revbrashematolhemoter.2017;39(3):285–287
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Letter
to
the
Editor
Patients
with
very
severe
anemia:
a
case
series
DearEditor,
Anemiaoccurscommonlyworldwideandatallagesoflife1
and,althoughfrequentlyoverlooked,itaffectsmortality, mor-bidityandqualityoflife,evenwhenmild.2,3Theprevalenceof
anemiavarieswidelydependingonitsdefinition.TheWorld HealthOrganizationhasestablishedsomecut-offhemoglobin (Hb)levels,stratifiedbygenderandinpartbyage,todefine thepresenceofanemia.4Foradults,theselevelsarelessthan
12g/dLforwomenandless than13g/dLformen,although these cut-off points may not be fully appropriate for the elderly.5SevereanemiahasbeendefinedasHb<8.0g/dLfor
both genders. However, hemoglobin is a simple surrogate markerforthedisease that hasprovoked anemia.To treat anemiassimplyrestoringa“safer”hemoglobinlevel(i.e.,by meansoftransfusionsorerythropoietin)maybeverydifferent than curing them byeliminating the causes that had pro-vokedthe condition.Moreover,several reportshaveshown thatbothtransfusionsanderythropoiesisstimulatingagents mayindeedcarryanincreasedriskofadverseevents. There-fore,it isquite surprisinglythatinhealthservices,anemia continuesto beregarded asa “minor” disease,evenwhen severe,tobeassignedtotheambulatorysettingintheabsence ofarobustbodyofliteraturetosupportthiscommonpractice. InItaly,disorders ofredbloodcellsinpeopleolderthan 17years[InternationalClassificationofDiseases–ninth revi-sionClinicalModification(ICD-IX-CM)codes280–285]“outside urgencies”areconsiderednottobeappropriateforhospital admission,regardlessoftheseverityoftheHbdeficiencyor thepresenceofimportantcomorbidities,includingareduced functionalcapacityinolderpeople.6Webelievethattorely
on assumptions of this kind in advance of evidence may carry a risk to induce somepotentially deleterious conse-quences,includingoveruseofbloodtransfusionstoreachan Hb level “safe” for emergency room discharge rather than patientclinicalstatus.Historically,andincurrentguidelines,7
theindicationfortransfusioncomesfrombothHb concentra-tionandtheclinicalscenario;totransfuseinordertoavoid hospitaladmissionshouldberegardedasunethical.
Weconductedanobservational, prospectivestudy ofall patients admittedto an Internal Medicine ward with very severeanemia,aimingtoexploretheclinicalandassistential burdenofseverelyanemicpatientsadmittedtothehospital. Patients with an Hb concentration of 6g/dL or less were
Table1–HierarchyoftheproceduresforInternational ClassificationofDiseases(ninthrevision)Clinical Modificationcoding.
1.Opensurgery
2.Endoscopicsurgicalprocedures
3.Otherinvasivediagnosticortherapeuticprocedures 4.Procedureswithclosedbiopsyoforganortissues 5.Allotherdiagnosticortherapeuticprocedures
eligible. Those presenting with overt hemorrhage or acute anemia were excluded. Patients were managed as usual, and nodiagnostic ortherapeuticprocedure wasperformed for study purposes alone. In defining the main diagnosis atdischarge,ourstandardprocedure wastoselectfirst the procedurethathadabsorbedthelargestamountofresources, accordingly to a predefined hierarchy (Table 1) and then to choose the consequent diagnosis. Accordingly to our laboratory, wedefined microcytic anemia asall caseswith a mean corpuscular volume (MCV) ofless than 81fL, and macrocyticanemiaasthosewithaMCVofmorethan 98fL andnormocyticanemiaasallothers.Thrombocytopeniawas definedasanabsoluteplateletcountoflessthan150×109/L;
leukopeniaasawhitebloodcellabsolutecountoflessthan 4.0×109/Landlymphopeniaasanabsolutelymphocytecount
oflessthan1.1×109/L.
Themainoutcomeofthestudywasall-cause,in-hospital mortality.Secondaryoutcomeswereone-yearmortalityand thepercentageofadmissionsforanemiathatwerelosttoa retrospectiveanalysisbasedonlyoncoding.Continuous vari-ablesareexpressedasmeans±standarddeviation(SD)oras medians with minimum and maximum values when data didnothaveanormaldistribution;categoricaldataaregiven as countsand percentages. TheInstitutionalReview Board approvedthe study,whichwas carriedout and isreported accordingtotheStrengtheningtheReportingofObservational StudiesinEpidemiology(STROBE)guidelinesforobservational studies.8
286
revbrashematolhemoter.2017;39(3):285–287Table2–Hematologicaldata.
Discharged77(89.5%) Deceased9(10.5%) p-Value
MeanHb,g/dL–n(SD) 5.02(0.81) 5.43(0.71) ns
MeanMCV,fL–n(SD) 85.4(20.7) 88.4(16.6) ns
Microcytic–n(%) 42(54.5) 2(22.2) nsa
Normocytic–n(%) 14(18.2) 5(55.6) <0.05b
Macrocytic–n(%) 21(27.3) 2(22.2) nsc
Thrombocytopenia–n(%) 14(18.2) 2(22.2) ns
Leukopenia–n(%) 12(15.6) 1(11.1) ns
Lymphopenia–n(%) 25(32.5) 4(44.4) ns
a Ascomparedwithnon-microcyticanemias.
b Ascomparedwithmicrocyticanemias.
c Ascomparedwithnon-macrocyticanemias.
hospitalization(10.5%);theremaining77patientswere dis-chargedandfollowedupforabout170patient-years.Deceased patientswereolderthandischargedpatients:meanagewas 90±10vs.75.5±15.7(p-value<0.01).Duringthesameperiod, generalin-hospitalmortalitywas12.3%.Meanfollow-upwas 806days (range:16–2072 days)duringwhich time32 more patientsdied.Meantimetodeathwas412days.The cumu-lativepercentagesofdeathat1,3and12monthswere3.9%, 13.0%and29.9%,respectively.Whenin-hospitalmortalitywas
includedandaddedtoone-monthmortality,the correspond-ingfiguresbecame13.9%,22.1%and37.2%.Hematologicaldata areshowninTable2.Therewerenosignificantdifferencesin meanHbandMCV,orinthepresenceofcytopeniasotherthan anemia.However,dischargedpatientsmoreoftenhad micro-cyticanemias(54.5%)comparedtodeceasedpatients,whose anemiasweremoreoftennormocyticormacrocytic(77.8%). Patientswithanormocyticanemiahadanincreasedriskto dieinthehospitalwhencomparedwiththosewithmicrocytic
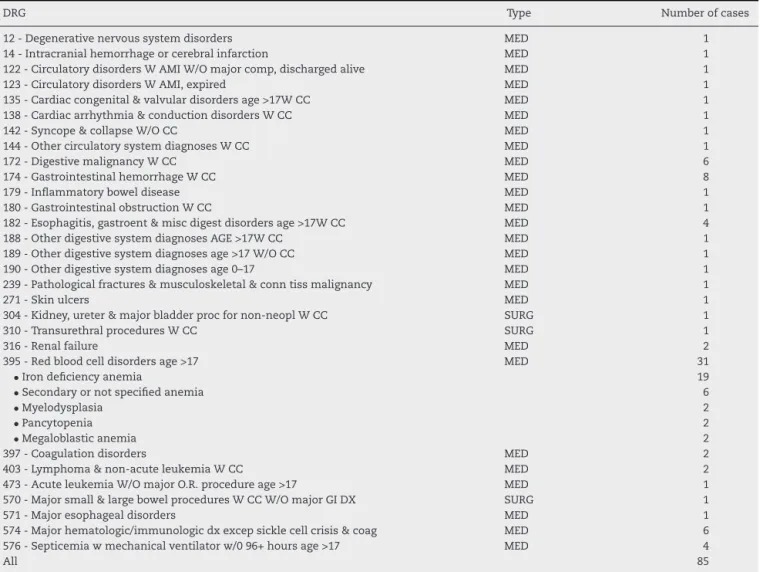
Table3–DiagnosisRelatedGroups(DRG)accordinglytoInternationalClassificationofDiseases(ninthrevision)Clinical Modificationcoding.
DRG Type Numberofcases
12-Degenerativenervoussystemdisorders MED 1
14-Intracranialhemorrhageorcerebralinfarction MED 1
122-CirculatorydisordersWAMIW/Omajorcomp,dischargedalive MED 1
123-CirculatorydisordersWAMI,expired MED 1
135-Cardiaccongenital&valvulardisordersage>17WCC MED 1
138-Cardiacarrhythmia&conductiondisordersWCC MED 1
142-Syncope&collapseW/OCC MED 1
144-OthercirculatorysystemdiagnosesWCC MED 1
172-DigestivemalignancyWCC MED 6
174-GastrointestinalhemorrhageWCC MED 8
179-Inflammatoryboweldisease MED 1
180-GastrointestinalobstructionWCC MED 1
182-Esophagitis,gastroent&miscdigestdisordersage>17WCC MED 4
188-OtherdigestivesystemdiagnosesAGE>17WCC MED 1
189-Otherdigestivesystemdiagnosesage>17W/OCC MED 1
190-Otherdigestivesystemdiagnosesage0–17 MED 1
239-Pathologicalfractures&musculoskeletal&conntissmalignancy MED 1
271-Skinulcers MED 1
304-Kidney,ureter&majorbladderprocfornon-neoplWCC SURG 1
310-TransurethralproceduresWCC SURG 1
316-Renalfailure MED 2
395-Redbloodcelldisordersage>17 MED 31
•Irondeficiencyanemia 19
•Secondaryornotspecifiedanemia 6
•Myelodysplasia 2
•Pancytopenia 2
•Megaloblasticanemia 2
397-Coagulationdisorders MED 2
403-Lymphoma&non-acuteleukemiaWCC MED 2
473-AcuteleukemiaW/OmajorO.R.procedureage>17 MED 1
570-Majorsmall&largebowelproceduresWCCW/OmajorGIDX SURG 1
571-Majoresophagealdisorders MED 1
574-Majorhematologic/immunologicdxexcepsicklecellcrisis&coag MED 6
576-Septicemiawmechanicalventilatorw/096+hoursage>17 MED 4
revbrashematolhemoter.2017;39(3):285–287
287
anemia (OR 7.5; 95% confidence interval: 1.3–43.1; p-value <0.05).Lymphopenia, asurrogatemarkerforhyponutrition, wasmoreprevalentindeceasedpatients(44.4%vs.32.5%).
Atotalof295unitsofpackedredcellsweretransfusedto the77dischargedpatients(mean:3.8),and29unitstothenine deceasedpatients(mean:3.2).Onepatientwhodiedrefused bloodtransfusionsbecauseofreligiousbeliefs.Patients dis-chargedalivewere submittedto77invasiveprocedures:39 toesophagogastroduodenoscopy,23 tocolonoscopy,four to capsular videoendoscopy (preceded by radiologic study of gastrointestinaltractinallfourcases)and 11tobone mar-rowbiopsies.Administrativedatawascompletefor85cases (98.8%).DiagnosisRelatedGroups(DRG)accordingtothe ICD-IX-CMcodingareshowninTable3;threeweresurgical,and theremainingwereclinical.Only31/85caseswerecodedas DRG395(redbloodcelldisorders–age>17),soabout63%of patientsadmittedforanemiawouldhavebeenlostifthis sur-veyhadbeenconductedretrospectivelyondischargedata.The meanreimbursementwas3165euros.
Inthis preliminarystudy,wereportdataonasampleof 86consecutive,unselectedelderlypatients(82.5%ofwhom were65yearsorolder).In-hospitalmortalitywas10.5%,but morethanonethirdofthesepatientseventuallydiedwithin a year after the index admission. Discharged patients, as comparedwiththosewhodiedinthehospital,hadmicrocytic anemiasmoreoften(54.5%vs.22.2%).Conversely,deceased patientshadahighprevalenceofnormocyticanemias(18.2% vs.55.6%).Wespeculatethatmicrocyticanemiacould have been more often the expression of a single and possibly curabledisease,whereasnormocyticanemiasshouldbethe resultof multiple comorbiditiesthat played the main role incausing death.In ourstudy,we demonstrated thatvery severeanemiaisnotabenignconditionwithhighmortality, andwequestiontheadvisabilityofhospitalization.Inmany casesanemia couldbe managed without transfusions(i.e., ironandvitaminB12deficiency,chronicrenalinsufficiency, myelodysplasiaandchemotherapy-relatedanemia),butthis isoftenimpossiblewithoutpatientmonitoring,andthereisa riskofoveruseofbloodtransfusionsinthiskindofpatientin ordertodischargethemfromtheEmergencyDepartment.To clarifythisissuethereisaneedforprospective,randomized studies;indeedinourcohort,63%ofdischargediagnoseswere notintheDRG395group,andwouldhavebeenmissedifwe conductedaninvestigationbasedonadministrativedataonly. Weacknowledgesomelimitations ofthis study beyondits observationalnature.Thisisasingle-centerexperience,and resultsmaynotbereproducibleinothercontexts.However, werecruitedallconsecutivepatientswithverysevereanemia overaperiodofmorethanfiveyears,andweexcludedonly patientswithacuteanemiafrombleeding.Furthermore,with about 170patient-years ofobservation, we think thatdata onmortalityaresufficientlyrobust.Weenrolledpatientson thebasisofanarbitrarythresholdofHbthatwedefinedas “verysevere”.Indeed,33patientshadHblessthan5.0g/dL, and 13 less than 4g/dL,values thatshould beregarded as lifethreatening,especiallyinold,comorbidpatients.There islittledoubtthatifwechoseamorepermissiveapproach (i.e.,anHblevelof7.0–8.0g/dL),wewouldhaverecruited a widersampleofpatients.Tostudypatientswithlesssevere anemiahowever,was notinourinterest,sincewefocused
ontheprognosisofpatientsforwhomtherearescarcedata intheliterature.Ourpatientsweretransfusedwiththreeto fourunitsofpackedredcellseach.Duetotheobservational designofthe study,we were notable toelucidateif there wasadetrimentaleffectoftransfusionsonpatientoutcomes. Finally, wedidnotevaluatetheimpactofcomorbiditieson mortalityin thiscohort ofpatients, but weare planning a follow-upstudytoaddressthisimportantquestion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DallmanPR,YipR,JohnsonC.Prevalenceandcausesof anemiaintheUnitedStates,1976to1980.AmJClinNutr. 1984;39(3):437–45.
2.RivaE,TettamantiM,MosconiP,ApoloneG,GandiniF,Nobili A,etal.associationofmildanemiawithhospitalizationand mortalityintheelderly:thehealthandanemia
population-basedstudy.Haematologica.2009;94(1):22–8.
3.NissensonAR,GoodnoughLT,DuboisRW.Anemia:notjustan innocentbystander?ArchInternMed.2003;163(12):1400–4.
4.WHO.Haemoglobinconcentrationsforthediagnosisof anaemiaandassessmentofseverity.VitaminandMineral NutritionInformationSystem.WHO/NMH/NHD/MNM/11.1. [Internet].Availablefrom:2011http://apps.who.int/iris/ bitstream/10665/85839/3/WHONMHNHDMNM11.1eng. pdf?ua=1.
5.SpivakJL.Anemiaintheelderly.Timefornewbloodinold vessels?ArchInternMed.2005;165(19):2187–9.
6.MinisterodellaSalute.Decretodelpresidentedelconsigliodei ministri29novembre2001.Definizionedeilivelliessenzialidi assistenza.(G.U.SerieGenerale,n.33del08febbraio2002). 7.Chronicanaemia.Bloodtransfusionguideline.Utrecht(The
Netherlands):DutchInstituteforHealthcareImprovement CBO;2011.p.108–65.
8.vonElmE,AltmanDG,EggerM,PocockSJ,GøtzschePC, VandenbrouckeJP.STROBEinitiative.TheStrengtheningthe ReportingofObservationalStudiesinEpidemiology(STROBE) statement:guidelinesforreportingobservationalstudies.Prev Med.2007;45(4):247–51.
MarcoCeia,AlessandroFerrettib, NicolaMumolib,∗ aOspedaleCivilediCecina,Cecina,Italy
bOspedaleCivilediLivorno,Livorno,Italy
∗Corresponding author at: Department of Internal Medicine,
OspedaleCivilediLivorno,vialeAlfieri36,57100Livorno,Italy. E-mailaddress:[email protected](N.Mumoli).
Received21January2017 Accepted12February2017 1516-8484/
©2017Associac¸ ˜aoBrasileiradeHematologia,Hemoterapiae TerapiaCelular.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
http://dx.doi.org/10.1016/j.bjhh.2017.02.001