w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Langerhans’
cell
histiocytosis
diagnosed
due
to
dermatological
perianal
lesion
Bruno
Lorenzo
Scolaro
a,b,
Gustavo
Becker
Pereira
a,b,
Daniel
Cury
Ogata
c,d,
Fernanda
Souto
Padrón
Figueiredo
Vieira
da
Cunha
a,
Ana
Cristina
Martins
Effting
e,∗,
Rafael
Oselame
Guanabara
eaUniversidadedoValedoItajaí,DepartamentodeCirurgia,Itajaí,SC,Brazil
bSociedadeBrasileiradeColoproctologia,Brusque,SC,Brazil
cUniversidadedoValedoItajaí,DisciplinaAnatomiaPatológica,Itajaí,SC,Brazil
dSociedadeBrasileiradePatologia,Brusque,SC,Brazil
eUniversidadedoValedoItajaí,FaculdadedeMedicina,Itajaí,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1September2016 Accepted27March2017 Availableonline10May2017
Keywords: CD1antigens Langerhans’cells
Langerhans’cellhistiocytosis HistiocytosisX
Vinblastine
a
b
s
t
r
a
c
t
Langerhans’cellhistiocytosisisararediseasecharacterizedbyproliferationofLangerhans cellsinthebody.Itaffectsmainlymales,predominantlyinchildhood.Ulceratedplaques areoneofthecutaneousformsofpresentation.Diagnosticconfirmationisdonethrough immunohistochemistry.Astherapeuticoptions,topicalcorticosteroidsandchemotherapy aregoodchoices.Thecaseisreportedofamalepatient,aged14,withperianal ulcera-tion.Heconsultedacoloproctologist,whoperformedabiopsyoftheregionandstarted localtriamcinoloneapplications.ImmunohistochemistrydiagnosedLangerhans’cells his-tiocytosis.Furtherinvestigationrevealeddiabetesinsipidus,osteolyticlesionsintheskull andlowerlimbs,enlargedliver,andencephalicalterations.Chemotherapywasstartedwith Vinblastine,withsignificantimprovementofthelesions.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Histiocitose
de
células
de
Langerhans
diagnosticada
por
lesão
perianal
dermatológica
Palavras-chave: AntígenosCD1 CélulasdeLangerhans Histiocitosedecélulasde Langerhans
r
e
s
u
m
o
AhistiocitosedecélulasdeLangerhanséumadoenc¸araracaracterizadapelaproliferac¸ão decélulasdeLangerhansnocorpo.Adoenc¸aafetaprincipalmenteoshomens, predomi-nantementenainfância.Placasulceradassãoumadasformascutâneasdeapresentac¸ão.A confirmac¸ãodiagnósticaéfeitaatravésdeanáliseimuno-histoquímica.Comoopc¸ões ter-apêuticas,corticosteroidestópicosequimioterapiasãoboasescolhas.Ocasoaquirelatado édeumpacientedosexomasculino,comidadede14anos,comulcerac¸ãoperianal.Ele
∗ Correspondingauthor.
E-mail:[email protected](A.C.Effting).
http://dx.doi.org/10.1016/j.jcol.2017.03.007
HistiocitoseX Vinblastina
consultouumcoloproctologista,querealizouumabiópsiadaregiãoeiniciouotratamento comaplicac¸õeslocaisdetriancinolona. Aanálise imunohistoquímicadiagnosticou his-tiocitosedecélulasde Langerhans.Outrosexamesrevelaram diabetesinsipidus,lesões osteolíticasnocrânioenosmembrosinferiores,aumentodofígadoealterac¸õesencefálicas. Aquimioterapiafoiiniciadacomvimblastina,commelhorasignificativadaslesões.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Histiocytosiscorrespondstoagroupofproliferativediseases relatedtohistiocytes,cells originatinginthebonemarrow. The first description of the disease was in 1939.1 A rare, little-known disease, it is characterizedby proliferation of Langerhans’cellsinvarioustissues.ThetermhistiocytosisX wasproposedbyLichtensteinin1953,2tocombinethethree formsofthediseasethathadbeendescribedupuntilthen: (1)EosinophilicGranuloma;(2)Hand-Schüller-Christian dis-ease;and(3)Letterer-Siwedisease.Thesethreeformsofthe diseaseexhibitthe histiocytesofLangerhans’asaprimary proliferativecellinwhichtheBirbeckgranuleis characteris-tic,evidencedbyelectronmicroscopy.Immunohistochemical analysisofthesecellsispositiveforantigensidenticaltothose foundinLangerhans’ cells,including theprotein S100and CD1a.3–5
In1987,withthecreationoftheInternationalHistiocyte Society,histiocytosisweregroupedintothreemajorclasses. ClassIwascalledhistiocytosisofLangerhanscells,replacing thedifferentnomenclatureshistoricallyused:histiocytosisX, eosinophilicgranuloma,Hand-Schüller-Christiansyndrome, Letterer-Siwe disease and Hashimoto-Pritzker syndrome.3 TheaetiologyofLangerhanscellhistiocytosisisstill uncer-tain,but someauthors havesuggestedthe possibility that itoriginatesinimmunehypersensitivityreactions,intestinal malabsorption,or pituitarydysfunction, orautoimmune or inflammatoryorigin.5Studiesdifferastotheprevalenceofthe diseasebetweensexes,andinsomestudies,aslight predilec-tionformaleswasobserved.Itcanoccuratanyage,butthe incidenceinchildhoodishigher.3,5–7
During the course ofthe disease, many organs may be involved,withbone,skinandlymphnodesbeingmost com-monsites.Thetreatmentvariesdependingontheextentand severityofthecase.8 Thediseaseresolvespontaneously,or mayevolve,leadingtoimpairedfunctionofvitalorgans,with severeorfatalconsequences.Recentstudieshavesuggested therapeuticregimensinvolvingvinblastineoretoposide, asso-ciatedwithcorticosteroidtherapy.Thelackofresponseafter sixweeksoftherapeutictreatmentisasignofpoorprognosis andoftheneedforcombinedtherapywithmoreaggressive regimens.3,6,8,9
InBrazil,reportsofLangerhans’cellhistiocytosiswith peri-analmargininvolvementarerare.10
TheaimofthisstudyistoreportacaseofLangerhans’ cellhistiocytosisdiagnosedduetoperianalskinlesionsthat presentedafavourableoutcomeafterinstitutionoftherapy.
Case
report
Male patient,aged14 years,bornand raisedinNavegantes –SantaCatarina,withsymptomsofdiffuseabdominalpain andpolydipsia.Hewastakentothepaediatrician,whoafter examiningthe patient’s medicalhistoryand anon-specific physicalexamination,foundnochanges.Theclinical symp-tomspersistedforoneyear,whenfacialoedemaandjaundice wereobserved.Concomitantly,thepatientbegantocomplain ofhaemorrhoids,and consultedacoloproctologyservicein hiscity.
Onphysicalexamination,analinspectionshowedan ulcer-ated lesion in the left anal margin, measuring about five centimetres in diameter at its longest axis, with poorly definededges,erythematous-violaceous,withirregular fun-dus,andpresenceofhyalinesecretion(Fig.1).Digitalrectal examinationand anoscopyshowed nochanges.There was no inguinal lymphadenopathy. Upon palpation ofthe jaw, increasedanglesofirregularsizewerenoted,whichweremore apparent on the left side. Abdominalexamination showed enlargedliverwithlefthepaticlobegoingbeyondthemidline. Therewerenootherchangesinthephysicalexamination.
Afterclinicalexamination,andrulingout thepossibility ofsexuallytransmittedandotheranorectaldiseases,biopsy and immunohistochemistryofthelesionwasperformedin analmarginandtherapeutictestswerestartedwithlocal tri-amcinoloneapplications,toelucidatethediagnosis.
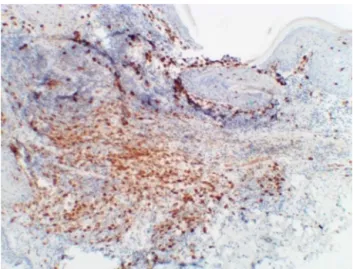
Pathological biopsyofthe ulceratedperianal skinlesion showedinfiltrateconsistingofamixtureofLangerhans’cells andeosinophilswithahistiocyticpattern(Fig.2). Immunohis-tochemistryshowedpositivityinthetestforsurfaceantigens CD1aandCD31,andconfirmedthediagnosisofLangerhans’ cellhistiocytosis(Figs.3and4).
Furtherinvestigationrevealedthefollowingchanges:
•Diabetesinsipidusandencephalicalterations,evidenced
byMRIwhichresultedintheabsenceofnormalhyperintensity oftheposteriorlobeofthepituitarygland,markedthickening ofthehypothalamicregionandsomethickeningofthe prox-imalportionsofthepituitarystalk,withatrophyofthedistal portions.
•Osteolyticlesionsintheskullandlowerlimbs,withX-ray
ofthelowerlimbsshowinghyperdenseboneareasinthetibia andtarsalbones;computedtomographyoftheskullshowed diffuseosteolyticlesions.
• Hepatomegaly observed in computed tomography of
Fig.1–Ulcerationintheanalmargin.
Fig.2–Photomicrograph(HE100×)showinginfiltrate
consistingofamixtureofLangerhans’cellsand eosinophils.
parenchyma;lymphadenopathyinthehepatichilum, porta-cavalchain,andbifurcationoftheceliactrunk.
Thepatientwasthenreferredtothecoloproctologyservice oftheUniversityofValedoItajaí,wherethemultidisciplinary carewouldbecomemoreviable.Attheservice,heunderwent assessment by the coloproctology, medical clinic, paedi-atric endocrinology, dermatology and haematology teams. The latter proposed starting chemotherapy, referring him tothe specializedcentre.Inadditiontolocaltriamcinolone applications,thepatientbeganchemotherapysessionswith Vinblastine,showingsignificantclinicalimprovement(Fig.5). Onthe recommendationofpaediatric endocrinology, treat-ment with Desmopressin (DDAVP) was indicated, with a significantreductionoftheurinarysymptomsinitially pre-sented.
Fig.3–Immunohistochemistry(200×)showingmembrane
patternreactivityforCD1a.
Fig.4–Immunohistochemistry(400×)showingmembrane
patternreactivityforCD31.
Discussion
Thereportedcaseisofamalepatient,ofschoolage,whose diagnosiswasbasedonulceratedskinlesionintheperianal region.Theperianal skindiseaseoutbreakreportsdescribe theinitiallesionaspruriticerythema,possiblyprogresstoa pink,friableandwartylesion,oralesionsimilartoaswollen skintag. This,inturn,could growtobecomeanextensive ulcerationwith infiltrated edges, which could compromise the entire circumference of the anal margin. In the case described,asimilarlesionwasobservedtothatreportedin theliterature.4,10,11Skinlesionsoflongerevolutionaremore frequentlyfoundinLangerhans’cellhistiocytosiswith multi-systeminvolvement.12
Among the non-skin disorders, diabetes insipidus is observedinapproximately50%ofpatients;osteolyticchanges in80%,andenlargedliverandspleeninapproximately20%.4,13 Osteolyticlesionsusuallyappearatamoreadvancedstageof disease,14inferringalongevolutionofthediseasedescribed. The involvement of craniofacial bones is associated with increasedriskofdiabetesinsipidusandincreasedfrequencyof adenohypophysealhormonedeficiency.7Intheabovepatient, all these signs were present. Furthermore, it is a young, malepatient,corroboratinginmanyaspectswiththecurrent literature.5,6,15
The diagnosis is often delayed, as the possibility of Langerhans’ cell histiocytosis is not usually considered, initially.3,5,6,10,16Asdescribedinthiscase,sexually transmit-teddiseasesandotheranorectaldisordersshouldberuledout, duetotheirhigherprevalencewhencomparedtoLangerhans’ cellshistiocytosis.
Histopathologyofthelesionguidesthediagnostic suspi-cionduetovisualizationofmixedinfiltrateinthepapillary dermis (Fig. 2). The abnormal proliferation of functionally immature Langerhans’ cells, morphologically surrounded byeosinophils,macrophagesandoccasionalmultinucleated giantcells,andBirbeckgranules(bodiesX),arecharacteristic detectionsofthispathology.3,11,16,17
Thediagnosticconfirmationisgivenbythe immunohisto-chemicalstudy,whenpositiveforCD1aandCD31antibodies (Figs.3and4),whicharehighlyspecificmarkersforhuman Langerhans’cell.3,10,11,16
Children and adolescents diagnosed with Langerhans’ cellhistiocytosisshouldreceivemultidisciplinarytreatment.7 In this study,after detailed evaluation bydifferent profes-sionals,it wasdecidedto continuethelocal triamcinolone applications, due to the good response shown by the patient. Faced with the pathophysiology of the disease, a proliferation of clonal cells, treatment with chemother-apeutic agents is a good choice. In the case described, Vinblastine was the prescribed medication. In patients with lesions of the bone, skin, lymph nodes, and dia-betes insipidus, therapy with Vinblastine and prednisone waseffectiveinpreventingreactivationofthedisease.18In casesofrecurrentperianallesions,radiationtherapymaybe considered.
PrognosticfactorsinLangerhans’cellhistiocytosiscanbe dividedandarrangedbyageatdiagnosis,responseto treat-ment,andinvolvementoforgans19;therapeuticresponseat
6–12weekshasbeenshowntobemoreimportantprognostic factorthanage.20
So far, the patient described in this case is showing favourabledevelopment,withsignificantregressionofthe ini-tiallesion.Ararediseaseisobserved,withawidespectrum of clinical manifestations,in apatient withcharacteristics compatible with the epidemiologicalprofileof thedisease, diagnosedbasedonadermatologicallesionintheperianal region, andwho showedsatisfactoryresponsetothe treat-mentused.
In view of this case, the importance is highlighted of payingheedtopatients’complaints,andofathorough physi-calexamination.Severaldiseaseshaveperianalinvolvement, and a proper investigation, through physical examination and local biopsies, determine the successofthe diagnosis inmostsituations.Thisreportisalsoimportantgiventhat thediagnosisofLangerhans’cellhistiocytosisisachallenge forthephysician,whorequiresprecisionand speed,and it shouldbekeptinmindasadifferentialdiagnosis,despiteits rareincidence.Theimportanceofdisseminatingknowledge ofthediseaseisalsoemphasized,seekingtoenableearlier diagnosis.3,5,6,10,16
Conflict
of
interests
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LaneCW,SmithMG.Cutaneousmanifestationsofchronic (idiopathic)lipoidosis(Hand-Schuler-Christiandisease): reportoffourcases.ArchDermatolSyphilol.1939;39:617–44.
2.LichtensteinL.HistiocytosisX:integrationofeosinophilic granulomaofbone,“Letterer-Swivedisease”and
Schüller-Christiandiseaseasrelatedmanifestationsofsingle nosologicentity.AMAArchPathol.1953;56:84–102.
3.CamposMK,VianaMB,deOliveiraBM,RibeiroDD,SilvaCM. HistiocitosedascélulasdeLangerhans:experiênciade16 anos.JPediatr(RioJ).2007;83:79–86.
4.GamaMRVS,SouzaHFS,GuerraGMLSR,FonsecaMFM, BálsamoF,FormigaGJS.HistiocitosedecélulasdeLangerhans perianal:Relatodecaso.RevBrasColoproct.2005;25:253–5.
5.OliveiraAJ,RamosAA,ImparatoJCP,AlencarAR,MenezesJFF. HistiocitosedecélulasdeLangerhans:revisãodeliteraturae apresentac¸ãodeumcasoclínico.RFacOdonto.2004;45:55–9.
6.FerreiraLM,DinizLM,RedighieriI,EmerichOS,LageL. HistiocitosedecélulasdeLangerhans:doenc¸ade
Letterer-Siwe–importânciadodiagnósticodermatológicoem doiscasos.AnBrasDermatol.2009;84:405–9.
7.PDQ® -LangerhansCellHistiocytosisTreatement:Health ProfessionalVersion.Availableat:http://www.cancer.gov/ types/langerhans/hp/langerhans-treatment-pdq#section/180. [accessed18June2016].
8.GoodmanWT,BarretTL.Histiocytoses.In:BologniaJL,Jorizzo JL,RapiniRP,editors.Dermatology.Philadelphia:Mosby;2003. p.1429–33.
9.AricòM,EgelerRM.ClinicalaspectsofLangerhanscell histiocytosis.HematolOncolClinNorthAm.1998;12:247–58.
11.NetoMS,CarvalhoCH,FadulJRR,AmbroginiC,FerreiraLM. HistiocitosedascélulasdeLangerhansnaregião
anogenital–relatodecaso.RevAssMedBrasil.1998;44:344–6.
12.MorrenMA,VandenBroeckeK,VangeebergenL,Sillevis-Smitt JH,VanDenBergheP,HaubenE,etal.Diversecutaneous presentationsofLangerhanscellhistiocytosisinchildren:a retrospectivecohortstudy.PediatrBloodCancer.
2016;63:486–92.
13.KaderHA,RuchelliE,MallerES.Langerhans’cellhistiocytosis withstoolretentioncausedbyaperianalmass.JPediatr GastroenterolNutr.1998;26:226–8.
14.KumarV,AbbasAK,AsterJC.RobbinsPatologiaBásica.9ed. RiodeJaneiro,2013.
15.Guyot-GoubinA,DonadieuJ,BarkaouiM,BellecS,ThomasC, ClavelJ.DescriptiveepidemiologyofchildhoodLangerhans cellhistiocytosisinFrance.2000–2004.PediatrBloodCancer. 2008;51:71–5.
16.RochaMTJr,TaveiraATA,DiasNA,ReisMF,FerreiraLCL. HistiocitosesdecélulasdeLangerhansnopaciente
pediátrico:apresentac¸ãodeumcasoclínico.RevCiênciasde SaúdedaAmazônia.2016;1:1.
17.LamanJD,LeenenPJ,AnnelsNE,HogendoornPC,EgelerRM. Langerhans-cellhistiocytosis‘insightintoDCbiology’.Trends Immunol.2003;24:190–6.
18.GadnerH,MinkovM,GroisN,PötschgerU,ThiemE,AricòM, etal.Therapyprolongationimprovesoutcomeinmultisystem Langerhanscellhistiocytosis.Blood.2013;121:5006–14.
19.GadnerH,GroisN,PötschgerU,MinkovM,AricòM,BraierJ, etal.ImprovedoutcomeinmultisystemLangerhanscell histiocytosisisassociatedwiththerapyintensification.Blood. 2008;111:2556–62.