 In cases ofarterial thrombosis, althoughwith this same rec-ommendation, some authors advocate the combination of anticoagulationwithanantiplateletagentormaintainingan INRabove3.0inrecurrentcases(C).98Theuseofstatinscould alsoplayanadjuvantroleinthetreatmentofpatientswith APS (C)98 and inpatients withAPSN, oneshould takeinto accounttheuseofHCLQandanantiplateletagent,or anti-coagulation(B).21,100
Adjuvant
therapy
in
lupus
nephritis
Inadditiontothejudicioususeofimmunosuppressiveagents, bothininductionofremissionasinthemaintenancephase, severalothermeasurescanalsocontributepositively,notonly toobtainabettercontroloftheinflammatoryprocess,butalso forthepreservationofrenalfunctioninthelongterm.These measuresconsistofnon-pharmacologicaland pharmacolog-icalrecommendationslistedbelow:
(a) Providedietarycounselingforthepreventionandcontrol ofdyslipidemia,diabetes,obesity,HBPandosteoporosis. Encourageabalanceddietwithproteins,lipidsand carbo-hydrates,withlowlevelsofsalt(D).101
(b) ConsidervitaminDsupplementationforallpatients,with doses800–4000IU/day,withsequentialadjustments;the serumlevelsof25(OH)vitaminDshouldremainabove 30ng/mL,althoughtheclinicalbenefitsarestill negligi-ble(B).102,103Encourageacalcium-richdietandconsider itssupplementationincaseswherethereisaneed, espe-ciallyinpatientstreatedwithCSandinpostmenopausal women(C).101
(c) Avoid the use of nephrotoxic drugs, particularly nons-teroidanti-inflammatorydrugs(NSAIDs)(C).104
(d) Stronglyencouragesmokingcessation(C).101
are already well establishedforchronic kidney disease from other etiologies, (a)106 and by their renoprotec-tor and antiproteinuric effects. For that reason, these agentsshouldbeusedeveninpatientswithnormalblood pressure levels. These drugs should be usedwith cau-tionincasesofrenalfailure,sincetheycanbothcause hyperkalemia,butcanalsoreducethefiltrationpressure, withasubsequentdeclineinglomerularfiltrationrates (A).107–110Theassociationoftheseclassesof antihyperten-sivedrugsappearstohaveanevengreaterantiproteinuric effect; however, their impact on renal function in the long term has not yet defined.110 The dose should be adequateforamaximumantihypertensiveand antipro-teinuriceffect,withmonitoringofpotassiumlevelsand renalfunction.21
(f) HCLQ is associated with higher rates of response to treatment,lower frequencyofrelapses,less severe kid-ney damage, reduction of thromboembolic events and increasedsurvival; forall that, thismedication is indi-cated for all patients with LN, both in their induction and in maintenance phases, unless contraindicated (B).20,21,87,111–114Anophthalmologicevaluationshouldbe performedbeforestartingthe treatmentandshould be repeated annually after five years of continuous use, exceptincaseswithincreasedriskfordevelopmentof reti-naltoxicity:elderlypatients;renalorhepaticdysfunction; HCLQ>400mg/day(>6.5mg/kg/day); cumulativedose of HCLQ>1000g;orpresenceofpriorretinaldiseaseor mac-ulopathy.Inthesecases,itisrecommendedanintervalof oneyearafterstartingthetreatmentwithHCLQ.115 (g) Contraceptives containingestrogensshould beavoided,
especially duringthe active phase ofthe disease,or if the patient has a priorhistory ofcardiovascular event or of increased risk of occurrence of thromboembolic events (B).116 Theuse ofhormone replacementtherapy alsoshouldbeavoided(B).117
(h) The treatment of dyslipidemia with statins should be recommended for patients with LDL cholesterol >100mg/dL,20despitethesmallnumberofstudies involv-ingpatientswithSLE(C).118,119
Refractory
lupus
nephritis
Despitethe significant improvementinsurvivaland inthe preservation of renal function in most patients with LN, about10–29%progresstoERF.16,120Thisprogressioncanoccur silently,78ormaybeevidentthroughtheevolution,beingmore commoninpatientswhodevelopproliferativeforms.Inmost studies,attheendoftheinductionperiod,lessthan50%of theindividualsachieveCR74;inclinicalpractice,amore real-isticgoalseemstobetheachievementofPRorCRinaperiod from6to12months.CasesthatdonotachieveCRorPRafter thistimewithanappropriatetreatmentcouldbeclassifiedas refractorytotheregimeninstituted.
Therearevariousclinicaland/orlaboratoryaspectsrelated torefractoriness,and amongthese,themostcommon are: LNappearanceinadolescence,malegender,lowbloodlevels ofcomplement,thrombocytopenia,elevatedserumcreatinine andmassiveproteinuriaatdiagnosisofLN.11,121Somefactors
aredirectlyrelatedtotheaggressivenessofglomerular inflam-matory events,suchas newepisodesofrenal reactivation, particularlyinthefirst18monthsofthedisease,massive pres-enceofcrescentsand/orvascularnecrosis,histological trans-formation,oroverlappingoflesionssecondarytoAPS.122–128 Ontheotherhand,therefractorinesstoLNmayberelatedto othervariables,suchasdelayingthestartofaneffective treat-ment,besidesanimpossibilityofcompliancewiththe treat-mentprotocol,eitherbyinfectionand/ortemporary suspen-sionofmedicines,orbypooradherencetotreatment.29,129–131 Patients withtreatment-refractory lupus nephritis (RLN) should befurtherevaluated forthe presenceofother pos-siblecausesofpersistentproteinuriaorrenalfunctionloss, forexample,useofnephrotoxicdrugs,thrombosisofrenal veins/arteries,infections,anddecompensatedhypertension or diabetesmellitus.20,21,29 Anothercondition thatdeserves tobeinvestigatedistheoverlapping ofinjurysecondaryto tubulointerstitial nephritis (TIN) related, in most cases, to the use of antimicrobialagents, toocommon in phasesof increasedimmunosuppression.Themostsuggestivefindings arehyperuricemia,hypokalemia,isosthenuriaandrenal tubu-laracidosis,aswellasfindingsintheurinarysediment,which maybethepresenceofagreaterquantityofkidneytubulecells inassociationwithabsenceoffindingsindicativeofactiveGN. Inisolatedcases,othercausesofproteinuria (glomerulopa-thysecondarytodiabetes,syphilis,ortoHIVorHCVinfection) canalsoco-exist,ormayariseduringtheevolution,givingthe impressionofrefractoriness.InthecaseofRLN,anewrenal biopsymaybeindicated,becausethisproceduremayallow theidentificationoflesions(likesomeofthoseabove)orthe characterizationofthepresenceofexclusivelychroniclesions –orcharacterizationofthepresenceofpurechroniclesions– andinthelattercase,furtherimmunosuppressionwouldnot benefitthepatient(A).131,132
After identifyinga non-treatmentresponsive, persistent inflammatory activity,RTX, ananti-CD20monoclonal anti-body,hasbeenconsidered astherapeuticoption. Published studiesofcaseseriesinvolvingpatientsclassifiedas refrac-tory totreatmenthave shown good responsein47–89%of cases.132,133InaprospectivecontrolledtrialwithRTX(LUNAR), whichincludedpatientswithLN,nosuperiorityofRTXwas demonstrated,whenthisdrugwasusedincombinationwith MMFandCSversusplacebo.Butitislikelythatthese nega-tiveresultsweremoreduetothestudydesignthanthelack ofefficacyofthedrug.134Despitethelackofcontrolled stud-ies demonstratingefficacy ofRTXfortreatmentofLN, this drughasbeenusedwithgoodresultsinmostreference cen-ters,andcurrentlyitsuseisrecommendedintheconsensuses ofEULARandACRforpatientsconsideredrefractory,bothin casesofPGNandMGN.20,21Theadministrationregimenand dosesusedaresimilartotherecommendationsfor rheuma-toidarthritis(twodosesof1000mg,withanintervalof15days) (C).
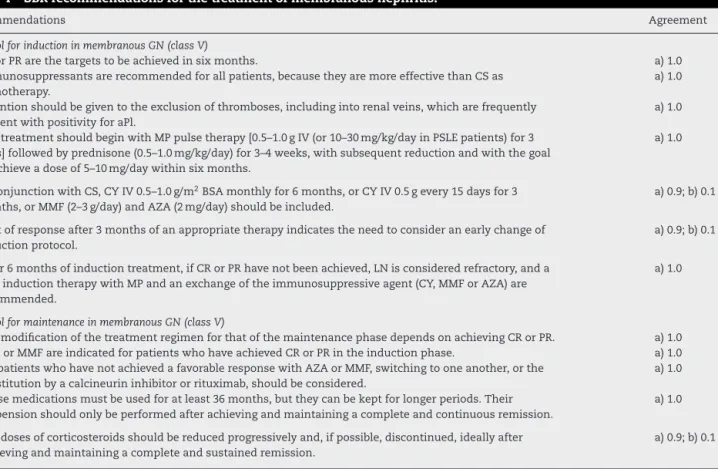
Table5–SBRrecommendationsforthetreatmentofrefractorylupusnephritis,APSN,LNinpregnancy,pediatricLNand managementinERF.
Recommendations Agreement
RefractoryLN
LNshouldbeconsideredrefractorywhenCRorPRisnotachievedafter12monthsofanappropriate treatment.
a)1.0
Consideranewkidneybiopsytoassistinidentifyingthecauseofrefractorinessandintherapeuticdecision. a)0.9;b)0.1
Rituximabisindicated,includingcaseswithrenalinsufficiency. a)1.0 Tacrolimus(aloneorincombinationwithMMF)maybeusedasanalternative. a)1.0
APSNassociatedtoLN
SearchaPlinpatientswithLN,duetothepossibilityofanassociationwithAPSN. a)1.0 MaintaincontrolofriskfactorsassociatedwithvasoocclusiveeventsinpatientswithaPl. a)1.0 InpatientswithAPSN,maintainINRcloseto3andconsidertheconcomitantuseofantiplateletagents. a)1.0
LNandpregnancy
SLEfemalepatientsshouldbeadvisednottobecomepregnantuntildiseaseremissionforatleastsixmonths andwithanormalrenalfunction.
a)1.0
Pregnancyshouldbeplanned,includingdiscontinuationofteratogenicmedications(ARB,CY,coumarin,ACE inhibitors,leflunomide,MMFandMTX).
a)0.75;b)0.25
Monitoringshouldbedonebyamultidisciplinaryteamthroughoutpregnancyandpuerperium. a)0.9;b)0.1
HCLQshouldbeusedthroughoutpregnancy. a)1.0
CSandAZAcanbeusedduringpregnancy. a)1.0
LNinPSLEpatients
ThetreatmentofnephritisinPSLEpatientsissimilartothatofadults,withdoseadjustmentofdrugs (AZA=2.0–3.0mg/kg/day,MP=20–30;MMF=30mg/kg/dayor600mg/m2BSA/day);reinforceadherenceatevery visit.
a)1.0
LNandERF
MaintainthetreatmentbyarheumatologistevenafterRRT,includingtheuseofHCLQwithadjustmentofits doses.
a)1.0
ExtrarenalrecurrencescanbetreatedwithCS,AZAandMMF(withadjusteddoses). a)1.0 ConsiderrenaltransplantationinpatientswithERF(livingorcadaverdonor). a)1.0 SpecialconsiderationshouldbegiventopatientswithaPl,becauseoftheriskofthrombosisinarteriovenous
fistulaandvasoocclusivelesionswithpotentialgraftloss.
a)1.0
Agreement:thenumbersineachrecommendationexpressthepercentagesofagreementamongthemembers,accordingtotheclassification used.
aPl,antiphospholipidantibodies;AZA,azathioprine;ARB,angiotensinreceptorblockers;CY,cyclophosphamide;CS,corticosteroids;ERF, estab-lishedchronickidneydisease;ACEI,angiotensin-convertingenzymeinhibitors;SLE,systemiclupuserythematosus;PSLE,pediatricSLE;MMF, mycophenolatemofetil;MP,methylprednisolone;MTX,methotrexate;LN,lupusnephritis;APSN,nephropathyofAPS;CR,completeremission; PR,partialremission;INR,internationalnormalizedratio;RRT,renalreplacementtherapy.
pregnancy(classC).However,itsknowndiabetogeniceffect should be taken into account, especially in patients with metabolic syndrome, inaddition to the thrombotic risk in aPlpositivepatients(C).135–138Belimumab,ananti-Blys anti-body,wasnotspecificallyevaluatedinpatientswithLN,but inthetwomainstudieswiththisagentapproximately10% ofpatientshadGNwithproteinuriaofupto6g/day.Inthe analysisofthis subgroup, thedrug was effectivein reduc-ingthelevelsofproteinuria139,140;however,morestudiesare neededtodeterminetheefficacyofbelimumabinthis condi-tion(Table5).141
Nephritis
in
pediatric
systemic
lupus
erythematosus
(PSLE)
Inabout10–20%ofpatients withSLE,the onsetofthe dis-easeoccursbeforereachingtheageof18,whenthecondition
isclassifiedasPSLE,142,143 characteristicallyshowinggreater activity,cumulativedamageanddiseaseseveritycomparedto theadults.Additionally,thesepatientsshowhighfrequency ofnephritis(inupto80%ofpatients),neurologicaland hema-tologicalinvolvementandpulmonaryhemorrhage.143–147
between4and6months21anddiscontinuationofthisdrug, whenever possible.As is recommended for adultpatients, HCLQ (5.0–6.0mg/kg/day) is indicated in all cases of PSLE nephritis.21 NL class I or II is generally controlled by CS andHCLQ.ForclassIIIorIV,inductiontherapyisindicated withacombinationofHCLQ,CSandanimmunosuppressive agent:CYIV(0.5–1.0g/m2BSA/monthfor6months)orMMF (30mg/kg/dayor600mg/m2 BSA/day).Maintenancetherapy issuggestedwithAZA(2.0–3.0mg/kg/day)orMMF.150A con-trolledstudyofLNinpatientswithPSLEsuggestsatherapeutic responsesimilartothatobtainedinstudiesofadultswithCY orMMF.151 CYseemstohaveabetterrisk-benefitprofilein childrenandadolescentscomparedwithadults,150withrare occurrencesofprimaryovarianfailure(earlymenopause),152 besidesfacilitatingadherence.149Theschemewithlowdoses ofCY(ET)hasnotbeenevaluatedinthepediatricpopulation.21 IncasesofLNclassV,drugstoreduceproteinuria–HCLQ,CS andimmunosuppressants(CY,MMForAZA)–areindicated,153 despitetheabsenceofadequateprospectivestudies evaluat-ingtheseagentsinpediatricpopulations.
TherapywithRTX(375mg/m2BSA/weekfor4doses)has beenusedinrefractorynephritisinPSLEpatients,154butthis schemestillrequiresstudieswithalargernumberofpatients. Todate,thereisstillnostudyofbelimumabinchildrenand adolescentswithlupus(Table5).
Established
chronic
kidney
disease
in
lupus
nephritis
Currently, about 10–29% of patients with NL develop ERF, requiringrenalreplacementtherapy(RRT).16 Data fromthe UnitedStatesRenalDataSystem(USRDS)showanincreased prevalenceofLNasacauseofERF,from1.13to3.2%intheage group20–44years,possiblyrelatedtoanearlierdefinitionof diagnosis(USRDS2011).Aswithinothercountries,inBrazil themeanageofpatientswithSLEattheonsetofRRTis38 years,muchlowerthanthatofpatientswithHBP(70years), diabetesmellitustype1(51years)andDMtype2(64years) (SBR2014census)(A).
ComplicationratesofERF inSLEpatientsare similar to otheretiologies,butwithhigherfrequencyoffistulaloss.155 Thereisalsothepossibilityofrenalfunctionrecovery,which mayoccuraftertheimplementationofdialysisinupto28% ofpatients,usuallyinthefirst6monthsofdialysis.156–158
Mostpatientsremaininremission,butoutbreaksof activ-itymayoccur.159–163 Infact,manysymptomsofERFmaybe confusedwithmanifestationsofSLE,suchasfever,arthralgia, arthritis,alopecia,retinalchanges,headache,serositis, hema-tologicalchangesandreducedlevelsofcomplementfractions. In this sense, non-renal SLEDAI score (SLEDAInr) which is derivedfromSLEDAI,wasvalidatedasausefulinstrumentfor assessingactivityinpatientsonRRT160,163,164;thistoolcanbe usedinapproachingthosepatients(B).Thesurvivalofpatients withSLEinRRTat5years rangesfrom 50 to89%and the mortalityistypically multifactorial.157,158,162,164–172 Recently, aprospectivestudy showedan independentassociation of diseaseactivity atthestartofRRT(withSLEDAInr>8)with increasedmortalityat5years(B).9
BothCSandHCLQcanbeemployedforRRT,butmyelotoxic drugssuchasmethotrexateandCYshouldbeavoided.Other drugssuchasAZAandMMFshouldbeevaluated individu-ally.Dosesofimmunomodulatorymedicationsshouldnotbe correctedanddonotrequireanadditionaldoseafterdialysis ofthedrugsalreadymentioned.Thereisnoevidenceonthe safetyoftheuseofimmunobiologicalsinSLEpatientson dial-ysis,butitislikelythatintheeventofsuchdrugsareused, thereisnoneedofdosagereadjustment,forthesearehigh molecularweightcompoundsnotremovablebydialysis mem-branes(D).Allthingsconsidered,allSLEpatientsinRRTshould bemonitoredbytherheumatologist.
Renal transplantation (TxR) from cadaveric source has proved a successful option since the 1950s, but its use in patients with LN was questioned by the potential risk of recurrence in the transplanted kidney. However, since 1975ithasbeendemonstrated thatpatientswithSLEhave a behavior similar to other patients (Advisory Committee, 1975); and sincethattime, TxRprocedures have been per-formedwithaverylowfrequencyofrecurrence.173–175Factors suchasanassociationwithAPSorhighaPltitles176,177 and donortype178contributetoworseresults,but thesearenot hindering factors to this procedure in these patients (C) (Table5).
Lupus
nephritis
and
pregnancy
ThefertilityrateinpatientswithSLEisconsiderednormal; however,severerenalfailureandhighdosesofCScancause menstrualirregularitiesandamenorrhea.179Atthesametime, someimmunosuppressants suchasCYcaninduceovarian failure,andthiscomplicationdependsonthepatient’sageat onsetofmedication,durationoftreatmentand,additionally, theaccumulateddose(D).180
Pregnancy inpatientswithSLEshould beconsideredas being ahigh-riskevent;amultidisciplinaryapproachupto puerperiumisrecommended.Studiesreportatwotothreefold increaseinthefrequencyofdiseaseactivityduringpregnancy (C)181,182 and theoccurrenceofcomplications,especiallyin womenwithmoderatetoseveredisease(C).183
Womenwith SLEshould beadvisedto avoidpregnancy until the disease is in remission for at least six months (D)184–186andthatGFR>50mL/min.21(D)Furthermore,theuse ofimpropermedicationfortheperiodisavoided.187
Theriskofobstetricandneonatalcomplicationishigherin womenwithSLEcomparedtothegeneralpopulation(A).188,189 However,inthelastdecadestherehasbeenareductionfrom 43%(between1965and1969)to17%(between2000and2003)in fetalloss(D).190Thefrequencyofmiscarriageisincreasedand intrauterinefetaldeathisfivetimesgreater.Pre-eclampsia(PE) occursinover20%versus7.6%inthepopulationwithoutlupus; onthe otherhand,intrauterinegrowth restriction(IUGR)is alsocommon,especiallywithpre-existingrenaldisease. Pre-maturityaffectsupto33%ofpregnanciesandisassociated withHBP,useofCSatthetimeofconceptionandduring preg-nancy,diseaseactivity,andpresenceofnephroticproteinuria andaPl(C).188,191