www.jped.com.br
ORIGINAL ARTICLE
Association between morphometric variables and
nocturnal desaturation in sickle-cell anemia
夽
Cristina Salles
∗, Marcelo Bispo, Regina Terse Trindade-Ramos
Faculdade de Medicina, Universidade Federal da Bahia (UFBA), Salvador, BA, Brazil
Received 16 September 2013; accepted 17 December 2013 Available online 28 March 2014
KEYWORDS Sickle-cell anemia; Desaturation; Maxilla; Mandible; Sleep apnea
Abstract
Objective: to evaluate associations between morphometric variables, cervical circumference (CC), and abdominal circumference (AC) with the presence of nocturnal desaturation in children and adolescents with sickle-cell anemia.
Methods: all patients were submitted to baseline polysomnography, oral cavity measurements (maxillary intermolar distance, mandibular intermolar distance, and overjet), and CC and AC measurements.
Results: a total of 85 patients were evaluated. A positive correlation was observed between the height/age Z-score and CC measurement (r = 0.233, p = 0.031). The presence of nocturnal desaturation was associated with CC (59.2±9.3vs. 67.5±10.7, p = 0.006) and AC measurements (27.0±2.0vs. 29.0±2.1, p = 0.028). There was a negative correlation between desaturation and maxillary intermolar distance (r = -0.365, p = 0.001) and mandibular intermolar distance (r = -0.233, p = 0.037).
Conclusions: the morphometric variables of CC and AC may contribute to raise suspicion of nocturnal desaturation in children and adolescents with sickle-cell anemia.
© 2014 Sociedade Brasileira de Pediatria. Published by Elsevier Editora Ltda. All rights reserved.
PALAVRAS-CHAVE Anemia falciforme; Dessaturac¸ão; Maxila; Mandíbula; Apneia do sono
Associac¸ão entre variáveis morfométricas e dessaturac¸ão noturna na anemia falciforme
Resumo
Objetivo: avaliar associac¸ões entre variáveis morfométricas e circunferências cervical (CC) e abdominal (CA) com a presenc¸a de dessaturac¸ão noturna em crianc¸as e adolescentes com anemia falciforme.
夽
Please cite this article as: Salles C, Bispo M, Trindade-Ramos RT. Association between morphometric variables and nocturnal desaturation in sickle-cell anemia. J Pediatr (Rio J). 2014;90:420---5.
∗Corresponding author.
E-mail:[email protected] (C. Salles).
http://dx.doi.org/10.1016/j.jped.2014.01.005
Métodos: todos os pacientes foram submetidos à polissonografia basal, medidas da cavidade oral (distância intermolar da maxila, distância intermolar da mandíbula eoverje), CC e CA.
Resultados: foram avaliados 85 pacientes. Foi observada correlac¸ão positiva entre o escore Z altura/idade e a medida da circunferência cervical (r = 0,233 p = 0,031). A presenc¸a da dessaturac¸ão noturna associou-se com as medidas da circunferência cervical (59,2 + 9,3vs67,5 + 10,7; p = 0,006) e abdominal (27,0 + 2,0vs29,0 + 2,1; p = 0,028). Houve correlac¸ão negativa entre a dessaturac¸ão e a distância entre os segundos molares da maxila (r = - 0,365, p = 0,001) e da mandíbula (r = - 0,233, p = 0,037).
Conclusões: as variáveis morfométricas e circunferências cervical e abdominal podem con-tribuir para a suspeita da dessaturac¸ão noturna em crianc¸as e adolescentes com anemia falciforme.
© 2014 Sociedade Brasileira de Pediatria. Publicado por Elsevier Editora Ltda. Todos os direitos reservados.
Introduction
The main aspect of sickle-cell anemia (SCA) physiopathology is the vaso-occlusive crisis, also called a painful crisis, result-ing from the polymerization of hemoglobin S that causes red blood cells to assume a ‘‘sickle’’ shape, resulting in the obstruction of small-caliber blood vessels, tissue hypoxia, necrosis, and severe pain.1
Among the consequences of red blood cell sickling are painful vaso-occlusive crises, stroke,2and chronic hemolytic
anemia.3Pulmonary complications account for 20% to 30%
of deaths in adults with SCA, followed the pulmonary lesions caused by upper airway (UA) obstruction.4
Regarding children with SCA, an important causal factor of airway obstruction is adenotonsillar hypertrophy (ATH). Salles et al.5 observed a prevalence of 55.3% of
obstruc-tive ATH in children and adolescents with SCA. When this UA obstruction is associated with obstructive sleep apnea syn-drome (OSAS), it can precipitate episodes of hypoxemia,6
increasing the risk of vaso-occlusive crises.7
The nocturnal arterial oxyhemoglobin desaturation in SCA occurs in up to 83% of children with the disease, and may result from OSAS or pulmonary disease, or may be sec-ondary to the decreased oxygen affinity of hemoglobin S.8
Oxyhemoglobin desaturation is common during sleep, which is associated with hypoventilation and is exacerbated by UA obstruction;6in patients with SCA, there may be increased
risk for airway obstruction due to ATH.9
Factors that worsen UA obstruction are ATH and the cra-niofacial consequences caused by obstructive ATH itself, such as predominant mouth breathing; vertical, horizontal, and transverse maxillary alterations, incompetent lip seal; and unbalanced orofacial muscles, mainly the mandibular elevator and depressor muscles.10,11
Thus, the present study aimed to evaluate associations between morphometric variables, cervical circumference (CC), and abdominal circumference (AC) with the presence of nocturnal desaturation in children and adolescents with SCA.
Material and Methods
This was a cross-sectional, contemporary cohort study with sequential allocation of 85 patients with SCA enrolled in a referral center for hematology and transfusion medicine,
between May of 2007 and May of 2008. The following inclu-sion criteria were used: diagnosis of SCA attained through the quantitative analysis of hemoglobin by hemoglobin electrophoresis or high-performance liquid chromatography (HPLC), performed with Variant II equipment (Bio-Rad, USA); age between 2 and 19 years; clinically stable; completed the questionnaire; allowing pediatric and otorhinolaryngologi-cal evaluation; and undergoing nocturnal polysomnography. The following exclusion criteria were used: other genetic syndromes, debilitating diseases, acute hepatitis, previous treatment for OSAS or recent craniofacial trauma; using hypnotic drugs; having been treated with corticosteroids; pregnancy; and presence of infection during the evaluation. The PEPI-Sample program (Sagebush Press,USA) was used to calculate sample size, and the following parameters were used: a confidence level of 95%, and the prevalence of OSAS in children/adolescents of 5% (4.9% as an acceptable preva-lence difference).
The sample was obtained from a population of approxi-mately 1,000 children and adolescents with SCA, registered at a referral center for hematology and transfusion medicine. Therefore, to meet the objectives, the calculated sample size consisted of 71 patients. Considering 10% losses, the total (n) consisted of 78 patients.
Age was measured in full years, according to the birth date. Ethnicity was self-reported, according to the official nomenclature of demographic censuses, using skin color as reference (white, mixed-race, or black).
Weight was measured using a mechanical scale (model 131; Filizola - Brazil). Length was measured with a stadiome-ter. These measurements were compared to the growth charts of the National Center for Health Statistics and con-verted into Z-scores for body mass index (BMI), weight/age, and height/age based on age and gender, using the Epi-Info software (release 3.4.1;CDC- USA).
Another compass was used to obtain the oral cavity mea-surements (maxillary intermolar distance, defined as the size of the maxilla; and mandibular intermolar distance, defined as mandibular size), which were then transposed to a ruler. To measure the OJ, a 40- mm ruler was used; to measure CC, a metric tape was placed at the cricothyroid membrane, and for AC, the same tape was used, after being placed at the umbilicus.10
Patients were submitted to polysomnography, accompa-nied by a parent or guardian, for at least 10 h, in a quiet environment, with appropriate temperature and lighting for the examination. This was performed during spontaneous sleep, with no prior sedation or sleep deprivation, avoiding stimulating foods (coffee, chocolate, soda, and black tea). Polysomnography was conducted in a hospital setting, using Sonolab 620 computerized equipment (Medtron - Brazil), and the report was issued by the same observer. The following were recorded during the polysomnography: EEG (C4-A1, C3-A2, O2-A1, and O1-A2), electro-oculogram, electromyogram of anterior tibial and chin nerves, and electrocardiogram.
Respiratory movements were assessed through thoracic and abdominal band, and SpO2 by pulse oximetry. An
oronasal cannula and thermistor were used to measure nasal airflow, in addition to a microphone placed in the neck to record snoring.
The American Thoracic Society11 provides the following
definition and the following criteria for the apnea-hypopnea index (AHI) in children: it corresponds to the sum of the number of obstructive and mixed apneas, and obstructive and mixed hypopneas; it must be expressed in events per hour; to calculate this number, the total sleep time must be used, and it is considered abnormal when AHI≥1 event per hour of sleep. Hypopnea was defined as a reduction > 50% of the flow amplitude associated with a microarousal and/or reduction > 3% of baseline oxygen saturation.
As for the apnea index (AI), the following assumptions were followed: the number of obstructive and mixed apneas (mixed apneas are initially central and can become obstruc-tive at the end of the event), lasting at least two respiratory cycles, which was expressed as events per hour; for the calculation, the total sleep time must be used, and it is considered abnormal when AI≥1 event per hour of sleep. Microarousal was defined as an abrupt change in the elec-troencephalogram frequency lasting 3 s, preceded by at least 10 s of sleep. Nocturnal desaturation was defined as patients who had more than 30% of total sleep time with peripheral oxygen saturation (SpO2) < 90%.
The project was approved by the research ethics com-mittee of the institution (Protocol 197; Opinion 98/2006). Parents or guardians signed the informed consent after agreeing to participate in the study.
Statistical Analysis
The SPSS statistical program (released 2012,USA) was used for data tabulation and analysis. Quantitative variables were expressed as mean ± standard deviation or median and interquartile range. Qualitative variables were expressed as absolute and relative frequencies. Student’s t-test for independent samples or the Mann-Whitney test was used to compare two means. Spearman’s test was used to test the
correlation between variables. The level of significance was set at 5% (p < 0.05).
Results
A total of 85 patients were evaluated, of whom 58.8% were males. Regarding ethnicity, 71.8% self-reported as mixed-race, 20% as black, and 8.2% as white. Table 1 shows the clinical profile of children and adolescents with SCA. There was no statistically significant difference between the mean ages, as it was 9±4 years in the apneic group and 9±3 years in the non-apneic group. The classification of pharyngeal and palatine tonsils in this sample, as well as their frequencies, are described by Salles et al.5
The distribution of polysomnographic data is shown in Table 2. There was no association between OSAS and the variables: ethnicity, gender, age, BMI Z-score, and height/age Z-score.
Of the 85 patients who were submitted to polysomno-graphy, only nine had AHI≥ 1 (events per hour of sleep), characterizing OSAS. Nocturnal desaturation was observed in 69 patients (81.2%), as reported in a previous study.12The
number of events per hour of sleep showed a mean of 13, ranging from 1.5 to 29 in the group of patients with apnea, and a mean of five, ranging from one to 11 events per hour of sleep in the non-apneic group.12
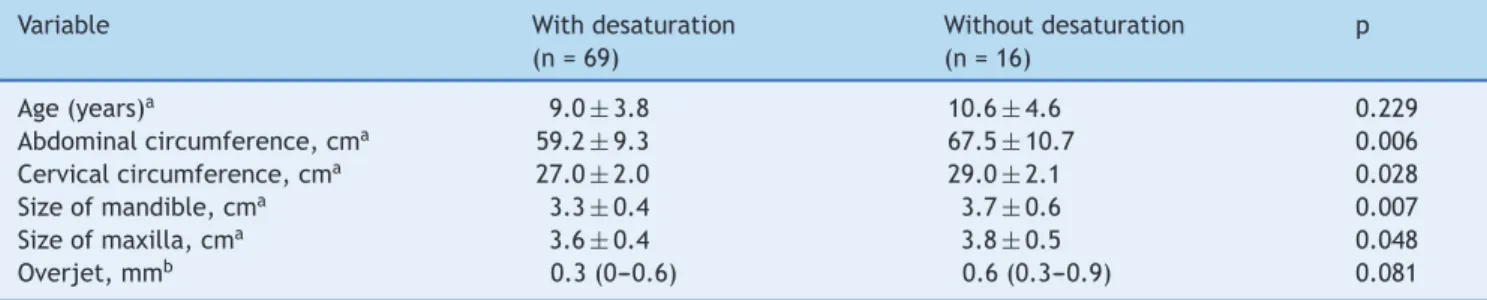
Table 3 shows the association between nocturnal desat-uration and CC and AC, as well as maxillary and mandibular measurements.
In this sample, measurements of CC and AC, as well as maxillary, mandibular, and overjet measurements were cor-related with nocturnal desaturation values obtained during the polysomnography using Spearman’s test (Table 4).
Discussion
The positive correlation between height/age Z-score and CC observed in the present study is in agreement with the literature, since studies have demonstrated that sickle-cell anemia patients younger than 18 have height deficit, when compared to normal children;13,14 the growth curve
alterations in these children may be associated with UA obstruction and obstructive events during sleep, and, conse-quently, with the decrease in growth hormone release.15Bar
et al.16compared the insulin-like growth factor I in children
with UA obstruction due to ATH, before and after submitting them to adenotonsillectomy. Prior to surgery, insulin-like growth factor I showed a mean value of 146.3 ng/mL and after surgery, it increased to 210.3 ng/mL (p < 0.01), while the disordered breathing index was within the normal range. In the present study, nocturnal desaturation in children and adolescents with SCA was associated with CC. One of the key structures for breathing is the laryngeal tract, which is located in the cervical region and, in the child, is shaped like a funnel, narrowing from the vocal folds to the subglottic region.17As the child grows, there is an expansion
of the subglottic area,15 and the thyroid cartilage, which
appears adjacent to the hyoid bone at birth, will move away from the latter in the craniocaudal direction.17 Therefore,
Table 1 Comparison of clinical data of apneic and non-apneic children and adolescents with sickle-cell anemia.
Variable Apneic
(n = 9)
Non-apneic (n = 76)
pa
Age, years 9±4 9±3 0.818
Mean annual hemoglobin, g/dL 7.6±0.6 7.9±2 0.295
Z-score for body mass index -0.4 (-2.8-0.5) -1.0 (-2.2 to -0.2) 0.875
Z-score for height/age -0.5 (-1.7-0.9) -0.7 (-1.4 to -0.1) 0.775
Episodes of pain in the last 12 months, n 12(3-26) 20(4-60) 0.936
Size of pharyngeal tonsils, % of cavum occupancy 90(25-95) 60(40-70) 0.135
Data shown as mean±standard deviation or median (interquartile range).
a Student’s test.
Table 2 Comparison of polysomnographic data using quantitative variables of apneic and non-apneic children and adolescents with sickle-cell anemia.
Variable Apneic
(n = 9)
Non-apneic (n = 76)
p
TST, Mina 332±79 368±63 0.223
AHI (events/h of sleep)a 1.3 (1.9---5.1) 0 (0---0) 0.000
Micro-arousals, events/h of sleepa 57 (30---147) 43 (29---67) 0.145
Desaturations, events/h of sleepa 13 (1.5---29) 5 (1---11) 0.083
Time of SpO2< 90%a,b 10 (1---29) 0.6 (0.1---4.9) 0.105
Time of SpO2< 80%a,c 0.1 (0---2) 0 (0---0) 0.021
Data shown as median (interquartile range). AHI, apnea-hypopnea index.
a Mann-Whitney test.
b Percentage of total sleep time (TST) in which oxygen saturation (SpO
2) was less than 90%. c Percentage of total sleep time in which SpO
2was less than 80%.
Table 3 Comparison of the morphometric variables between children with and without desaturation.
Variable With desaturation
(n = 69)
Without desaturation (n = 16)
p
Age (years)a 9.0±3.8 10.6±4.6 0.229
Abdominal circumference, cma 59.2±9.3 67.5±10.7 0.006
Cervical circumference, cma 27.0±2.0 29.0±2.1 0.028
Size of mandible, cma 3.3±0.4 3.7±0.6 0.007
Size of maxilla, cma 3.6±0.4 3.8±0.5 0.048
Overjet, mmb 0.3 (0---0.6) 0.6 (0.3---0.9) 0.081
a Student’s test. b Mann-Whitney.
Table 4 Correlation between morphometric variables and nocturnal desaturation in children and adolescents with sickle-cell anemia.
Morphometric variables R p
Cervical circumferencevs. nocturnal desaturationa -0.278 0.012
Abdominal circumferencevs. nocturnal desaturationa -0.188 0.092
Overjetvs. nocturnal desaturationa -0.178 0.115
Size of mandiblevs. nocturnal desaturationa -0.233 0.037
Size of maxillavs. nocturnal desaturationa -0.365 0.001
Z-score height/agevs. cervical circumferencea 0.233 0.031
and the greater the chance that a child with sickle-cell anemia will have oxyhemoglobin desaturation at night, which, combined with the fact that 55.3% of these children had obstructive ATH,5 contribute to the obstruction of the
UAs and corroborate the finding that up to 83% of chil-dren with sickle-cell anemia have nocturnal desaturation.
18
In this study, obesity was not a contributing factor to air-way obstruction. Children and adolescents with sickle-cell disease are not characterized by obesity or overweight; on the contrary, most children were within the normal weight range. The literature has drawn attention to the measure-ment of CC in children≥29 cm at the prepubertal age, which is associated with overweight and obesity.19 The degree of
desaturation in an apnea event is known to be correlated with the degree of obesity expressed as BMI.20 As children
and adolescents with SCA did not have such characteristics, but showed nocturnal desaturation, there is a clear need to perform future studies with imaging and polysomnography assessment to evaluate the characteristics of the cervical region in this population.
In the present study, children and adolescents with SCA who had nocturnal desaturation also had lower maxillary and mandibular measures, demonstrating a positive correlation between the maxilla and mandible with nocturnal desatu-ration. It is known that obstructive ATH can alter the oral cavity anatomy and that it is the main cause of UA obstruc-tion in children.21
Studies have demonstrated that at birth, the craniofacial skeleton of a North-American individual corresponds to 60% of the adult head size; at 8 months, it corresponds to 80%; at 3 years, to 90%; and at 9 years, it reaches 95% of the adult size.22 As a consequence, the individual may develop
high palate, narrow dental arches, and mandibular retrac-tion. These structures start to occupy the tongue space and force the tongue back toward the posterior oropharynx.23
Moreover, patients with reduced mandibular and maxillary dimensions have a tendency to have UA lumen restriction, as the tongue moves toward the posterior pharyngeal wall, as well as the soft palate and tissues in the oral cavity,24
result-ing in the collapse of the UAs when in a state of hypotension of the pharyngeal abductor muscles during sleep, favoring oxyhemoglobin desaturation.24
AC is usually used as an indicator of central obesity, which is typically observed in adults with OSAS.21However, in this
study, children and adolescents with nocturnal desaturation had lower AC measurements. As the evaluated sample was not characterized by obesity or overweight, AC measure-ment may be influenced by the increased liver and spleen volumes, characteristic of SCA.
It is known that, in patients with SCA, oxyhemoglobin desaturation does not necessarily means hypoxemia, as it may correspond to decreased arterial oxygen content, probably due to the presence of carboxyhemoglobin and methemoglobin, as well as decreased affinity of Hb S for oxygen, even with normal SpO2.25
Although the present study did not aim to evaluate patients with SCA by polysomnography and blood gas anal-ysis, it draws attention to future studies involving this association.
Finally, it was observed that the morphometric variables and CC may contribute to raise the suspicion of
noctur-nal desaturation in children and adolescents with sickle-cell anemia.
Funding
Fundac¸ão de Amparo à Pesquisa do Estado da Bahia ---FAPESB.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Thornton JB, Sams DR. Preanesthesia transfusion and sickle cell anemia patients: case report and controversies. Spec Care Den-tist. 1993;13:254---7.
2. Pauling L, Itano HA, Singer JS, Wells IC. Sickle cell anemia, a molecular disease. Science. 1949;110:543---8.
3. Zago MA, Pinto AC. The pathophysiology of sickle cell disease: from the genetic mutation to multiorgan dysfunction. Rev Bras Hematol Hemoter. 2007;29:207---14.
4. Moreira GA. Respiratory repercussions of sickle cell anemia. J Bras Pneumol. 2007;33:18---20.
5. Salles C, Ramos RT, Daltro C, Nascimento VM, Matos MA. Associa-tion between adenotonsillar hypertrophy, tonsillitis and painful crises in sickle cell disease. J Pediatr (Rio J). 2009;85:249---53. 6. Block AJ, Boysen PG, Wynne JW, Hunt LA. Sleep apnea, hypop-nea and oxygen desaturation in normal subjects. A strong male predominance. N Engl J Med. 1979;300:513---7.
7. Robertson PL, Aldrich MS, Hanash SM, Goldstein GW. Stroke associated with obstructive sleep apnea in a child with sickle cell anemia. Ann Neurol. 1988;23:614---6.
8. Kaleyias J, Mostofi N, Grant M, Coleman C, Luck L, Dampier C, et al. Severity of obstructive sleep apnea in children with sickle cell disease. J Pediatr Hematol Oncol. 2008;30:659---65. 9. Wittig RM, Roth T, Keenum AJ, Sarnaik S. Snoring,
day-time sleepiness, and sickle cell anemia. Am J Dis Child. 1988;142:589.
10. Soares MC, Bittencourt LR, Zonato AL, Gregório LC. Appli-cation of the Kushida morphometric model in patients with sleep-disordered breathing. Rev Bras Otorrinolaringol. 2006;72:541---8.
11. American Thoracic Society/American Sleep Disorders Associa-tion. Statement on health outcomes research in sleep apnea. Am J Respir Crit Care Med. 1998;157:335---41.
12. Salles C, Ramos RT, Daltro C, Barral A, Marinho JM, Matos MA. Prevalence of obstructive sleep apnea in children and adolescents with sickle cell anemia. J Bras Pneumol. 2009;35:1075---83.
13. Phebus CK, Gloninger MF, Maciak BJ. Growth patterns by age and sex in children with sickle cell disease. J Pediatr. 1984;105:28---33.
14. Platt OS, Rosenstock W, Espeland MA. Influence of sickle hemoglobinopathies on growth and development. N Engl J Med. 1984;311:7---12.
15. Valera FC, Demarco RC, Anselmo-Lima WT. Obstructive sleep apnea syndrome (OSAS) in children. Rev Bras Otorrinolaringol. 2004;70:232---7.
17. Braga JN. Freqüência fundamental de 100 crianc¸as de 6 a 8 anos de Belo Horizonte [dissertation]. Rio de Janeiro: Universidade Veiga de Almeida; 2007.
18. Spivey JF, Uong EC, Strunk R, Boslaugh SE, DeBaun MR. Low daytime pulse oximetry reading is associated with nocturnal desaturation and obstructive sleep apnea in children with sickle cell anemia. Pediatr Blood Cancer. 2008;50:359---62.
19. Hatipoglu N, Mazicioglu MM, Kurtoglu S, Kendirci M. Neck cir-cumference: an additional tool of screening overweight and obesity in childhood. Eur J Pediatr. 2010;169:733---9.
20. Uchiyama LN, Magalhães CC, Durval MR, Pinho HA, Oliveira LV. Estudo da dessaturac¸ão da oxihemoglobina durante o sono em pacientes portadores de insuficiência cardíaca congestiva. IX Encontro Latino Americano de Iniciac¸ão Científica, V Encontro Latino Americano de Pós-Graduac¸ão --- Universidade do Vale do
Paraíba. [cited 13 Jul 2013]. Available from: http://www. inicepg.univap.br/cd/INIC 2005/epg/EPG4/EPG4-37%20ok.pdf 21. Guilleminault C. Obstructive sleep apnea syndrome and its
treatment in children: areas of agreement and controversy. Pediatr Pulmonol. 1987;3:429---36.
22. Meredith HV. Growth in head width during the first twelve years of life. Pediatrics. 1953;12:411---29.
23. Palmer B. Snoring and sleep apnea: how it can be prevented in childhood. Das Schlafmagazin. 2005;3:22---3.