w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Prophylactic
strategies
for
acute
hemolysis
secondary
to
plasma-incompatible
platelet
transfusions:
correlation
between
qualitative
hemolysin
test
and
isohemagglutinin
titration
Cinthia
Silvestre
Landim,
Francisco
Carlos
Almeida
Gomes,
Bernardete
Martin
Zeza,
Alfredo
Mendrone-Júnior,
Carla
Luana
Dinardo
∗Fundac¸ãoPró-Sangue,HemocentrodeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received7December2014 Accepted12March2015 Availableonline3June2015
Keywords:
Platelettransfusion Hemolysis
ABOblood-groupsystem Bloodgroupincompatibility Hemolysinproteins
a
b
s
t
r
a
c
t
Objective:Brazilianlegislationhasrecentlysuggestedtheuseofthequalitativehemolysin test instead of isohemagglutinin titers as prophylaxis for acute hemolysis related to plasma-incompatibleplatelettransfusions.Theefficacyofthistestinpreventinghemolytic reactionshasneverbeenevaluatedwhileisohemagglutinintitershavebeenextensively studied.Themainobjectiveofthisstudywastoevaluatethecorrelationbetweentheresults ofthesetwotests.Theimpactofeachtypeofprophylaxisontheplateletinventory man-agementandtheabilityofthequalitativehemolysintesttopreventredcellsensitization afterthetransfusionofincompatibleunitswerealsostudied.
Methods:Atotalof246donorbloodsampleswereevaluatedusingbothisohemagglutinin titersandthequalitativehemolysintest,andtheresultswerestatisticallycompared. Subse-quently,600plateletunitsweretestedusingthehemolysinassayandthepercentageofunits unsuitablefortransfusionwascomparedtohistoricaldatausingisohemagglutinintiters (cut-off:100).Moreover,tenpatientswhoreceivedunitswithminorABOincompatibilities thatwerenegativeforhemolysisaccordingtothequalitativehemolysintestwereevaluated regardingthedevelopmentofhemolysisandredcellsensitization(anti-Aoranti-B).
Results:Isohemagglutinintitrationandtheresultsofqualitativehemolysintestdidnot cor-relate.Theroutineimplementationofthequalitativehemolysintestsignificantlyincreased thepercentageofplateletunitsfoundunsuitablefortransfusions(15–65%;p-value<0.001). Furthermorethequalitativehemolysintestdidnotpreventredbloodcellsensitizationina smallexploratoryanalysis.
Conclusion: Qualitativehemolysintestresultsdonotcorrelatetothoseofisohemagglutinin titersanditsimplementationastheprophylaxisofchoiceforhemolysisassociatedwith plasma-incompatibleplatelettransfusionslacksclinicalsupportofsafetyandsignificantly affectsplateletinventorymanagement.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:HemocentrodeSãoPaulo,AvenidaDr.EnéasdeCarvalhoAguiar,151,1◦Andar,CerqueiraCésar,05403-000
SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](C.L.Dinardo).
http://dx.doi.org/10.1016/j.bjhh.2015.05.001
Introduction
Thetransfusionofnon-ABOidenticalplateletsmaybe asso-ciated withacute hemolysis, fever, recipient inflammation and a decreased response in the post-transfusion platelet count.1TherearetwotypesofABOincompatibilities:(1)major, in which the recipient plasma is not compatible with the transfusedplatelets,asituationassociatedwithasuboptimal responsetothetransfusedproductand(2)minor,inwhichthe recipientisexposedtoABO-incompatibleplasmawhenthere isthe riskofacutehemolytictransfusionreactions.2Inthe routineofanybloodbank,thetransfusionofplatelets with minorABOincompatibilitiesisnotrareduetotheshortageof plateletconcentratesandthenumberofemergencyplatelet requestswhennoABOtypingisavailable.
The incidence of acute hemolysis due to plasma-incompatibleplatelettransfusionsislow(approximately50in every1,000,000incompatibletransfusions),3buttheseverityof theeventjustifiestheapplicationofprophylacticpolicies.The AmericanAssociationofBloodBanks(AABB)standardsstate thatthetransfusionserviceshallhaveapolicyconcerningthe transfusionofcomponentscontainingsignificantamountsof incompatibleABOantibodies.4Titrationofdonor isohemag-glutinins(anti-Aand/or anti-B)followed bythetransfusion ofincompatibleproductswithtitersbelow100isthe most studiedprophylacticmethodreportedintheliterature.1,5In spiteofthediscussionoverthesafestisohemagglutinintiter, thisstrategyhasalreadybeenevaluatedinlargestudieswhich demonstrateditsefficacyinpreventingacutehemolysisafter plasma-incompatibleplatelettransfusions.5–7
Recently,theBrazilianlegislationhassuggestedtheuseof thequalitativehemolysintest(QHT)insteadof isohemagglu-tinintiters(IT)asprophylaxisforacutehemolysissecondary toplasma-incompatibleplatelettransfusions.8Therationale istoidentify,withintheincompatiblesera,the presenceof antibodieswiththeabilityofcausingredbloodcell(RBC)lysis, therebyreducingthe risktobloodrecipients. Theproposed testhasthreepossibleresults:‘absenceofhemolysis’, ‘par-tialhemolysis’ and ‘total hemolysis’,withthe‘partial’ and ‘total’hemolysiscategoriesprecludingtransfusion.Inspiteof itsbiologicalplausibility,theefficacy oftheQHTin preven-tinghemolyticreactionsafterthetransfusionofproductswith minorABOincompatibilitieshasneverbeenevaluatedinthe literature,raisingconcernsaboutthesafetyofitsuse.
Thus,themainobjectiveofthisstudywastoevaluatethe correlation between isohemagglutinin titers (gold-standard prophylaxis)and the qualitative hemolysintest (suggested prophylaxis).Asecondaryobjectivewastoevaluatetheimpact ofeachtypeofprophylaxisonplateletinventorymanagement andthepresenceofRBCsensitizationbyanti-Aoranti-B anti-bodiesafterplasma-incompatibleplatelettransfusionstested negativeforhemolysis(absenceofhemolysis)byQHT.
Methods
Studydesign
ThisstudywasapprovedbythelocalEthicsCommittee (Fac-uldadedeMedicinadaUniversidadedeSãoPaulo#797.385).In
thefirststage,samplesobtainedfromtypeOplateletdonors betweenJanuary9,2014andSeptember30,2014were eval-uatedusingboththeQHTandITtechniques.TheQHTwas performedintheimmunohematologylaboratoryandtheIT wasmeasuredinthelaboratoryresponsibleforthe distribu-tionofplateletunits.Alldonorsampleswerecollectedusing tubes without anti-coagulantand the QHT was performed within6hofcollection.TheITwasperformeddirectlyfrom theseraofplateletunits.TheresultsofQHTandITwere sta-tisticallycomparedusingtheKruskal–Wallistest,Chi-square testandlogisticregression.Statisticalanalysiswasperformed usingtheSPSSsoftware(18thversion)andap-valuelessthan 0.05wasconsideredsignificant.
Inthesecondstageofthestudy,anexploratorysampleof tenpatientswho receivedminorABO-incompatible platelet transfusionswereevaluatedregardingthedirectantiglobulin test (DAT),lactatedehydrogenase(LDH)andindirect biliru-bin(IB)beforeand1hafterthetransfusionofplateletunits with negativeresultsfor hemolysisusing the QHT test. In the specific case of type O platelet units, only those pre-sentingabsenceofhemolysiswithbothtypeA1andBRBCs were included, irrespective ofthe recipients’ ABO type. All thepatientsweretransfusedinaday-hospitalregimenand patients were observedfor1h aftertheend oftransfusion forsignsandsymptomsofacutehemolysis:fever,darkurine, hypotensionandlumbarpain.Increasesof15%inLDHorIB levels were considered evidence ofhemolysis as this level exceedsthe analyticalvariability ofthelaboratoryforboth tests.
TheQHTwasalsoperformedinsamplesobtainedfromall plateletapheresisdonorsbetweenJuneandSeptember2014. Thepercentageofunitsclassifiedasunsuitablefor transfu-sionusingtheQHT(partialortotalhemolysis)wascompared tohistoricaldataofunitsclassifiedasunsuitablefor transfu-sionusingITwithacut-offof100(OlympusPK7200).These percentageswerecomparedusingtheChi-squaretest.
Acidelution
Acid elutionwas performedincasesofpositiveDAT using the DiaCidel® kit, according tomanufacturer’s instructions
(Biorad®).Briefly,theRBCsofrecipientswerewashedtentimes
with0.9%salinesolutionand1mLoftheelutionsolutionwas addedto1mLofwashedRBC.Themixturewascentrifuged and buffer solution was added tothe supernatant until it became blue. Theeluate wasthen testedwith commercial typeA1andBRBCs.
Isohemagglutinintitrationtechnique
Anti-Aand anti-Btitrationwasperformedintubes accord-ingtotheAABBTechnicalManual(18thversion).9Briefly,the serum of platelet units was sequentially dilutedin sterile salinesolutionfrom1:1until1:2048givingafinalvolumein eachcaseof100L.Thetiterswereaddedtoproperly
identi-fiedtubescontaining50LoftypeA1orBRBCs(Biorad®).After
representedbythehighesttiteratwhich1+hemagglutination wasobserved.
Qualitativehemolysintest
QHT was performed according to a previously published technique.10 AsBrazilianlawsuggestsperforming theQHT after15minofincubationat37◦C,thiswasthefirstmethod
used in the current study. However, a 30% rate of inter-observer disagreement was detected. In the literature, the equivalentQHTtechniqueuses45minofincubationatroom temperature. This was also employed in this study with-out any inter-observer disagreement. Briefly, freshtype A1 andBnon-commercial RBCs wereused toprepare3% sus-pensionsforthetests.Freshdonorsera(100L)wereadded
totubescontaining50LofspecificRBCsuspensions(type
A1and/orB).After45min-incubationatroomtemperature, thepresenceor absence ofhemolysiswasmacroscopically observedinthetubes.Thetestwasconsidered negativein theabsenceofhemolysis.Iftherewashemolysis,thetestwas consideredpositiveandclassifiedaspartialortotal hemol-ysis.Macroscopic evaluationofall sampleswasperformed byonetechnicianandconfirmed byasecond toavoidany interpretationbias.
Results
Correlationbetweenqualitativehemolysintestand isohemagglutinintitrationresults
Twohundredandforty-sixdonorswereevaluatedusingboth theQHLandITtechniques.OnusingtheQHT,61.38%ofdonors didnotexhibithemolysisand38.62%exhibitedeitherpartial (17.07%)ortotalhemolysis(21.54%).ByIT,85.8%and67.1%of plateletunitswereclassifiedaslow-titerconsideringcut-offs of1:128and1:64,respectively(Table1).
ThemedianvalueofITdidnotstatisticallydifferbetween the groups with different QHT results, either when they
Table1–Isohemagglutinintitersandthequalitative hemolysintestresultsofthestudysample.a
Qualitativehemolysintest Frequency Percent
Absenceofhemolysis 151 61.38 Partialhemolysis 42 17.07
Totalhemolysis 53 21.54
Presenceofhemolysis 151 61.38 Absenceofhemolysis 95 38.62
Isohemagglutinintiters(cut-off) Frequency Percent
<1:128 211 85.8
≥1:128 35 14.2
<1:64 165 67.1
≥1:64 81 32.9
a Theisohemagglutinintitertestwasperformedinplateletunits
inonespecificbloodbanklaboratoryresponsiblefortheir dis-tribution.Thus,thefrequenciesexhibitedherearenotthesame asthoseoftheoverallplateletunitsoftheinstitution,especially regardingthequalitativehemolysintest,duetonecessityof pro-vidingunitsnegativeforhemolysistopatients.
200
A
150
50
0
Isohemagglutinin tite
r
Absence of hemolysis
Absence of hemolysis Presence of hemolysis Partial
hemolysis
Total hemolysis
P=0.919
P=0.733
100
200
B
150
50
0
Isohemagglutinin tite
r
100
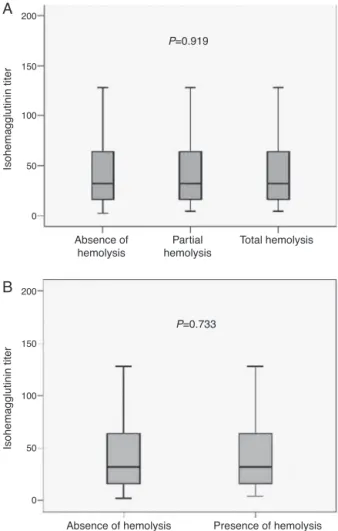
Figure1–Comparisonofthemedianvalueof
isohemagglutinintiters(IT)presentedbythegroupswith differentresultsinthequalitativehemolysintest(QHT). GroupsdidnotstatisticallydifferintermsofIT,inspiteof theirclassificationasabsenceofhemolysis,partial hemolysisandtotalhemolysis(p-value=0.919)(A)or
absenceofhemolysisandpresenceofhemolysis
(p-value=0.733)(B).Infact,themedianITwas32andthe
interquartilerangewas48forallanalyzedgroups.
were classified as absent, partial and total hemolysis (p-value=0.919) or whenthey were classified as absence and presenceofhemolysis(p-value=0.733)(Figure1).Infact,the medianvalueofITwas32andtheinterquartilerangewas48 inallanalyzedgroups.
Neithertitersabove64nortitersabove128werecorrelated totheriskofhemolysisaccordingtotheQHT(p-value=0.454 and 0.677, respectively)(Table2). Logisticregression analy-sisdemonstratedthattheITwasunabletopredicttheQHT results(p-value=0.702).
Evaluationoftheefficacyofthequalitativehemolysintest inpreventingredcellsensitization
Table2–Comparisonbetweenisohemagglutinintiters(IT)andqualitativehemolysintestresultsusingtheChi-square test.
Cut-off Qualitativehemolysintest Total p-value
Presenceofhemolysis Absenceofhemolysis
IT <1:128 127 84 211 0.677
≥1:128 24 11 35
Total 151 95 246
IT <1:64 103 62 165 0.454
≥1:64 48 33 81
Total 151 95 246
plasma-incompatibleplatelettransfusionswithnegativetest resultsforhemolysisusingtheQHT.Allthepatientsreceived less than 600mL of incompatible plasma and there were noincreasesinthelevels ofDHLor IBinany patientafter thetransfusion.OnepatientdevelopedanovelpositiveDAT afterthetransfusionandtheeluateanalysisconfirmedanti-B specificity(IT1:128)(Table3).Nosignsorsymptomsof trans-fusionreactionsweredetected.
Impactoftheimplementationofthequalitativehemolysin testonthebloodbankroutine
Sixhundredplateletunits(apheresisonly)werestudiedand thepercentageconsideredasunsuitablefortransfusiondueto minorABOincompatibilitywascalculated.Thepercentageof groupOplateletapheresisconsideredasunsuitablefor trans-fusionusingtheQHTwas65%and,basedonhistoricaldata, thepercentageofgroupOplateletunitsconsideredas unsuit-ablefortransfusionusingIT(cut-offof100)was15%(p-value <0.01).Thiswouldsignificantlyaffectplateletsupplyinblood banksinthecaseofminorABOincompatibility.Asthetest couldnotbeautomatized,QHTwasperformedmanuallyand onlyusingtheseraofapheresisdonors.
Discussion
ThepresentstudydemonstratesthattheresultsofIT,the gold-standardprophylaxisagainstthehemolysisassociatedwith plasma-incompatibleplatelettransfusions,arenotcorrelated totheresultsoftheQHT, therecentlyproposed prophylac-ticstrategy.Moreoverinanexploratoryanalysis,theabsence ofhemolysisinQHTdidnotpreventRBCsensitizationafter transfusionandtheimplementationofthisprophylaxisinthe bloodbankroutinenegativelyaffectedplateletinventory man-agementduetoasignificantincreaseinthenumberofunits classifiedasunsuitablefortransfusion.
IT has been the method of choice for the prophylaxis of hemolysis associatedwith plasma-incompatible platelet transfusions in most blood bank services, mainly due to reports of its safety in spiteof the fact that the best cut-offlevelremainselusive.5,6,11,12 TherationaleunderlyingIT prophylaxis is that incompatible transfused antibodies are diluted within the recipients’ organism due to the pres-ence of A and/or B antigens in epithelial tissues and in plasmaticproteins,besidesthe RBCmembrane.Thehigher the titer of isohemagglutinins, the greater the chances of RBCsensitizationandpassivehemolysis.13Otheralternatives
Table3–Overallcharacterizationofthepatientsincludingtheoutcomeafterplasma-incompatibleplatelettransfusions.
Case Transfusedplateletunits Patient
Typeof transfused
platelet
Transfused volume(mL)
%ofincompatible plateletunits(pool)
ABO/ RhD
QHT result
ABO/ RhD
Signsor symptomsof acutehemolysis
Post-transfusional
DAT
Increasein LDH/IB
1 Apheresis 250 O+ AH B+ No Negative No
2 Poolofrandom units
420 100 O− AH A− No Negative No
3 Poolofrandom units
360 100 O+ AH B+ No Negative No
4 Apheresis 250 O+ AH AB+ No Negative No
5 Apheresis 250 O+ AH B+ No Positive3+a No
6 Apheresis 250 A+ AH AB+ No Negative No
7 Poolofrandom units
300 100 O− AH B+ No Negative No
8 Apheresis 250 O+ AH A+ No Negative No
9 Apheresis 250 O+ AH A+ No Negative No
10 Apheresis 250 O+ AH A+ No Negative No
AH:absenceofhemolysis.
to this strategy are platelet washing, which is associated withdecreased transfusion efficacy,1 or the preparation of hyper-concentrated platelets re-suspended in an additive solutionduringstorage,whichismoretime-consumingand expensive.14
ItisimportanttostressthatgroupOblooddonorstypically presenthigherisohemagglutinintiters,athreattorecipients inthecaseofincompatible platelettransfusions.Similarly, apheresisplateletunitswithhigherisohemagglutinintiters aremoredangeroustoincompatiblerecipientsthanrandom plateletunits,astheirplasmacontentishigherandcannot bedilutedbeforetransfusion.Thus,performingITintypeO apheresisdonorsisavalidprophylacticstrategyusedbysome bloodbankstoavoidhemolyticreactionsfollowing plasma-incompatibleplatelettransfusions.Oneexceptiontothisrule isthe useofrandom units forthe transfusionofpediatric patients,asituationassociatedwithriskofhemolysis.
Inourservice,approximately2468transfusionsofplatelet unitsareperformedeachmonthand,ofthose,5%haveminor ABO incompatibilities. Since the implementation of IT as hemolysis prophylaxis ten years ago (cut-off level of100), no casesofacute hemolytic reactionshave been reported. Consideringacut-offlevelof128(tube-method),14.2%ofour typeOplateletunitswereconsideredashigh-titer,irrespective oftheABOtyping.Thisdataisconsistentwithotherreportsin theliterature,inwhichapproximately26.3%oftypeOplatelet unitsexhibit isohemagglutinin titersgreater than 256 (gel-method).5,13SinceITcanbeautomatized,ifacut-offlevelof 100ischosen,lessthan15%oftypeOplateletunitswillbe considered‘dangerous’inmosttransfusionservices,making iteasiertodealwithshortagesofplateletsandavoidingthe expiryofunits.
QHThasrecentlybeensuggestedasapossiblesubstitute toITasthe prophylaxisofchoiceforplasma-incompatible platelettransfusions.Therearetwotypesofhemolysintest: QHT and thequantitative hemolysintest, which measures thehemolysintiterandwasnotinthescope ofthis study. QHT evaluateswhether the anti-Aor anti-Bantibodies are capable,undertheworstconditions,ofcausingRBClysis.The objectiveofthistestisdifferenttothatofIT,which evalu-atesthetiterofanti-Aoranti-Bantibodiescapableofcausing RBCagglutination.Asdemonstratedbyourresults,ahigher titerofisohemagglutininsdoes notforesee thepresenceof hemolysinswithinonesample,andviceversa.
Even though the rationale underlyingthis recently pro-posedprophylacticmethodwasvalid(detectingthepresence ofanti-Aandanti-BantibodiescapableofcausingRBClysis indonorsera),itcompletelylackedevidenceofefficacyinthe literature.Thecurrentstudydemonstratesthatthereisno cor-relationbetweentheresultsofITandthoseofQHT.Hence, someplateletunitswithnegativeQHTresultsforhemolysis (suitablefortransfusion)exhibitedhighITandotherslowIT, consideringboththecut-offsof128and64.Asthesafetyof QHThadneverbeenclinicallyevaluated,incontrasttothatof IT,thisproposalisamatterofconcern.
Theresultsoftheexploratoryanalysisregardingtheability ofQHTtopreventRBCsensitizationshowedthat10%of recip-ientswho receivedunits withminorABO incompatibilities withnegativeQHT results forhemolysispresented a posi-tiveDATaftertransfusion.Eventhoughthestudysamplewas
small,duetoethicallimitations,thepercentageofRBC sen-sitizationwashigherthanthatreportedintheliteraturefor plasma-incompatibleplatelettransfusions(3.7%)withITtiters greaterthan512(gel-method).13Astheobjectofprophylaxisin plasma-incompatibleplatelettransfusionsistopreventacute hemolysis,whichisrare,alargecohortofpatientstransfused basedonQHTresultsaloneisnecessarytoprovetheclinical efficacy.
Theimplementation ofQHT caused somelogistic prob-lemstothebloodbankroutine.Itisknownfromtheliterature thatapproximately60%ofisohemagglutininsarecapableof causingRBC lysisand,asaconsequence,thepercentageof plateletunitslabeledasunsuitablefortransfusionafterthe implementationofthismethodologyinourservicewas sim-ilar toother publicationsat65%.15 Thisnegatively affected platelet inventory management and caused delays in the transfusionprocess.Moreover,anextrabloodsamplehadto becollected from donors,due tothenecessityof perform-ingQHTusingserainsteadofplasma,whichisthematerial commonlyavailableintheimmunohematologylaboratory.By collectingthisextratube,thevolumerecommendedby Brazil-ianlawregardingthemaximumauthorizedbloodvolumethat canbecollectedfortestingwasexceeded.8Finally,astheQHT couldnotbeautomatized,itwasperformedmanuallyby tech-nicians,therebyincreasingthechancesofmistakes.
This study has some limitations. The most important concerns the number of recipients transfused with non-compatible plateletunits basedonQHTresults, whichwas low.OurmainobjectivewastocorrelateQHTandITresults, withthe evaluationofRBC sensitizationas secondary.The idealstudydesigntoevaluatetheefficacyofQHTin preven-tinghemolyticreactionsshouldinvolveatleast5000patients. However, considering the lackof correlation between QHT and IT, the absence ofstudies in the literatureaddressing theefficacyofQHTinpreventinghemolyticreactions, prob-lemsrelatedtoplateletinventorymanagementusingtheQHT routineandtheprovenefficacyofITinpreventinghemolytic complications,enrollingmorepatientstobetransfusedbased onlyonQHTresultswouldbeagainstethicalprinciples.
Conclusions
QHT results do not correlate to IT and the implementa-tion ofthis technique asthe prophylaxisofchoiceagainst thehemolysisassociatedwithplasma-incompatibleplatelet transfusionslacksclinicalsupportofsafetyandwould signif-icantlyaffectplateletinventorymanagement.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DunbarNM,OrnsteinDL,DumontLJ.ABOincompatible
platelets:risksversusbenefit.CurrOpinHematol.
2. CoolingL.ABOandplatelettransfusiontherapy.
Immunohematology.2007;23(1):20–33.
3. MenisM,IzurietaHS,AndersonSA,KroppG,HolnessL,Gibbs
J,etal.Outpatienttransfusionsandoccurrenceofserious
noninfectioustransfusion-relatedcomplicationsamongUS
elderly,2007–2008:utilityoflargeadministrativedatabasesin
bloodsafetyresearch.Transfusion.2012;52(9):1968–76.
4. AABB.Standardsforbloodbanksandtransfusionservices.
Bethesda:AABB;2009.
5. BerseusO,BomanK,NessenSC,WesterbergLA.Risksof
hemolysisduetoanti-Aandanti-Bcausedbythetransfusion
ofbloodorbloodcomponentscontainingABO-incompatible
plasma.Transfusion.2013;53Suppl.1:114S–23S.
6. QuillenK,SheldonSL,Daniel-JohnsonJA,Lee-StrokaAH,
FlegelWA.Apracticalstrategytoreducetheriskofpassive
hemolysisbyscreeningplateletpheresisdonorsforhigh-titer
ABOantibodies.Transfusion.2011;51(1):92–6.
7. CoolingLL,DownsTA,ButchSH,DavenportRD.Anti-Aand
anti-BtitersinpooledgroupOplateletsarecomparableto
apheresisplatelets.Transfusion.2008;48(10):2106–13.
8. DiarioOficialdaUnião(DOU)PortariaN◦2.712,de12de
novembrode2013.Redefineoregulamentotécnicode procedimentoshemoterápicos.
9.FungMK,editor.AABBtechnicalmanual.18thed.Bethesda:
AABB;2014.
10.Brasil,MinistériodaSaúde.Técnicoemhemoterapia:livro
texto/SecretariadeGestãodoTrabalhoedaEducac¸ãona
SaúdeDepartamentodeGestãodaEducac¸ãonaSaúde.
Brasília:MinistériodaSaúde;2013,292pp.
11.SadaniDT,UrbaniakSJ,BruceM,TigheJE.Repeat
ABO-incompatibleplatelettransfusionsleadingtohaemolytic
transfusionreaction.TransfusMed.2006;16(5):375–9.
12.JosephsonCD,CastillejoMI,GrimaK,HillyerCD.
ABO-mismatchedplatelettransfusions:strategiestomitigate
patientexposuretonaturallyoccurringhemolyticantibodies.
TransfusApherSci.2010;42(1):83–8.
13.KarafinMS,BlaggL,TobianAA,KingKE,NessPM,SavageWJ.
ABOantibodytitersarenotpredictiveofhemolyticreactions
duetoplasma-incompatibleplatelettransfusions.
Transfusion.2012;52(10):2087–93.
14.PerseghinP.Highconcentrationplasma-reduced
plateletapheresisconcentrates.TransfusApherSci.
2011;44(3):273–6.
15.KhampanonK,ChanprakopT,SriwanitchrakP,SetthakarnM,
OotaS,NathalangO.ThecharacteristicsofABOantibodiesin